
Abstract
Restricting cervical spine movement after a collision and reducing its initial impact may prevent serious spinal cord injuries. This study aimed to use computer simulations to compare the head and neck behavior and spinal cord loading patterns with and without a neck stabilizer. A computer-simulated human body model was used to investigate this neck behavior in three collision directions (frontal, rear, and lateral) using an adult male at the 50th and 95th percentiles and an adult female at the 5th percentile. The angles of motion in the sagittal and coronal planes were measured with and without the neck stabilizer. Following frontal collision with the head and neck, the anterior surface loads at the upper and middle cervical levels (C2 and C5) increased during head and neck extension, and the loads increased with increasing extension angle. The neck stabilizer restricted the head and neck within the normal range of motion even after a frontal or rear collision in the 50th and 95th percentile adult male and 5th percentile female models, respectively. Thus, neck stabilizers may be effective in reducing cervical spinal cord loading by restricting the movement of the head and neck during collisions in this simulation study.
Similar content being viewed by others

Introduction
Traumatic cervical spine injuries can damage the cervical spine and spinal cord, causing significant functional impairment, loss of sensation, and in some cases complete paralysis. Per a national survey by the Japan Medical Society of Spinal Cord Lesion, 4603 spinal cord injuries occurred in JAPAN in 20181. The estimated incidence of traumatic spinal cord injury, excluding Frankel E, is 49 per million, with a median age of 70 years. Cervical cord injuries accounted for 88.1% of cases. The primary causes of falls included falls on level surfaces (38.6%), traffic accidents (20.1%), falls from low places (13.7%), falls from high places (10.2%), falls downstairs (9.9%), and sports-related incidents (3.1%). The common causes of traffic accidents were four-wheeled vehicle accidents (46.3%), two-wheeled vehicle accidents (26.6%), and bicycle accidents (20.7%). The clinical outcomes of spinal cord injury depend on its severity and location. The 40-year survival rate of patients with spinal cord injury is 47% for quadriplegia and 62% for paraplegia2. The life expectancy of a patient with American Spinal Injury Association (ASIA) Impairment Scale grade D requiring a wheelchair for daily living is 75% of that of a healthy person, whereas the life expectancy of a patient not requiring a wheelchair or catheterization is approximately 90% of that of a healthy person2. Therefore, the prevention or reduction of spinal cord injury is paramount. Spinal cord injuries are due to sudden traumatic impacts that fractures or dislocates the spine. Recently, cases have emerged where the spinal cord was injured without bony injury. The initial mechanical force applied to the spinal cord at the time of injury is called the primary injury, in which “displaced bone fragments, disc materials, and/or ligaments bruise or tear the spinal cord tissue”3. Four main mechanisms of primary injury exist: (1) impact plus persistent compression, (2) impact alone with transient compression, (3) distraction, and (4) laceration/transection4. The most common primary injury is impact plus sustained compression, typically caused by a burst fracture or fracture-dislocation injury where a bone fragment compresses the spinal cord. Immediate immobilization of the cervical spine and reduction of the initial impact can help prevent severe spinal cord injury. Several studies have investigated the biomechanical mechanisms underlying traumatic cervical spinal cord injury. Finite element models and cadaveric experiments have demonstrated how rapid head acceleration, axial loading, and hyperflexion can cause spinal cord compression or shear deformation even in the absence of fractures. For example, Nightingale et al. and Yoganandan et al. used experimental and computational approaches to show that inertial forces and cervical kinematics play crucial roles in injury mechanisms5,6. Finite element modeling studies have also contributed to understanding how cervical stabilization devices may reduce mechanical load or displacement of the spinal cord during impact events7,8. Given the ethical and technical challenges of studying spinal cord injury mechanisms in vivo or through cadaveric impact experiments, computer-based finite element modeling offers a safe and reproducible method for analyzing biomechanical responses and spinal cord loading under various traumatic scenarios. Such simulations allow for detailed assessment of how external stabilization devices, such as neck collars, affect the dynamics of cervical motion and spinal cord loading during impact. This approach is particularly suitable for exploring conditions that are difficult to recreate experimentally, including subtle variations in impact angle, velocity, and restraint application. Therefore, in this study, we used computer simulations to evaluate head and neck motion and cervical spinal cord loading patterns during various types of collision. We also investigated how these parameters change when a neck stabilizer is applied to restrict motion during impact.
Results
Analysis of head and neck response following cervical frontal collision in a 50th percentile adult male model
The head and neck extension angles following frontal collision of the head and neck in a 50th percentile adult male model is demonstrated in Fig. 1A (Supplementary Video 1). The head and neck extension angles increased with time after the collision. During extension, the load on the anterior surface of the cervical spinal cord increased after the head and neck extension exceeded 30° at the C2 vertebral level, reaching 30 N at 50° of the extension. At the C5 level, the load on the anterior surface of the cervical spinal cord increased rapidly after the extension exceeded 50° and reached 30 N when the extension angle exceeded 60° (Fig. 1B). Conversely, in the load analysis of the posterior surface of the cervical spinal cord, the load increased after head and neck extension exceeded 30° at the C1 level, reaching 30 N at an extension of 40–50° (Fig. 1C).

Head and Neck Extension and Spinal Cord Loading Following Frontal Collision. Head and neck extension angles (A), anterior spinal cord load (B), and posterior spinal cord load (C) in a 50th percentile adult male model during frontal impact.
Analysis of head and neck response following rear-end collision in a 50th percentile adult male model
The head and neck flexion angles after the rear-end collision of the head and neck in a 50th percentile adult male model are shown in Fig. 2A (Supplementary Video 2). The flexion angles increased over time following the collision but decreased after 70 ms. During the flexion, the highest load was applied to the anterior surface of the cervical spinal cord at the C3 level (Fig. 2B). In the load analysis of the posterior surface of the cervical spinal cord, maximum load was applied to the C7 level (when the head and neck were flexed at 20°) and C3 level (when the head and neck were flexed at 50°) (Fig. 2C).

Head and Neck Flexion and Spinal Cord Loading Following Rear Collision. Head and neck flexion angles (A), anterior spinal cord load (B), and posterior spinal cord load (C) in a 50th percentile adult male model during rear impact.
Analysis of head and neck response following lateral collision in a 50th percentile adult male model
The head and neck lateral bending angles of the lateral collision of head and neck in 50th percentile adult male model are shown in Fig. 3A (Supplementary Video 3). The lateral bending angle increased over time from the collision side to the non-collision side but decreased after 70 ms (Fig. 3A). During the lateral bending, very little load was applied to the impacted side of the cervical spinal cord (Fig. 3B). In the load analysis of the non-collision side of the cervical spine, the greatest load was applied to the C2 level (when the head and neck were bent approximately 45° to the non-collision side) (Fig. 3C).

Head and Neck Lateral Bending and Spinal Cord Loading Following Lateral Collision. Lateral bending angles (A), spinal cord load on the impacted side (B), and non-impacted side (C) in a 50th percentile adult male model during lateral impact.
Comparison of head and neck range of motion and cervical spinal cord load with and without neck stabilizer in a 50th percentile adult male model
Following frontal collision of the head and neck in a 50th percentile adult male model, the range of motion was reduced by the neck stabilizer and was within the normal range of motion (Fig. 4A) (Supplementary Video 1). Following a rear collision of the head and neck in the 50th percentile adult male model, the range of motion was reduced by wearing the neck stabilizer and was within the normal range of motion (Fig. 4B) (Supplementary Video 2). The range of motion was reduced by the neck stabilizer after a lateral collision of the head and neck in the 50th percentile adult male model and was within the normal range of motion (Fig. 4C) (Supplementary Video 3).

Head and Neck Range of Motion With and Without Neck Stabilizer. Comparative analysis of head and neck motion with and without the neck stabilizer in frontal (A), rear (B), and lateral (C) collisions in a 50th percentile adult male model.
Comparison of head and neck range of motion with and without neck stabilizer in a 95th percentile adult male model
Following frontal collision of the head and neck in the 95th percentile adult male model, the range of motion was reduced by the neck stabilizer but still within the normal range of motion (Supplementary Fig.S1A). Following rear collision of the head and neck in the 95th percentile adult male model, the range of motion was slightly reduced by wearing the neck stabilizer but still within the normal range of motion (Supplementary Fig. S1B). The range of motion of the head and neck was reduced by the neck stabilizer following a lateral collision of the head and neck in the 95th percentile adult male model and was within the normal range of motion (Supplementary Fig. S1C).
Comparison of head and neck range of motion with and without neck stabilizer in a 5th percentile adult female model
Following frontal collision of the head and neck in a 5th percentile adult female model, the range of motion was reduced by the neck stabilizer but was within the normal range of motion (Supplementary Fig. S1A). Similarly, after rear collision of the head and neck in the 5th percentile adult female model, the range of motion was slightly reduced by wearing the neck stabilizer and was within the normal range of motion (Supplementary Fig. S1B). The range of motion of the head and neck was reduced by the neck stabilizer after a lateral collision of the head and neck in a 5th percentile adult female model and was within the normal range of motion (Supplementary Fig. S1C).
Comparative analysis across anthropometric models
To evaluate the influence of anthropometric factors on cervical biomechanics, we compared cervical motion and spinal cord loading in the 50th percentile male, 95th percentile male, and 5th percentile female models. The 5th percentile female model exhibited greater cervical motion, with extension angles exceeding 70° and higher spinal cord loads during frontal impact. During rear-end collisions, this model also demonstrated increased cervical motion, with flexion angles exceeding 50 degrees. These findings highlight the impact of body size on cervical kinematics and support the need for adaptive stabilization strategies tailored to individual anthropometric characteristics.
Discussion
This study analyzed the effect of neck stabilizers on head and neck range of motion and cervical spinal cord load during cervical injury using THUMS version 6.1. The test conditions were set with reference to the JIS helmet drop test (JIS T 8133). In our literature review, we found no standardized biomechanical testing protocols specifically designed to evaluate cervical spinal cord loading from direct head impacts simulating ground contact during real-world falls or crashes. Therefore, we adopted the helmet drop test protocol as a reference, as it provides a reproducible head impact condition that could approximate such scenarios and allow for controlled comparison of cervical loading across different impact directions. The head and neck collision model for 50th percentile adult males in THUMS version 6.1 was validated for its behavior by multiple dynamic sled and loading tests using cadavers and volunteers9,10,11,12. To evaluate the biomechanical effectiveness of the neck stabilizer, we compared cervical motion across three anthropometric models—50th and 95th percentile adult males and a 5th percentile adult female—under stabilized and unstabilized conditions in three collision directions. Following frontal impact, head and neck extension angles progressively increased, often exceeding the normal physiological range in the absence of a stabilizer. In contrast, the application of a neck stabilizer effectively limited extension to within 50°, the established physiological threshold, in all models. This effect was particularly pronounced in the 5th percentile female model, which demonstrated the greatest extension in the unstabilized state.
In rear-end collisions, flexion angles remained within the 60° physiological limit across all models, regardless of stabilization. However, in lateral collisions, lateral bending exceeded 50° in the 5th percentile female model without stabilization, while the neck stabilizer successfully restricted motion within the normal range.
These findings highlight the potential value of neck stabilizers in reducing harmful mechanical responses by constraining cervical motion. Although the protective effect varied depending on impact direction and body size, the ability of the stabilizer to maintain physiological motion ranges may help mitigate the risk of cervical fractures, intervertebral dislocations, and ligamentous injuries. Given that the initial mechanical insult is a key determinant of neurological outcome in spinal cord injury2, limiting excessive cervical motion may offer clinically meaningful benefits. Although this study did not directly quantify internal spinal cord stress or strain, cervical angular motion was used as a practical surrogate for mechanical loading. Prior research suggests that excessive motion is closely linked to increased risk of spinal cord injury due to mechanical deformation, such as compression or elongation13,14. Therefore, the observed reductions in cervical range of motion with the neck stabilizer may reflect meaningful reductions in injury risk, particularly in vulnerable populations such as smaller-statured individuals.
This study, while providing valuable insights into the biomechanical effects of neck stabilizers, has certain limitations. Firstly, the study relied on computer simulations using the THUMS human body model, which involves inherent assumptions and simplifications of complex biological systems. The accuracy of the simulations depends on the fidelity of the model and the input parameters used. Secondly, the study focused on a limited number of collision scenarios and anthropometric variations. In addition, there is currently a lack of validated experimental models that replicate cervical spinal cord loading due to direct cranial impact with the ground surface in real-world accidents. The adoption of a helmet drop impact model was intended to approximate such a mechanism, although it does not fully capture the complex inertial forces acting on the neck. Future work should explore more physiologically representative loading protocols to further validate our finding. Further research is needed to investigate the effectiveness of neck stabilizers in a wider range of real-world scenarios and across a broader population. Finally, the study did not directly assess the clinical impact of neck stabilizer use in preventing or mitigating spinal cord injury in human subjects. Although clinical research is necessary to verify the findings of this computer research, it is difficult to carry out. In addition, while we used standard physiological ranges of motion (60° flexion, 50° extension, and 50° lateral bending) based on guidelines from the Japanese Orthopaedic Association, these values are not stratified by body size or sex. Specific normative data for cervical range of motion in 50th or 95th percentile adult males or 5th percentile females are not widely available. Therefore, the same thresholds were applied across all anthropometric models in this study, which may not fully account for individual biomechanical variability. Moreover, this study did not differentiate between upper and lower cervical spine motion during analysis. Given that real-world injury mechanisms can vary significantly between these regions—such as hyperextension-related injuries being more common in the upper cervical spine and axial compression injuries in the lower segments—future studies should incorporate segment-specific assessments to better capture clinically relevant motion patterns and injury risks15,16.
In conclusion, we analyzed head and neck motion and estimated cervical spinal cord loading patterns following collisions using a human body simulation. The use of a neck stabilizer was associated with a reduction in excessive cervical motion, particularly in smaller anthropometric models, suggesting its biomechanical utility in limiting cervical movement after impact. While this study did not directly assess clinical outcomes such as fractures or ligament injuries, the findings support further investigation into the stabilizer’s role in mechanical injury prevention.
Methods
Computer simulation
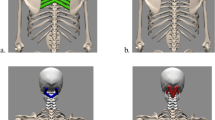
In this study, the computer-simulated human body models—the total human body model for safety (THUMS), were used to investigate the neck’s behavior in three collision directions (frontal, rear, and lateral) using LS-DYNA (Fig. 5A, B)17. The THUMS (version 6.1), developed by Toyota Motor Corporation (Toyota, Aichi, Japan), was used12. Three THUMS models were used: an adult male at the 50th and 95th percentiles and an adult female at the 5th percentile. LS-DYNA SMP971 R11.2.2 (Ansys, Livermore, CA, USA) was used to perform the crash (dynamic loading) simulations. LS-DYNA is a general-purpose multiphysics simulation software package that includes a nonlinear explicit finite element solver. The neck’s angles of motion in the sagittal and coronal planes and the anterior and posterior loads on the cervical spinal cord at each vertebral body level were measured (Fig. 6A–C). The neck angles were defined as the angle between a line connecting the center of the head to C7 and a vertical reference line. This method was applied in both the sagittal and coronal planes to represent gross cervical motion. This approach accounts for curvature and flexibility of the cervical spine and allowed for consistent comparison of head–neck motion across different collision directions (Fig. 6A, B). The loads were obtained as reaction forces from the finite element model, extracted directly from LS-DYNA at the contact interfaces between the spinal cord and adjacent anatomical structures. In the lateral impact scenario, spinal cord loading was evaluated separately on the collision (ipsilateral) and non-collision (contralateral) sides. This distinction was made to capture potential asymmetries in spinal cord loading distribution resulting from lateral bending and directional impact forces. To replicate a physiologically realistic posture during impact, the upper surface of the T7 vertebral body and the structures below were restrained by applying fixed boundary conditions. These constraints restricted both translational and rotational movement of the torso, simulating a stabilized seated or standing posture. This setup allowed for isolated evaluation of head and neck motion and spinal cord loading in response to external impact.

Head and Neck Behavior During Simulated Collisions. Impactor approach direction and head–neck response during frontal and rear (A) and lateral (B) collisions.

Head and Neck Motion and Spinal Cord Loading. Sagittal (A) and coronal (B) plane motion, and cervical spinal cord loading (C) as assessed in simulation.
Test conditions
In this study, test conditions were set with reference to the drop weight test specified in JIS T 8133, a Japanese helmet safety standard. Based on our review of the literature and available protocols, no standardized experimental or simulation methods were identified that directly evaluate cervical spinal cord loading due to cranial impact with the ground surface during real-world falls or crashes. Therefore, we adopted the helmet impact protocol as a reproducible and directionally applicable loading condition to approximate such scenarios. An impactor with a mass of 4.7 kg and a velocity of 5.42 m/s was used to apply an impact to the head, and cervical motion and spinal cord loading after frontal and lateral collisions were evaluated. In each collision scenario, the impactor was positioned in alignment with the intended direction of impact. For frontal collisions, it advanced from the front and contacted the forehead. For rear collisions, the impactor moved forward from behind the head and struck the occipital region. In lateral collisions, the impactor approached from the side and impacted the temporal region. In all cases, the impact direction was perpendicular to the cranial surface to ensure consistent loading conditions across simulations (Fig. 5A, B). Regarding the direction of rear-end collision, under the above conditions, the speed was increased (5.42 [m/s] → 7.67 [m/s]) to evaluate the load on the cervical spinal cord when neck flexion exceeds the normal range of motion. This condition was selected to reproduce a cervical flexion angle greater than 60°, which is defined as the upper limit of physiological range in the sagittal plane by the Japanese Orthopaedic Association. Our aim was not to simulate a real-world crash velocity but to investigate the biomechanical response of the cervical spine and spinal cord under excessive flexion, which is relevant for understanding injury mechanisms in high biomechanical loding scenarios.
Analysis with neck stabilizer
A computer-simulated head and neck model was worn with a neck stabilizer, and the angles of the head and neck movement in the sagittal and coronal planes were measured for the three collision directions (
Fig. 7A, B). The stabilizer was modeled with an inner diameter of 138 mm, outer diameter of 298 mm, and a volume of 2524 cm3. The material was polyamide 66 (PA66), with a Young’s modulus of 7000 MPa and an internal pressure setting of 40 kPa. To simulate its biomechanical behavior, the stabilizer was modeled as a pressure-influenced elastic structure, rather than a rigid body. This configuration allowed for partial deformation under load, reflecting the compliant nature of the real device. The design and material properties of the modeled stabilizer were based on an actual clinically used device, providing anatomical conformity and mechanical behavior consistent with real-world applications. The same stabilizer model was used across all three anthropometric THUMS models (50th and 95th percentile male, 5th percentile female), with minor adjustments in positioning to ensure a proper fit. To account for anthropometric differences such as neck length and body size, the fitting of the neck stabilizer was adjusted for each model, and the resulting differences in positioning were visualized and are presented in Supplementary Fig. S1. The stabilizer contacted the mandible, occiput, scapular region, and anterior chest wall, thereby extending from the head down to the upper thoracic area. Regarding the test conditions, an impactor with a mass of 4.7 kg and a velocity of 5.42 m/s was made to collide with the head of an adult male at the 50th percentile and 95th percentile, and an impactor with a mass of 3.1 kg and a velocity of 5.42 m/s was made to collide with the head of an adult female at the 5th percentile. The impactor mass of 3.1 kg was selected to reflect the smaller body size and weight of the 5th percentile female model, in proportion to the standard 4.7 kg used for male models. This same 3.1 kg impactor was applied in both the stabilizer and non-stabilizer conditions to ensure consistent loading and enable comparative analysis. The behavior after the collision was observed for three different types of collision.

Head and Neck Motion with Neck Stabilizer During Collisions Head and neck kinematics during rear (A) and lateral (B) collisions with the neck stabilizer in place.
Normal range of motion of the head and neck
The normal range of motion of the head and neck in the human body is defined by the Japanese Orthopedic Association as 60° flexion and 50° extension in the sagittal plane18. In the coronal plane, the right and left lateral bending angles were 50°. These values are based on clinical measurements of voluntary active motion in healthy adults and represent physiological motion limits under non-loaded conditions, without external impact or mechanical constraint.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Miyakoshi, N. et al. A nationwide survey on the incidence and characteristics of traumatic spinal cord injury in Japan in 2018. Spinal Cord 59, 626–634. https://doi.org/10.1038/s41393-020-00533-0 (2021).
Middleton, J. W. et al. Life expectancy after spinal cord injury: A 50-year study. Spinal Cord 50, 803–811. https://doi.org/10.1038/sc.2012.55 (2012).
Alizadeh, A., Dyck, S. M. & Karimi-Abdolrezaee, S. Traumatic spinal cord injury: An overview of pathophysiology, models and acute injury mechanisms. Front Neurol 10, 282. https://doi.org/10.3389/fneur.2019.00282 (2019).
Rowland, J. W., Hawryluk, G. W., Kwon, B. & Fehlings, M. G. Current status of acute spinal cord injury pathophysiology and emerging therapies: Promise on the horizon. Neurosurg Focus 25, E2. https://doi.org/10.3171/foc.2008.25.11.E2 (2008).
Nightingale, R. W., Camacho, D. L., Armstrong, A. J., Robinette, J. J. & Myers, B. S. Inertial properties and loading rates affect buckling modes and injury mechanisms in the cervical spine. J. Biomech. 33, 191–197. https://doi.org/10.1016/s0021-9290(99)00156-6 (2000).
Yoganandan, N., Kumaresan, S. & Pintar, F. A. Biomechanics of the cervical spine Part 2. Cervical spine soft tissue responses and biomechanical modeling. Clin Biomech (Bristol) 16, 1–27. https://doi.org/10.1016/s0268-0033(00)00074-7 (2001).
Babu, R. D. & Veezhinathan, M. Design and development of a 3D printable neck brace: A finite element approach. J Clin Diagn Res 16, PC10–PC15. https://doi.org/10.7860/JCDR/2022/57066.16975 (2022).
Farajzadeh Khosroshahi, S., Mazdak, G. & Galvanetto, U. Assessment of the protective performance of neck braces for motorcycle riders: A finite-element study. Int J Crashworthiness 24, 487–498. https://doi.org/10.1080/13588265.2018.147893 (2019).
Ono, K., Kaneoka, K., Wittek, A. & Kajzer, J. Cervical injury mechanism based on the analysis of human cervical vertebral motion and head-neck-torso kinematics during low speed rear impacts. SAE Trans. 106, 339–356 (1997).
White, N. et al. Investigation of upper body and cervical spine kinematics of post mortem human subjects (PMHS) during low-speed rear-end impacts. SAE Tech Papers https://doi.org/10.4271/2009-01-0387 (2009).
Wismans, J., Philippens, M., van Oorschot, E., Kallieris, D. & Mattern, R. Comparison of human volunteer and cadaver head-neck response in frontal flexion. SAE Trans. 96, 1323–1335 (1987).
Total HUman Model for Safety: https://www.toyota.co.jp/thums/. Accessed October 18, 2024.
Nightingale, R. W., McElhaney, J. H., Richardson, W. J., Best, T. M. & Myers, B. S. Experimental impact injury to the cervical spine: relating motion of the head and the mechanism of injury. J Bone Joint Surg Am 78, 412–421. https://doi.org/10.2106/00004623-199603000-00013 (1996).
Nightingale, R. W., McElhaney, J. H., Richardson, W. J. & Myers, B. S. Dynamic responses of the head and cervical spine to axial impact loading. J. Biomech. 29, 307–318. https://doi.org/10.1016/0021-9290(95)00056-9 (1996).
Carter, D. R. & Frankel, V. H. Biomechanics of hyperextension injuries to the cervical spine in football. Am. J. Sports Med. 8, 302–309. https://doi.org/10.1177/036354658000800502 (1980).
Ivancic, P. C. Cervical spine instability following axial compression injury: A biomechanical study. Orthop Traumatol, Surg Res: OTSR 100, 127–133. https://doi.org/10.1016/j.otsr.2013.10.015 (2014).
Kimpara, H. et al. Investigation of anteroposterior head-neck responses during severe frontal impacts using a brain-spinal cord complex FE model. Stapp Car Crash J 50, 509–544. https://doi.org/10.4271/2006-22-0019 (2006).
Kubo, T., Nakashima, Y. & Tanaka, Y. Regarding the revised method for displaying and measuring joint range of motion(revised April 2022) (in Japanesse). Jpn J Rehabil Med 58, 1188–1200 (2021).
Acknowledgements
We would like to thank Editage for English language editing.
Funding
This study was supported by Daicel Corporation.
Author information
Authors and Affiliations
Contributions
HA and KI designed the study; KI, MY, TY and YH acquired the data.; HA and KI designed the study; KI, MY, TY and YH acquired the data.; HA, KI, MY, TY and YH analyzed the data; All authors interpreted the data; HA and KI drafted the manuscript; All authors revised it critically; YM supervised the analysis. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
HA, TH, and YM were received research funds from Daicel Corporation in support of this work. HA, TH, and YM were received research funds from Daicel Corporation in support of this work. TH received donated laboratory funding from Medtronic Sofamor Danek Inc. (Memphis, TN, USA), Japan Medical Dynamic Marketing Inc. (Tokyo, Japan), and Meitoku Medical Institute Jyuzen Memorial Hospital (Hamamatsu, Japan). KI, MY, TU, and YH are employees of Daicel corporation.
Ethics approval
This study does not require ethical review.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Supplementary Video 1.
Supplementary Video 2.
Supplementary Video 3.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Arima, H., Hasegawa, T., Imoto, K. et al. Clinical efficacy of neck stabilizer for cervical spine injury. Sci Rep 15, 32888 (2025). https://doi.org/10.1038/s41598-025-16984-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-16984-5
