
Abstract
This study compared the surgical outcomes of total laparoscopic hysterectomy (TLH) and vaginal-assisted natural orifice transluminal endoscopic surgery (vNOTES) in patients with a history of gynecologic and obstetric surgery. This cross-sectional study included 100 women who underwent TLH (n = 50) and vNOTES hysterectomy (n = 50) for benign gynecological pathologies. The demographic features and surgical outcomes of all the patients were recorded retrospectively. Postoperative hematocrit values, Visual Analog Scale (VAS) scores (6-24th hour), uterine weights, operation time, hospital stay, postoperative analgesic application requirement, blood transfusion, vaginal cuff closure time, and intraoperative and postoperative complications were assessed. There were no differences in demographic features between the groups. The need for analgesic application was similar between groups (p = 0.590). Vaginal closure time was significantly shorter in the vNOTES group (p < 0.001). The surgery time and hospital stay were significantly shorter in the vNOTES group (p = 0.001 and p = 0.006, respectively), and there was no difference in complication rates between the groups (p = 0.992). The preoperative Htc values were similar in both groups (P = 0.980). There was no significant difference in the postoperative Htc values (p = 0.901). Postoperative 6th hour VAS score of the vNOTES group was significantly lower than that of the TLH group (p = 0.001). The vNOTES hysterectomy procedure has more advantages than TLH in terms of minimally invasive surgery, even in patients with a history of gynecologic and obstetric surgery.
Similar content being viewed by others


Introduction
Hysterectomy is the most frequently performed gynecological operation worldwide. It can be performed laparoscopically, abdominally, or vaginally1. The vaginal route appears to be the least invasive method1. Total laparoscopic hysterectomy (TLH), which is widely used, was first described in 1988. Although the operation time was longer in the first application period of TLH, it decreased the level of abdominal hysterectomy after the learning process2. The natural orifice transluminal endoscopic surgery (NOTES) technique, defined as entering the peritoneal cavity using natural openings, was first described in 20043, and the reliability and applicability of vaginally applied NOTES were demonstrated in a study conducted in 20124. NOTES is a new technique that combines the advantages of endoscopic techniques and the vaginal route, and is used in an increasing number of gynecological operations5.
Studies have shown that vaginal NOTES (vNOTES) is associated with less blood loss, less postoperative pain, shorter hospital stay, better cosmetic results, and less postoperative morbidity than conventional laparoscopy6,7,8. Although a history of pelvic surgery poses a potential risk for complications, it may not be accepted as a contraindication for vNOTES9.
No study has compared vNOTES hysterectomy with TLH in patients with a history of surgery. Within the scope of this study, we aimed to elucidate the surgical and visual analog pain (VAS) score outcomes of vNOTES hysterectomy and TLH procedures in patients with a history of previous surgery for benign reasons.
Materials and methods
This study reviewed the records of patients who underwent vNOTES hysterectomy (group 1) and TLH (group 2) in our Gynecology and Obstetrics clinic between January 2023 and July 2024. This study was conducted in accordance with the guidelines set forth in the Declaration of Helsinki and approved by the Diyarbakır Gazi Yaşargil Training and Research Hospital Ethics Committee (approval no: 174/2024). A total of 100 consecutive patients aged > 18 years with a history of gynecological pelvic surgery or cesarean section were included. The choice of surgical approach (vNOTES or TLH) was determined by the operating surgeon’s preference and the patient’s anatomical characteristics (e.g., uterine size and vaginal access), which is a common practice during the adoption phase of a new technique. Thus, the cohort was divided into two groups: 50 patients who underwent vNOTES hysterectomy and 50 patients who underwent TLH for benign gynecological diseases. All individuals provided their written, informed permission for the use of their clinical data in this study.
Patients with a history of endometriosis, gynecological malignancy, pelvic radiotherapy, and pelvic inflammatory disease were excluded from the study.
All patients underwent preoperative gynecological examinations, and cervical smear tests were performed and evaluated using ultrasonography. Informed consent was obtained from all the patients preoperatively. Patient age, Body Mass Index (BMI), parity, previous surgical history, and preoperative and postoperative blood counts were recorded. Postoperative hematocrit values, visual analog scale scores (6-24th hour), uterine weights, operation time, hospital stay, postoperative analgesic requirement, blood transfusion, vaginal cuff closure time, and intraoperative and postoperative complications were evaluated. All procedures in both the vNOTES and TLH groups were performed by a dedicated team of three senior surgeons from the same institution. All procedures were proficient in both conventional laparoscopy and the vNOTES technique, which independently performed a minimum of 50 procedures of each type prior to the commencement of this study to ensure that outcomes were not influenced by the initial learning curve.
In both groups, surgery was performed under general anesthesia with endotracheal intubation in the lithotomy position. A standardized intraoperative and postoperative pain management protocol was used for all patients. Anesthesia was maintained with sevoflurane and intraoperative analgesia consisted of fentanyl and paracetamol. For postoperative pain management, all patients were administered intravenous opioids (e.g., tramadol) on an as-needed (PRN) basis when their Visual Analog Scale (VAS) score was greater than 4. The total amount of opioids consumed by each patient during the first 24 h was meticulously recorded. A key finding of this study was that the total postoperative opioid requirement was significantly higher in the TLH group than in the VNOTES group. No local anesthetics or regional blocks were used in either group, ensuring that any differences in early postoperative pain and analgesic consumption could be attributed to the surgical technique. Preoperatively, 2 g and 3 g of intravenous cefazolin were administered according to the patient’s BMI. All patients received urinary and nasogastric catheters during surgery.
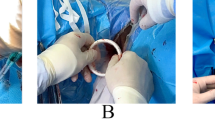
vNOTES hysterectomy procedure
Patients were placed in a high lithotomy position. The anterior and posterior lips of the cervix were held with tenaculum. A circumferential cervical incision was made with.
monopolar cautery. The cervical fascia was separated from the vaginal mucosa by dissection. Posterior colpotomy was opened with sharp dissection. The cardinal and sacrouterin ligaments were then grasped, cut, tied, and suspended with sutures. Anterior colpotomy was then performed. The abdomen was placed with a retractor and observed. The metal retractors were then removed, and an access platform (GelPoint vPath®, Applied Medical, Rancho Santo Margarita, CA) was placed. Pneumoperitoneum was created by CO2 insufflation. The pressure was adjusted to 12 mm Hg. Three trocars were used in the study. A 30 °camera was inserted through a 10 mm trocar. The other laparoscopic instruments were inserted through a 5-mm trocar. The bipolar electrocoagulation (LigaSure™, Covidien Company, MA, USA) energy modality was used for tissue cutting. The uterine vessels, adnexal pedicles, and infundibulopelvic ligaments were caudally and cranially divided. The specimen was then vaginally removed. The vaginal cuff was peritonized and sutured with a polyglactin 910 1 − 0 suture (Vicryl®, Ethicon, Piscataway, NJ, USA).
TLH procedure
All the patients underwent surgery in the lithotomy position. A Veres needle (Ethicon Endo- Surgery, Inc., USA) was inserted through the umbilical incision, and the abdomen was inflated with CO2 to 20 mmHg. After entering the abdomen from the umbilicus with a 10 mm trocar, a 30° 10 mm optic camera was inserted. The patient was placed in a Trendelenburg position. The pressure was then reduced to 15 mm Hg. In all cases, a uterine manipulator (RUMI-II®, CooperSurgical, Trumbull, USA) uterine manipulator was used to manipulate the uterus. After visualizing all abdominal organs, 5 mm trocars were inserted: two from the left and one from the right. Bipolar electrocoagulation (LigaSure™; Covidien Company, MA, USA) was used as the energy source. The uterine artery and ligaments were cut cranially and caudally, respectively. The bladder was then excised from the uterus. The parametrial tissue around the cervix was dissected using ligature. Circular colpotomy was performed over the uterosacral ligament with monopolar cautery, and the uterus was completely separated from the vagina. The uterus and adnexa were removed from the vagina to the exterior of the abdomen. The vaginal cuff was closed laparoscopically using a polyglactin 910 1 − 0 suture (Vicryl®; Ethicon, Piscataway, NJ, USA).
Statistical analysis
SPSS 26 software was used for all statistical analyses, and both parametric and nonparametric tests were used to compare the vNOTES and TLH groups. Differences between groups for normally distributed continuous variables (e.g., age, BMI, uterine weight, analgesic use, HTC, and VAS pain scores) were assessed using the independent samples t-test, and differences between preoperative and postoperative measurements were evaluated using the dependent samples t-test. The Mann-Whitney U test was used for non-normally distributed or ordinal data (e.g., surgery duration, hospital stay, and number of complications). In all analyses, p < 0.05 was the basis for statistical significance.
Post-hoc power analysis was performed using the t-test. Assuming a medium effect size (Cohen’s d = 0.5), total sample size (n = 100), and error rate of 5% (α = 0.05), the statistical power of the study was calculated to be 80.6%. An 80% power level, generally accepted in the literature, indicates that the probability of detecting a significant effect is sufficient for this study10. Accordingly, the value of 80.6% obtained was considered appropriate in terms of the reliability of the study.
Results
This study included 100 patients who underwent 50 vNOTES hysterectomy (group 1).
and 50 TLH (group 2) for benign reasons and had a history of previous surgery. No significant differences were found between the groups with respect to age, parity, or BMI (p = 0.749, p = 0.454, and p = 0.982, respectively) (Table 1). There were no significant differences between the groups in terms of the variety of previous gynecologic or obstetric surgeries (p = 0821Cesarean section was the most common prior surgery in both groups. The mean number of prior cesarean sections per patient was similar between the vNOTES group (1.0 ± 1.1) and the TLH group (1.08 ± 1.2), and this difference was not statistically significant (p = 0.621) (Table 1). Therefore, the data obtained in this study are comparable. The mean uterine weight did not differ between the groups based on the final pathological results (p = 0.067) (Table 2). There was no significant difference in analgesic use between the groups (p = 0.590). The vaginal closure time was shorter in the vNOTES group (p < 0.001) (Table 2). Surgery duration and duration of hospital stay were significantly more advantageous in the vNOTES group (p < 0.001 and p = 0.006, respectively) (Table 2). Surgical complications occurred in two patients in both groups. No significant differences were found in terms of complications (p = 0.992) (Table 2). In Group 1, one patient had bladder perforation and two patients had postoperative ileus. In Group 2, one patient had bladder perforation (Table 2).
A comparison of the preoperative and postoperative Htc values between the vNOTES and TLH groups is shown in Table 3.Preoperative Htc values were similar in both groups (p = 0.980), and no significant difference was found in the postoperative Htc values (p = 0.901). This shows that the two surgical methods have similar blood loss profiles. However, a significant decrease was observed from the preoperative Htc values to the postoperative values in both groups (p < 0.001), which shows that both surgical methods have similar blood loss profiles. These findings revealed that the safety profiles of the vNOTES and TLH methods are similar in terms of blood loss.
The groups’ postoperative VAS scores at 6 and 24 h are compared in Table 4. At 6 h, the pain score in the vNOTES group was significantly lower than that in the TLH group (p = 0.000), indicating that the vNOTES method provided better pain management in the early period. However, at 24 h, no significant difference was found in the pain scores between the two groups (p = 0.847). These results indicate that the vNOTES method is more advantageous in terms of pain management in the short term, but the pain levels between the two methods equalized within 24 h.
Discussion
Minimally invasive gynecologic surgery has gained popularity annually6. Restrictions of these types of surgeries are thought to be due to previous pelvic surgeries or obesity9,11. It can cause adhesions between pelvic organs and structures; therefore, some surgeons may decide to perform open surgery or conventional laparoscopic surgery instead of vNOTES. This study provides a critical head-to-head comparison of vNOTES and TLH in a challenging patient cohort with a history of prior pelvic surgery. Our principal findings demonstrate that vNOTES is not only a feasible and safe alternative but also offers significant advantages in this high-risk population. Specifically, vNOTES was associated with shorter operative times, reduced early postoperative pain, and faster hospital discharge than conventional TLH, without an increase in complication rates. These results challenge the traditional reluctance to apply novel vaginal techniques in patients with potentially altered pelvic anatomy9. Perhaps the most significant clinical advantage observed was the efficiency of bladder dissection in the vNOTES group. By approaching the cervix transvaginally, the vNOTES technique allows the surgeon to develop a clean anatomical plane ‘from the bottom up,’ effectively bypassing the most common areas of dense post-cesarean scar tissue. This is in stark contrast to conventional ‘top-down’ laparoscopic dissection, which must first navigate this potentially hostile adhesive field. Although our study population consisted exclusively of patients with a history of gynecologic or obstetric surgeries, conversion to open surgery was not necessary in any case. Baekelandt et al. emphasized that previous surgical history was not an obstacle to vNOTES surgery; however, their study was only a case series that included nine patients. However, this study included a large number of patients9.
One study reported that the vNOTES method is effective and safe for obese patients11. We also found that the vNOTES method is effective and safe in patients with a history of previous pelvic surgery who are considered surgically at risk, as well as in overweight patients. A study comparing vNOTES hysterectomy and TLH reported that better results were obtained in the vNOTES group with shorter hospital stays and less surgical time12. Our study determined that hospital stay was shorter in the vNOTES hysterectomy group than in the TLH group in patients who underwent hysterectomy for benign reasons. We also found that the surgery time was significantly lower in the vNOTES hysterectomy group.
One study found that patients who underwent vNOTES had lower postoperative pain and postoperative wound infection rates, and this study also reported good cosmetic results13. However, we did not detect postoperative wound infection in either group, and achieved better cosmetic results in the vNOTES group. Kim and Kaya et al. reported that no significant difference was observed in terms of postoperative 6th and 24th-hour vas scores in patients who underwent vNOTES surgery14,15. In contrast, our study found the postoperative 6th-hour vas score was significantly lower in the vNOTES group. Because the vNOTES procedure is performed by entering the abdomen using the natural vaginal orifice without making an incision on the anterior abdominal wall, it causes less nerve injury. The reason for the lower postoperative 6th-hour pain level compared with TLH may be this. The meta-analysis showed that vNOTES had shorter operation time, shorter hospital stay, and less blood loss than TLH16, but we did not find a difference between the groups in terms of blood loss in our study. In the Halon study, the surgery time was longer in the vNOTES group than in the TLH group (61versus 41 min). In contrast, our study found that the surgical time was shorter in the vNOTES group. We believe that this was probably due to the shorter vaginal closure time during vNOTES. A study comparing single-port TLH with vNOTES hysterectomy found less pain and less surgical time in the vNOTES group, similar to our results17. We found that the vaginal closure time was shorter in the vNOTES group, which is consistent with the results of a previous study.
A key contributor to the shorter overall surgical time in the vNOTES group was the significantly faster vaginal cuff closure, a finding that warrants deeper discussion. This advantage is likely multifactorial and is rooted in the fundamental ergonomics of the vNOTES approach. First, the transvaginal platform provides direct, straight-line access to the vaginal cuff, which is anatomically a more natural and efficient angle for suturing than the often challenging tangential angles required in conventional laparoscopy. Second, visualization of cuff edges is typically superior and more stable with vNOTES, minimizing the need for extensive tissue manipulation to expose the suturing plane. Finally, the entire process of needle introduction, driving, and knot tying is performed in a more confined but direct workspace, which can be considerably faster than intracorporeal suturing performed at a distance in TLH. This combination of superior ergonomics, direct visualization, and efficient suturing mechanics directly translates to a significant reduction in the key time-consuming steps of the procedure, thereby contributing substantially to the shorter total operative time.
It is also important to contextualize our study’s patient population. We deliberately excluded patients with severely distorted pelvic anatomy due to extensive adhesions or advanced endometriosis to ensure procedural safety during the initial adoption of this novel strategy. We concur with the notion that other advanced surgical platforms may be more appropriate for this challenging subgroup of patients. Specifically, robotic surgery can offer enhanced 3D visualization and instrument dexterity, potentially providing a viable minimally invasive alternative to open surgery in complex cases18,19.
Beyond shorter operative times and reduced early postoperative pain, a significant advantage of the vNOTES approach is its superior cosmetic outcomes. Although this study did not employ a formal patient-reported cosmetic scale, this superiority is based on an objective, undeniable procedural difference: the complete absence of abdominal incisions. Unlike TLH, which necessitates a minimum of three to four port-site incisions resulting in permanent scars, vNOTES is a truly ‘scarless’ abdominal surgery from the patient’s external perspective. This inherent advantage is a critical component of preoperative patient counseling and is emerging as a significant factor in patient preference for minimally invasive techniques16,20.
This study had several important limitations that must be acknowledged. First, the retrospective design introduces an inherent risk of selection bias, particularly in the allocation of the surgical method, which is based on surgeon preference rather than randomization. While the groups were well-matched in terms of baseline characteristics, unmeasured confounding variables may still exist. Second, as this was a single-center study involving a small cohort of 100 patients, the generalizability of our findings to other settings with different patient populations or surgical teams may be limited. The single-team experience, while ensuring consistency, also means that our results reflect the outcomes after the initial learning curve, which may not be immediately replicable by surgeons new to the vNOTES technique. Finally, our follow-up was limited to the immediate postoperative period, and long-term outcomes, particularly pelvic organ prolapse recurrence, were not assessed.
Conclusion
Our study showed that vNOTES is a safe and effective method in patients who have undergone pelvic surgery, with less surgical time, lower 6th-hour VAS scores, shorter hospital stays, and better cosmetic results. Our study contributes to the literature and encourages practitioners owing to the limited number of publications. However, this relatively new method requires a larger series and longer-term studies.
Data availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Change history
16 December 2025
The original online version of this Article was revised: In the original version of this Article the ORCID ID for Süleyman Cemil Oğlak was omitted. The ORCID ID for Süleyman Cemil Oğlak is 0000-0001-7634-3008. The original Article has been corrected.
References
Aarts, J. W. et al. Surgical approach to hysterectomy for benign gynecological diseases. Cochrane Database Syst. Rev. 2015 (8), CD003677. https://doi.org/10.1002/14651858 (2015).
Wattiez, A. et al. The learning curve of total laparoscopic hysterectomy: comparative analysis of 1647 cases. J. Am. Assoc. Gynecol. Laparosc. 9 (3), 339–345. https://doi.org/10.1016/s1074-3804(05)60414-8 (2002).
Kalloo, A. N. et al. Flexible transgastric peritoneoscopy: a novel approach to diagnostic and therapeutic interventions in the peritoneal cavity. Gastrointest. Endosc. 60 (1), 114–117. https://doi.org/10.1016/s0016-5107(04)01309-4 (2004).
Ahn, K. H. et al. Transvaginal single-port natural orifice transluminal endoscopic surgery for benign uterine adnexal pathologies. J. Minim. Invasive Gynecol. https://doi.org/10.1016/j.jmig.2012.04.001 (2012).
Kaya, C. et al. Hysterectomy by vaginal-assisted natural orifice transluminal endoscopic surgery: initial experience with twelve cases. J. Turk. Ger. Gynecol. Assoc. 19 (1), 34–38. https://doi.org/10.4274/jtgga.2017.0075 (2018).
Li, C. B. & Hua, K. Q. Transvaginal natural orifice transluminal endoscopic surgery (vNOTES) in gynecologic surgeries: A systematic review. Asian J. Surg. 43 (1), 44–51. https://doi.org/10.1016/j.asjsur.2019.07.014 (2020).
Kapurubandara, S. et al. Consensus on safe implementation of vaginal natural orifice transluminal endoscopic surgery (vNOTES). Eur. J. Obstet. Gynecol. Reprod. Biol. ; 263:21–222.https://doi.org/10.1016/j.ejogrb.2021.06.019 (2021).
Baekelandt, J. et al. HALON-hysterectomy by transabdominal laparoscopy or natural orifice transluminal endoscopic surgery: a randomised controlled trial (study protocol). BMJ Open. 6 (8), e011546. https://doi.org/10.1136/bmjopen-2016-011546 (2016).
Vanhooren, E. & Baekelandt, J. Vaginal NOTES surgery in patients with prior hysterectomy: A first case series. Asian J. Endosc. Surg.https://doi.org/10.1111/ases.12940 (2021).
Keskin, B. Does statistical power affect the results of a study?? How to decide on sample size?? Manisa Celal Bayar Univ. J. Social Sci. 18 (Armagan Issue), 157–174. https://doi.org/10.18026/cbayarsos.644692 (2020).
Mat, E. et al. Transvaginal natural orifice endoscopic surgery for extremely obese patients with early-stage endometrial cancer. J. Obste Gynaecol. Res. 47 (1), 262–269. https://doi.org/10.1111/jog.14509 (2021).
Baekelandt, J. F. et al. Hysterectomy by transvaginal natural orifice transluminal endoscopic surgery versus laparoscopy as a day-care procedure: a randomised controlled trial. BJOG 126 (1), 105–113. https://doi.org/10.1111/1471-0528.15504 (2019).
Michener, C. M. et al. Meta-analysis of laparoendoscopic Single-site and vaginal natural orifice transluminal endoscopic hysterectomy compared with multiport hysterectomy: real benefits or diminishing returns?? J. Minim. Invasive Gynecol. 28 (3), 698–709e1 (2021).
Kim, M. S., Noh, J. J. & Kim, T. J. Hysterectomy and adnexal procedures by vaginal natural orifice transluminal endoscopic surgery (VNH): initial findings from a Korean surgeon. Front. Med. (Lausanne). 7, 583147. https://doi.org/10.3389/fmed.2020.583147 (2021).
Kaya, C. et al. Comparison of hysterectomy cases performed via conventional laparoscopy or vaginally assisted natural orifice transluminal endoscopic surgery: a paired sample cross-sectional study. J. Obstet. Gynaecol. 41 (3), 434–438 (2021).
Housmans, S. et al. Systematic review and Meta-Analysis on hysterectomy by vaginal natural orifice transluminal endoscopic surgery (vNOTES) compared to laparoscopic hysterectomy for benign indications. J. Clin. Med. 9 (12), 3959. https://doi.org/10.3390/jcm9123959 (2020).
Noh, J. J. et al. Comparison of surgical outcomes of hysterectomy by vaginal natural orifice transluminal endoscopic surgery (vNOTES) versus Single-Port access (SPA) surgery. J. Pers. Med. 12 (6), 875. https://doi.org/10.3390/jpm12060875 (2022).
Perrone, A. M. et al. Combined robotic and vaginal surgery for pelvic exenteration due to vaginal sarcoma relapse in an obese woman. J. Minim. Invasive Gynecol. 31 (10), 823–824 (2024).
Perrone, A. M. et al. Synergizing health: combined gynecological and bariatric robotic surgery for endometrial cancer in obese women. Int J Gynecol Cancer. 34(6):956–957. https://doi.org/10.1136/ijgc-2023-005121. (2024).
Halisçelik, M. A. et al. Comparison of pelvic organ prolapse and sexual function after vaginal natural orifice transluminal endoscopic surgery and conventional laparoscopic hysterectomy. J. Clin. Med. 14 (8), 2590. https://doi.org/10.3390/jcm14082590 (2025).
Author information
Authors and Affiliations
Contributions
Surgical and Medical Practices: M.A.H., S.C.O., İ.B., S.A., B.C., K.A., A.D.E; Concept: M.A.H., S.C.O., İ.B., S.A., B.C., K.A., A.D.E., S.E., M.B., C.B.; Design: M.A.H., S.C.O., İ.B., S.A., B.C. M.O., C.Ş.; Data Collection or Processing: M.A.H,, K.A., A.D.E.; Analaysis or Interpretation: M.A.H., S.C.O., İ.B.; Literature Review: M.A.H., S.C.O., İ.B., B.C.; Writing: M.A.H., S.C.O., İ.B., S.E.; Critical Review: M.A.H., S.C.O., İ.B.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Diyarbakır Gazi Yaşargil Training and Research Hospital (approval no: 174/2024). All study procedures complied with the ethical standards of the institutional and national committees and the Declaration of Helsinki. Informed consent was obtained from all participants.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Halisçelik, M.A., Oğlak, S.C., Bağlı, İ. et al. Comparison of conventional laparoscopic hysterectomy and vNOTES hysterectomy in previous pelvic surgery: a retrospective study. Sci Rep 15, 30629 (2025). https://doi.org/10.1038/s41598-025-16525-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-16525-0
