
Abstract
Amid the alarming global forecast of age-related cognitive-communicative disorders like dementia, Speech-Language Pathologists (SLPs) are poised to play a crucial role in dementia-related services, ranging from counselling to end-of-life care. A key step in this direction is enhancing public health literacy regarding optimal age-linked cognitive-communicative health. Given the potential of educational multimedia (EM) programs to promote public health literacy, and the recent development of one such EM in our research, this study aimed to evaluate the efficacy of an SLP-designed and facilitated EM in changing young adults (YAs) knowledge and beliefs about cognitive health in the Indian context. In a randomized controlled trial, 220 YAs aged 18–25 years were equally and randomly assigned to either the experimental group (EG) or the active control group (CG). The EG viewed an EM on cognitive health, while the CG watched an animated fictional video. Both groups completed a retrospective pre-post survey evaluating self-perceived knowledge, factual knowledge, and beliefs about cognitive health. The effect of the EM was analyzed using mixed-model ANOVA. A significant improvement in the EG compared to the CG across all three domains was observed. These findings highlight the efficacy of the EM in enhancing understanding and attitudes toward cognitive health among YAs. The EM shows promise as a structured cognitive health education tool, fostering awareness, encouraging preventive measures, and potentially contributing to early detection and intervention of cognitive health issues. This study aligns with the emerging role of SLPs in educating communities about cognitive-communicative health and well-being.
Similar content being viewed by others


Introduction
According to the Global Burden of Diseases (GBD) 2019 Dementia Forecasting Collaborators, an estimated 57.4 million people worldwide were affected by dementia in 2019, a number projected to rise to 152.8 million by 20501. In light of this, a survey by the American Speech-Language-Hearing Association (ASHA) reported that dementia-related services constitute the second largest area of clinical practice for Speech-Language Pathologists (SLPs)2. A recently published work outlining the role of SLPs in Mild Cognitive Impairment (MCI) and Dementia-related services has underscored a critical area of responsibility as 'Counselling+' activities, in addition to the standard screening, assessment, and management services3. In addition to addressing the psychosocial aspects of cognitive disorders and collaborating with healthcare professionals, individuals, and families to enhance services and optimize outcomes, the 'Counseling+' role for SLPs also integrates a critical focus on prevention of age-linked cognitive communicative disorders and the associated wellness, aimed at mitigating both the prevalence and impact of these conditions3. Prevention and wellness related activities include dissemination of knowledge regarding measures for healthy cognitive lifestyle, age-associated cognitive declines, and cognitive pathologies, targeting the community at large. Enhancing cognitive health awareness among the general population has also been emphasized by the 'Global Action Plan on public health’s response to Dementia’4. As such, it may be a logical and necessary task for SLPs to focus on enhancing public health literacy (HL) about cognitive health among typically aging adults as part of our professional responsibilities.
HL is an important predictor of health outcomes since it defines the capacity of an individual to receive, process, communicate information related to basic health decisions5. Individuals with low HL are associated with higher hospitalization rates, developing more medical conditions6 and poor adherence to medication7. Recent studies indicate a significant association between low HL and high risk of developing Mild Cognitive Impairment (MCI)8,9 and Alzheimer’s disease10. Poor HL correlates with reduced cognitive abilities across many of its domains9,11,12,13. On the contrary, optimum HL is associated with increased participation in cognitive, social, and physical activities13,14. Individuals with high levels of HL promote and maintain good health not only for themselves but their families and communities15. Consequently, possessing good cognitive HL is both a personal and social resource, yielding society benefits thereby prompting policy makers and the health care system to provide adequate, appropriate, and accessible information to the society16. Therefore, prioritizing the enhancement of cognitive health literacy is paramount for facilitating wellness and preventive measures.
A wide range of studies have been carried out with the aim of advancing knowledge and beliefs pertaining to cognitive health literacy. In this regard, Aihara and Maeda17 investigated the effectiveness of the "Dementia Supporter Caravan" campaign in Japan, which included in-person classes educating on dementia. Heger et al.18 assessed the impact of an e-health promotion campaign called "My Brain Coach," focusing on three themes: maintaining a healthy diet, regular exercise, and fostering curiosity. Farina et al.19 explored the influence of dementia awareness classes on changing attitudes toward dementia, while Askari et al.20 aimed to evaluate a dementia awareness campaign that utilized the Community-based Participatory Research (CBPR) model to develop training materials for social workers. The outcomes of these studies collectively affirm the positive impact of HL programs in shaping knowledge and beliefs related to cognitive health.
While prior research has primarily focused on improving cognitive HL among aging populations, there is a relative lack of emphasis on enhancing cognitive health awareness and skills among younger adults. Developing these skills and safeguarding mental well-being should begin at an early life stage to yield greater long-term benefits. Research has demonstrated that cognition enhancing activities undertaken during young adulthood are associated with improved cognitive functioning in later years21,22. Promoting cognitive health literacy among this demographic is essential, as they represent the future population at increased risk of cognitive pathologies, making them a crucial target for preventive interventions. Thus, proactive initiatives to enhance cognitive health in young adulthood can help mitigate the risk of cognitive disorders in old age23. Educating young adults (YAs) can yield positive impacts not only on their personal health, but also on the well-being of their families and communities, as they can contribute to the cognitive functioning of those around them24. Additionally, cultivating an attitude of promoting cognitive well-being during young adulthood can help mitigate cognitive deficits associated with acquired brain injuries, benefiting their current cognitive functioning as well23.
Innovative digital media tools hold significant potential to enhance cognitive HL among YAs, given the recent surge in internet accessibility. As of 2022, online usage was higher among individuals aged 15–24 years25,26. One of the most widely used digital media for promoting HL in the recent years is an Educational Multimedia (EM). EM-based programs can enhance communication and educational experiences of individuals with limited HL by decreasing reliance on reading skills, and instead providing information through visual aids and audio presentations. EM have been shown to better hold participants’ interest, enhance their experience, satisfaction, knowledge, and behavior change while also improving information retention27,28. While generic health promotion programs and campaigns frequently encounter challenges in engaging diverse communities due to the oversight of unique cultural and linguistic aspects within segmented populations29, a well-designed multimedia provides flexibility in its delivery and can be tailored to meet linguistic, cultural, and physical needs of diverse populations.
In the Indian context, one such promising digital health tool such as EM has potential for wide reach and impact, given the rapid pace of digitization in the country with over 900 million internet users30. Recognizing this potential of EM tools in India, one of our recent projects involved a team of SLPs, with expertise in cognitive-communication, designing a comprehensive, evidence-based EM aimed at promoting cognitive well-being in the Indian population31. This resource, carefully tailored to the linguistic and cultural context of its target audience, demonstrates great promise in supporting public health initiatives focused on cognitive health31. Following the demonstration of robust content validity, high levels of understandability, and strong actionability, the next step will be to evaluate its real-world impact in enhancing public health literacy about cognitive health among diverse demographic groups. Empirical evaluation of this resource could offer concrete evidence of its effectiveness in advancing cognitive well-being, moving it from theoretical potential to proven utility in practice. This EM could then be advocated among clinical practitioners in the field of cognitive sciences as a structured educational intervention aiming to enhance cognitive health literacy.
Materials and methods
The research followed a randomized controlled trial (Clinical Trail Registration Number: CTRI/2022/08/044785 registered on 22.08.2022) and was conducted between January 2022 and February 2023. Ethical approval was obtained from the Institutional Ethics Committee (IEC KMC MLR 05-2022/171). All methods and procedures were performed in accordance with the relevant guidelines and regulations.
Participants
The study recruited healthy YAs aged 18–25 years32, who were pursuing non-health-related bachelor’s degrees at an institute in Mangalore, India. Those with a history of neurological, psychological, or psychiatric disorder, and uncorrected hearing or vision were excluded. Functional disability among the participants was assessed using the WHODAS 2.033. A total of 220 YAs met the selection criteria and were recruited for the study. Participants were randomized in 1:1 ratio to either experimental group (EG) (n = 110) or active control group (CG) (n = 110) using the block size of four and the sealed envelope approach. Six respondents from EG and 34 from CG had incomplete questionnaire responses and thus excluded. Thus, the total number of responses from EG was 104 and CG was 76. Individuals in EG viewed the EM related to cognitive health, whereas those in the CG viewed an animated fictional video lacking any educational content about cognitive health. Informed consent and demographic details were obtained at the beginning of the study. Appropriate permissions were obtained from the university authorities for recruitment of the participants.
Intervention
The EM on cognitive health developed in our previous work31 was selected as the EM intervention for the EG in the present study due to its comprehensive coverage of cognitive health topics and favorable validation scores it received in both scientific and technical evaluations, as assessed by stakeholders such as SLPs and representatives of general public. The development of this educational content is guided by theoretical foundations, including the integrated HL framework, the cognitive health module provided by the National Institute of Aging, and scientific methodologies such as the modified nominal group technique. The total duration of the EM on cognitive health is 15.38 min revolving around key aspects related to cognitive aging, MCI and dementia, cognitive reserves and metacognition. The components of the EM, including theme-specific details, approaches employed to convey the content, and the duration of each segment, are outlined in Fig. 1. This multimedia disseminates the information in an animated form featuring a central character, Dr. Cognition, who delivers a 'TED-like’ talk titled ‘Towards healthy cognitive aging’ in an engaging and interactive manner. The interaction between Dr. Cognition and the audience serves as a crucial element in keeping viewers engaged. The content of the EM possesses a content validation index of 0.93 and 0.86, and ratings of 92.8% and 98.8% for understandability and 100% for actionability from SLPs and general public.

Description of the educational multimedia.
The CG viewed a pre-existing animated fictional video in which a central character attempts to start small food-related businesses from his home. The video featured simple English dialogues spoken solely by the central character and depicted goal-directed sequences delivered in a neutral tone. It contained no content related to health, cognition, or aging. This video was selected to closely match the experimental video in terms of animation style and duration.
To evaluate the structural and affective comparability of the videos used for the EG and CG, a pilot validation was conducted using a 5-item Likert scale assessing visual engagement, attention-holding capacity, emotional response, enjoyment, and background score. Two independent groups of YAs (n = 10 each), distinct from the main study participants and exposed to either the experimental or control video, rated these dimensions. Statistical comparisons using the Mann–Whitney U test revealed no significant differences across any parameter: visual engagement (U = 45, p = 0.71), attention-holding capacity (U = 28.5, p = 0.09), emotional response (U = 37.5, p = 0.32), enjoyment (U = 31.5, p = 0.15), and background score (U = 31, p = 0.113). These findings suggest that the two videos were structurally and affectively comparable, apart from their thematic content.
Instrument to assess knowledge and beliefs about cognitive health
A retrospective pre-post questionnaire was developed based on the framework used in the EM31, specifically assessing the attributes such as cognitive domains and importance of cognitive health, cognitive changes in typical and pathological aging, cognitive disorders and risk factors associated with it, and preventative measures for cognitive well-being that it claimed to address. The questionnaire was also informed by elements from the Global Brain Health Survey34. Retrospective pre-post questionnaire are known to minimize the potential impacts of response-shift bias and improve the accuracy of measure of change35. In this study, participants rated their knowledge and beliefs about cognitive health after the intervention, reflecting on their perspectives before and after viewing the EM content through a retrospective pre-post questionnaire. Six SLPs, with over a decade of experience in cognitive sciences, validated the appropriateness of the questionnaire using a 5-point Likert scale where 1—“High inappropriate/Highly incomprehensible/Highly irrelevant”; and 5—“Highly Appropriate/Highly comprehensive/Highly relevant. Modifications were made based on their recommendations to finalize the questionnaire. The modifications included adding a “Not Sure” option for select questions, presenting pre- and post-ratings within a single table for easier comparison, and incorporating descriptive phrases alongside rating scale options for certain items to enhance clarity. The final questionnaire received an acceptable score of > 0.83 by the examiners.
The final questionnaire comprised 15 questions across three domains: Self-perceived Knowledge (SK), Factual Knowledge (FK), and Beliefs (Bf) regarding cognitive health (Tables 1, 2 & 3). SK had three questions, scored on a 4-point scale (maximum score: 12). FK included seven questions, each scored 0.5, 0.75, or 1, with a total possible score of 63. The belief domain consisted of five questions, rated on four or five points, with a potential total score of 68. Additionally, ten YAs outside the study completed the questionnaire twice to assess test–retest reliability, yielding a satisfactory interclass coefficient of 0.87, indicating good reliability.
Procedure
Data collection took place in university auditorium halls, with participants from the EG and CG seated separately in different auditoriums. Investigators provided both groups with a brief introduction to the session’s purpose and schedule, ensuring a distraction-free environment. The EG watched an educational video on cognitive health, while the CG watched a pre-existing animated video of equal duration which was not related to brain health. Both videos were shown on a large screen with audio through loudspeakers. Participants from both groups completed a retrospective pre-post survey on cognitive health immediately after watching the videos. The survey was administered using a paper-and-pen format. To ensure an accurate baseline for assessing participants’ initial knowledge, and to minimize recall bias and overestimation of change, participants were instructed prior to completing the form as follows.
“For each item on the questionnaire, please reflect on how you would have rated yourself before watching this video on healthy cognitive aging. Then, indicate your level of knowledge after watching the video for the same item. If you’re unsure, you may select the ‘Unsure’ option. There are no right or wrong answers—please respond as honestly as possible.”
Data analysis
Data from the retrospective pre-post questionnaire was analyzed using Jamovi software (v2.3.21). Descriptive statistics were used to calculate the mean and standard deviation of the pre- and post-test scores on the SK, FK, and Bf domains. A mixed model ANOVA with a post hoc Bonferroni pairwise analysis was conducted to examine the effects of an EM intervention on knowledge and beliefs related to cognitive health between the EG and CG.
Results
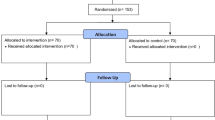
The flow of participants through this study is presented in Fig. 2. Participants from both the groups were significantly similar in terms of age [t(178) = − 0.583, p = 0.560], gender [\({\chi }^{2}\)(180) = 0.989, p = 1], family history of Dementia [\({\chi }^{2}\)(180) = 0.00251, p = 0.960], acquaintance with Individuals with dementia [\({\chi }^{2}\)(180) = 0.0588, p = 0.808], prior exposure to multimedia on cognitive health [\({\chi }^{2}\)(180) = 0.0331, p = 0.856], and acquaintance with health professionals [\({\chi }^{2}\)(180) = 0.132, p = 0.716]. The demographic details are illustrated in Table 4.

Flow of participants through the evaluation.
Effect of the educational multimedia on knowledge and belief about cognitive health
The mean scores for both groups across both time points on all the three domains are provided in Figs. 3, 4 and 5. There were no statistically significant differences in baseline scores between both groups across any of the three domains (SK (t = − 0.47, p = 1.0), FK (t = − 1.92, p = 0.34), and Bf (t = − 2.23, p = 0.16)) (Table 5). The results obtained from the mixed model ANOVA revealed a significant improvement at post-test for participants in the EG as compared to CG for SK domain (F(1,178) = 106, p < 0.001, η2 = 0.89) (Fig. 3 and Table 5), on measures of FK (F(1,178) = 130, p < 0.001, η2 = 0.113) (Fig. 4 and Table 5), and in the Bf domain (F(1,178) = 57.2, p < 0.001, η2 = 0.060)) (Fig. 5 and Table 5). Further, the post-hoc tests revealed significant improvement in the scores of the three domains for EG (SK (t = − 22.34, p < 0.001), FK (t = − 18.57, p = 0.001), and Bf (t = − 12.75, p < 0.001)) and SK domain for CG (t = − 5.55, p < 0.001). There was no significant change in FK scores (t = − 0.88, p = 1.0) and Bf ratings (t = − 0.96, p = 1.0) for the CG.

Mean and SD of self-perceived knowledge ratings. Error bars represent standard deviation.

Mean and SD of factual knowledge scores. Error bars represent standard deviation.

Mean and SD of the belief ratings. Error bars represent standard deviation.
Discussion
The results of the present study indicate a significant increase in SK, FK, and Bf scores for the EG following the intervention. These findings align with earlier studies showing the effectiveness of educational interventions on cognitive health, including cognitive aging, dementia, and Alzheimer’s, among adolescents, middle-aged adults, and the elderly17,18,19,20.
The EG’s improvement in the SK domain suggests that participants perceived the educational intervention as enhancing their knowledge on cognitive health, mild cognitive impairment, and dementia. This is significant considering the general lack of understanding about dementia and its prevention among the public36,37,38. The key factors driving user acceptance of any health literacy videos are the informational value, relevance, and social connection it offers39. The EM used in this study is reported to be strategically designed to include dyadic interactions between characters, and relatable real-life examples depicting the importance of cognitive health and the signs of cognitive disorders31. In the present study, such strategic components likely influenced participants’ acceptance of the EM, contributing to the observed increase in SK scores. The increase in SK scores may indicate that participants perceived an improvement in their ability to comprehend and use information related to cognitive health following the EM, suggesting enhanced self-efficacy. Self-efficacy, or one’s belief in their capacity to action40, is a key factor influencing health behaviors41. Individuals with higher self-efficacy tend to be more likely to adhere to recommended self-care practices42. Thus, this enhanced SK score may aid in promoting cognitive well-being practices among the YAs. However, follow-up assessments to capture their practice patterns post-intervention may be necessary to confirm this. Future studies could focus on incorporating these follow-up assessments to better understand the long-term impact of the EM.
The increase in FK scores indicate enhanced understanding of cognitive functions, their significance in daily life, age-related cognitive changes, signs of impairment, risk factors for cognitive decline, and the importance of cognitive health across the lifespan. The increase in FK ratings could be attributed to the rich and holistic content about cognitive health included in the EM. The EM had been developed with an intention to promote cognitive health and prevent cognitive disorders. It emphasized key themes centered around significance of preserving cognitive function, assessing risk factors that could jeopardize cognitive health, evaluating one’s cognitive status in relation to established norms, and being cognizant of appropriate preventive measures to mitigate the risk of developing cognitive disorders in the future. The EM content has been reported to have high content validity as deemed by experts and general public representation31. The results of the present study further reinforce these reports. Moreover, creating a mental representation through multisensory experiences increases the likelihood that the information will be remembered and therefore, followed43. Thus, the multimedia format of the intervention that aided in participants comprehension and retention of the content could have also contributed to these results. To confirm this, further studies may be needed to compare the effects of EM with non-EM formats. The FK ratings are a testimony to the appropriateness and usefulness of the EM intervention in enhancing people’s knowledge about cognitive health. This enhancement in their FK may favorably influence their ‘need for cognition’, the propensity to engage in cognitively stimulating pursuits44. It could also facilitate the timely detection of cognitive impairments such as MCI and Dementia in themselves as well as in the older adults in their social circles. Furthermore, it may empower them to proactively address risk factors associated with cognitive health and make well-informed lifestyle decisions that could positively impact their cognitive functioning over the long term. Overall, this enhanced knowledge equips YAs with resources and motivation to maintain and enhance their cognitive well-being throughout their lifespan.
Bf ratings suggest that the intervention effectively motivated participants to seek cognitive assessments, adopt healthy cognitive lifestyles, and engage in cognitive training programs. The Health Belief Model45 suggests that one’s likelihood of engaging in healthy behaviors is based on their perceived susceptibility and severity of disease, as well as their perceived benefits and barriers to preventive actions. For example, people are more inclined to adopt cognitively healthy habits if they feel at risk of cognitive decline (perceived susceptibility), recognize the importance of cognitive skills for daily functioning, and understand the serious implications of cognitive disorders on overall health (perceived severity). Additionally, their cognitive practices are influenced by their beliefs about the effectiveness of preventive measures (perceived benefits). The Health Belief Model45 and HL Skills Framework36 indicate that health literacy can shape behavioral outcomes by influencing people’s motivations and beliefs about health. Notably, the educational materials used in the present study directly addressed the significance of cognitive health in daily life, relevant risk factors, symptoms of cognitive disorders, and various preventive strategies. Consequently, the increase in participants’ Bf ratings may be attributed to their enhanced cognitive health literacy, as reflected in their SK and FK scores.
The present study specifically was addressed for YA population as a positive influence on them could have optimistic effects on the society in the coming years26. Majority of the behaviors one practices are established in the young adulthood46 making it essential to educate YAs about the benefits of HL and lack thereof, as they are at a crucial stage of their lives where the behaviours established today will affect their decisions later in adulthood. Moreover, YAs are increasingly taking on more responsibility for making health-related decisions and acting as “primary caregivers” for themselves and their families47. Although theoretical knowledge alone may not inspire lifestyle changes or promote health, it may contribute in better understanding of how one’s choices impact their well-being48. Moreover, research has linked greater knowledge with greater interest and motivation to decrease the risk of cognitive disorders18,49,50. In this essence, the present attempt could be a small step towards fostering greater interest, motivation, and knowledge about cognitive health and well-being, which could potentially offer some relief to the alarming statistical predictions of cognitive disorders51,52. The rising demand for SLP services in cognitive-communicative health, coupled with the growing recognition of the crucial role SLPs can play in prevention and wellness efforts3, our present work highlights the value and utility of the EM resource that has been developed. This comprehensive and scientifically-grounded EM could serve as a valuable guiding tool and resource for SLPs as we work to promote cognitive health and well-being within our clinical practice and community-based initiatives.
Limitations and future directions
The present research primarily focused on immediate changes in knowledge and beliefs related to cognitive health following the EM and lacks assessment of changes in participant’s practice patterns concerning cognitive health. However, it is acknowledged that participants intentions may serve as influential factors in shaping their behavior53, offering a potential indication of their practice patterns. Future studies could directly explore its effect on enhancing self-efficacy and encouraging adoption of healthy cognitive practices by conducting a follow-up assessment through booster sessions and follow-up surveys. Further, as the study focused on core symptoms of dementia, signs such as hair loss and weight loss were not considered as symptoms during analysis, despite certain evidence suggesting their association with dementia. The assessment of factual knowledge regarding cognitive changes with aging broadly encompassed reasoning and memory. However, evidence on changes in these abilities is heterogeneous, with different types of reasoning and memory domains showing distinct trajectories. Future research should aim to assess domain-specific knowledge, such as memory for names, memory for faces, verbal reasoning, social reasoning, analogical reasoning, familiar reasoning, etc. With regard to the data collection method, the present study used a retrospective pre-post questionnaire, which may present certain challenges such as recall bias, overestimation of change, and lack of a clear baseline to gauge participants’ initial knowledge and attitude. Although these limitations were addressed by providing appropriate instructions to participants, future studies could consider incorporating this questionnaire at two different time points—before and after the educational multimedia. Also, designing custom, closely matched placebo videos for control groups may be an important methodological consideration for upcoming research. Further, as prior experience with any form of multimedia education may influence engagement and responsiveness to the intervention, screening for it could be considered in future iterations of the study. Research evaluating the efficacy of the EM across a broader range of demographics such as age, clinical conditions, and educational and linguistic backgrounds is warranted, particularly through the use of culturally and linguistically appropriate material.
Conclusions
The present research aimed to evaluate the efficacy of an EM intervention on YAs self-perceived knowledge, factual knowledge, and beliefs about cognitive health using a retrospective pre-post questionnaire. The results confirmed a significant improvement in all three domains among the EG compared to the CG, suggesting that the selected EM effectively enhanced YAs understanding and attitudes towards cognitive health. The EM used in the present study could serve to spread awareness about cognitive health, encourage the general population to take preventive measures, and promote early detection and intervention of cognitive health issues. Unlike traditional public health initiatives, EM can reach large and remote audiences with minimal recurring costs, making it a cost-effective tool for health promotion. Its flexibility and low training requirements also allow for seamless integration into routine health education, community outreach programs, and clinic waiting areas. The present research aligns with the growing responsibilities of SLPs in cognitive well-being, offering a tool that can be integrated into our ‘Counselling+’ services, a crucial aspect of our evolving professional role. Future studies could examine changes in participants’ behaviour and explore how multimedia can promote healthy cognitive practices while also considering more diverse demographics and linguistically suitable approaches.
Data availability
The data that supports the findings of this study are available from the authors upon reasonable request.
References
Nichols et al. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: an analysis for theGlobal Burden of Disease Study 2019. The Lancet Public Health 6, e105–e125 (2022).
ASHA. 2019 SLP Health Care Survey: Caseload Characteristics. (2019).
Lanzi, A. M., Ellison, J. M. & Cohen, M. L. The, “Counseling+” roles of the speech-language pathologist serving older adults with mild cognitive impairment and dementia from Alzheimer’s disease. Perspect. ASHA Spec. Interest Groups 6, 987–1002 (2021).
World Health Organization. Global Action Plan on the Public Health Response to Dementia 2017–2025 (2017).
NIH National Institute of Health National Institute on Aging. Cognitive Health and Older Adults. National Institute on Aging (2020).
Hickey, K. T. et al. Low health literacy. Nurse Pract. 43, 49–55 (2018).
Jia, Q., Wang, H., Wang, L. & Wang, Y. Association of health literacy with medication adherence mediated by cognitive function among the community-based elders with chronic disease in Beijing of China. Front. Public Health 10, (2022).
Liu, Y. B., Chen, Y. L., Xue, H. P. & Hou, P. Health literacy risk in older adults with and without mild cognitive impairment. Nurs. Res. 68, 433 (2019).
Geboers, B. et al. Health literacy among older adults is associated with their 10-years’ cognitive functioning and decline—The Doetinchem Cohort Study. BMC Geriatr. 18, 77 (2018).
Oliveira, D., Bosco, A. & di Lorito, C. Is poor health literacy a risk factor for dementia in older adults? Systematic literature review of prospective cohort studies. Maturitas 124, 8–14 (2019).
Nguyen, H. T. et al. Cognitive function is a risk for health literacy in older adults with diabetes. Diabetes Res. Clin. Pract. 101, 141–147 (2013).
Serper, M. et al. Health literacy, cognitive ability, and functional health status among older adults. Health Serv. Res. 49, 1249–1267 (2014).
Then, F. S. et al. Differential effects of enriched environment at work on cognitive decline in old age. Neurology 84, 2169–2176 (2015).
Lee, Y. & Chi, I. Do cognitive leisure activities really matter in the relationship between education and cognition? Evidence from the aging, demographics, and memory study (ADAMS). Aging Ment. Health 20, 252–261 (2016).
França, A. S. et al. Evaluating health literacy among adolescent and young adult pregnant women from a low-income area of Northeast Brazil. Int. J. Environ. Res. Public. Health 17, 8806 (2020).
Rudd, R. E. The evolving concept of Health literacy: New directions for health literacy studies. J. Commun. Healthc. 8, 7–9 (2015).
Aihara, Y. & Maeda, K. National dementia supporter programme in Japan. Dementia 20, 1723–1728 (2021).
Heger, I. et al. Dementia awareness and risk perception in middle-aged and older individuals: Baseline results of the MijnBreincoach survey on the association between lifestyle and brain health. BMC Public Health 19, 678 (2019).
Farina, M. P., Zhang, Y. S., Kim, J. K., Hayward, M. D. & Crimmins, E. M. Trends in dementia prevalence, incidence and mortality in the United States (2000–2016). J. Aging Health 34, 100–108 (2022).
Askari, N., Bilbrey, A. C., Ruiz, I. G., Gallagher-Thompson, D. & Humber, M. B. Dementia awareness campaign in the Latino community: A novel community engagement pilot training program with promotoras. Clin. Gerontol. 41, 200–208 (2018).
Mridula, J., George, V. M., Bajaj, G., Namratha, H. G. & Bhat, J. S. Effect of working memory training on cognitive communicative abilities among young- and middle-aged adults. Cogent Psychol. 4, 1416885 (2017).
Stern, Y. Cognitive reserve: implications for assessment and intervention. Folia Phoniatr. Logop. 65, 49–54 (2013).
Stern, Y. et al. Brain networks associated with cognitive reserve in healthy young and old adults. Cereb. Cortex. 1991(15), 394–402 (2005).
Paakkari, L. & Paakkari, O. Health literacy as a learning outcome in schools. Health Educ. 112, 133–152 (2012).
Ani Petrosyan. Internet and social media users in the world 2023. Statista https://www.statista.com/statistics/617136/digital-population-worldwide/ (2023).
Stassen, G., Grieben, C., Sauzet, O., Froböse, I. & Schaller, A. Health literacy promotion among young adults: A web-based intervention in German vocational schools. Health Educ. Res. 35, 87–98 (2020).
Greenlaw, C., Elhefnawy, Y., Jonas, R. & Douglass, L. M. Using an animated video to promote an informed discussion on SUDEP with adolescents. Epilepsy Behav. EB 122, 108182 (2021).
Vandormael, A. et al. The effect of a wordless, animated, social media video intervention on COVID-19 prevention: Online randomized controlled trial. JMIR Public Health Surveill. 7, e29060 (2021).
O’Mara, B. Social media, digital video and health promotion in a culturally and linguistically diverse Australia. Health Promot. Int. 28, 466–476 (2013).
Tanushree Basuroy. Internet usage in India. Statista https://www.statista.com/topics/1145/internet-usage-worldwide/ (2023).
Rooha, A. et al. Development and validation of educational multimedia to promote public health literacy about healthy cognitive aging. Health Expect. (2023).
Simpson, A Rae. Young Adult Development Project. (2018).
World Health Organisation Disability Assessment Schedule 2.0 – Interview (WHODAS-interview). NovoPsych https://novopsych.com.au/assessments/health/world-health-organisation-disability-assessment-schedule-2-0-interview-whodas-interview/ (2022).
Budin-Ljøsne, I. et al. The global brain health survey: development of a multi-language survey of public views on brain health. Front. Public Health 8, (2020).
Bhanji, F., Gottesman, R., de Grave, W., Steinert, Y. & Winer, L. R. The retrospective pre-post: A practical method to evaluate learning from an educational program. Acad. Emerg. Med. 19, 189–194 (2012).
Ansari, Z. et al. Validity and reliability of a questionnaire measuring knowledge, attitude, and practice regarding dementia among general population and healthcare workers in Urban India. Cureus 14, e28196 (2022).
O’Connor, D. World Alzheimer Report 2019: Attitudes to dementia. (2019).
Cations, M., Radisic, G., Crotty, M. & Laver, K. E. What does the general public understand about prevention and treatment of dementia? A systematic review of population-based surveys. PLoS ONE 13, e0196085 (2018).
Jamil, N. A. et al. Development and evaluation of an integrated diabetes-periodontitis nutrition and health education module. BMC Med. Educ. 21, 278 (2021).
Bandura A. (ed.) Self-Efficacy in Changing Societies. (Cambridge University Press, Cambridge, 1995). https://doi.org/10.1017/CBO9780511527692.
Bandura, A. Health promotion by social cognitive means. Health Educ. Behav. 31, 143–164 (2004).
Reisi, M. et al. Impact of health literacy, self-efficacy, and outcome expectations on adherence to self-care behaviors in Iranians with type 2 diabetes. Oman Med. J. 31, 52–59 (2016).
Campos, D. C. D. et al. Development and validation of an educational video to prevent falls in hospitalized children. Texto Contexto Enferm. 30, e20190238 (2021).
Rovner, B. W., Casten, R. J. & Leiby, B. E. Determinants of activity levels in African Americans with mild cognitive impairment. Alzheimer Dis. Assoc. Disord. 30, 41–46 (2016).
Andrulis, D. P. & Brach, C. Integrating literacy, culture, and language to improve health care quality for diverse populations. Am. J. Health Behav. 31, S122–S133 (2007).
Abel, T., Hofmann, K., Ackermann, S., Bucher, S. & Sakarya, S. Health literacy among young adults: A short survey tool for public health and health promotion research. Health Promot. Int. 30, (2014).
Sansom-Daly, U. M. et al. Health literacy in adolescents and young adults: An updated review. J. Adolesc. Young Adult Oncol. 5, 106–118 (2016).
Česnavičienė, J., Kalinkeviciene, A. & Ustilaite, S. Young adult health literacy on health promotion as social determinant of health: Challenges for health education practice in Lithuania. SHS Web Conf. 40, 02005 (2018).
Kim, S., Sargent-Cox, K. A. & Anstey, K. J. A qualitative study of older and middle-aged adults’ perception and attitudes towards dementia and dementia risk reduction. J. Adv. Nurs. 71, 1694–1703 (2015).
Smith, B. J., Ali, S. & Quach, H. The motivation and actions of Australians concerning brain health and dementia risk reduction. Health Promot. J. Aust. 26, 115–121 (2015).
Anstey, K. J. et al. Future directions for dementia risk reduction and prevention research: An international research network on dementia prevention consensus. J. Alzheimers Dis. 78, 3–12 (2020).
Wesselman, L. M. et al. Web-based multidomain lifestyle programs for brain health: Comprehensive overview and meta-analysis. JMIR Ment. Health 6, e12104 (2019).
Aubeeluck, A. Behaviour change for dementia prevention and risk reduction. in 117–130 (2018). https://doi.org/10.4324/9781351122719-9.
Acknowledgements
The study is supported by funding received from Department of Science and Technology (DST) under Cognitive Science Research Initiative (CSRI), Government of India (DST/CSRI/2018/29).
Funding
Open access funding provided by Manipal Academy of Higher Education, Manipal
Author information
Authors and Affiliations
Contributions
All authors (AR, SS, AS, NLJ, GB, VMG, JSB) were involved in Conceptualization and designing the Methodology of the research idea. AR, SS and NLJ carried out the Investigation. Formal analysis was done by AR, SS, AS, GB. Project administration and Resources were provided by GB, VMG and JSB. AR, SS, AS, and GB wrote the original draft. All authors (AR, SS, AS, NLJ, GB, VMG, JSB) were involved in validation and writing – review & editing of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shetty, S., Rooha, A., Soni, A. et al. Efficacy of an educational multimedia in promoting public health literacy on age-related cognitive-communicative health: a randomized controlled trial. Sci Rep 15, 32915 (2025). https://doi.org/10.1038/s41598-025-16857-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-16857-x
