
Abstract
Primary healthcare centers (PHCs) play a crucial role in China’s hierarchical medical system by providing essential community-level services. This study takes Tianjin, a major northern metropolis, as a case study to evaluate the spatial accessibility of PHCs and identify intra-city disparities. Using POI data to locate PHCs, population data to model healthcare demand, and road network data to simulate travel times, the Gaussian Two-Step Floating Catchment Area method was applied to measure primary healthcare accessibility within a 15 min travel threshold. The results revealed that PHC accessibility declined from the city center to the periphery, influenced by population density, economic development, and road network. Central districts like Heping and Nankai exhibited high accessibility, while Wuqing and Jizhou also performed well due to their strategic locations. In contrast, suburban and outer suburban districts such as Dongli, Jinghai, and Ninghe faced significant shortages in primary healthcare services. Spatial autocorrelation analysis using Global and Local Moran’s I identified high-accessibility clusters in Nankai Beichen, Wuqing, and Jizhou, and low-accessibility clusters mainly in the outer suburbs. Furthermore, K-means clustering analysis categorized Tianjin into four groups, suggesting targeted policies to enhance healthcare equity by redistributing resources, improving transport infrastructure, and expanding telemedicine, particularly in underserved areas.
Similar content being viewed by others

Introduction
Healthcare accessibility remains a critical issue in global public health, especially in its contribution to improving population health outcomes and quality of life1. Equitable access to healthcare services not only enhances individuals’ ability to make informed health decisions but also mitigates disparities in healthcare utilization. However, many countries continue to struggle with uneven distribution of medical resources, particularly in the context of rapid urbanization and population mobility2,3,4. Geographic conditions, economic development levels, and unequal distribution of resources further complicate this landscape, influencing the spatial distribution of healthcare facilities and access to services5,6. In this context, the assessment of healthcare accessibility is important for identifying barriers and informing resource prioritization to improve health outcomes and ensure equitable service delivery.
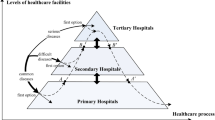
China, with one of the largest populations in the world, provides healthcare mainly through a traditional three-tiered healthcare system7. In this system, tertiary hospitals manage severe and complex conditions, secondary hospitals deliver comprehensive medical services at the regional level; and primary healthcare institutions (PHCs) acts as the “first line of defense” for common and frequent illnesses within community settings8. As the first point of contact for patients, PHCs play an important role in providing close-to-home healthcare and safeguarding public health9. As of 2023, China had established 33,753 township health clinics and 37,177 community health centers10. Studies suggest that regions with a more extensive network of PHCs tend to have more equitable access to healthcare services and improved health outcomes1,11. Moreover, efficient utilization of PHCs significantly reduces patient traffic to tertiary hospitals, helping to lower healthcare costs and improve resource allocation efficiency12,13,14. In response to rising healthcare demand and the overcrowding of higher-level hospitals, China officially implemented the hierarchical healthcare system nationwide in 2016, requiring patients to seek initial treatment at PHCs and be referred to higher-level hospitals when necessary15. This system aims to optimize patient flow and reduce the burden on large hospitals16. However, the operation of this system places greater demands on the allocation efficiency of primary healthcare resources17.
Spatial accessibility is a key measure for evaluating the equity of healthcare resource allocation, reflecting the spatial alignment between healthcare facilities and the populations they serve18. Early approaches used in these assessments included distance-based measures, buffer analysis, cumulative opportunity models, and balance coefficient methods. While these methods helped reveal physical proximity, they often overlooked critical factors like travel costs and the complexity of transportation networks19,20,21. Advancements in Geographic Information Science (GIS) and computational technologies have led to the development of more sophisticated methods, such as network analysis, cost-weighted distance models, gravity models, and the Two-Step Floating Catchment Area (2SFCA) method22,23,24. The 2SFCA method has become a leading tool due to its ability to combine healthcare supply, population demand, and travel costs into a comprehensive framework, making it highly effective for large-scale accessibility analyses. However, the traditional 2SFCA uses a binary approach to distance decay, treating all locations within a threshold as equally accessible while excluding those beyond it. To address this, models like the Enhanced 2SFCA, Gravity 2SFCA, Kernel Density 2SFCA, and Gaussian 2SFCA (G2SFCA) have introduced more refined decay functions25.
Several studies have employed these models to evaluate the spatial equity of healthcare services, identifying service gaps and regional clusters across different contexts. For instance, Hao et al.26 applied the G2SFCA to evaluate the accessibility of hospitals with antivenom serum across different regions of Hainan. Similarly, Wei et al.27 categorized healthcare services and utilized a Three-Step Floating Catchment Area method to assess the accessibility of outpatient and inpatient services across 31 provinces in China. These studies offer valuable insights into handling transportation networks, integrating supply–demand matching, and quantifying distance decay models. However, most of these analyses focus on nationwide or city-wide healthcare resource distribution and lack a specific focus on PHCs27,28,29. In contrast, Guo et al.30 included PHCs in their analysis of public health resources in Tianjin using the Ga2SFCA method. However, their study was limited to the central urban area, analyzing only 400 out of 3000 PHCs, and primarily focused on supply–demand balance, rather than evaluating the accessibility of PHCs within the framework of hierarchical healthcare systems. Recent advancements have been made to improve accessibility models. For example, Liu et al.31 applied G2SFCA to assess healthcare accessibility across different age groups in Karamay, highlighting the importance of considering demographic variations in accessibility analysis. Liu et al.32 further improved the 2SFCA model by incorporating facility supply capacity, enhancing the comprehensiveness of the analysis. Despite these improvements, existing studies still fail to fully account for real-time factors. In particular, despite the growing significance of China’s 15 min health service circle, which mandates that PHCs should be within a 15 min travel distance for all residents, many studies do not incorporate this concept into accessibility evaluations. Moreover, most studies focus primarily on large hospitals, leaving the distribution and accessibility of PHCs largely underexplored, especially in the context of tiered healthcare policies that prioritize initial treatment at primary care institutions. Furthermore, traditional accessibility models, while valuable, often rely on basic data sources that fail to account for real-time transportation networks and dynamic population changes, leading to inaccuracies in evaluating true accessibility.
As an international logistics hub in northern China, Tianjin has developed into one of the country’s megacities, ranking 11th nationwide in terms of GDP (as shown in Fig. 1). By 2023, Tianjin’s urbanization rate reached 85.49%, with a population of 13.64 million and a population density of 1139.9 people per square kilometer, placing it fifth nationally33. The rapid urbanization and high population concentration place increasing pressure on the city’s primary healthcare services. At present, Tianjin has over 3000 PHCs, including clinics, community health centers, and township hospitals, with density declining from central districts to peripheral areas. Moreover, as an early adopter of China’s hierarchical healthcare system, Tianjin has focused on strengthening primary care through reforms aimed at promoting resource allocation to lower-level institutions and fostering collaboration among healthcare providers34. These reforms have led to the establishment of medical groups to facilitate resource sharing, along with the integration of specialists into primary care. Additionally, the city has established 241 grassroots chest pain units, 92 community pain clinics, and 178 chronic disease management centers to enhance primary care capacity35. However, it remains unclear whether these resources adequately meet accessibility needs within acceptable travel times. Therefore, this study analyzes the spatial distribution of PHCs in Tianjin and conducts a cluster analysis of accessibility across its districts to provide evidence for optimizing primary healthcare resource allocation and improving equity in primary care.

Study area location in Tianjin China.
This study adds to existing research by providing a PHC-centered, policy-oriented assessment of healthcare accessibility under China’s hierarchical healthcare system. It has three primary objectives. First, we used multi-source, high-resolution data—including Points of Interest (POI) from the Gaode Open Platform, population data from WorldPop, and road network data from OpenStreetMap—to apply the G2SFCA method with a 15 min travel threshold. This design directly tests whether PHCs meet the service standards set by China’s “15 min health service circle” policy and improves accessibility estimation by modeling continuous distance decay, rather than treating all locations within a threshold as equally accessible. Second, we combined spatial autocorrelation analysis with K-means clustering to identify statistically significant high- and low-accessibility clusters and to group districts by shared accessibility characteristics, allowing us to pinpoint where resource shortages are most severe and where accessibility is unexpectedly high despite limited infrastructure. Third, by explicitly situating the analysis within the hierarchical healthcare policy context, we translated these results into targeted recommendations, specifying which areas should prioritize PHC expansion, transportation improvements, or telemedicine services to address accessibility inequities. Collectively, this study integrates policy-relevant thresholds, refined spatial analytics, and high-resolution data to produce evidence directly applicable to PHC resource planning.
Data source and processing
Study area
Located along the Bohai Sea, Tianjin is one of China’s four directly-administered municipalities and serves as a major port city. Its strategic position near Beijing makes it a crucial gateway to the sea for northern China. The city spans approximately 11,900 km2, featuring flat plains and coastal terrain. It is divided into 16 administrative districts, including the central urban areas of Heping, Hexi, Nankai, Hebei, Hongqiao, and Hedong. Surrounding the urban core are suburban districts such as Dongli, Xiqing, Jinnan, and Beichen. The outer suburban districts, including Binhai New Area, Wuqing, Baodi, Jinghai, Ninghe, and Jizhou, support broader regional expansion (as shown in Fig. 2a). With a population of approximately 13.9 million, a significant proportion resides in the urban core and the rapidly growing Binhai New Area. In the first half of 2024, the city’s GDP reached 819.112 billion RMB, reflecting a 4.9% year-on-year growth36.

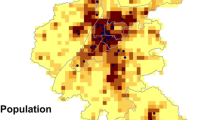
Spatial distribution of PHCs, population density, administrative zones, and road network in Tianjin. (a) Administrative zones in Tianjin, highlighting the core, suburban, and outer districts. (b) Road network classification in Tianjin, categorized by road types. (c) Distribution of PHCs across Tianjin. (d) Population density of residential areas within Tianjin (measured in individuals per km2).
Data
This study utilized POI data for all PHCs in Tianjin, including community health service centers, township health centers, and village clinics. The POI data, obtained from the Gaode Open Platform (https://lbs.amap.com/), provided precise geographic coordinates for each facility. As shown in Fig. 2d, we identified a total of 3211 PHCs. Due to the unavailability of service capacity data for each individual PHC in Tianjin, we used the number of healthcare personnel per 1000 population in PHCs across each district as a pr for service capacity, following previous studies with similar data limitations27,30,37.
The 2021 population data for Tianjin was sourced from the WorldPop dataset (https://www.worldpop.org/), with a spatial resolution of 100 m. To minimize spatial resolution errors, the WorldPop data was adjusted using a correction factor calculated by comparing the WorldPop-derived total population with the results from Tianjin’s Seventh National Population Census38. Following this adjustment, the data was aggregated into 4 km2 hexagonal grids, producing a total of 5429 cells. Based on the terrain and river network distribution, grid cells with a population density of zero were excluded, resulting in a final set of 4592 cells. This hexagonal structure reduces edge effects and ensures more uniform spatial coverage, enhancing the accuracy of the accessibility analysis.
The road network data used in this study was obtained from the OpenStreetMap (OSM) database (https://www.openstreetmap.org/), a comprehensive and freely accessible global mapping resource (as shown in Fig. 2b). OSM offers detailed and regularly updated spatial data, including road classifications, paths, and other transportation infrastructure. The downloaded road network included road categories and corresponding explanations for each classification. (http://wiki.openstreetmap.org/wiki/Key:highway). As shown in Table 1, we matched OSM road classifications with Chinese standards and assigned speed values based on Tianjin’s local conditions, using 80% of the maximum speed limit for each road type to simulate realistic travel conditions, as done by Wei et al.27.
Rather than relying on road network distance, we applied a maximum travel time threshold of 15 min to assess accessibility. This method more accurately reflects real-world healthcare access by accounting for both speed variations and road conditions. Prioritizing travel time over distance enhances the precision of accessibility assessments, particularly in urban environments where traffic congestion and variable road speeds significantly influence travel outcomes.
Model
Gaussian two-step floating catchment area (G2SFCA) method
The accessibility of healthcare services is influenced not only by geographic proximity but also by the capacity of healthcare facilities. This study employed the G2SFCA method, which incorporates distance decay effects and adjusts for variations in service capacity and population distribution, to analyze the spatial accessibility of PHCs for Tianjin residents within a 15 min travel time. This analysis assesses the feasibility of the “minor ailments treated at the grassroots level” principle within China’s hierarchical healthcare system under real-world conditions.
The standard 2SFCA method is based on supply and demand points, performing a two-step search within a specified distance threshold, and then summing the supply-to-demand ratios to determine accessibility at each demand point22. Cheng37 successfully applied the 2SFCA method to identify medically underserved areas in Nanjing, China. However, this method does not account for the effect of distance decay in the interaction between supply and demand. To address this limitation, researchers have extended the 2SFCA method by adding an additional distance decay function within the search radius25. Common distance decay functions include segmented decay forms with distance-weighted differentiation39, gravity-based decay models40, kernel density forms41, and Gaussian functions42. The primary differences among these extensions lie in the varying decay trends of their respective distance decay functions.
The G2SFCA method in this study uses the Gaussian function for smooth, continuous decay over distances. Empirical studies confirm its effectiveness in assessing spatial accessibility of healthcare institutions43,44,45. The steps are as follows:
In the first step, each PHC was designated as a supply point, and the center point of each population grid cell \(k\) was extracted as the demand point \(i\). A search domain \(j\) was established with a radius corresponding to the maximum travel time to a healthcare facility (\(d_{0}\) = 15 min). Within this search domain, the total population was aggregated, and the Gaussian function was applied to calculate weights according to the distance decay rule. These weighted population values were then summed to compute the supply-to-demand ratio \(R_{j}\):
Here, \(S_{j}\) denotes the service capacity of primary healthcare facility \(j\), measured as the number of healthcare personnel per 1000 population in PHCs. \(P_{k}\) represents the population of each demand unit \(k\), and \(d_{kj}\) is the travel time between demand unit \(k\) and facility \(j\). The demand unit \(k\) must be located within the search domain (\(d_{kj} \le d_{0}\)). \(G\left( {d_{kj} ,d_{0} } \right)\) is the Gaussian decay function, which accounts for spatial friction, and is expressed in the following form:
In the second step, a search domain was centered on each demand point \(i\), with the radius defined by the maximum allowable travel time \(d_{0}\) to a PHC. Within this domain, all relevant PHCs \(j\) were identified. The supply-to-demand ratios \(R_{j}\) for these facilities were then aggregated, with each ratio weighted according to the Gaussian decay function. This aggregation yields the time-based spatial accessibility \(A_{i}\) for each demand point:
In formula (3), \(A_{k}\) represents the spatial accessibility at demand point \(i\). The distance decay function \(G\left( {d_{ij} , \, d_{0} } \right)\) assigns smaller weights to more distant PHCs, reflecting the reduced likelihood of residents accessing primary healthcare as travel time increases. This ensures that PHCs closer to the demand point contribute more significantly to the overall accessibility score than those farther away. A higher value of \(A_{i}\) indicates better accessibility to PHCs for residents at that specific demand point.
To interpret the accessibility scores, we categorized values into five levels to reflect service adequacy: extremely low (0.000–0.010) indicates severe mismatch between PHC supply and demand; low (0.011–0.300) reflects limited access due to sparse distribution or long travel times; moderate (0.301–0.500) suggests basic needs are met but under pressure; high (0.501–1.000) implies balanced access; and very high (> 1.000) represents surplus capacity and abundant service availability.
Global Moran’s I
To evaluate the spatial autocorrelation of the calculated accessibility results, we employed Global Moran’s I, a widely used statistic in spatial analysis46. This metric helps identify whether areas with similar accessibility values tend to form clusters or are randomly distributed within the study area47. Global Moran’s I values range from − 1 to 1, with values close to 1 suggesting strong positive spatial autocorrelation. By applying this method, we can learn about the spatial patterns of primary healthcare accessibility in Tianjin.
The Global Moran’s I index was calculated as follows:
Here, \(N\) represents the total number of grid cells. \(x_{i}\) and \(x_{j}\) denote the accessibility values for grid cells \(i\) and \(j\), respectively. \(\overline{x}\) is the mean accessibility value across all grid cells, serving as a reference point for measuring deviations from the average. \(w_{ij}\) is the spatial weight matrix, defining the spatial relationship between units \(i\) and \(j\). Finally, \(W\) is the sum of all spatial weights \(w_{ij}\), which normalizes the spatial interactions within the system.
Anselin local Moran’s I
We used Anselin’s Local Moran’s I to capture the local spatial variations in primary healthcare accessibility across Tianjin. While Global Moran’s I assesses overall spatial autocorrelation, Local Moran’s I identifies specific clusters of high and low accessibility48. This method reveals “hotspots” of high accessibility and “coldspots” of low accessibility, allowing for a more detailed analysis of disparities in primary healthcare access.
The Anselin Local Moran’s I for a grid cell \(i\) was calculated as follows:
where \(x_{i}\), \(x_{j}\), \(\overline{x}\), and \(w_{ij}\) represent the same variables as previously explained in section “Global Moran’s I”. The local variance for unit \(i\), \(S_{i}^{2}\) was expressed as:
In this study, Local Moran’s I was applied to examine regions where primary healthcare access is either concentrated or lacking.
K-means clustering analysis
To further identify distinct spatial patterns across districts, we employed a K-means clustering algorithm. This unsupervised learning technique enables the grouping of districts based on multiple standardized indicators, supporting the identification of characteristic accessibility profiles. K-means clustering partitions the data into \(k\) non-overlapping clusters by minimizing the within-cluster sum of squared distances (WCSS). Formally, the objective function is:
where \(x\) denotes an observation vector (i.e., a district’s attribute profile), \(\mu_{i}\) is the centroid of cluster \(i\), and \(\left\| {x - \mu_{i} } \right\|^{2}\) is the squared Euclidean distance. This ensures that districts grouped into the same cluster are more similar to each other than to those in other clusters.
Five standardized indicators were used as input features for the clustering: PHC accessibility scores derived from the G2SFCA method, road network density, population density, healthcare personnel per 1000 residents in PHCs, and the density of PHCs in each district. All variables were z-score normalized to ensure comparability across dimensions and to prevent any single variable from dominating the clustering outcome. The optimal number of clusters was determined using the elbow method, which evaluates the marginal gain in explained variance with increasing cluster numbers; four clusters were selected based on the inflection point in the WCSS curve, providing a balance between analytical granularity and interpretability.
Results
Descriptive statistics
Tianjin’s districts exhibited spatial disparities in population density, residential units, and healthcare resources. Despite covering only 15% of the total land area, the central districts were home to approximately 30% of the city’s population. As shown in Fig. 2c, these areas had the highest population densities, averaging 20,000 people per km2, while outlying districts Wuqing and Jinghai had densities below 1000 people per km2. Table 2 showed that the top four central districts—Hedong, Nankai, Hebei and Heping—accounted for the densest urban areas, hosting 27% of the city’s residential units despite their smaller geographic size. In contrast, the largest districts by land area—Binhai, Baodi, Wuqing, Jizhou and Jinghai—occupied nearly 70% of the city’s land but only contained 31% of its residential units.
When considering primary healthcare resources, central districts contained 25% of Tianjin’s total PHCs, suburban districts held 26%, and outlying districts accounted for 49%. As illustrated in Fig. 2d, the six central districts had the highest concentration of PHCs. Moreover, the healthcare personnel-to-population ratio further highlighted gaps in service delivery. Table 2 showed that central districts, which employed about 40% of the city’s primary healthcare workforce, generally offered better access to primary care. Notably, Heping district led with 3.56 healthcare personnel per 1000 residents in PHCs, while most other central districts had ratios close to or above 2.5 per 1000, compared to less than 2 per 1000 in many outlying areas.
Tianjin’s spatial distribution of population and primary healthcare resources mirrored a typical urban development model, where central districts gathered both population and services. Meanwhile, suburban and outlying areas, despite their larger size, faced lower population densities and delayed primary resource allocation.
Accessibility of PHCs
The overall accessibility of PHCs in Tianjin was moderate, with a citywide mean value of 0.386. As shown in Fig. 3, primary healthcare accessibility decreased from central urban to suburban and outer suburban regions, where disparities in healthcare coverage became more significant.

Accessibility analysis of PHCs in Tianjin using health technicians as the supply.
Table 3 revealed that central urban areas had the highest accessibility of PHCs, with non-accessibility points ranging from 0 to 6.67% and mean accessibility values from 0.283 to 0.616. These districts benefited from well-distributed primary healthcare resources, demonstrated low variability (CV < 0.60) and minimal access disparities, particularly in Nankai and Hebei, where primary infrastructure was more evenly developed (see Fig. 3).
The accessibility in suburban districts reflected a transition between the central urban and outer suburban areas, with a clear trend of decreasing accessibility as residential zones moved further from the urban core (see Fig. 3). Among the four districts, Beichen showed the greatest variability in accessibility, followed by Xiqing, Jinnan and Dongli. While Dongli demonstrated more consistency in variation, it had the lowest average accessibility at 0.194 and the highest proportion of non-accessible points at 37.17% (see Table 3).
In outer suburban districts, except for Wuqing and Jizhou, primary healthcare accessibility in the remaining four districts was below the Tianjin average. Figure 3 highlighted underserved regions in southwestern Baodi, southeastern Binhai, central and western Ninghe, and southwestern Jinghai, where non-accessibility rates exceeded 40%, reflecting extremely low primary care coverage in vast rural areas. Despite Jizhou achieving a relatively high overall accessibility score, it exhibited significant internal disparities, revealing a severe imbalance in the distribution of PHC resources.
Despite being China’s first national comprehensive reform and innovation zone with a high GDP, Binhai lagged behind in primary healthcare development. Targeted policy intervention and resource allocation are urgently needed to align its primary healthcare services with economic growth and residents’ health needs. To further complement the main analysis, we also evaluated accessibility using a 15 min walking threshold, which better reflects the travel patterns of older adults and residents without private vehicles. The results of this supplementary scenario are presented in Appendix A1.
Spatial analysis of primary healthcare accessibility using Moran’s I
The Global Moran’s I for primary healthcare accessibility in Tianjin was 0.008, with a highly significant P value of 0, using inverse distance to define the distance threshold. This result showed a weak positive spatial autocorrelation, indicating minimal overall clustering despite some localized patterns. Consequently, the accessibility to PHCs did not have strong global clustering or dispersion across Tianjin. To explore potential localized clusters, we applied Anselin Local Moran’s I analysis, again employing inverse distance for the threshold. Figure 4 illustrates the presence of spatial clustering in primary healthcare accessibility across different regions of the city.

Spatial analysis of primary healthcare accessibility in Tianjin.
High-high clusters were primarily concentrated in Nankai and Wuqing, with small clusters in western Beichen and northeastern Jizhou. These clusters reflected a dense distribution of PHCs, which extended to surrounding areas and suggested potential positive spillover effects. This pattern aligns with the broader urban development model, where central districts typically receive more healthcare investment and better service coverage. Additionally, competitive behaviors and imitation effects may have emerged, as adjacent areas emulated the efficient resource allocation of central districts, thereby enhancing their own primary healthcare systems49.
Low-low clusters were mainly located in the outer suburban districts, including Baodi, Binhai, Jizhou, Jinghai and Ninghe, with a small low-value cluster also detected in northeastern Dongli within the suburban region. These areas showed low primary healthcare accessibility, with neighboring regions reflecting similarly poor accessibility. This pattern is likely driven by geographic isolation and infrastructural deficiencies, particularly in remote rural districts50.
Additionally, high–low and low–high outlier patterns were observed in parts of Wuqing, Jizhou, and Jinnan. These outliers indicated areas where primary healthcare accessibility was significantly higher or lower than in surrounding regions, highlighting localized imbalances in the distribution of healthcare resources.
Discussion
This study provides a spatial evaluation of primary healthcare accessibility in Tianjin based on the 15 min service threshold. The application of the G2SFCA method revealed clear spatial disparities, with the highest accessibility scores concentrated in central districts such as Nankai and Heping, where resources are abundant and well distributed. In contrast, peripheral districts like Baodi, Jinghai, and Ninghe exhibit limited access, indicating a core-periphery structure that is common in many Chinese megacities. However, certain outer districts—particularly Wuqing and Jizhou—demonstrate unexpectedly high accessibility. This result highlights the role of spatial connectivity and lower population pressure in offsetting infrastructure deficiencies, echoing findings from comparable cities such as Beijing and Nanjing4,15.
To better understand these spatial patterns and underlying disparities, we conducted a K-means clustering analysis51. As shown in Table 4, districts were categorized into four types: underdeveloped areas, highly concentrated areas, balanced areas, and peripheral high-accessibility areas. Underdeveloped areas, including Dongli, Xiqing, Jinnan, Beichen, Baodi, Ninghe, Jinghai, and Binhai, suffer from low accessibility scores due to insufficient PHCs, healthcare personnel, and poor public transport, requiring urgent interventions such as workforce expansion and telemedicine52,53. In contrast, highly concentrated areas like Heping and Nankai boast dense populations, abundant healthcare resources, and excellent infrastructure, but face the risk of inefficiencies due to over-saturation, highlighting the need for resource redistribution. Balanced areas, such as Hedong, Hexi, Hebei, and Hongqiao, feature well-aligned infrastructure with population needs, representing stable systems that should be maintained through efficient resource management54. Finally, peripheral high-accessibility areas like Wuqing and Jizhou achieve good access despite limited internal infrastructure, owing to their strategic locations, low population density, and proximity to arterial roads, demonstrating the compensatory effect of external connectivity.
Compared with previous studies in other megacities—such as Seoul, where service centralization leads to oversupply inefficiency55, or Singapore, where integrated health and land-use planning mitigates such disparities—our findings reinforce the need for locally adapted policies. While the core-periphery divide in Tianjin echoes national trends, the emergence of high-accessibility peripheral clusters reveals the compensatory role of urban connectivity, a dynamic less emphasized in the existing literature.
Importantly, disparities in primary care accessibility are not only structural or spatial issues but may also have profound public health consequences. Limited access to PHCs has been linked to delayed treatment, unmanaged chronic diseases, and unmet preventive needs, particularly among vulnerable populations such as the elderly and rural-to-urban migrants. Studies in China and other countries have shown that poor local access can increase social isolation and depressive symptoms, while better integration of primary healthcare and community services can enhance social cohesion and overall well-being56,57. In this light, the districts identified as underdeveloped or imbalanced in our clustering analysis may be early indicators of “healthcare deserts”—areas where limited spatial access to care is likely to compound with other barriers, such as weak community health linkages or insufficient social support, thus restricting residents’ ability to obtain timely and sustained care58,59.
The findings of this study can inform the development of targeted policy interventions. In the short term, expanding primary healthcare infrastructure in low-accessibility areas, particularly in outer suburban districts, should be prioritized. Strengthening transportation networks and redistributing healthcare personnel are also essential to reducing the accessibility gap53,60. Long-term efforts should focus on integrating initiatives across health, transportation, and urban planning sectors to ensure more equitable healthcare access. Telemedicine could further enhance accessibility in underserved regions by mitigating geographical barriers61.
Conclusion
This study investigates the spatial accessibility of PHCs in Tianjin under the framework of China’s hierarchical medical system, with a particular emphasis on whether the current spatial configuration of PHCs supports the policy goal of encouraging residents to seek care at the primary level. Using the G2SFCA method, we quantified accessibility within a 15 min travel threshold, aiming to capture whether PHC resources are equitably distributed in relation to population needs. Spatial autocorrelation analysis and K-means clustering were applied to further examine regional disparities and classify district-level patterns.
The findings confirm a distinct “core-periphery” pattern, with central districts benefiting from high accessibility and peripheral districts suffering from systemic shortages. The K-means results identified four types of spatial configurations—underdeveloped, highly concentrated, balanced, and peripheral high-accessibility areas—each calling for differentiated policy responses. These findings carry important implications for the implementation of tiered healthcare delivery: equitable access to PHCs is a necessary condition for redirecting patient flow to the grassroots level. In the short term, targeted infrastructure investment, personnel allocation, and telemedicine adoption are needed in underserved regions. In the long term, cross-sectoral integration between healthcare, transportation, and urban planning will be essential to sustaining equitable access and fulfilling the goals of hierarchical healthcare reform.
This study also has some limitations. First, the study relies on POI data from the Gaode Open Platform and population data from WorldPop, which may introduce inaccuracies due to data resolution and potential mismatches with census data. Second, the 15 min travel time threshold may not fully capture the complexity of real-world healthcare access, as factors like traffic congestion, road quality, and public transportation availability can further impact accessibility. Third, this study uses the number of healthcare personnel per 1000 population at the district level as a pr for PHC service capacity due to the unavailability of PHC-level personnel or bed data in Tianjin, which may reduce accuracy when assessing accessibility at smaller geographic units. Future research could enhance the realism of accessibility simulations by using more refined data on service capacity, as well as incorporating waiting times and population mobility. Dynamic models may also better capture how healthcare accessibility evolves with urban development and healthcare system reforms.
Data availability
The data used in this study are publicly available from the following sources: Gaode Map (https://lbs.amap.com), WorldPop (https://www.worldpop.org), and OpenStreetMap (https://www.openstreetmap.org). For data access assistance, please contact the corresponding author at 16611895389@163.com.
References
Kelly, C., Hulme, C., Farragher, T. & Clarke, G. Are differences in travel time or distance to healthcare for adults in global north countries associated with an impact on health outcomes? A systematic review. BMJ Open 6, e013059 (2016).
Wątróbski, J., Bączkiewicz, A. & Rudawska, I. A strong sustainability paradigm based analytical hierarchy process (SSP-AHP) method to evaluate sustainable healthcare systems. Ecol. Indic. 154, 110493 (2023).
Qin, A. et al. Does unequal economic development contribute to the inequitable distribution of healthcare resources? Evidence from China spanning 2001–2020. Access. Shapes Land Use 20, 20 (2024).
Du, X., Du, Y., Zhang, Y., Zhu, Y. & Yang, Y. Urban and rural disparities in general hospital accessibility within a Chinese metropolis. Sci. Rep. 14, 23359 (2024).
Frew, R., Higgs, G., Harding, J. & Langford, M. Investigating geospatial data usability from a health geography perspective using sensitivity analysis: The example of potential accessibility to primary healthcare. J. Transp. Health 6, 128–142 (2017).
Maláková, K. A geodemographic view of the accessibility of selected outpatient services in Czechia. Int. J. Public Health 67, 1604067 (2022).
Zhou, Z. et al. Evaluating the effect of hierarchical medical system on health seeking behavior: A difference-in-differences analysis in China. Soc. Sci. Med. 268, 113372 (2021).
Yip, W. et al. 10 years of health-care reform in China: Progress and gaps in Universal Health Coverage. Lancet 394, 1192–1204 (2019).
Li, X. et al. The primary health-care system in China. Lancet 390, 2584–2594 (2017).
National Health Commission of China. The 2023 Statistical Bulletin on the Development of China’s Health care. http://www.nhc.gov.cn/guihuaxxs/s3585u/202408/6c037610b3a54f6c8535c515844fae96/files/58c5d1e9876344e5b1aa5aa2b083a51a.pdf (2024).
Starfield, B., Shi, L. & Macinko, J. Contribution of primary care to health systems and health. Milbank Q. 83, 457–502 (2005).
Dusheiko, M., Gravelle, H., Martin, S., Rice, N. & Smith, P. C. Does better disease management in primary care reduce hospital costs? Evidence from English primary care. J. Health Econ. 30, 919–932 (2011).
Taubman, S. L., Allen, H. L., Wright, B. J., Baicker, K. & Finkelstein, A. N. Medicaid increases emergency-department use: Evidence from Oregon’s health insurance experiment. Science 343, 263–268 (2014).
Bailey, M. J. & Goodman-Bacon, A. The war on poverty’s experiment in public medicine: Community health centers and the mortality of older Americans. Am. Econ. Rev. 105, 1067–1104 (2015).
Lu, C., Zhang, Z. & Lan, X. Impact of China’s referral reform on the equity and spatial accessibility of healthcare resources: A case study of Beijing. Soc. Sci. Med. 235, 112386 (2019).
Huang, X., Zuo, R., Xu, T. & Li, N. Can hierarchical healthcare system improve public health efficiency? Evidence from 27 eastern Chinese cities. J. Clean. Prod. 447, 141369 (2024).
Wang, X., Yang, H., Duan, Z. & Pan, J. Spatial accessibility of primary health care in China: A case study in Sichuan Province. Soc. Sci. Med. 209, 14–24 (2018).
Pooler, J. A. The use of spatial separation in the measurement of transportation accessibility. Transp. Res. A-Pol. 29, 421–427 (1995).
Ingram, D. R. The concept of accessibility: A search for an operational form. Reg. Stud. 5, 101–107 (1971).
Geurs, K. T. & Van Wee, B. Accessibility evaluation of land-use and transport strategies: Review and research directions. J. Transp. Geogr. 12, 127–140 (2004).
Lucas, K., Van Wee, B. & Maat, K. A method to evaluate equitable accessibility: Combining ethical theories and accessibility-based approaches. Transportation 43, 473–490 (2016).
Radke, J. & Mu, L. Spatial decompositions, modeling and mapping service regions to predict access to social programs. Ann. GIS 6, 105–112 (2000).
Wang, F. Measurement, optimization, and impact of health care accessibility: A methodological review. Ann. Assoc. Am. Geogr. Assoc. Am. Geogr. 102, 1104–1112 (2012).
Weiss, D. J. et al. Global maps of travel time to healthcare facilities. Nat. Med. 26, 1835–1838 (2020).
Stacherl, B. & Sauzet, O. Gravity models for potential spatial healthcare access measurement: a systematic methodological review. Int. J. Health Geogr. 22, 34 (2023).
Hao, W. et al. Spatial accessibility analysis of snake antivenom. Int. J. Public Health 69, 1606903 (2025).
Wei, Z., Bai, J. & Feng, R. Evaluating the spatial accessibility of medical resources taking into account the residents’ choice behavior of outpatient and inpatient medical treatment. Socioecon. Plann. Sci. 83, 101336 (2022).
Zhang, C. et al. Evaluating the spatial accessibility and spatial layout optimization of HIV/AIDS healthcare services in Shandong Province, China. Sci. Rep. 14, 11258 (2024).
Chen, Y., Ding, Q. & Shen, Y. Assessing accessibility and social equity of tertiary hospitals for older adults: A city-wide study of Tianjin, China. Buildings 12, 2107 (2022).
Guo, X., Zeng, S., Namaiti, A. & Zeng, J. Evaluation of supply-demand matching of public health resources based on Ga2SFCA: A case study of the central urban area of Tianjin. ISPRS Int. J. Geo-Inf. 12, 156 (2023).
Liu, L., Gao, R. & Zhang, L. An equity evaluation of healthcare accessibility across age strata using the G2SFCA method: A case study in Karamay District, China. Land 13, 1259 (2024).
Liu, L., Lyu, H., Zhao, Y. & Zhou, D. An improved two-step floating catchment area (2SFCA) method for measuring spatial accessibility to elderly care facilities in Xi’an, China. Int. J. Environ. Res. Public Health 19, 11465 (2022).
Tianjin Bureau of Statistics. The 2023 Statistical Bulletin on National Economic and Social Development of Tianjin. https://www.tj.gov.cn/sq/tjgb/202403/t20240319_6564208.html (2024).
Luo, D. et al. Healthcare preferences of chronic disease patients under China’s hierarchical medical system: An empirical study of Tianjin’s reform practice. Sci. Rep. 14, 11631 (2024).
Tianjin Health Commission. Tianjin: Focusing on the grassroots so that people can enjoy health services close to home. https://wsjk.tj.gov.cn/XWZX6600/MTBD3030/202406/t20240614_6653099.html(2024).
Tianjin Bureau of Statistics. Gross Regional Product (2024 Q2). https://stats.tj.gov.cn/tjsj_52032/ (2024).
Cheng, L., Yang, M., De Vos, J. & Witlox, F. Examining geographical accessibility to multi-tier hospital care services for the elderly: A focus on spatial equity. J. Transp. Health 19, 100926 (2020).
Tianjin Bureau of Statistics. Tianjin 7th national population census bulletin (No.1). https://stats.tj.gov.cn/tjsj_52032/tjgb/202105/t20210521_5457266.html (2021).
Luo, W. & Wang, F. Measures of spatial accessibility to health care in a GIS environment: synthesis and a case study in the Chicago region. Environ. Plan. B Plan. Des. 30, 865–884 (2003).
Luo, W. & Qi, Y. An enhanced two-step floating catchment area (E2SFCA) method for measuring spatial accessibility to primary care physicians. Health Place 15(4), 1100–1107 (2009).
Dai, D. & Wang, F. Geographic disparities in accessibility to food stores in southwest Mississippi. Environ. Plan. B Plan. Des. 38, 659–677 (2011).
Dai, D. Black residential segregation, disparities in spatial access to health care facilities, and late-stage breast cancer diagnosis in metropolitan Detroit. Health Place 16, 1038–1052 (2010).
Mao, L. & Nekorchuk, D. Measuring spatial accessibility to healthcare for populations with multiple transportation modes. Health Place 24, 115–122 (2013).
Chen, B. Y., Cheng, X.-P., Kwan, M.-P. & Schwanen, T. Evaluating spatial accessibility to healthcare services under travel time uncertainty: A reliability-based floating catchment area approach. J. Transp. Geogr. 87, 102794 (2020).
Li, C. & Wang, J. A hierarchical two-step floating catchment area analysis for high-tier hospital accessibility in an urban agglomeration region. J. Transp. Geogr. 102, 103369 (2022).
Moran, P. A. P. Notes on continuous stochastic phenomena. Biometrika 37, 17–23 (1950).
Lu, Y., Yue, W., He, T. & Shan, Z. Urban form centrality and thermal environment: An empirical study of Chinese megacities. Sustain. Cities Soc. 83, 103955 (2022).
Anselin, L. Local indicators of spatial association—LISA. Geogr. Anal. 27, 93–115 (1995).
Sun, X., Lv, B., Gao, X. & Meng, K. A spatial Dubin model study in China. BMC Prim. Care 25, 62 (2024).
Mansour, S. Spatial analysis of public health facilities in Riyadh Governorate, Saudi Arabia: A GIS-based study to assess geographic variations of service provision and accessibility. Geo-Spat. Inf. Sci. 19, 26–38 (2016).
Ja, H. A K-means clustering algorithm. JR Stat. Soc. Ser. C-Appl. Stat. 28, 100–108 (1979).
Balarajan, Y., Selvaraj, S. & Subramanian, S. Health care and equity in India. Lancet 377, 505–515 (2011).
Chen, L., Chen, T., Lan, T., Chen, C. & Pan, J. The contributions of population distribution, healthcare resourcing, and transportation infrastructure to spatial accessibility of health care. Inq. J. Health Care Organ. Provis. Financ. 60, 00469580221146041 (2023).
Wu, H., Zhao, C., Zhu, Y. & Pan, Y. A multiscale examination of heat health risk inequality and its drivers in mega-urban agglomeration: A case study in the Yangtze River Delta, China. J. Clean. Prod. 458, 142528 (2024).
Yoon, Y. & Park, J. Equitable city in an aging society: Public transportation-based primary care accessibility in Seoul, Korea. Sustainability 14, 9902 (2022).
Wang, M. et al. Social isolation and depressive symptoms among Chinese older adults: Serial mediating roles of social support and resilience. Geriatr. Nur. (Lond.) 61, 589–595 (2025).
Dambha-Miller, H. et al. Integrated primary care and social services for older adults with multimorbidity in England: A scoping review. BMC Geriatr. 21(1), 674 (2021).
Väisänen, V., Satokangas, M., Huhtakangas, M., Antikainen, H. & Sinervo, T. Medical deserts in Finland: Measuring the accessibility and availability of primary health care services. BMC Health Serv. Res. 25, 281 (2025).
Flinterman, L. E. et al. Characteristics of medical deserts and approaches to mitigate their health workforce issues: A scoping review of empirical studies in western countries. Int. J. Health Policy Manag. 12, 7454 (2023).
Pan, J., Deng, Y., Yang, Y. & Zhang, Y. Location-allocation modelling for rational health planning: Applying a two-step optimization approach to evaluate the spatial accessibility improvement of newly added tertiary hospitals in a metropolitan city of China. Soc. Sci. Med. 338, 116296 (2023).
Carrillo De Albornoz, S., Sia, K.-L. & Harris, A. The effectiveness of teleconsultations in primary care: Systematic review. Fam. Pract. 39, 168–182 (2022).
Funding
This work was supported by the National Social Science Foundation of China [20AGL034], the Hainan Provincial Natural Science Foundation of China [724QN233] and the Graduate School of Tianjin University [A1-2021-009].
Author information
Authors and Affiliations
Contributions
Jiarui Han: Methodology, Writing—original draft. Liping Fu: Formal analysis, Validation. Xiaowang Zhang: Methodology, Data Collection and Processing. Tong Pei: Data Collection and Processing. Huayu Long: Supervision.
Corresponding author
Ethics declarations
Competing interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Han, J., Fu, L., Zhang, X. et al. Spatial accessibility evaluation and clustering analysis of primary healthcare within 15 min circles in a northern Chinese megacity. Sci Rep 15, 35643 (2025). https://doi.org/10.1038/s41598-025-19640-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-19640-0
