
Abstract
This study aimed to investigate the relationship between C-peptide levels, specifically 180-min postprandial C-peptide levels, and diabetic retinopathy (DR) in individuals with type 2 diabetes. This cross-sectional study involved 1545 participants divided into two groups: one with diabetic retinopathy (742 individuals) and one without (803 individuals). To assess the connection between C-peptide levels and DR, multivariate logistic regression and Spearman correlation analysis were performed, including subgroup analyses to ensure robustness of the results. Compared with individuals without DR, individuals with DR had significantly lower postprandial C-peptide levels. Additionally, these postprandial C-peptide levels were inversely correlated with Haemoglobin A1c (HbA1c), fasting blood glucose, and duration of diabetes but positively correlated with body mass index (BMI) and triglyceride levels. Logistic regression analysis revealed a strong inverse association between postprandial 180-min C-peptide levels and the risk of DR. Specifically, higher C-peptide levels were linked to a lower prevalence of DR, a relationship that persisted even after adjusting for potential confounding factors. Furthermore, when different subgroups were analyzed based on sex, age, BMI, and HbA1c levels, individuals without DR consistently had higher C-peptide levels than those with DR. A stratified analysis further confirmed that the inverse relationship between C-peptide levels and DR risk was consistent across most subgroups. In conclusion, the results of this study suggest that higher postprandial 180-min C-peptide levels are inversely related to the risk of diabetic retinopathy, implying that elevated C-peptide levels could offer some protection against the retinal damage associated with diabetes.
Similar content being viewed by others
Introduction
Diabetes has become one of the major issues threatening human health. According to a 2021 report by the International Diabetes Federation (IDF), approximately 536.6 million people aged 20–79 years have type 2 diabetes mellitus worldwide, and this figure is expected to increase to 783.2 million by 20451. Diabetes not only reduces quality of life and life expectancy but also serves as a leading cause of various microvascular and macrovascular complications, including blindness, kidney failure, and stroke2. Among these complications, diabetic retinopathy (DR) is a common complication in type 2 diabetes patients3 and is among the leading causes of vision impairment and blindness globally4. With the increasing incidence of diabetes and the increasing lifespan of patients, the prevalence of DR and its associated vision impairment are also increasing5.
Currently, in clinical practice, DR screening primarily relies on imaging technologies. For example, fundus fluorescein angiography, optical coherence tomography angiography, and fluorescence lifetime imaging ophthalmoscopy (FLIO) are novel noninvasive imaging technologies6. To some extent, these technologies have improved the sensitivity and accuracy of diagnosis. However, imaging detection is already at the stage of DR onset. The key lies in how to predict DR early, identify risk factors, and intervene in advance before its occurrence.
Biochemical markers could serve as valuable tools for detecting earlier stages of DR, identifying patients at high risk of retinal disease progression, and monitoring therapeutic efficacy7. Many studies based on clinical data have revealed associations between amino acids8 cholesterol9 and serum albumin10 and the development and progression of DR, indicating their potential as predictive biomarkers for this condition. Additionally, studies have shown that a decrease in fasting C-peptide levels is a risk factor for DR11,12 but the relationship between postprandial late-phase C-peptide levels and DR progression still needs further investigation.
Compared with insulin, C-peptide has a longer circulatory half-life and prevents first-pass metabolism in the liver; thus, it serves as a reliable indicator of β-cell function13,14. Moreover, C-peptide exhibits anti-angiogenic properties, reducing retinal neovascularization15. Research indicates that C-peptide serves not only as a predictor of whether type 2 diabetes patients need insulin therapy16,17,18 but also as a potential treatment for long-term complications of type 2 diabetes, such as DR19. However, fasting C-peptide levels mainly represent the basal secretion of pancreatic β-cells, whereas postprandial C-peptide can more accurately assess the function of pancreatic β-cells and the condition of diabetes patients20,21. Previous studies have confirmed that the occurrence of DR is closely associated with islet cell function22. Nevertheless, the connection between postprandial C-peptide levels and chronic complications such as DR remains debatable13 especially the link between 180-min post-load C-peptide (C-peptide-180) levels and DR, which is still unclear.
Thus, the present study aims to explore the correlation between C-peptide-180 levels and DR through a cross-sectional study involving 1545 patients with type 2 diabetes.
Results
Participant characterization description
Participants were categorized based on the presence or absence of DR (Table 1). Among the 1,545 participants, 803 (51.97%) had no DR, whereas 742 (48.03%) were diagnosed with DR. DR patients were older (53 years vs. 48 years, P < 0.01) and had a longer diabetes duration (8 years vs. 3 years, P < 0.0001) than NDR patients. Additionally, DR patients had lower postprandial C-peptide (PCP) and insulin levels than NDR patients. Significant differences in body mass index (BMI) (P = 0.012), (triglycerides) TG (P = 0.003), (high-density lipoprotein cholesterol) HDL-C (P = 0.003), and FCP levels (P < 0.0001) were also detected. No significant differences were observed in Haemoglobin A1c (HbA1c), (fasting blood glucose) FBG, fasting insulin, (total cholesterol) TC, (low-density lipoprotein cholesterol ) LDL-C, and DBP between groups.
Correlation of C-peptide with DR and other variables
Spearman’s correlation coefficient was used to evaluate the relationships between C-peptide and DR, as well as 180-minute postprandial C-peptide and other parameters (Table 2). Postprandial C-peptide was significantly negatively correlated with DR. 180-min postprandial C-peptide was significantly negatively correlated with HbA1c (r = −0.369, p < 0.0001), FBG (r = −0.218, p < 0.0001), HDL-C (r = −0.193, p < 0.0001), LDL-C (r = −0.125, p < 0.0001), and diabetes duration (r = −0.217, p < 0.0001) but significantly positively correlated with BMI (r = 0.279, p < 0.0001) and TG (r = 0.129, p < 0.0001).
Associations between 180-minute postprandial C-peptide and DR risk
After adjusting for potential confounders, we assessed the associations using multivariate logistic regression analysis. As shown in Table 3, the risk of DR significantly decreased with increasing 180-minute postprandial C-peptide levels. The unadjusted model showed that the OR for 180-minute postprandial C-peptide was 0.70 (95% CI 0.62–0.80; P < 0.0001). After adjusting for age, sex, and BMI in adjusted Model I, the OR for 180-minute postprandial C-peptide was 0.74 (95% CI 0.64–0.84, P < 0.0001). In Model 2, with further adjustments for hypertension, smoking status, drinking status, diabetes duration, and fatty liver, the corresponding OR was 0.79 (95% CI 0.69–0.90; P = 0.0002). In adjusted Model 3, after further adjustments, the association remained significant (OR, 0.69; 95% CI 0.59–0.80; P < 0.0001). Moreover, we performed ROC curve analysis to assess the predictive value of 180-minute postprandial C-peptide levels for diabetic retinopathy (DR). Model 2 showed the best performance (AUC = 0.69, 95% CI 0.66–0.72), with an optimal cutoff of 0.44 (sensitivity 67.3%, specificity 63.9%) according to the Youden index (Figure S1).
Comparison of C-peptide levels within various subgroups of DR categorized by sex, age, HbA1c level, and BMI
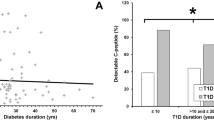
We grouped the participants based on sex, age, BMI, and HbA1c levels and compared the differences in C-peptide levels between those with and without DR in each group (Fig. 1). The results showed significant differences in C-peptide levels across all subgroups. Across all subgroups, C-peptide levels were significantly higher in patients without DR than in those with DR, suggesting that higher C-peptide levels may offer some degree of protection against diabetes-related retinal damage.

180-Minute Postprandial C-Peptide Levels in T2DM Patients with and without Diabetic Retinopathy. Comparison between males and females (a), older age (≥ 60) and younger age (< 60) (b), higher HbA1c levels (< 7%) and lower HbA1c levels (≥ 7%) (c), and higher BMI (≥ 25 kg/m2) and lower BMI (< 25 kg/m2) (d). Sample sizes for each subgroup are indicated above the corresponding bars. * p < 0.05, **p < 0.01, ***p < 0.001, ****p < 0.0001.
Stratified analysis of 180-minute postprandial C-peptide and the risk of diabetic retinopathy
As shown in Table 4, subsequent stratified analyses were conducted considering variables such as age, sex, BMI, diabetes duration, smoking status, FBG, HbA1c, and fatty liver. In most subgroup analyses, the association between 180-minute postprandial C-peptide and the risk of DR remained significant. This consistency highlights the significant association between 180-minute postprandial C-peptide levels and DR across various conditions and demographic characteristics. For patients aged ≥ 60 years and with a duration of diabetes > 10.0 years, the correlation was not significant. Additionally, in the subgroup analysis, the interaction effects of 180-minute postprandial C-peptide with diabetes duration (P value for interaction < 0.0001), smoking (Pvalue for interaction < 0.0001), and fatty liver (Pvalue for interaction 0.0002) on DR were significant.
Discussion
This cross-sectional study revealed that among 1545 type 2 diabetes patients, those with DR had lower postprandial C-peptide levels. Furthermore, 180-minute postprandial C-peptide levels were significantly negatively correlated with DR. After adjusting for major confounding factors, this correlation remained significant. Therefore, based on these observations, the 180-minute postprandial C-peptide level can serve as an effective predictive marker for assessing DR risk in individuals with type 2 diabetes.
Previous studies have shown significant variability in the prevalence of DR among diabetic patients. A study conducted in the UK revealed that among 46,962 type 2 diabetes patients, the prevalence of any form of DR was 38.0% in European whites, 52.4% in African/African-Caribbean individuals, and 42.3% in South Asians23. Another meta-analysis conducted in mainland China indicated that the prevalence of DR, nonproliferative diabetic retinopathy (NPDR), and proliferative diabetic retinopathy (PDR) among diabetic patients was 23%, 19.1%, and 2.8%, respectively24. A recent cross-sectional study conducted in the endocrinology department of Qingdao University Affiliated Hospital reported that 41.24% of patients had DR10. Based on data from this study, the prevalence of DR among type 2 diabetes patients was 48.03%. In studies involving hospitalized patients, the prevalence of DR was higher among type 2 diabetes patients, possibly because of poor glycemic control and a greater number of complications in this population.
The relationship between C-peptide levels and DR in type 2 diabetes patients remains controversial. Some previous studies have shown that fasting C-peptide, 30-minute postprandial C-peptide, and 2-hour postprandial C-peptide are negatively correlated with DR in type 2 diabetes patients25,26,27. A study from Korea found that lower quartiles of fasting and 2-hour postprandial serum C-peptide levels were associated with increased severity of retinopathy28. A European cohort study demonstrated that after adjusting for multiple confounding factors, the highest quartile of baseline C-peptide levels was negatively associated with the risk of retinopathy29. The above studies did not include 180-minute postprandial C-peptide, possibly because its level at this time point is relatively low, with smaller variations, making it difficult to obtain sufficient data to support its clinical relevance in practice. The 180-minute postprandial C-peptide reflects the functional state of the pancreas during the later postprandial phase (when blood glucose levels gradually decline), including pancreatic reserve function and delayed insulin secretion. C-peptide captures the dynamic changes during the recovery phase of postprandial blood glucose30,31. Additionally, it can accurately assess the impact of prolonged high blood glucose exposure on the retina and the relationship between chronic metabolic imbalance and DR, helping to identify high-risk patients at an early stage. However, our analysis of data from 1,545 patients indicates a negative correlation between 180-minute postprandial C-peptide levels and DR in patients with type 2 diabetes. A decline in insulin secretion capacity is typically accompanied by poor glycemic control, which increases the risk of DR. Adequate insulin secretion and early intervention can help delay the progression of DR, making 180-minute postprandial C-peptide a potential clinical marker for predicting DR risk. Additionally, our study employed standard diagnostic methods for DR and type 2 diabetes, with a relatively large sample size, enhancing its generalizability.
The results of the present study offer a simpler and more cost-effective indicator for clinical application. However, some studies have not found such an association. A study conducted in India involving 195 type 2 diabetes patients reported no association between serum C-peptide levels and retinopathy or diabetes duration32. A study from the United States involving 1,007 type 2 diabetes patients indicated that glycemic control, rather than C-peptide, was associated with the incidence and progression of DR. These findings might have resulted from small sample sizes, random errors, or the use of less accurate biomarker measurement methods two decades ago, which may have led to biased data. Taken together, our present data suggested a negative correlation between C-peptide levels and the occurrence of DR.
Moreover, we conducted a stratified analysis of the association between 180-minute postprandial C-peptide and DR. In most subgroup analyses, the association remained significant. However, it is noteworthy that no significant association was observed in individuals aged ≥ 60 years or those with a diabetes duration of more than 10 years. As shown in Table 1, the differences in age and diabetes duration between the DR and NDR groups were significant. These findings align with those of established consensus and research33,34 confirming that advanced age and long diabetes duration are critical risk factors for DR. These factors may entirely overshadow the influence of C-peptide on DR. Nonetheless, even after adjusting for confounding factors, the risk of DR remained significantly associated with 180-minute postprandial C-peptide levels.
Neovascularization in DR is a multifactorial process involving microvascular endothelial damage caused by hyperglycemia, exacerbation of oxidative stress, and the expression of pro-angiogenic factors35,36,37. C-peptide, a biologically active polypeptide, has been shown to reduce reactive oxygen species (ROS) production in endothelial cells and mitigate apoptosis38,39. In diabetic mice, C-peptide supplementation improved retinal neurodegeneration and inhibited VEGF-induced pathological changes40. Additionally, C-peptide acts as an anti-angiogenic agent, reducing retinal neovascularization by mitigating oxidative stress, vascular leakage, and inflammation15,41. In summary, C-peptide appears to protect retinal blood vessels by suppressing hyperglycemia-induced oxidative stress, reducing endothelial cell injury, and minimizing neovascular formation.
This study has certain limitations. First, due to the cross-sectional design, a causal relationship between C-peptide and diabetic vascular complications could not be established; further prospective studies are needed to confirm these effects. Second, the patients included in this study were from a single center, and the sample may not represent the entire population. Additionally, confounding factors such as dietary habits, genetics, and osteoporosis may have been present.
Conclusion
Based on the results from this hospitalized population, 180-minute postprandial C-peptide was negatively correlated with the risk of DR. Even after accounting for confounding factors, this correlation persisted. Our findings not only add to the current evidence but also suggest that maintaining optimal C-peptide levels may reduce the risk of DR. As research progresses, we aim to identify the clinical utility of monitoring and modulating C-peptide levels to inform future diabetes care strategies.
Methods
Study design and patients
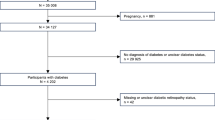
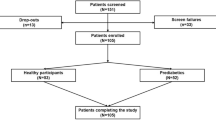
This cross-sectional study included patients aged 18 years and older who were diagnosed with type 2 diabetes. Data were collected from hospitalized patients at the First Affiliated Hospital of Zhengzhou University between January 2018 and December 2020. Person data were extracted from the hospital’s electronic medical records system. The exclusion criteria were as follows: (1) special types of diabetes or gestational diabetes; (2) severe systemic diseases (hematologic diseases, rheumatic diseases, or malignancies); (3) severe ocular conditions such as uveitis, glaucoma, or vitreous hemorrhage; (4) history of intraocular surgery; (5) incomplete or inconsistent clinical and laboratory data; and (6) renal insufficiency (serum creatinine ≥ 115 µmol/L) or hepatic dysfunction (alanine aminotransferase ≥ 97.5 U/L and/or aspartate aminotransferase ≥ 55.5 U/L). A total of 1545 patients, including 1060 men, were included in the final analysis. The study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the ethics committee of the First Affiliated Hospital of Zhengzhou University.
Anthropometric and biochemical measurements
After overnight fasting, venous blood samples were collected in the morning to measure FBG, fasting C-peptide, fasting insulin, TC, TG, LDL-C, and HDL-C levels. Fasting C-peptide levels were measured using the Elecsys C-Peptide assay (Roche Diagnostics) on a cobas e 801 analyzer. Intra- and inter-assay CVs were 0.9–2.9% and 2.3–3.6% respectively, validated across clinical concentrations with human serum and quality controls. Patients subsequently underwent an oral glucose tolerance test (OGTT), during which blood samples were collected again at 30, 60, 120, and 180 min to measure postprandial C-peptide and insulin levels. The above measurements were performed using a chemiluminescence assay on an automated analyzer. HbA1c concentrations were quantified using high-performance liquid chromatography (HPLC). At baseline, weight and height were measured, and BMI was calculated as weight (kg) divided by height squared (m2). After resting for at least 10 min, blood pressure was measured using an automated sphygmomanometer, and the average of three readings was recorded. Hypertension was defined as a blood pressure ≥ 140/90 mmHg or the use of antihypertensive medication. Obesity was defined according to the Asia-Pacific criteria as a BMI ≥ 25 kg/m242 and fatty liver was diagnosed by ultrasound.
Assessment of diabetic retinopathy
A standardized clinical ophthalmic evaluation was administered to all participants by board-certified endocrinologists or ophthalmologists with a minimum of 10 years of clinical experience. Protocol components included a comprehensive ophthalmologic history, visual acuity assessment, slit lamp biomicroscopy, and dilated fundoscopic examination. Subsequent to pharmacological mydriasis, two-field (macular and optic disc) 45° digital fundus photography was executed per a standardized protocol utilizing a digital retinal camera (Carl Zeiss Meditec AG). DR was diagnosed per Early Treatment Diabetic Retinopathy Study (ETDRS) criteria, defined by the presence of at least one microaneurysm or blot hemorrhage, with or without additional findings such as exudates (hard/soft), intraretinal microvascular abnormalities, venous beading, neovascularization (disc/elsewhere), or vitreous hemorrhage.
Statistical analyses
Normality tests were conducted, with continuous variables expressed as medians with interquartile ranges or means with standard deviations and categorical variables expressed as percentages. To evaluate differences between DR and NDR subjects, we used the Mann–Whitney U test for continuous variables via the wilcox.test function in R and the chi-square test for categorical variables using the chisq.test function. The correlation between C-peptide and DR, as well as other parameters, were assessed using Spearman’s correlation coefficients. Multivariate binary logistic regression was further employed to determine the association between postprandial 180-minute C-peptide levels and DR. A receiver operating characteristic (ROC) curve (AUC) was constructed to evaluate the discrimination of different models for DR. The maximum Youden index was used to determine the optimal cutoff point. Binary logistic regression was used to perform subgroup analysis of different clinical parameters and their interactions. Statistical significance was defined as P < 0.05. All analyses were conducted using R software version 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria; https://www.R-project.org).
Data availability
The data presented in this study can be obtained from the corresponding author upon reasonable request.
References
Sun, H. et al. IDF diabetes atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 183, 109119. https://doi.org/10.1016/j.diabres.2021.109119 (2022).
Kanter, J. E. & Bornfeldt, K. E. Impact of diabetes mellitus. Arterioscler. Thromb. Vasc Biol. 36, 1049–1053. https://doi.org/10.1161/atvbaha.116.307302 (2016).
Cai, K., Liu, Y. P. & Wang, D. Prevalence of diabetic retinopathy in patients with newly diagnosed type 2 diabetes: A systematic review and meta-analysis. Diabetes Metab. Res. Rev. 39, e3586. https://doi.org/10.1002/dmrr.3586 (2023).
Sabanayagam, C. et al. Incidence and progression of diabetic retinopathy: A systematic review. Lancet Diabetes Endocrinol. 7, 140–149. https://doi.org/10.1016/s2213-8587(18)30128-1 (2019).
Li, J. Q. et al. Prevalence, incidence and future projection of diabetic eye disease in Europe: A systematic review and meta-analysis. Eur. J. Epidemiol. 35, 11–23. https://doi.org/10.1007/s10654-019-00560-z (2020).
Nanegrungsunk, O., Patikulsila, D. & Sadda, S. R. Ophthalmic imaging in diabetic retinopathy: A review. Clin. Exp. Ophthalmol. 50, 1082–1096. https://doi.org/10.1111/ceo.14170 (2022).
Kaštelan, S., Orešković, I., Bišćan, F. & Kaštelan, H. Gverović antunica, A. Inflammatory and angiogenic biomarkers in diabetic retinopathy. Biochem. Med. (Zagreb). 30, 030502. https://doi.org/10.11613/bm.2020.030502 (2020).
Zong, G. W. et al. A metabolism-based interpretable machine learning prediction model for diabetic retinopathy risk: A cross-sectional study in Chinese patients with type 2 diabetes. J. Diabetes Res. 2023, 3990035. (2023). https://doi.org/10.1155/2023/3990035
Pan, W., Han, Y., Hu, H. & He, Y. The non-linear link between remnant cholesterol and diabetic retinopathy: A cross-sectional study in patients with type 2 diabetic mellitus. BMC Endocr. Disord. 22, 326. https://doi.org/10.1186/s12902-022-01239-5 (2022).
Li, X., Hao, W. & Yang, N. Inverse association of serum albumin levels with diabetic retinopathy in type 2 diabetic patients: A cross-sectional study. Sci. Rep. 14, 4016. https://doi.org/10.1038/s41598-024-54704-7 (2024).
Yau, J. W. et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care. 35, 556–564. https://doi.org/10.2337/dc11-1909 (2012).
Wang, Y. et al. Association of C-peptide with diabetic vascular complications in type 2 diabetes. Diabetes Metab. 46, 33–40. https://doi.org/10.1016/j.diabet.2019.04.004 (2020).
Vejrazkova, D., Vankova, M., Lukasova, P., Vcelak, J. & Bendlova, B. Insights into the physiology of C-peptide. Physiol. Res. 69, S237–s243. https://doi.org/10.33549/physiolres.934519 (2020).
Lin, Y., McCrimmon, R. J. & Pearson, E. R. Exploring the potential role of C-peptide in type 2 diabetes management. Diabet. Med. https://doi.org/10.1111/dme.15469 (2025).
Moon, C. H., Lee, A. J., Jeon, H. Y., Kim, E. B. & Ha, K. S. Therapeutic effect of ultra-long-lasting human C-peptide delivery against hyperglycemia-induced neovascularization in diabetic retinopathy. Theranostics 13, 2424–2438. https://doi.org/10.7150/thno.81714 (2023).
Iwao, T., Sakai, K. & Sata, M. Postprandial serum C-peptide is a useful parameter in the prediction of successful switching to liraglutide monotherapy from complex insulin therapy in Japanese patients with type 2 diabetes. J. Diabetes Complications. 27, 87–91. https://doi.org/10.1016/j.jdiacomp.2012.07.001 (2013).
Ohbatake, A. et al. C-Peptide area under the curve at glucagon stimulation test predicts glucose improvements by GLP-1 receptor analogue: A retrospective observational study. Diabetes Ther. 10, 673–681. https://doi.org/10.1007/s13300-019-0586-6 (2019).
Uehara, R. et al. Casual C peptide index: Predicting the subsequent need for insulin therapy in outpatients with type 2 diabetes under primary care. J. Diabetes. 14, 221–227. https://doi.org/10.1111/1753-0407.13257 (2022).
Yosten, G. L., Maric-Bilkan, C., Luppi, P. & Wahren, J. Physiological effects and therapeutic potential of proinsulin C-peptide. Am. J. Physiol. Endocrinol. Metab. 307, E955–968. https://doi.org/10.1152/ajpendo.00130.2014 (2014).
Si, Y. et al. Impact of acute-phase insulin secretion on glycemic variability in insulin-treated patients with type 2 diabetes. Endocrine 68, 116–123. https://doi.org/10.1007/s12020-020-02201-y (2020).
Liu, W. et al. Predictive value of postprandial C-peptide for utilizing multiple daily injection therapy in type 2 diabetes. Endocrine 85, 1162–1169. https://doi.org/10.1007/s12020-024-03820-5 (2024).
Roy Chowdhury, S. et al. Incidence of diabetic retinopathy in newly diagnosed subjects with type 2 diabetes mellitus over 5 years: Contribution of Β-cell function. J. Diabetes Complications. 36, 108028. https://doi.org/10.1016/j.jdiacomp.2021.108028 (2022).
Sivaprasad, S. et al. Ethnic variations in the prevalence of diabetic retinopathy in people with diabetes attending screening in the united Kingdom (DRIVE UK). PLoS One. 7, e32182. https://doi.org/10.1371/journal.pone.0032182 (2012).
Song, P., Yu, J., Chan, K. Y., Theodoratou, E. & Rudan, I. Prevalence, risk factors and burden of diabetic retinopathy in China: A systematic review and meta-analysis. J. Glob Health. 8, 010803. https://doi.org/10.7189/jogh.08.010803 (2018).
Huang, Y. et al. C-peptide, glycaemic control, and diabetic complications in type 2 diabetes mellitus: A real-world study. Diabetes Metab. Res. Rev. 38, e3514. https://doi.org/10.1002/dmrr.3514 (2022).
Pan, T. et al. The average 30-minute post-prandial C-peptide predicted diabetic retinopathy progress: A retro-prospective study. BMC Endocr. Disord. 23, 63. https://doi.org/10.1186/s12902-023-01300-x (2023).
Rouse, R. V., Bolin, L. M., Bender, J. R. & Kyewski, B. A. Monoclonal antibodies reactive with subsets of mouse and human thymic epithelial cells. J. Histochem. Cytochem. 36, 1511–1517. https://doi.org/10.1177/36.12.2461413 (1988).
Kim, B. Y., Jung, C. H., Mok, J. O., Kang, S. K. & Kim, C. H. Association between serum C-peptide levels and chronic microvascular complications in Korean type 2 diabetic patients. Acta Diabetol. 49, 9–15. https://doi.org/10.1007/s00592-010-0249-6 (2012).
Bo, S. et al. C-peptide and the risk for incident complications and mortality in type 2 diabetic patients: A retrospective cohort study after a 14-year follow-up. Eur. J. Endocrinol. 167, 173–180. https://doi.org/10.1530/eje-12-0085 (2012).
Wen, X. et al. Factors that determine glucose variability, defined by the coefficient of variation in continuous glucose monitoring values, in a Chinese population with type 2 diabetes. Diabetes Obes. Metab. 26, 611–621. https://doi.org/10.1111/dom.15350 (2024).
Kilberg, M. J. et al. Hypoglycemia and islet dysfunction following oral glucose tolerance testing in Pancreatic-Insufficient cystic fibrosis. J. Clin. Endocrinol. Metab. 105, 3179–3189. https://doi.org/10.1210/clinem/dgaa448 (2020).
Snehalatha, C., Mohan, R., Mohan, V., Ramachandran, A. & Viswanathan, M. Pancreatic B-cell function in relation to diabetic retinopathy in Asian Indian NIDDM patients. Acta Diabetol. Lat. 25, 95–100. https://doi.org/10.1007/bf02581372 (1988).
Wong, T. Y., Cheung, C. M., Larsen, M., Sharma, S. & Simó, R. Diabetic retinopathy. Nat. Rev. Dis. Primers. 2, 16012. https://doi.org/10.1038/nrdp.2016.12 (2016).
Wang, F., Mao, Y., Wang, H., Liu, Y. & Huang, P. Semaglutide and diabetic retinopathy risk in patients with type 2 diabetes mellitus: A meta-analysis of randomized controlled trials. Clin. Drug Investig. 42, 17–28. https://doi.org/10.1007/s40261-021-01110-w (2022).
Kang, Q. & Yang, C. Oxidative stress and diabetic retinopathy: Molecular mechanisms, pathogenetic role and therapeutic implications. Redox Biol. 37, 101799. https://doi.org/10.1016/j.redox.2020.101799 (2020).
Brownlee, M. Biochemistry and molecular cell biology of diabetic complications. Nature 414, 813–820. https://doi.org/10.1038/414813a (2001).
Liu, K. et al. Capsaicin ameliorates diabetic retinopathy by inhibiting poldip2-induced oxidative stress. Redox Biol. 56, 102460. https://doi.org/10.1016/j.redox.2022.102460 (2022).
Luppi, P. & Drain, P. C-peptide antioxidant adaptive pathways in β cells and diabetes. J. Intern. Med. 281, 7–24. https://doi.org/10.1111/joim.12522 (2017).
Bhatt, M. P. et al. C-peptide protects against hyperglycemic memory and vascular endothelial cell apoptosis. J. Endocrinol. 231, 97–108. https://doi.org/10.1530/joe-16-0349 (2016).
Lee, A. J. et al. Systemic C-peptide supplementation ameliorates retinal neurodegeneration by inhibiting VEGF-induced pathological events in diabetes. Faseb J. 37, e22763. https://doi.org/10.1096/fj.202201390RR (2023).
Jeon, H. Y. et al. Simultaneous attenuation of hyperglycemic memory-induced retinal, pulmonary, and glomerular dysfunctions by proinsulin C-peptide in diabetes. BMC Med. 21, 49. https://doi.org/10.1186/s12916-023-02760-7 (2023).
Jeon, H. Y. et al. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 363, 157–163. https://doi.org/10.1016/s0140-6736(03)15268-3 (2004).
Acknowledgements
We would like to thank the participants in this study.
Funding
WL is funded by the National Natural Science Foundation of China (82000831). XP is funded by the Joint Construction Project of Henan Medical Science and Technology Research Plan (Grant number: SBGJ202103068).
Author information
Authors and Affiliations
Contributions
Y. L.: Data curation, Formal Analysis, Investigation, Visualization, Writing – original draft, Writing – review & editing. B. L, Y. Z.: Formal Analysis, Investigation, Writing – original draft, Writing – review & editing. X. J., K. G., W H: Resources, Supervision, Writing—original draft, Writing—review & editing. M. X., Y. D., and Q. L.: Resources, Supervision, Writing—original draft, Writing—review & editing. W. L.: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. X. P.: Conceptualization, Methodology, Writing – original draft, Writing – review & editing.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics statement
Research involving human participants was reviewed and approved by the Ethics Committee of the First Affiliated Hospital of Zhengzhou University. All participants provided informed consent during the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, Y., Liu, B., Xue, M. et al. Correlation between C-peptide and diabetic retinopathy in patients with type 2 diabetes mellitus: a cross-sectional study. Sci Rep 15, 35896 (2025). https://doi.org/10.1038/s41598-025-19714-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-19714-z
