
Abstract
Small bowel obstructions (SBOs) account for about a fourth of hospital admissions related to acute abdominal complaints. Adhesive small bowel obstruction (ASBO) is the most common cause of SBO worldwide, and there are reported high success rates for conservative management. Understanding the success rate of conservative management in the Ethiopian context and the factors that influence it is crucial to prevent unnecessary surgeries and delays in treatment. To determine how often non-surgical treatment works for adhesive small bowel obstruction and to identify the factors that influence its success at Dessie Comprehensive Specialized Hospital, Ethiopia, between 2021 and 2023. A retrospective chart review was conducted on 350 ASBO cases at Dessie Comprehensive Specialized Hospital from June 1, 2021, to July 30, 2023. Cases were selected to represent each year of the study period, and patient charts were chosen randomly. Information from the records was compiled and analyzed to explore factors linked to patient outcomes. Associations between these factors and treatment results were examined, and findings were considered significant when the evidence strongly suggested a real relationship. The study included 350 ASBO cases, with a conservative management success rate of 45.1% (158 cases). Success was linked to factors like previous similar illnesses (AOR = 0.143), obstipation (AOR = 0.002), and the duration of current illness: <24 h (AOR = 0.143), 24–48 h (AOR = 9.250), and 48–72 h (AOR = 0.005). Additionally, the timing of the index operation influenced success: <1 month (AOR = 21.80), 1–3 years (AOR = 6.541), and 3–10 years (AOR = 31.997). The success rate of conservative management is higher than that reported in a similar local study; however, it remains low compared to global studies. Factors significantly associated with the success rate include the presence of previous episodes of illness, the duration of the current illness, the timing of the index operation, the presence of obstipation, and the length of the conservative management period.
Similar content being viewed by others

Introduction
Adhesive small bowel obstruction (ASBO) occurs when scar tissue (adhesions) forms between loops of the small intestine or between the intestine and surrounding structures, blocking the passage of intestinal contents1,2. It is a major cause of surgical admissions and can lead to serious complications, including bowel ischemia, perforation, and even death if not treated promptly. In many countries, especially in Western settings, post-operative adhesions account for the majority of small bowel obstruction cases, accounting for roughly 75% of occurrences3.
Adhesions are bands of scar tissue that form between normally separate abdominal structures or surfaces. They typically develop as part of the body’s natural healing process of the peritoneum after it has been damaged, often due to surgery3,4.
Adhesions form due to injury to the peritoneal mesothelium, which triggers local inflammation and activates fibrinocoagulative pathways. This process increases cellular turnover and the deposition of fibrinogen. Fibrin formation and fibrinolysis are normally balanced, but an imbalance leads to adhesive bands. Surgical injury also causes decreased blood flow and a persistent fibrin matrix, obstructing the resolution of clots3. Adhesions can be either filmy or dense, present as isolated bands or matted, making it difficult to recognize the visceral structures3.
The Zühlke classification categorizes post-operative adhesions into five grades: grade 0 indicates no adhesions, while grade IV represents strongly attached organs where dissection requires sharp techniques, risking organ damage. Additionally, the Peritoneal Adhesion Index (PAI) offers a more detailed classification that considers the anatomical locations of adhesions5.
The risk of developing adhesive small bowel obstruction (SBO) after transperitoneal surgery varies by procedure. Patients undergoing lower abdominopelvic or gynecologic surgeries, or those affecting a large area of the peritoneum, are at higher risk. The estimated risks are: 1% to 10% after appendectomy, 6.4% after open cholecystectomy, 10% to 25% after intestinal surgery, and 17% to 25% after restorative proctocolectomy (IPAA)4. Laparoscopy is believed to reduce the rate of SBO by minimizing trauma to the peritoneal surfaces, leading to less inflammation and fibrin deposition6,7.
The clinical presentation of patients with ASBO is similar to that of SBO of other causes, ranging from mild to severe central abdominal pain/cramp with progressive worsening, emesis, abdominal distension, and constipation/obstipation in cases of complete obstruction. Peculiar to ASBO is that patients will have a history of previous abdominal or pelvic surgeries for a similar or related disease1,4.
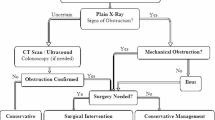
The management of adhesive SBO is based on the patient’s condition on clinical evaluation, laboratory investigations, and specific imaging studies. The choice between initial operative or non-operative treatment of SBO is usually controversial because surgical treatment may seem like a paradox, as it may be the source of new adhesions, and conversely, successful conservative treatment may leave adhesions that could cause recurrence8. Studies indicate that 70% to 80% of adhesive small bowel obstruction (ASBO) cases can be effectively managed through conservative treatment5,8. This approach typically includes the use of a nasogastric tube, intravenous fluids, analgesics, regular monitoring, and correction of any electrolyte imbalances8. In the absence of symptoms such as peritonitis, ischemia, or strangulation, initial conservative treatment is considered safe and successful in up to 70% to 90% of all ASBO episodes5,9,10,11.
From a global perspective, conservative management of ASBO is notably effective, particularly in developed countries7,12,13,14,15,16,17,18,19. Even in some developing nations, higher success rates have been reported. For instance, a study in Bangladesh reported a 72% success rate, which remained unaffected by the number of previous attacks20.
There is limited published data on the success of conservative management of ASBO in Ethiopia, with notable research only from Nekemte hospital21. Despite being a leading cause of mechanical SBO, the success rate of conservative management was notably low in this study compared to global studies for reasons that remain unclear21.
Conservative management of ASBO is advantageous for reducing morbidity, mortality, and hospital stays, especially in cases without peritonitis, bowel ischemia, or closed-loop obstruction1. A study indicated that average hospitalization after surgery for ASBO is 16 days, compared to 5 days for non-operative treatment, with an in-hospital mortality rate of 3%22.
Adhesive small bowel obstruction is by far one of the most common causes of SBO in our setup21. Despite the significant impact and challenges posed by the issue, no studies have been conducted in DCSH or in other regions of the country to determine the actual success rate of conservative management, its associated factors, and the optimal timing for implementing such management.
This study will provide insights into the effectiveness of non-operative management and the factors that can either enhance or hinder the success rate. By doing so, we hope to minimize the risk of complications related to surgery in appropriately selected cases.
Additionally, this study will be valuable for health program managers, health ministries, and regional health bureau personnel. It will help them emphasize the need for resources and support necessary for the successful management of ASBO, which can ultimately reduce the costs associated with surgery and extended hospital stays.
This study aimed to determine the success rate and associated factors with the conservative management of ASBO among patients admitted to DCSH from 2021 to 2023.
Methods and materials
Study area and period
The study was conducted at Dessie Comprehensive Specialized Hospital (DCSH), which is located 401 km northeast of Addis Ababa and 480 km southwest of Bahirdar, in South Wollo Zone, Amara regional state, Ethiopia. DCSH serves over 8 million people from the Afar, Amhara, and Tigray regions. As the area’s largest and oldest public hospital, it trains medical students and residents in collaboration with Wollo University. The hospital has 494 adult inpatient beds, including 80 in the surgical ward, four intensive care unit beds, and around 650 staff members. Medical personnel include 15 general surgeons, five general practitioners, two neurosurgeons, 20 nurses, 40 surgical residents, and 10 interns. With four operating rooms, the hospital performs an average of 4,866 major surgeries annually, along with a minor operation room. The study reviewed patient card registry data from June 1, 2021, to July 30, 2023.
Study design
A retrospective chart review was conducted to assess the success rate of conservative management and factors associated with the management outcome of patients admitted with ASBO at DCSH.
Population
Source population
All adult emergency ASBO patients in the department of surgery at DCSH from June 1/2021-July 30/2023G.C.
Study population
All adult ASBO patients managed conservatively at DCSH from June 1/2021-July 30/2023G.C.
Sample size
The sample size was estimated by the single proportion formula.
n- The initial sample size required.
p- prevalence of ASBO =35%(From Nekemte hospital, Ethiopia).
d- The margin of sampling error tolerated mostly 5% (0.05).
z- Standard normal variable at 95% confidence level (1.96)
n = 350.
The final sample size was 350 for both the first and the second outcomes.
Sampling technique
A computer-generated simple random sampling method was used to study all patients admitted for ASBO in DCSH during the specified time period.
Inclusion and exclusion criteria
Inclusion Criteria.
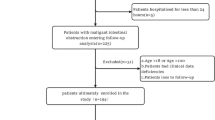
This study included all patients admitted to Dessie Comprehensive Specialized Hospital (DCSH) between January 1, 2021, and July 30, 2023 G.C. with a diagnosis of adhesive small bowel obstruction (ASBO) who were considered eligible for an initial trial of conservative (non-operative) management. Eligibility for conservative treatment was determined based on clinical stability and the absence of features suggesting complicated obstruction, in line with established surgical guidelines. Patients were required to have no evidence of bowel strangulation, perforation, generalized peritonitis, or other conditions mandating immediate surgical intervention at the time of presentation.
Exclusion Criteria.
Patients were excluded if they met any of the following conditions:
-
1.
Direct indications for urgent laparotomy on presentation, including signs of peritonitis (e.g., rebound tenderness, guarding), hemodynamic instability, radiologic evidence of perforation, or clear signs of bowel ischemia or gangrene.
-
2.
Pediatric patients under 14 years of age, as their pathophysiology, management protocols, and outcomes differ from those of the adult population.
-
3.
Incomplete clinical documentation or missing medical charts, which precluded accurate data extraction for study variables.
-
4.
Loss to follow-up during hospitalization, including patients transferred to other facilities before completion of the conservative management trial.
This approach ensured that the study cohort represented a uniform population of adult ASBO cases in whom conservative management was an appropriate initial therapeutic option, allowing for meaningful assessment of its success rate and associated factors.
Study variables
Dependent variable
-
Outcome of conservative management of patients with ASBO.
Primary outcome
A good outcome after conservative management is defined by the successful resolution of obstruction symptoms, which include abdominal pain, distention, and nausea or vomiting. Additionally, it involves the return of normal bowel function, characterized by the passage of feces and gas (flatus). There should also be no signs of strangulation or peritonitis; this means that symptoms such as fever, rapid heart rate (tachycardia), severe abdominal pain, or peritoneal signs like guarding and rebound tenderness should be absent.
Independent variables
Sociodemographic variables
Age; Sex; Religion.
Clinical variables
Type of previous surgery (colorectal surgery, appendectomy, gynecologic surgery); Number of prior surgeries; Duration of the illness; Comorbid conditions; NGT output; Small bowel dilatation; Absence of gas in the large bowel; Duration of follow-up for conservative management; Intraoperative finding.
Data collection tools
Patients’ card numbers were retrieved from the morning morbidity and mortality registry, and the patients’ cards were collected from the record office using their medical record numbers. Patients’ data were then extracted from their medical records (case files).
Sampling technique and procedure
Data was collected using a systematically structured data checklist in English by five trained junior residents, and completeness was verified after completing each checklist.
Data quality assurance
Training for data collectors was conducted over 2 days, focusing on the study’s purpose, checklist completion, and data quality. To minimize variation, the same data collectors gathered data throughout the study, with daily supervision to ensure consistency and completeness.
Data analysis and presentation
Data were checked for completeness and entered into SPSS 27.0, where frequency and percentages for key variables were calculated. The regression analysis model fit was perfect (Nagelkerke R square = 1), with no issues of multicollinearity (VIF < 10; average VIF = 1.68). Logistic regression was used to assess the association between dependent and independent variables, with p < 0.05 considered statistically significant. Results are presented in tables, graphs, and narrative form, followed by conclusions and recommendations.
Ethical consideration
Ethical clearance was obtained from the Institutional Review Board (IRB) at Wollo University College of Medicine and Health Sciences. Written consent was also obtained from the records office department to collect patient cards. The information gathered from these patient cards during data collection was kept confidential by assigning codes to each card throughout the study.
Definitions
Conservative management: patients managed nonoperatively with one or more of the following: IV fluids, electrolyte supplementation, NG tube decompression, and close follow-up19, but omits WSCS as it isn’t available in our setup.
The duration of symptoms:
the time span between the initial pain perception due to IO and the visit to the hospital.
Small bowel dilatation:
small bowel diameter > 3 cm on plain abdominal X-ray.
Distal bowel gas:
presence of air in the colon/rectum on plain abdominal X-ray.
A good outcome after Conservative management of ASBO:
defined by the successful resolution of obstruction symptoms, which include abdominal pain, distention, and nausea or vomiting. Additionally, it involves the return of normal bowel function, characterized by the passage of feces and gas (flatus). There should also be no signs of strangulation or peritonitis; this means that symptoms such as fever, rapid heart rate (tachycardia), severe abdominal pain, or peritoneal signs like guarding and rebound tenderness should be absent.
Results
Sociodemographic factors
The study included 350 charts of conservatively managed cases of adhesive small bowel obstruction at DCSH, predominantly involving young adult males (80.6%) and Muslims (65.4%) (see Table 1).
Major causes and the success rate of conservative management of ASBO in DCSH, from 2021 to 2023 G.C.
The most common cause identified was laparotomy for various causes in 55.7% of the cases, and the majority of them had the index operation within 1–12 months(45.7%), as depicted in Table 1 (Table 1).
The success rate of conservative management was observed in 158 out of 350 cases. All patients were treated with nothing by mouth (NPO), NGT decompression, and intravenous crystalloid fluids, primarily normal saline. None of the patients received electrolyte supplementation, as routine serum electrolyte determination is not standard practice in our facility.
Most cases (86%) responded to conservative management within the first 72 h. Specifically, 69 cases (43.6%) responded within 24 to 48 h, and 67 (42.4%) responded between 48 and 72 h.
Patients who effectively responded to conservative management had a daily NGT output of less than 300mL. Conversely, none of the 53 cases (15%) with an NGT output greater than 300 mL responded favorably to conservative management. Similarly, all 18 cases (5%) with more than one index operation as the cause of adhesive small bowel obstruction (ASBO) failed to respond to this management approach. Notably, the presence of comorbidities did not impact the response to conservative treatment (see Table 2).
Factors associated with the success rate of Conservative management of ASBO in DCSH, Ethiopia 2021-2023G.C
This study showed that the odds of success rate of conservative management for ASBO was higher in patients who had no similar episode of the same illness than those who had [AOR(95%C.I) = 42.995(9.811-188.067)]. Similarly, the odds of success rate for conservative management was significantly higher [AOR(95%C.I) = 9.250(1.701–50.295)] in patients who presented with a total duration of the current illness 24–48 h than those who came after 72 h of the start of the illness. The success rate was also higher ([AOR(95%C.I) = 21.803(2.872-165.533)], [AOR(95%C.I) = 6.541(1.117–38.304)], and [AOR(95%C.I) = 31.997(4.391-232.886)]) in patients having their index surgery less than one month, 1–3 years and 3–10 years before the development of ASBO, respectively than those whose index operation was greater than 10 years. The study also showed that patients having obstipation on history were less likely to respond to conservative management than those who were not obstipated[AOR (95%C.I) = (0.002[0.000-0.009)].
Likewise, the absence of distal bowel gas on plain abdominal X-ray was a significant risk factor for success rate of conservative management on bivariable logistic regression [COR(95%C.I) = 5.173(2.766–9.675), p-value < 0,001] but was not found to be significant on multivariate analysis (see Table 2).
Discussions
Our study found a modest proportion of good outcome (45%) after conservative management of small bowel obstruction (SBO) caused by post-operative adhesions. This rate is significantly higher compared to a study conducted at Nekemte Referral Hospital in the eastern part of Ethiopia21. The difference in success rates may be attributed to the characteristics of the studies; our research focused exclusively on patients with post-operative adhesions as the sole cause of SBO, while the Nekemte Referral Hospital study included patients with SBO from various causes. Other factors, such as the sociodemographic characteristics of the cases studied, the type and timing of the initial operation, the duration of conservative management before classifying it as a failure, and the type of management used, may also have contributed to the significant gap in the success rate.
However, this study’s success rate is significantly lower than most studies outside Ethiopia23. For example, it is almost half the success rate reported in large-scale studies done in Canada8, China7, Singapore3, and Bangladesh20, which can mainly be attributed to the type of index operation (the adhesion tissue could be limited because of limited and localized peritoneal injury in these studies as most of the surgeries are undertaken laparoscopically as compared to our setup where we are using the open approach for every surgical case) and the use of WSCS which has a significant role in the conservative management of ASBO: increasing the success rate and decreasing the need for surgery as the study conducted in China7. WSCS is currently not utilized and is unavailable in our setup, potentially limiting our success rate for the conservative management of ASBO.
The difference in sociodemographic characteristics of the studied cases could have also played a role in this discrepancy in outcome. For instance, in this study, we excluded pediatric ASBO cases that likely have different biological responses to peritoneal injury and, hence, different adhesion formation and physiology compared to the adult population. The dietary and bowel habit of the studied cases is another example to this regard.
In our cohort, two bedside features stood out for predicting the course of adhesive small-bowel obstruction (ASBO): a history of multiple prior operations and the presence of obstipation. This aligns with contemporary understanding that prior surgery increases adhesion burden and complexity, thereby lowering the likelihood of spontaneous resolution; several real-world and model-based studies now incorporate prior operative history among variables used to predict non-operative management (NOM) failure or strangulation risk24. In addition, recent data suggest that the type of previous operation alone does not reliably determine the need for surgery in an SBO admission, highlighting that it is probably the cumulative adhesion load, not merely operative category, that drives outcomes25.
Generally, in this study, the absence of previous similar illnesses, absence of obstipation, early patient presentation, and having their index surgery/surgeries less than a year of the current complaint were significant associated factors for the success rate of conservative management of ASBO.
Like a study conducted in China15, other variables such as sex, age, number of previous abdominal operations, and maximal diameter of the small bowel on admission were not associated with failed conservative management. However, unlike the study conducted in China, our study showed that a history of previous adhesive small bowel obstruction and the duration of symptoms before admission were significantly associated with the success rate. Again, contrary to this study, our study revealed that the amount of daily NGT output didn’t affect the success rate.
Unlike the study conducted in Bangladesh, which showed that the success rate of conservative management was not affected by the number of previous attacks20, the success rate of conservative management in this study was affected by the number of previous surgeries as none responded for conservative management among those cases having greater than or equal to two operations, although the number of prior surgeries was not found to be significant on bivariable logistic regression analysis.
Our study also showed that patients having obstipation on history were less likely to respond to conservative management than those who were not obstipated, which could be explained by the difference in the severity of obstruction, meaning that obstipated patients had a more complete obstruction than those who were not and thereby decreasing the success rate of spontaneous resolution of the obstruction with conservative management.
Strengths and limitations of the study
Our study addresses a poorly explored issue in the Ethiopian context and will serve as a baseline for future research. However, it is important to note that this study was conducted only in our routine clinical setup at DCSH and did not include patients managed at other neighboring primary and general hospitals. Additionally, the data used were sourced from secondary sources, which may introduce bias or result in missing or incomplete information.
Conclusion
Although the success rate of conservative management of ASBO is good compared to the study in another part of the country, it is still very low compared to the global studies, where most were done in setups where WSCS is being used routinely.
The presence of similar episodes of the same illness, duration of the current illness, time of the index operation, and the length of conservative management were significantly associated with the success rate. On the other hand, obstipation significantly affected the success rate of conservative management.
Recommendations
For regional health bureau, FMOH, and DCSH administrators:
The Regional Health Bureau and FMOH should try to avail WSCS for clinical use in our setup, which could help predict the success rate of non-operative management of ASBO so that some unnecessary operations and/or unnecessary patient delays and their consequences can be avoided.
For DCSH surgeons, residents, interns, nurses, and other involved staff in the management of ASBO:
Patient evaluation (history, physical exam) should be adequate, and patient management should be tailored accordingly and timely, together with the available imaging and laboratory results, to avoid the grave complications of unnecessary surgery and unnecessary delay.
Researchers:
It will be imperative if future prospective studies are conducted to deal with the problem further by adding some essential variables and developing better outcomes.
Data availability
All generated and analyzed data is available upon request. The datasets created during the study are in the possession of the principal investigator (PI), S.A.A. For access to this information, please contact the PI directly at the following email address: setegnabebaw34@gmail.com.
Abbreviations
- AOR:
-
adjusted odds ratio
- ASBO:
-
Adhesive small bowel obstruction
- CI:
-
Confidence interval
- COR:
-
Crude odd ratio
- DCSH:
-
Dessie Comprehensive Specialized Hospital
- GIT:
-
Gastrointestinal tract
- IBD:
-
Inflammatory bowel disease
- IO:
-
Intestinal obstruction
- IPAA:
-
Ileal pouch-anal anastomosis
- IV:
-
Intra venous
- NIT/NGT:
-
Nasointestinal tube/Nasogastric tube
- PAI:
-
Peritoneal adhesion index
- SBO:
-
Small bowel obstruction
- VIF:
-
variance inflation factor
- WSCA/WSCS:
-
Water soluble contrast administration/study
References
Health Shackelford’s Surgery of the Alimentary Tract, 2 - 9780323402323. US Elsevier https://www.us.elsevierhealth.com/shackelfords-surgery-of-the-alimentary-tract-2-volume-set-9780323402323.html (accessed 2023-08-31).
Mu, J. F. et al. Clinical factors associated with intestinal strangulating obstruction and recurrence in adhesive small bowel obstruction. Med. (Baltim). 97 (34), e12011. https://doi.org/10.1097/MD.0000000000012011 (2018).
Tong, J. W. V., Lingam, P. & Shelat, V. G. Adhesive small bowel Obstruction - an update. Acute Med. Surg. 7 (1), e587. https://doi.org/10.1002/ams2.587 (2020).
Attard, J. A. P. & MacLean, A. R. Adhesive small bowel obstruction: epidemiology, biology and prevention. Can. J. Surg. 50 (4), 291–300 (2007).
Fugazzola, P. et al. Validation of peritoneal adhesion index as a standardized classification to universalize peritoneal adhesions definition. J. Peritoneum (and Other Serosal surfaces). 2 https://doi.org/10.4081/joper.2017.61 (2017).
Krielen, P. et al. Adhesive small bowel obstruction in the minimally invasive Era. In Intestinal Obstructions IntechOpen, (2020). https://doi.org/10.5772/intechopen.91896
Choi, H. K., Chu, K. W. & Law, W. L. Therapeutic value of gastrografin in adhesive small bowel obstruction after unsuccessful Conservative treatment. Ann. Surg. 236 (1), 1–6 (2002).
Behman, R. et al. Association of surgical intervention for adhesive Small-Bowel obstruction with the risk of recurrence. JAMA Surg. 154 (5), 413–420. https://doi.org/10.1001/jamasurg.2018.5248 (2019).
ten Broek, R. P. G. et al. Burden of adhesions in abdominal and pelvic surgery: systematic review and Met-Analysis. BMJ 347, f5588. https://doi.org/10.1136/bmj.f5588 (2013).
Stommel, M. W. J. et al. Multicenter observational study of adhesion formation after Open-and laparoscopic surgery for colorectal cancer. Ann. Surg. 267 (4), 743–748. https://doi.org/10.1097/SLA.0000000000002175 (2018).
van Steensel, S. et al. Adhesion awareness in 2016: an update of the National survey of surgeons. PLoS One. 13 (8), e0202418. https://doi.org/10.1371/journal.pone.0202418 (2018).
Jeong, W. K., Lim, S. B., Choi, H. S. & Jeong, S. Y. Conservative management of adhesive small bowel obstructions in patients previously operated on for primary colorectal cancer. J. Gastrointest. Surg. 12 (5), 926–932. https://doi.org/10.1007/s11605-007-0423-5 (2008).
Keenan, J. E. et al. Trials of nonoperative management exceeding 3 days are associated with increased morbidity in patients undergoing surgery for uncomplicated adhesive small bowel obstruction. J. Trauma. Acute Care Surg. 76 (6), 1367–1372. https://doi.org/10.1097/TA.0000000000000246 (2014).
Cox, M. R., Gunn, I. F., Eastman, M. C., Hunt, R. F. & Heinz, A. W. The safety and duration of Non-Operative treatment for adhesive small bowel obstruction. Aust N Z. J. Surg. 63 (5), 367–371. https://doi.org/10.1111/j.1445-2197.1993.tb00404.x (1993).
Dong, X. W., Huang, S. L., Jiang, Z. H., Song, Y. F. & Zhang, X. S. Nasointestinal tubes versus nasogastric tubes in the management of Small-Bowel obstruction: A Meta-Analysis. Med. (Baltim). 97 (36), e12175. https://doi.org/10.1097/MD.0000000000012175 (2018).
Fleshner, P. R. et al. Randomized trial of short versus long tubes in adhesive Small-Bowel obstruction. Am. J. Surg. 170 (4), 366–370. https://doi.org/10.1016/s0002-9610(99)80305-5 (1995).
Ceresoli, M. et al. Water-Soluble contrast agent in adhesive small bowel obstruction: A systematic review and Meta-Analysis of diagnostic and therapeutic value. Am. J. Surg. 211 (6), 1114–1125. https://doi.org/10.1016/j.amjsurg.2015.06.012 (2016).
Bueno-Lledó, J. et al. Adhesive small bowel obstruction: predictive factors of lack of response in Conservative management with gastrografin. Dig. Surg. 33 (1), 26–32. https://doi.org/10.1159/000441530 (2016).
Catena, F. et al. Adhesive small bowel adhesions obstruction: evolutions in diagnosis, management and prevention. World J. Gastrointest. Surg. 8 (3), 222–231. https://doi.org/10.4240/wjgs.v8.i3.222 (2016).
Mohibul Hassan, Md., Paul, S. C., Sarkar, A. & Sarker, S. Outcome of conservative approach in the management of postoperative adhesive small bowel obstruction. IOSR J. Dent. Med. Sci. 18(3), 32–36. https://doi.org/10.9790/0853-1803013236 (2019).
Jemere, T., Getahun, B., Tesfaye, M., Muleta, G. & Yimer, N. Causes and management outcome of small intestinal obstruction in Nekemte Referral Hospital, Nekemte, Ethiopia, 2017. Surg. Res. Pract. 2021, 9927779. https://doi.org/10.1155/2021/9927779 (2021).
Ten Broek, R. P. G. et al. Bologna guidelines for diagnosis and management of adhesive small bowel obstruction (ASBO): 2017 update of the Evidence-Based guidelines from the world society of emergency surgery ASBO working group. World J. Emerg. Surg. 13, 24. https://doi.org/10.1186/s13017-018-0185-2 (2018).
Shen, C. J. & Wang, J. J. Advancements in the clinical management of adhesive small bowel obstruction: A perspective. Med. (Baltim). 104 (27), e43246. https://doi.org/10.1097/MD.0000000000043246 (2025). PMID: 40629606; PMCID: PMC12237302.
Amara, Y. et al. Diagnosis and management of small bowel obstruction in Virgin abdomen: a WSES position paper. World J. Emerg. Surg. 16 (1), 36. https://doi.org/10.1186/s13017-021-00379-8 (2021). PMID: 34217331; PMCID: PMC8254282.
Van Horn, A. L., Soult, A. P., Sternick, M. E., Sturm, E. L. & Britt, R. C. Type of prior operation does not predict surgical intervention for small bowel obstruction. Am. Surg. 90 (7), 1896–1898 (2024). Epub 2024 Mar 26. PMID: 38532245.
Acknowledgements
The authors express their deepest gratitude to the Department of Surgery and the School of Public Health for their unwavering support and dedication.
Funding
Not Applicable.
Author information
Authors and Affiliations
Contributions
S.A.A conceived and designed the study, writing review and editing original draft, formulated the study design, data quality check, performed statistical analysis, and drafted initial manuscript. A.A.A, A.E, and A.N.A contributed to the literature review, and manuscript revision. S.M contributed to the editing of the original document and the revision of the manuscript. S.A.A and S.M contributed to the conception, revised data extraction sheet, collected patient data, reviewed, and interpreted the data, and revised the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study was approved by the Institutional Health Research Ethics Review Committee of the College of Health and Medical Sciences, Wollo University (Ref No: IHRERC/056/2024) and informed consent was obtained from all patients and/or their legal guardian(s). The research was conducted in full compliance with the principles outlined in the Declaration of Helsinki, ensuring ethical standards and the well-being of all participants were prioritized. This is an observational study that does not assign participants to an intervention or evaluate the effect of an intervention on them.
Consent for publication
Not Applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Abera, S.A., Adem, A.A., Endawkie, A. et al. Success rate and associated factors of conservative management of adhesive small bowel obstruction at Dessie comprehensive specialized hospital, Northeast Ethiopia. Sci Rep 15, 36570 (2025). https://doi.org/10.1038/s41598-025-20288-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-20288-z
