
Abstract
Global warming is intensifying heat risks globally, yet understanding of these rising risks on a global scale remains limited. We introduce a standardized heat-sensitivity indicator (ΔRR)—the change in relative risk (RR) per 1 °C above the minimum mortality temperature (MMT)—which enables like-for-like comparisons across heterogeneous city studies. Using ΔRR, we quantify how sensitively heat-related mortality responds to incremental warming rather than only to extremes. This study reveals that over a latitude of around 40°N, development inequality disrupts the patterns of heat risk variability, and high-risk cities primarily cluster in ranges with temperatures between 10 °C and 22 °C. These findings emphasize the urgent need for more focus on cities in temperate zones. Our results also position ΔRR as a transferable metric for global surveillance, comparison, and planning of heat-health adaptation.
Similar content being viewed by others

Introduction
As global temperatures continue to rise under the influence of climate change, significant burdens on health and exacerbations of inequality are projected worldwide1,2. From a geographical perspective, large-scale studies for heat-related risks predominantly focus on aspects such as population exposure and heat stress, often overlooking the influence of socio-economic developments on enhancing resilience against risks3,4. This oversight might introduce biases for understanding heat-related risk change, given the broad range of factors influencing risk (e.g., individual and environment)5. Meanwhile, in the medical health domain, the relative risk (RR) of death is a commonly used metric for studying temperature-related risks at specific locations6,7. The RR is generally defined as the relative risk that describes the increase in cumulative mortality risk as temperatures rise above the minimum mortality temperature (MMT)8, and is widely used to measure the association between mortality and heat exposure epidemiologically9,10. Notably, the MMT used as the baseline data for RR calculation varies with latitude, as has been agreed upon11,12.
Therefore, most of these studies with RR predominantly focus on specific cities or regions, examining the local variations in risk with changing temperatures. Although there are noticeable differences in the change pattern of RR for different cities or regions, the lack of standardized metrics hinders the risks’ comparison among cities or regions. This limitation also results in a fragmented understanding of the mechanisms driving global changes in relative risk. To overcome the limitation of lacking standardized risk metrics between regions, we employ RR changes per increasing 1 °C, denoted as ΔRR, to explore globally variability of heat death relative risk (see methods section for detailed calculations). Unlike most existing studies that focus on extreme temperature events, this study emphasizes the effects of general background warming and long-term shifts in heat-related mortality sensitivity across cities.
Although some research has used RR-derived metrics to explore global or intercontinental variations in heat-related mortality risk among cities2,13, these studies do not adequately capture the diverse responses to heat under global warming scenarios. Specifically, Vicedo-Cabrera et al.2 considered the cumulative relative risk up to the 99th percentile of warm-season temperatures, potentially leading to an overestimation of risk, while Kephart et al.13 focused on heat-related mortality per 1 °C increase above the 95th percentile of daily temperatures, without considering temperatures below extreme thresholds. However, recent research has demonstrated that normal weather or climate changes should be given sufficient attention except for extreme weather14. Our approach extends beyond extreme temperatures to encompass the impacts of overall temperature increases across all ranges.
This study aims to provide novel insights into the global geographical disparities in risk escalation associated with each degree of temperature increase, as well as its primary influencing mechanism. Specifically, we utilized the Human Development Index (HDI) for various regions—a composite measure encompassing life expectancy, educational attainment, and GDP—to represent developmental disparities across different geographical areas15. By integrating data on HDI, temperature, and latitude, we investigated the variability patterns of ΔRR and explained how these patterns are influenced by developmental inequalities and climate factors. This analysis not only facilitated the examination of ΔRR variability from southern to northern latitudes but also enabled a comprehensive understanding of how global development inequalities modulate ΔRR. Consequently, our study is poised to significantly enhance the current understanding of the intricate interplay between climate-induced health risks and socioeconomic factors.

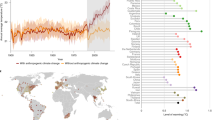
ΔRR with latitudes at Northern Hemisphere.
Latitudinal variation in ΔRR and development disparity
According to the definition of ΔRR, it is generally believed that as temperatures decrease and latitudes increase, ΔRR should rise, like Liu et al.11 found MMT fall. Because residents in colder regions may not be well-adapted to temperature increases. This phenomenon can be attributed to differences in climate adaptation and physiological responses across latitudes16. This means that in colder regions, a 1 °C rise in temperature poses a greater health risk compared to warmer areas. Conversely, inhabitants of relatively warmer regions are exposed to hot conditions year-round, making them more acclimated and less vulnerable to similar temperature changes11. It was found that high-latitude regions exhibit greater sensitivity to high temperatures compared to mid-latitude regions17. Therefore, from a geographical perspective, ΔRR is generally expected to increase with latitude.
However, in this study the trend of ΔRR variation in the northern hemisphere shows an unexpected pattern above 40°N, where ΔRR starts to shift from increasing to decreasing with latitude increase (Fig. 1). To investigate this, we categorized the studies into two groups based on the UNDP-defined four-tier HDI classification, separating only the “very high development” group (HDI ≥ 0.8) and combining the other levels (high, medium, and low) as “non–very high development”. Our analysis indicates an obviously increased proportion of studies from very high development regions above 40°N, whereas below this latitude, the proportion from non-very high development regions increases (Fig. 1). Therefore, we believe that development inequality may disrupt the variability patterns of ΔRR in the north-south spatial gradient, as higher development levels could enhance the capability to mitigate heat-related risks.
Experts in relevant fields have found that global warming will increase economic inequality18. This is because extreme heat results in more severe economic losses in poorer regions, whereas richer regions, such as Europe, may experience less economic loss or even economic growth19,20. Previous experience has shown a non-linear relationship between economic growth and temperature that first increases and then decreases with temperature19. Increasing temperatures below the optimal threshold (about 13 °C) has a positive effect on labor supply, productivity, and crop yields, contributing to economic production. However, continuous temperature increases above the optimal threshold have a negative impact on these factors19. Consequently, for cooler or colder high-latitude regions, warming climates are likely to contribute to economic growth, while hot and arid low-latitude regions face more economic losses18,19. Our aggregated studies’ data on ΔRR on latitudes and HDI show that the regions in hot and arid low-latitude regions tend to have a non-very high development level, while very high development areas are mainly in cooler or colder mid- and high-latitude regions (Fig. 1). This could lead to a severe scenario in which rich regions could loss less even benefit from global warming while poor regions suffer more as a result.

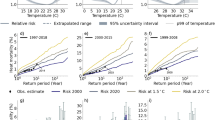
The relationship between average temperature and Human Development Index for specific study period, and the corresponding ΔRR in these cities (a). (b,c) the cities of top nine ΔRR values with below 10 °C (b), 10–22 °C (c), and above 22 °C (d).
Temperature-zone heterogeneity in risk sensitivity
In terms of temperature, Fig. 2a shows a relationship between temperature and HDI, where HDI increases and then decreases as temperature rises, forming an inverted U-shape. This pattern is consistent with the findings of Burke et al.19, which highlight the negative impact of temperatures above a certain threshold on economic development and human well-being. While Burke et al.19 suggest this threshold to be 13 °C, our analysis proposes a threshold of approximately 10 °C. In conjunction with the distribution of ∆RR, in this study we divided the temperatures into three distinct ranges: below 10 °C, 10–22 °C, and above 22 °C (Fig. 2). This categorization allows for a more detailed analysis of the temperature effects on HDI and heat-related risks.
In cities where the average temperature for specific study period falls below 10 °C (Fig. 2b), an increase in temperatures below the optimal threshold (approximately 13 °C) has been shown to positively impact economic development according to Burke et al. 20. Therefore, these cities (Fig. 2b), predominantly in temperate and polar zones, exhibit relatively lower ΔRR values, indicating a smaller increase in heat-related mortality risk per degree rise in temperature. This indicates that in these temperature zones, economic development tends to be the dominant factor influencing ΔRR.
In cities with average temperatures ranging from approximately 10 °C to 22 °C, recognized as temperate climate zones21, high ΔRR values are almost concentrated in this temperature range (Fig. 2c). These temperate zone cities show higher ΔRR values compared to cooler regions, indicating a greater sensitivity to temperature increases. The climate in temperate zone is generally more conducive to human habitation22,23, but the combination of favorable climatic conditions, economic opportunities, and historical patterns of human settlement adds to the complexity24, leading to a more compound influence of temperature and human activities on heat-related risks in this area. For example, in temperate regions, long-term human settlement and economic concentration have led to high population density24. At the same time, future urban expansion and the resulting warming will significantly increase heat exposure risks25. Although temperate cities as a whole have higher income and better infrastructure, there are clear inequalities in adaptive capacity across regions (Fig. 2a). In addition, residents in temperate zones have less historical experience with extreme heat, which means limited physiological adaptation and risk perception. Moreover, high temperatures have not traditionally been a central concern in urban planning, and many infrastructures were not originally designed to cope with frequent extreme heat, resulting in weaker technical adaptive capacity. Thus, ΔRR values in this temperature range exhibit chaotic variability with temperature and HDI (Fig. 2c), concentrating almost all high-risk cities, though there are some low-risk cities as well.
In cities where temperatures exceed 22 °C, recognized as tropical climate zones26, the ΔRR is predominantly represented by blue dots, signifying relatively lower ΔRR values compared to the temperate zone (Fig. 2d). This observation suggests that human adaptability to high temperatures, where physiological adjustments play a significant role, might be the predominant factor influencing ΔRR in these areas, even though the low HDI and complex human activities in some cities (e.g., Bangkok9 (Fig. 2).
Our findings highlight that temperate-zone cities, with 10 °C to 22 °C temperature range, are facing a more serious threat from rising heat-related mortality, given the significant human activities and the complex interaction of factors in this area. Therefore, temperate-zone cities should receive increased attention concerning the rising heat risks associated with global warming.
Discussion and limitations
Previous studies have contributed significantly to understanding how climate and economic development influence the health impacts of temperature exposure27,28. Building on this foundation, our study adds two important extensions. First, we introduce the ΔRR indicator to standardize and quantify the sensitivity of heat-related mortality risk across a global set of cities. Previous studies often relied on region-specific models to estimate exposure–response functions, making cross-regional comparisons difficult due to differences in model structures and assumptions. Moreover, most existing studies have emphasized the absolute magnitude of heat-related mortality risk, while the dimension of sensitivity remains relatively understudied. Second, we apply the ΔRR metric to investigate how development inequality modifies the spatial gradient of risk sensitivity. Our findings reveal that cities in the temperate zone (10–22 °C), despite having generally favorable climatic conditions, exhibit the most rapid increases in heat-related mortality risk. This finding suggests that the interaction between economic development and climate conditions produces a complex and nonlinear pattern of risk sensitivity at the global urban scale. These findings offer new insights for macro-scale analyses of climate-related health risks and adaptation planning.
Additionally, we acknowledge that the ΔRR indicator represents a linear approximation between MMT and extreme heat, which cannot fully capture the complex, nonlinear shape of the temperature–mortality relationship. This simplification was necessary to enable standardized comparisons across heterogeneous studies in a meta-analytic framework. Nevertheless, future studies with access to full exposure–response data should consider modeling the full curve to better reflect the dynamics of heat-related mortality risks.
Although our analysis reveals clear spatial patterns of ΔRR, the low goodness-of-fit of regression curves and potential omitted macro-scale variables (e.g., regional climate, topography, coastal proximity) suggest caution in interpreting causal links. In terms of modeling strategy, while we used polynomial regression for consistency and interpretability across analyses, we acknowledge that nonparametric methods may better capture localized nonlinearities and reduce sensitivity to outliers. Future studies may explore these approaches when working with larger or more balanced datasets. With respect to climatic characterization, although both latitude and multi-year average daily temperature were used to characterize spatial and climatic patterns, these indicators do not fully capture the heterogeneity of local climate. Future research could improve upon this by incorporating more refined climate metrics, such as degree-days, seasonal humidity, or bioclimatic classifications, which may better represent environmental exposure. While we used HDI to represent developmental differences, additional physical factors related to HDI may also influence the sensitivity of heat-related mortality. For example, coastal regions may benefit from oceanic moderation effects, and high-altitude cities may experience different thermal exposures. Future studies should incorporate high-resolution covariates and spatial modeling to address these uncertainties and better isolate the underlying mechanisms.
This study is constrained by the uneven distribution of sample cities, especially the underrepresentation of low-HDI and tropical regions. This limitation arises mainly from data availability issues rather than selection bias. As a result, the ΔRR pattern reported here may not fully reflect the global landscape. Future research should strive to improve epidemiological data coverage in these regions to enable more complete and representative global assessments.
The temperature intervals (< 10 °C, 10–22 °C, > 22 °C) were selected based on both climatic and socioeconomic considerations. The < 10 °C and > 22 °C thresholds approximately align with the Köppen–Geiger climate classification system, which distinguishes between temperate climate subtypes (Kottek et al., 2006). Although this system does not explicitly define a 10–22 °C range, the chosen thresholds reflect common climatic transitions across temperate regions. Additionally, the central range near 13 °C aligns with the global productivity optimum reported by Burke et al. (2015). This classification provides a consistent and interpretable framework for examining ΔRR variability across different climate and development contexts.
In summary, this study introduces a standardized ΔRR metric to evaluate spatial disparities in heat-related mortality sensitivity. The findings demonstrate how development inequality and climatic context jointly shape structural heat risk, contributing to the broader field of climate-health research. While acknowledging limitations such as uneven sample distribution and the exclusion of certain environmental variables, the proposed approach offers a foundation for future risk assessments and climate adaptation planning. Moreover, the study underscores the disproportionate vulnerability of temperate-zone cities and highlights the importance of high-resolution demographic and environmental data for advancing more mechanistic and integrated global risk analyses.
Materials and methods
Literature search and data collection
A comprehensive literature search was firstly conducted using the Web of Science database with the keywords (Extreme heat OR Extreme temperature OR Heat) AND (Heat vulnerability OR Heat-related mortality) AND Human. We did not isolate extreme events, but instead standardized ΔRR as a general response to temperature elevations above the MMT threshold. The search aimed to identify epidemiological studies reporting quantitative risk associations between high temperatures and all-cause mortality. As of September 2022, 63 publications met the inclusion criteria and were included in the study. All included references are listed in Supplementary Table S1.
Data extraction and standardization
For each publication, we extracted data on study location, study period, minimum mortality temperature (MMT), extreme heat (EH) temperatures, and the corresponding heat-related mortality relative risk (RR) data at extreme temperatures. To maximize the collection of available urban data and expand the sample size, we gathered the temperatures corresponding to the 95th percentiles or 99th percentiles as appropriate. For studies involving multiple locations, we collected results for all different study sites. For studies covering single locations over multiple periods, we collected results for all distinct study periods. Ultimately, 163 original records meeting the criteria were collected as samples. To make these sample data comparable, the study designed a new standardized heat-related mortality risk indicator, ΔRR, defined as the change in RR per 1 °C, calculated using the following equation:
where \(\:{RR}_{{Temp}_{EH}}\) represents the accumulated heat mortality RR at extreme temperatures. RRMMT, the relative risk at the minimum mortality temperature, is treated as the reference value and typically set to 1 to ensure standardization across studies. MMT is the minimum mortality temperature, which varies for each location. This new data, ΔRR, allows us to analyze the differences in the increased heat-related mortality risk faced by different cities globally.
Statistical analysis
For each record with ΔRR, we calculated the HDI and average temperatures for the corresponding study period. For HDI data, mean annual HDI data were derived from the gridded global datasets published by Kummu et al.15. Using the center coordinates of the study locations, we extracted the corresponding HDI data and calculated the average HDI for the study period. For average temperature data, we used daily mean temperature time series from the National Oceanic and Atmospheric Administration (NOAA) (https://www.ncdc.noaa.gov/) to calculate the multi-year average temperature during the study period. We note that these values do not represent standardized 30-year climatological normals, but rather reflect typical temperature conditions during the time frame of each individual study.
This enabled us to plot scatter of ∆RR original samples and average ∆RR for each 4-degree latitude band against latitude. Polynomial regression was employed to fit the trend and analyze the north-south gradient of ∆RR. We integrated Human Development Index (HDI) data to assess the development level of regions within each latitude band (developed vs. underdeveloped regions) and its impact on ∆RR (Fig. 1). Here, latitude was used solely to group cities into 4-degree bands for examining spatial gradients, rather than being treated as a climate variable.
Scatter diagrams of average HDI against average temperature for the ∆RR samples were plotted. Polynomial regression was used to fit the trend, and point markers were assigned colors and sizes based on their ∆RR values. This approach allowed us to explore the compound influence of socioeconomic and temperature rises on ∆RR, identifying key city types that require attention for heat-related risk management.
Data availability
The datasets used and analyzed during the current study available from the corresponding author on reasonable request.
References
Alizadeh, M. R. et al. Increasing heat-stress inequality in a warming climate. Earths Future. 10, e2021EF002488 (2022).
Vicedo-Cabrera, A. M. et al. The burden of heat-related mortality attributable to recent human-induced climate change. Nat. Clim. Change. 11, 492–500 (2021).
Tuholske, C. et al. Global urban population exposure to extreme heat. Proc. Natl. Acad. Sci. USA 118, e2024792118 (2021).
Vecellio, D. J., Kong, Q., Kenney, W. L. & Huber, M. Greatly enhanced risk to humans as a consequence of empirically determined lower moist heat stress tolerance. Proc. Natl. Acad. Sci. USA 120, e2305427120 (2023).
Guo, Y. et al. Extreme temperatures and mortality in Latin america: voices are needed from the global South. Med 3, 656–660 (2022).
Gasparrini, A. et al. Small-area assessment of temperature-related mortality risks in England and wales: a case time series analysis. Lancet Planet. Health. 6, e557–e564 (2022).
Psistaki, K., Dokas, I. & Paschalidou, A. Analysis of the heat-and cold-related cardiovascular mortality in an urban mediterranean environment through various thermal indices. Environ. Res. 216, 114831 (2023).
Gasparrini, A. Modeling exposure–lag–response associations with distributed lag non-linear models. Stat. Med. 33, 881–899 (2014).
McMichael, A. J. et al. International study of temperature, heat and urban mortality: the ‘ISOTHURM’ project. Int. J. Epidemiol. 37, 1121–1131 (2008).
Schmidt, C. O. & Kohlmann, T. When to use the odds ratio or the relative risk? Int. J. public. Health. 53, 165 (2008).
Liu, J. et al. Is there an association between hot weather and poor mental health outcomes? A systematic review and meta-analysis. Environ. Int. 153, 106533 (2021).
Yin, Q. et al. Mapping the increased minimum mortality temperatures in the context of global climate change. Nat. Commun. 10, 4640 (2019).
Kephart, J. L. et al. City-level impact of extreme temperatures and mortality in Latin America. Nat. Med. 28, 1700–1705 (2022).
Ballester, J. et al. Heat-related mortality in Europe during the summer of 2022. Nat. Med. 29, 1857–1866 (2023).
Kummu, M., Taka, M. & Guillaume, J. H. A. Gridded global datasets for Gross Domestic Product and Human Development Index over 1990–2015. Dryad (2020). https://doi.org/10.5061/dryad.dk1j0
Curriero, F. C. et al. Temperature and mortality in 11 cities of the Eastern united States. Am. J. Epidemiol. 155, 80–87 (2002).
Fan, Y. & Im, E. S. A comparative assessment of changes in Heat-Related mortality risk under the RCP2. 6 and RCP8. 5 scenarios based on the CORDEX-CORE ensembles. Asia-Pac. J. Atmos. Sci. 59, 207–218 (2023).
Diffenbaugh, N. S. & Burke, M. Global warming has increased global economic inequality. Proc. Natl. Acad. Sci. USA 116, 9808–9813 (2019).
Burke, M., Hsiang, S. M. & Miguel, E. Global non-linear effect of temperature on economic production. Nature 527, 235–239 (2015).
Callahan, C. W. & Mankin, J. S. Globally unequal effect of extreme heat on economic growth. Sci. Adv. 8, eadd3726 (2022).
Kottek, M. et al. World map of the Köppen-Geiger climate classification updated. Meteorol. Z. 15, 259–263 (2006).
Klinger, B. A. & Ryan, S. J. Population distribution within the human climate niche. PLOS Clim. 1, e0000086 (2022).
Xu, C. et al. Future of the human climate niche. Proc. Natl. Acad. Sci. USA 117, 11350–11355 (2020).
Rae, A. & Mapped The world’s population density by latitude. Visual Capitalist (2022). https://www.visualcapitalist.com/cp/mapped-the-worlds-population-density-by-latitude/
Huang, K., Li, X., Liu, X. & Seto, K. C. Projecting global urban land expansion and heat Island intensification through 2050. Environ. Res. Lett. 14, 114037 (2019).
Peel, M. C., Finlayson, B. L. & McMahon, T. A. Updated world map of the Köppen-Geiger climate classification. Hydrol. Earth Syst. Sci. 11, 1633–1644 (2007).
Heutel, G., Miller, N. H. & Molitor, D. Adaptation and the mortality effects of temperature across US climate regions. Rev. Econ. Stat. 103, 740–753 (2021).
Carleton, T. et al. Valuing the global mortality consequences of climate change accounting for adaptation costs and benefits. Q. J. Econ. 137, 2037–2105 (2022).
Author information
Authors and Affiliations
Contributions
Y.L. and L.M. wrote the main manuscript text, and X.W. analyzed the data and prepared Figs. 1 and 2., G.H. and H.L. reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Liang, Y., Wang, X., Ma, L. et al. A standardized indicator reveals sharper increases in heat related mortality in temperate zone cities worldwide. Sci Rep 16, 216 (2026). https://doi.org/10.1038/s41598-025-21897-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-21897-4
