
Abstract
Malaria and soil-transmitted helminths (STHs) infections continue to be public health burden in Cameroon. This study investigates the prevalence, severity and impact of Malaria and soil-transmitted helminth infections on haemoglobin levels among armed forces in the North West and South West Regions of Cameroon. This cross-sectional study enrolled 812 male participants in the military camps of the North West and South West regions of Cameroon. Questionnaire survey was used to document participants demographic and clinical data. Venous blood was collected and used for testing malaria parasitaemia by microscopy as well as measurement of haemoglobin (Hb) levels using an Hb metre. Also, the direct smear method and Kato-Katz technique were used to detect intestinal parasites amongst the participants. The study identified two Plasmodium species, Plasmodium falciparum and Plasmodium vivax, with an overall prevalence of 13.6%. Equally, Loa loa microfilaria was identified during the study with a prevalence of 0.2% (2/812). Five intestinal helminthic species were also identified, including Ascaris lumbricoides, Trichuris trichiura, hookworms, Schistosoma mansoni, and Schistosoma intercalatum. Two intestinal protozoan species, Entamoebacoli and Entamoeba histolytica were recorded. The overall prevalence of intestinal parasites was 22.8%. Plasmodium falciparum was the most prevalent parasite with 86.6% of infected participants having mild malaria. The parasitic density was significant across age groups. Malaria parasites, Trichuris trichiura and Schistosoma mansoni significantly affected the mean Hb concentration level. Malaria and intestinal helminths remain public health issues in Cameroon, affecting haemoglobin levels. Asymptomatic malaria and intestinal helminthic carriers are transmission agents, necessitating government consideration to eradicate or limit transmission rates.
Similar content being viewed by others

Introduction
Health encompasses complete physical, mental, and social well-being1, which is often compromised by common diseases like malaria, soil-transmitted helminthiasis, and bacterial viruses2. Malaria has significantly impacted wars throughout history, causing significant morbidity and mortality in conflict zones3. Despite its historical impact, malaria continues to play a significant role in warfare outcomes and public health, particularly in areas of the Global South, where it is endemic and has been a significant factor in brutal conflicts3. Also, Helminth infections caused by parasitic worms can cause chronic symptoms and serious clinical outcomes4. Military personnel frequently carryout peace keeping activities in helminth-endemic regions, but screenings for these infections and comprehensive surveillance studies are never carried out4. These infections affect haemoglobin levels and increase the risk of iron deficiency anaemia among co-infected individuals5. The major effect of infection with malaria parasites and helminths is anaemia, which is a significant health concern in sub-Saharan Africa6.
Haemoglobin levels are influenced by malaria and soil-transmitted helminthic infections, which can cause pathological effects in humans7. Fluctuating levels are believed to vary among asymptomatic adults with these parasites8. Haemoglobin concentration is a reliable indicator of anaemia at the population level9. In developing countries, anaemia is considered a public health problem when the haemoglobin value is below the Hb threshold. Anaemia is a major complication of neglected tropical diseases, such as soil-transmitted helminths10. In Africa, anaemia prevalence ranges from 64.3 to 71%9, and in the Mount Cameroon area, it ranges from 19.8 to 44.2%10.
Therefore, this study aimed to determine the prevalence, severityand impact of Malaria and helminthic infections on Haemoglobin levels among the armed forces in the North and South West regions of Cameroon.
Materials and methods
Ethics statement
Ethical clearance was obtained from the Bamenda University Ethical Review Board (2022/0786H/Uba/IRB) and administrative authorizations were gotten from the North West and South West Regional Delegations of Public Health (R11/MPH/SWR/RDPH/PS/680/520) and the Minister of Defence (06068/DV/MINDEF/024/4). All methods were performed in accordance with the relevant guidelines and regulations of the ethical review board. Participants were informed about the study’s purpose and aim through an information sheet written in English and French, and all collected information remained confidential. Blood and stool samples were collected after participants provided written informed consent. Results were made known to participants, and positive subjects were referred to medical doctors for proper management and treatment. Participants were also educated on preventive treatments and self-protection from intestinal helminths and malaria.
Study area
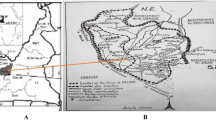
This study was military-based conducted in the North West and South West regions of Cameroon, focusing on the Legions, Air Force Military Units, Rapid Intervention Units, and amphibians military base Tiko. The North West Region has a surface area of 17,910 km² and an estimated population of 2 million, while the South West Region has a surface area of 25.410 km2 and a population of 1.153.125. The study was conducted in various units, such as Bafut, Buea, Limbe, Idenao, and Tiko, due to participants being redeployed to different divisions and sub-divisions (Fig. 1).
Bamenda is located between longitude 5°56’ N and latitude 10°10’E, with a cosmopolitan population of 393, 835 inhabitants and a surface area of 22.9 Km2. It is characterized by cold, tropical climatic conditions, with an annual rainfall of about 2,145 mm and an annual temperature range of 16°C–25°C. Bafut Sub-division is located between latitude 06º05΄–06º11΄N and longitude 09º58΄–10º11́E, and covers an area of roughly 340 km211. Buea, located at an elevation of 1000 m above sea level on the south-eastern slopes of Mount Cameroon, has an estimated population of over 176,000. Limbe, located between longitude 4°01′N and latitude 9°13′E, has a population of approximately 120,000 and a surface area of 545 km212. Tiko, located between Latitude 40 07’ N and 4030’N of the Equator and Longitude 9021’ 36’’ E and 90 36’ East of the Greenwich Meridian, has a surface area of 484 km2 and a population of 134,649 inhabitants13. The North West and South West Regions of Cameroon fall in the large equatorial forest, where malaria and soil-transmitted helminthic parasites transmission are high and perennial7,14.

Map of North West and South West regions of Cameroon adapted from open-source web image.
Study design, study population, and selection criteria
This cross-sectional study was conducted in military camps in the North West and South West regions of Cameroon from May 2023 to April 2024. The sample size was calculated using the formula n = Z2 P [1-P]/D215, Where D = Margin of error between the sample and the population (5%), n = Sample size, Z = 95% confidence interval (1.96 at 95% confidence interval), P = Prevalence based on previous study. P = 50% since the prevalence was unknown in the calculation16. The minimum sample size was determined and adjusted by 11%. as described by Cochran15.
N= (1.96)2 × 0.5 (10.5) ÷ (0.05)2 =384.
N = 384 + 384 = 768.
A total of 812 male participants were recruited, which included only Armed Forces returning from an operational service, who had not taken anthelminthic or antimalaria drugs, and who consented to participate. Participants who could not provide stool or blood samples were excluded.
Questionnaire administration
The ages of the participants; their duration in the intervention zones, the use of mosquito bed nets, malaria and intestinal helminth history and their life styles during the interventions were collected using a well-structured questionnaire.
Clinical assessment
Every participant’s axillary temperature was measured using a digital thermometer and pyretic status was defined as body temperature exceeding 37.5 °C17.
Blood sample collection and laboratory analysis
Venous blood (3mL) was collected from each study participant into Ethylenediaminetetra-acetic (EDTA) tubes using standard procedures. Participants’ haemoglobin (Hb) concentration was determined using the URIT-12 Hb meter (URIT Medical Electronic co., Ltd, London, United Kingdom). The displayed Hb value on the meter was documented to the nearest 0.1 g/dL. Anaemia status was defined by Hb < 11 g/dL of blood19 and was further classified as mild (Hb 10–10.9 g/dL), moderate (Hb 7–9.9 g/dL) and severe (Hb < 7 g/dL)20.
Malaria parasite detection
Both thick and thin films were prepared on well labelled grease-free slides for the identification of malaria parasites. Thin blood smears were fixed for 10 s using methanol after which, both blood films were stained with 10% Giemsa for 10 min20. The slides were then washed, air dried, and observed under the oil immersion objective (x100) of a light microscope. The WHO’s bench aid was used to identify malaria parasites19. Thin films were used for identifying malaria parasitic species, while thick films were used to quantify parasite density/µL of blood. Parasitic density was calculated by counting asexual parasite stages (trophozoites) against 200 leukocytes, assuming a total White Blood Cell count of 8000 leukocytes/µL of blood. Slides with no asexual or sexual stages were reported as negative. Parasite densities were classified as mild (MP < 1 000 parasites/µL), moderate (MP 1 000–4 999 parasites/µL) and severe (MP ≥ 5 000 parasites/µL)19,20.
Stool collection and processing
Each study respondent provided stool in a well labelled clean, dry, leak-proof container for the diagnosis of intestinal helminth infections using the direct smear method first followed by the Kato-Katz technique. For the Kato-Katz diagnostic procedure, a fine mesh was used to sieve the stool samples from which approximately 41.7 mg was collected and used to fill the hole of a template placed on a microscope slide. The template was later removed from the slide and the stool sample covered with cellophane soaked in glycerol. Next, the slide was inverted and gently pressed down to form a smear. The glycerol on the piece of cellophane serves to clear faecal material around helminth eggs. The slides were then examined under a light microscope within an hour of preparation to avoid missing the hookworm eggs.
Data analysis
Data collected from the field was entered in Excel spreadsheet then exported and analysed using the Statistical Package for Social Scientists (SPSS) version 16. Mean differences between groups for normally distributed variables were assessed using the student t-test and One-Way ANOVA (analysis of variance).Multiple comparisons within groups were computed using the Tukey Multi comparison Test. The binary logistic regression was used to assess the level of association between variables. The malaria parasite density and helminth egg count in co-infected samples were log-transformed in base 10. The cut-off points for assessing all statistical significance between groups was set at a probability level of (p) ≤ 0.05.
Results
Socio-demographic characteristics of the study population
In this study, a total of 812 participants were recruited all of single-sex (males) which were sub-divided into three3 age groups. The age group with the highest number of participants was the 18−30years age group (425/812; 52.3%) while those of the 41−50 years age group had the least number of participants (147/812; 18.1%). In addition, the participants’ marital status was taken into consideration of which 54.2% (440/812) were married and 45.8% (372/812) were single as shown on Table 1.
Prevalence of parasitic infections among the study group
According to Table 2, Out of the 812 participants, the prevalence of Plasmodium falciparum, was observed to be 11.9% (97/812) while Plasmodium vivax prevalence was 1.7% (14/812). The overall prevalence of malaria obtained from the study was 13.7% (111/812). Equally, Loa loa microfilaria was identified during the study with a prevalence of 0.2% (2/812). Five5 different species of intestinal helminths were identified which included Ascaris lumbricoides, Trichuris trichiura, Hookworms, Schistosoma mansoni, and Schistosoma intercalatum,of which Ascaris lumbricoides was most prevalent (4.7%; 38/812) and the least prevalent species was Schistosoma intercalatum (1.2%; 10/812) as indicated in Table 2. In addition, two2 species of intestinal protozoa were recorded, with Entamoeba coli having a prevalence of 6.8% (55/812) and Entamoeba histolytica with a prevalence of 4.1% (33/812). The overall prevalence of intestinal parasites was 22.8% (185/812).
Prevalence of the different parasitic species based on age group
According to Table 3, age group prevalence showed that the 31–40 years age group had the highest prevalence of prevalence P. falciparum (13.3%; 32/240) while the least prevalence of 0.4% (1/240) observed for S. intercalatum was found in the same age group. However, none of the results was statistically significant at p < 0.05%.
Prevalence of parasitic infections based on marital status
Table 4 shows that, participants who were not married had the highest prevalence of P. falciparum (12.4%; 46/372) while the least prevalence of 0.8% (3/372) was observed for S. intercalatum was found in the same marital status. However, infected participants to S. mansoni were statistically significant (p = 0.040).
Prevalence of the parasitic infections based on the severity in the study group
We observed in Table 5 that, out of the 97 participants who were positive forPlasmodium falciparum, 86.6% (84/970) had mild (MP < 1000 parasite/µL) malaria while 13.4% (13/97) had moderate (MP 1000–4 999 parasite/µL). Nevertheless, the severity of the other parasitic infections was mild (100%)as reported in Table 5.
Parasite densities of different parasite species for age groups and marital status
A non-parametric analysis using Kruskal Wallis test between age groups (Table 6) showed that, the parasitic density for Plasmodium falciparum was statistically significant (p = 0.019) across the age groups.Nonetheless, no statistical significance was observed in the parasitic densities for marital status (Table 7).
Haemoglobin concentration variation based on malaria parasite infection
The Haemoglobin concentrations were log-transformed in base 10 and malaria parasites had a highly significant impact (F = 49.866, p = 0.000) on the mean Haemoglobin concentration in infected patients see Table 8. Also, the student t-test was used to assess the mean difference in means at 95% C.I with equal variances in mean reported in Table 8 that, the mean Haemoglobin concentration levels were lower and statistically significant both in P. falciparum and P. vivax (p = 0.000). The Haemoglobin concentration level for P. falciparum-positive infected participants was 10.76 ± 1.29 g/dL and that of P. vivax was 11.06 ± 2.32 g/dL as compared to non-infected participants.
Haemoglobin concentration level variation based on intestinal helminths infection
The Haemoglobin concentrations were log-transformed in base 10 and intestinal helminths had a highly significant impact (F = 49.866, p = 0.000) on the mean Haemoglobin concentration in infected patients see Table 9. The student t-test mean Haemoglobin concentration level was statistically significant p = 0.017 for participants positively infected with T. trichiura(14.08 ± 3.54 g/dL). In addition, the mean concentration haemoglobin level of S. mansoni was statistically significant (p = 0.037) lower than those negatively infected withS. mansoni.
Discussion
Parasitic diseases, particularly intestinal parasites and malaria, are a significant public health concern in developing countries, particularly in Sub-Saharan Africa. People of all ages are susceptible to infection, with HIV-positive individuals, pregnant women, and children under five years having a higher burden21.This study was a community-based cross-sectional study conducted among the Armed Forces of the North West and South West of Cameroon, aimed to determine the impact of Malaria and Soil-Transmitted Helminths on haemoglobin concentration levels.
The study found a 13.7% malaria prevalence, higher than Gontie et al.22. 10.2% in west Ethiopia. This difference may be due to the study population’s frequent intervention in bushes and areas endemic to malaria vectors. Participants often lack mosquito repellents or bed nets, making it possible that only one infected person could transmit the disease to the entire group.
However, the prevalence was lower than that investigated along the slope of Mount Cameroon in the South West Region (33.8%)23 and in the North West region of Cameroon (34.7%)7. This could be due to the study being community-based rather than hospital-based, and the asymptomatic carriers in these communities could significantly contribute to the transmission of the parasite. Variations in prevalence could be attributed to weather conditions, intervention measures, environmental or behavioral risk factors, and the different study periods, target populations, and methodologies used24,25.
Intestinal parasitic infections continue to pose a global health concern, particularly for children, pregnant women, and immune-depressed people but they equally affect other people residing in endemic and low-income nations due to factors such as poverty, low literacy rates, inadequate hygiene, and malnourishment.
The overall prevalence of intestinal parasites was 21.4% higher than that obtained by Peter et al.26 and also higher than that observed amongst outpatients attending two public hospitals (17.6%) in Bamenda, North West Cameroon6.The study reveals that the higher prevalence of intestinal parasites among the population is due to the constant movement of the population, which often faces food and drinking water shortages during deployments. Participants often use unclean water and roadside foods, and the most available toilet facility is the bush, making it possible for one infected participant to reinfect the entire battalion. The risk factors assessed in the study include poor drinking water sources, hygienic practices, fecal disposal systems, socioeconomic status, and wide variations of parasites within human communities. However this prevalence was lower than that observed by Lindrose et al.4.
In this study, Ascaris lumbricoides was most prevalent (4.7%) and the least prevalent species was Schistosoma intercalatum (1.2%). This is in agreement with previous studies that showed Ascaris lumbricoides as the most prevalent helminth species14,27. This prevalence could be due to poor hygienic risk factors linked to crowded living conditions in the camps, lack of clean sufficient toilets/latrines, poor sewage waste disposal, and insufficient clean drinking water that encourages the reproduction, transmission, and reinfection of Ascaris lumbricoides. Hamad and Mauti28, reported that the prevalence and intensity of STH infections within populations are linked to different factors most importantly socioeconomic, environmental, parasitic, and host factors.
The mean Haemoglobin concentration was significant at p = 0.000 in positively infected participants to P. falciparum and P. vivax.This is most likely because higher parasite densities cause more RBCs to be destroyed and more intense attacks.The increase in red blood cell breakdown by the parasites may be the cause of reduced haemoglobin in malaria.This finding is in agreement with those previously reported by Asmerom et al.29 and Njewa et al.30. Haemoglobin variation across the intestinal parasites was normal in both infected and non-infected participants. The current investigation also shows that, depending on the parasite species, the mean Hb concentration had different relationship with the infection intensities.This finding is in agreement with that conducted in the North West region of Cameroon by Ntonifor et al.7. However, this is contrary to studies reported by Genanew et al.31 and Tofel et al.32. The disparity might be ascribed to the various study populations which were apparently healthy asymptomatic participants as well as the methods’ sensitivity for determining haemoglobin levels. Participants infected with Trichuris trichiura (p = 0.017) and Schistosoma mansoni(p = 0.037) had a significant impact on haemoglobin concentration levels. An infection with Trichuris trichuira can affect the concentration of haemoglobin because the worm inserts its head into the intestinal mucosa until trauma occurs, causing irritation and inflammation of the mucosa. In addition to causing bleeding at the site of attachment, this worm can cause anaemia by sucking the host’s blood according to Aryadnyani et al.33. Also, Schistosoma mansoni impacted haemoglobin concentration. This can be attributed to chronic blood loss that results from the bleeding induced by migration of the worms through the intestinal wall or due to blood consumption by adult schistosomes34.
Conclusion
Malaria and STHs are still public health concern in Cameroon. Malaria infection negatively influences haemoglobin level. Asymptomatic malaria and STHs carriers are transmission factors to these parasites so the government needs to take into consideration these groups of people to eradicate or limit the transmission rate.
Limitations
The study worked only with male military personnel. Secondly, we could not determine the exact location where the participants got infected to carry out an epidemiological survey. Schistosoma intercalatum was gotten for the first time in the study area but the relative abundance and transmission dynamics on the snails was not done to determine if the vectors are available in the regions.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
WHO. Constitution of the World Health Organization–Basic documents. (2006).
Brooker, S. et al. Epidemiology of Plasmodium- helminth co-infection in africa: populations at risk, potential impact on anaemia and prospects for combining control. Am. J. Trop. Med. Hyg. 77 (6S), 88–98 (2007).
Mertens, J. E. A history of malaria and conflict. Parasitol. Res. 123 (3), 165 (2024).
Lindrose, A. R., Mitra, I., Fraser, J., Mitre, E. & Hickey, P. W. Helminth infections in the US military: from strongyloidiasis to schistosomiasis. J. Travel Med. 28 (6), taab004 (2021).
Farrington, L. et al. Both inflammatory and regulatory cytokine responses to malaria are blunted with increasing age in highly exposed children. Malar. J. 16, 499 (2017).
Ntonifor, H. N., Chewa, J. S., Oumar, M. & Mbouobda, H. D. Intestinal helminths as predictors of some malaria clinical outcomes and IL-1β levels in outpatients attending two public hospitals in bamenda, North West Cameroon. PLoS Negl. Trop. Dis. 15 (3), 0009174 (2021).
Ntonifor, H. N., Fakeh, N. B. & Lem, A. E. Prevalence of malaria and associated clinical manifestations and myeloperoxidase amongst populations living in different altitudes of Mezam division, North West region, Cameroon. Malar. J. 22, 20 (2023).
Sumbele, I. U. N., Nkain, A. J., Ning, T. R., Anchang-Kimbi, J. K. & Kimbi, H. K. Influence of malaria, soil-transmitted helminths and malnutrition on haemoglobin level among school-aged children in muyuka, Southwest cameroon: Across-sectional study on outcomes. PLoS ONE. 15 (3), 0230882 (2020).
De Benoist, B., McLean, E., Egli, I. & Cogswell, M. Worldwide Prevalence of Anaemia 1993–2005: WHO Global Database on Anaemia (World Health Organization, 2008).
Sumbele, I. U. N. et al. Malarial anaemia and anaemia severity in apparently healthy primary school children in urban and rural settings in the Mount Cameroon area: cross sectional survey. PloS One. 10 (4), 0123549 (2015).
Letouzey, R. Phytogeographic map of Cameron. In: JA, editor. Les Atlas Jeune Afrique: Paris, France ; 20–24. (1980).
Mojoko, F. M. Urban Development in Fako Division (Unpublished M.Sc. Thesis). Department of Geography, University of Buea. (2011).
Council Development Plan. TIKO - communes et Villes unies du Cameroun, (2011). cvuc.cm/national/index.php/fr/carte-communale/region-du-sud/142../575-Tiko
Mugob, B. B. et al. Analysis of oxidative status, inflammatory cytokines, and Ascaris lumbricoides infection in women at a health district in bamenda, northwest, Cameroon. Egypt. J. Intern. Med. 36, 42. https://doi.org/10.1186/s43162-024-00306-8 (2024).
Cochran, G. W. Sampling techniques. 3rd Edition. Wiley, New York. ISBN: 047116240X. (1977).
Pourhoseingholi, M. A., Mohsen, V. & Mitra, R. Sample size calculation in medical studies. Gastroenterol. Hepatol. Bed Benchv. 6(1), 4017493 (2013).
O’connell, K. & White, C. Everything you need to know about fever. https://www.healthline.com/health/fever. Date accessed 18/04/2020.
Katz, N., Chaves, A. & Pellegrino, J. A simple device for quantitative stool thick-smear technique in schistosomiasis mansoni. Rev. Inst. Med. Trop. Sao Paulo. 14, 397–400 (1972).
WHO. Bench aids for the diagnosis of intestinal parasites, second edition. Geneva. (2019).
Cheesbrough, M. District Laboratory Practice in Tropical Countries (Cambridge University Press, 2009).
Mekachie Sandie, S., Sumbele, I. U. N., Tasah, M. M. & Kimbi, H. K. Malaria and intestinal parasite co-infection and its association with anaemia among people living with HIV in Buea, Southwest Cameroon: A community-based retrospective cohort study. PLoS One 22, 16 (2021).
Gontie, G. B., Wolde, H. F. & Baraki, A. G. Prevalence and associated factors of malaria among pregnant women in Sherkole district, Benishangul Gumuz regional state, West Ethiopia. BMC Infect. Dis. 20 (1), 573. https://doi.org/10.1186/s12879-020-05289-9 (2020). PMID: 32758164; PMCID: PMC7405459.
Kimbi, H. K. et al. Malaria and haematologic parameters of pupils at different altitudes along the slope of Mount cameroon: a cross-sectional study. Malar. J. 12, 193 (2013).
Nyasa, R. B., Fotabe, E. L. & Ndip, R. N. Trends in malaria prevalence and risk factors associated with the disease in nkonghombeng; A typical rural setting in the Equatorial rainforest of the South West region of Cameroon. PLoS ONE. 16, 1–20 (2021).
Tampubolon, S. K. M., Raharjo, M. & &Sulistiyani, S. Environmental vulnerability against the presence of Anopheles spp. With malaria cases in North Jakarta. JurnalPenelitian Pendidikan IPA. 9 (Special Issue), 878–884 (2023).
Peter, V., Benjamin, D., Chris, M., Marjan, V. E. & Patrick, S. Screening the asymptomatic soldiers after a stay in sub-Saharan africa. A retrospective observational study. Travel Med. Infect. Dis. 39, 101941. https://doi.org/10.1016/j.tmaid.2020.101941 (2021).
Bashi, B. M., Ntonifor, H. N., Boubga, C., Ngwenah, F. E. & Mahamat, O. Analysis of oxidative status, inflammatory cytokines, and Ascaris lumbricoides infection in women at a health district in bamenda, northwest, Cameroon. Egypt. J. Intern. Med. 36, 42. https://doi.org/10.1186/s43162-024-00306-8 (2024).
Hamad, A. A. & Mauti, O. G. Determination of the prevalence of Ascaris lumbricoides in children under the age of five years attending at Kongowe health centre, Kibaha district, Pwani region. J. Parasitol. Res. https://doi.org/10.1155/2024/1932633 (2024).
Asmerom, H., Gemechu, K., Sileshi, B. & Arkew, M. Hematological abnormalities among malaria infected adult patients in association with ABO blood groups at Jinella health center, harar, Eastern Ethiopia. J. Blood Med. 14, 463–476 (2023).
Njewa, B., Eyong, E. E. J. & Ebai, C. B. Malaria parasitaemia and its impact on biological parameters among children < 16 years old attending the Nkwen District Hospital. Cameroon. Malariaworld J. 15, 3. https://doi.org/10.5281/zenodo.10731943 (2024).
Genanew, B., Getu, F., Walle, M. & Hailu, A. Anemia among malaria patients with and without soil-transmitted helminths in Arba Minch town health facilities: a comparative cross-sectional study. Medicine https://doi.org/10.1097/MD.0000000000036835 (2024).
Tofel, H. K., Abongwa, L. E., Ndifor, R. F. & Ntonifor, H. N. Intestinal helminthiasis, anaemia and associated risk factors in a cross-section of the population of melong, littorial region of Cameroon. Sci. Rep. 14, 649. https://doi.org/10.1038/s41598-023-46446-9 (2024).
Aryadnyani, N. P., Inderiati, D. & Ulfah, F. Hemoglobin levels on Trichuris trichiura infection in children. Med. Lab. Technol. J. https://doi.org/10.31964/mltj.v6i1.289 (2020).
Lamyman, M. J., Noble, D. J., Narang, S. & Dehalvi, N. Small bowel obstruction secondary to intestinal schistosomiasis. Trans. R. Soc. Trop. Med. Hyg. 100 (9), 885–887. https://doi.org/10.1016/j.trstmh.2005.10.013 (2006).
Acknowledgements
The authors express immense gratitude to the University of Bamenda, University of Buea, the Delegations of public health and the Ministry of defence that authorised and approved this research study. We forever remain thankful to the Armed Forces of the North West and South West Regions of Cameroon that consented to take part in this study.
Author information
Authors and Affiliations
Contributions
S.B.C., H.N.N., T.H.K., V.T.J., B.Y.W. and G.S.T. conceived and designed the experiments. S.B.C., V. T. J., B. Y. W. and G.S.T. enrolled and performed the experiments. S.B.C., H.N.N., and G.S.T. contributed to data management, analysis, and interpretation. S.B.C wrote the manuscript. H.N.N., and S.B.C. collaborated on the scientific writing of the manuscript. H.N.N. and S.B.C. reviewed the analyses and the final version of the manuscript. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Che, S.B., Ntonifor, H.N., Tofel, K.H. et al. The impact of malaria and intestinal helminths on haemoglobin concentrations among armed forces of the North West and South West Cameroon. Sci Rep 15, 35684 (2025). https://doi.org/10.1038/s41598-025-19507-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-19507-4
