
Abstract
We aimed to identify and validate key predictive factors influencing 28-day survival rates in patients with diabetes and sepsis and to develop a predictive model based on these factors to assist clinical decision-making. In this retrospective cohort study, we examined data from 303 patients with diabetes and sepsis treated at the Emergency Department of West China Hospital, Sichuan University, between June 2022 and November 2023. The Least Absolute Shrinkage and Selection Operator (LASSO) method was employed to identify key predictive factors from 52 characteristics. A logistic regression model was then developed to create a nomogram for predicting 28-day survival rates. Model performance was assessed using calibration curves, Harrell’s C-index, bootstrap validation, decision curve analysis, and receiver operating characteristic (ROC) curve analysis. Six major predictive factors were identified: age, consciousness level, acid–base balance (pH level), aspartate aminotransferase (AST) level, myoglobin concentration, and the need for mechanical ventilation. The nomogram exhibited excellent concordance with the calibration curve, achieving a C-index of 0.833 and demonstrating robust discriminative capability, as validated through bootstrapping. Decision curve analysis indicated that the model provided a greater net benefit within a patient survival probability threshold ranging from 20% to 80%. ROC curve analysis revealed an area under the curve of 0.833, highlighting the model’s strong discriminatory power. The predictive model developed in this study for the 28-day survival rate of patients with diabetes and sepsis demonstrates high predictive accuracy and serves as an effective clinical decision-making tool for healthcare professionals.
Similar content being viewed by others
Introduction
Diabetes is a widespread chronic metabolic disorder characterized by high blood glucose levels, usually resulting from inadequate insulin secretion or impaired biological responses to insulin1. A report from the International Diabetes Federation (IDF) states that approximately 537 million adults globally are living with diabetes, equating to approximately 1 in every 10 adults. The prevalence rate, currently approximately 10.5%, continues to rise2. Poor long-term management of diabetes can result in various complications, such as cardiovascular diseases, kidney issues, retinopathy, and neuropathy, all of which significantly threaten patients’ health and quality of life3.
Sepsis is a clinical syndrome caused by dysregulation of the host response to infection, which subsequently leads to life-threatening multi-organ dysfunction4. It is one of the leading causes of in-hospital mortality worldwide, with high incidence and mortality rates. Globally, it is estimated that tens of millions of individuals are affected by sepsis annually, with death rates exceeding 20%5. The incidence of sepsis increases with age and is closely associated with chronic diseases, including diabetes6.
Owing to the immunosuppressive effect of sustained high blood glucose levels, individuals with diabetes are susceptible to infections, which often result in severe manifestations7. Additionally, the onset of sepsis can worsen the metabolic problems associated with diabetes, perpetuating a detrimental cycle8. This heightened susceptibility is associated with compromised white blood cell function under elevated glucose levels, characterized by reduced chemotaxis, phagocytosis, and bactericidal functions, which are essential elements of the immune system’s defense against pathogens9. Furthermore, patients with diabetes often experience a persistent inflammatory condition that not only impedes their ability to repair tissues but also fosters an environment conducive to bacterial growth10. In diabetes, sepsis may further exacerbate metabolic complications11. Systemic inflammatory reactions triggered by sepsis may result in increased insulin resistance, complicating the management of blood glucose levels. This metabolic imbalance not only disrupts energy metabolism but also hinders the coagulation process and inflammatory responses, ultimately worsening the progression of organ dysfunction12.
Individuals with diabetes and sepsis experience accelerated disease progression and an increased risk of organ failure, including acute kidney damage, respiratory failure, and cardiovascular collapse13. Additionally, the mortality rate in patients with diabetes and sepsis is significantly elevated compared with that in non-diabetic patients with sepsis14. The heightened risk of mortality could be intricately associated with impaired tissue perfusion and a reduced capacity for healing, both of which result from diabetes-related complications of the microvascular and macrovascular systems15. Considering the gravity of the situation, managing individuals with diabetes and sepsis requires a comprehensive, multidisciplinary approach that prioritizes infection management, regulation of blood glucose levels, and support for organ functionality.
Timely identification of at-risk patients, prompt intervention, and diligent monitoring are essential for enhancing prognostic outcomes. However, a significant gap remains in our understanding of the most effective strategies for predicting and improving the prognosis of patients with diabetes and sepsis. This limitation underscores the pressing need for advanced methods to provide clearer insights into patient outcomes16. The absence of a reliable assessment model capable of accurately predicting the prognosis of patients with diabetes and sepsis hinders our ability to tailor personalized treatment plans and effectively optimize the distribution of medical resources.
In this study, we aimed to address this gap by developing and validating a prognostic assessment model tailored to patients with diabetes and sepsis. The goals of this study were to identify the key factors influencing prognosis and to establish a scientific foundation to guide clinical decision-making. By establishing this model, we seek to facilitate early and effective interventions for high-risk patients, thereby improving patient outcomes and overall healthcare efficiency.
Patients and methods
Research design
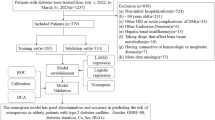
This retrospective study included patients with diabetes complicated by sepsis who visited the Emergency Department of West China Hospital of Sichuan University from June 2022 to November 2023, with the enrollment date as Day 0, follow-up was conducted by phone or through the medical record system until Day 28;The research protocol was approved by the Ethics Committee of West China Hospital, Sichuan University (Approval No.: [2024] 216 K). All methods were performed in accordance with relevant guidelines and regulations. Owing to the retrospective nature of the study, the Ethics Committee of West China Hospital, Sichuan University, waived the need for obtaining informed consent.
Study population
This study included patients aged 18 years and older who had a confirmed diagnosis of diabetes and sepsis according to the International Consensus Definition (Sepsis-3) and who received in-hospital treatment during the study period. The inclusion and exclusion criteria are listed below.
Inclusion criteria:
-
Patients aged 18 years or older.
-
Diagnosis of diabetes according to the diagnostic criteria of the International Diabetes Federation (IDF).
-
Diagnosis of sepsis according to the International Consensus Definition (Sepsis-3).
-
Receipt of in-hospital treatment during the study period with complete clinical records.
Exclusion criteria:
-
Patients under the age of 18 years.
-
Missing or incomplete medical records.
-
Patients without diabetes or sepsis.
-
Patients transferred to another hospital or lost to follow-up during treatment.
-
Unclear diagnosis of diabetes (lack of blood glucose tests or clinical diagnosis records).
-
Patients with terminal diseases (such as terminal cancer, severe heart and lung failure).
-
Data from patients with recurrent admissions (for recurrent admissions, only the data from the first admission should be included).
Data collection
We systematically collected data on indicators covering multiple physiological, biochemical, and clinical scoring systems from patients with diabetes complicated by sepsis who were admitted to the Emergency Department. These indicators included.
-
Blood glucose and lactate levels: Glucose (Glu), lactate (LAC).
-
Hematological indices: Bicarbonate levels (HCO3), hemoglobin (HB), hematocrit (HCT), white blood cell count (WBC), neutrophil percentage (N), and platelet count (PLT).
-
Liver function indices: Total bilirubin (TB), alanine aminotransferase (ALT), aspartate aminotransferase (AST), and albumin (ALB).
-
Renal function indices: Blood urea nitrogen (BUN), creatinine (CysC), uric acid (UA), and serum creatinine (SCr).
-
Lipid metabolism indices: Triglycerides (TG) and total cholesterol (TC).
-
Cardiac enzymes: Creatine kinase (CK), CK-MB isoenzyme (CKMB), and cardiac troponin T (CTnT))
-
Other biochemical indices: Electrolytes, including sodium (Na), potassium (K), and calcium (Ca); and coagulation markers, such as prothrombin time (PT), activated partial thromboplastin time (APTT), D-dimer (DD), and fibrinogen (Fib).
Specific biomarkers included cardiac troponin (Myo), brain natriuretic peptide (BNP), and procalcitonin (PCT). Clinical scoring systems, including the Sequential Organ Failure Assessment (SOFA), quick Sequential Organ Failure Assessment (qSOFA), and Acute Physiology and Chronic Health Evaluation (APACHE) II were used as prognostic indicators.
The primary outcome measure was survival status within 28 days17,18. This measure was used to validate the accuracy and practicality of the constructed prognostic evaluation model in predicting patient survival probability.
Statistical analysis and model development
Demographic, disease-related, and laboratory examination data were expressed as counts (%). Statistical analyses were performed using R software.
First, we performed univariate logistic regression on all candidate indicators and retained those significantly associated with 28-day mortality (P < 0.1).The Least Absolute Shrinkage and Selection Operator (LASSO) method, suitable for dimensionality reduction in high-dimensional datasets, was used to select the best predictive features from risk factors in laboratory examinations of patients with sepsis. Features with non-zero coefficients in the LASSO regression model were selected. Subsequently, a predictive model was developed by combining the selected features in a multivariate logistic regression analysis. The features were characterized by odds ratios (ORs), 95% confidence intervals (CIs), and P-values. A two-sided P-value of < 0.05 was considered statistically significant. Demographic variables with P < 0.05, as well as variables related to disease and treatment characteristics, were included in the model.
All potential predictors were applied to develop a predictive model for medication non-adherence risk using the cohort. A calibration curve was plotted to assess the calibration of the non-adherence nomogram. The significance test statistics indicated that the model was not fully calibrated. Harrell’s C-index was used to quantify the discriminative performance of the non-adherence nomogram. Bootstrapping validation of the non-adherence nomogram (1,000 bootstrapping resamples) was performed to calculate the relatively corrected C-index. Decision curve analysis was conducted to determine the clinical usefulness of the non-adherence nomogram by quantifying the net benefit at different threshold probabilities in the IRD cohort. The net benefit was calculated by subtracting the proportion of false-positive patients from the proportion of true-positive patients and weighing the relative harm of foregoing interventions against the negative consequences of unnecessary interventions.
Results
Patients’ characteristics
A total of 303 patients were enrolled between June 2022 and November 2023. with 63 deaths recorded within the 28-day follow-up period. Among those who died, 24 were women (38.1%), and 39 were men (61.9%), compared to 98 women (40.8%) and 142 men (59.2%) among the survivors. The average age of the deceased patients was 67.0 ± 12.1 years, while that of the surviving patients was 61.6 ± 14.2 years. We compared baseline characteristics between the two groups, including heart rate, blood pressure, and oxygen saturation. Significant differences were observed in certain indicators, such as blood pH levels (P < 0.001), the fraction of inspired oxygen (FIO2) (P < 0.001), lactate levels (P = 0.023), base excess (P = 0.006), SOFA score (P < 0.001), and APACHE II score (P < 0.001). A comprehensive set of data, including demographic information, disease characteristics, and treatment features for both groups, is presented in Table 1.
Feature selection
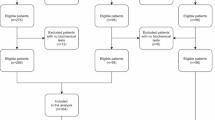
Using data from the cohort of 303 patients, 52 characteristics were reduced to six key potential predictive factors (Fig. 1A and B). These factors exhibited non-zero coefficients in the LASSO regression model, indicating their significant impact on predictive outcomes. The selected features included patient age, level of consciousness, acid–base status (pH value), AST levels, myoglobin levels, and the need for mechanical ventilation support (Table 2).

Demographic and clinical feature selection using the LASSO binary logistic regression model. (A) This plot displays the LASSO coefficient profiles for 52 features across various log(lambda) values. The vertical line at lambda.min = 0.04151642, determined through five-fold cross-validation, indicates the optimal lambda. At this point, five features have non-zero coefficients, highlighting the most influential predictors in the model. (B) The binomial deviance curve is plotted against log(lambda) to select the optimal lambda for the LASSO model. The dotted lines indicate the lambda.min and its 1-SE range, guiding the choice of lambda that balances model performance and complexity. The lambda.min of 0.04151642 is central to this selection, ensuring effective regularization and feature selection in the model. LASSO, Least Absolute Shrinkage and Selection Operator; SE, standard error.
Development of a 28-day survival rate prediction model
The outcomes of the logistic regression analysis for age, level of consciousness, acid–base status (pH value), AST levels, myoglobin levels, and need for mechanical ventilation support are detailed in Table 2. A model incorporating these independent predictive factors was constructed and depicted as a nomogram (Fig. 2).

Developed 28-day survival rate nomogram. The 28-day survival nomogram was developed in the cohort using age, consciousness level, pH, AST, Myo, and mechanical ventilation requirement. PH, potential of hydrogen; AST, Aspartate Aminotransferase; Myo, Myoglobin.
Apparent performance of the 28-day survival rate nomogram in the cohort
The calibration curve of the nomogram demonstrated excellent agreement in the cohort (Fig. 3). The C-index for the survival rate nomogram was 0.833 (95% CI: 0.833–1.96*se), which was confirmed to be robust through bootstrapping validation, suggesting the model’s strong discriminative performance. In the 28-day survival rate nomogram, the apparent performance indicated high predictive capability (Fig. 3).

Calibration curves of the 28-day survival rate nomogram prediction in the cohort. The x-axis represents the predicted 28-day survival rate, while the y-axis represents the actual diagnosed 28-day survival. The diagonal dotted line represents a perfect prediction by an ideal model, whereas the solid line represents the nomogram’s performance, a closer fit of which to the diagonal dotted line represents a better prediction.
Clinical use
Figure 4 shows the decision curve analysis for the 28-day survival rate prediction nomogram. The curve indicates that when the threshold probabilities for both patients and physicians range between 20% and 80%, employing this survival rate nomogram to forecast the likelihood of survival at 28 days yields greater benefits compared to assumptions that all patients will either survive or not survive. Within this range, the net benefit aligns closely with the nomogram’s predictions, demonstrating its utility in clinical decision-making (Fig. 4).

Decision curve analysis for the 28-day survival rate nomogram. The y-axis measures the net benefit, which quantifies the additional benefit of using the 28-day survival rate nomogram compared to assuming that all patients will survive or none will survive. The x-axis represents the threshold probability, which is the minimum probability of survival that a patient or clinician would consider acceptable to take a particular action or intervention. The dotted line represents the 28-day survival rate prediction nomogram, which is the model used to predict the likelihood of a patient surviving for 28 days. The thin solid line represents the assumption that all patients will survive, which would be the scenario if no action is taken and all patients are assumed to have a 100% survival rate. The thick solid line represents the assumption that no patients will survive, which would be the scenario if no action is taken and all patients are assumed to have a 0% survival rate. The decision curve shows that the nomogram provides a net benefit over the “all” and “none” strategies when the threshold probability is between certain values (20–80%). This indicates that using the nomogram to guide treatment decisions can be more beneficial than assuming all patients will either survive or not survive.
The area under the curve (AUC) under the receiver operating characteristic (ROC) curve
The ROC curve analysis for the 28-day survival rate nomogram is presented in Fig. 5, showing the model’s performance in discriminating between survivors and non-survivors within the 28-day period. The area under the ROC curve (AUC) for the nomogram is 0.833, with a 95% CI of 0.714 to 0.850, indicating the model’s high discriminatory ability.

Receiver operating characteristic (ROC) curve analysis for the 28-day survival rate nomogram. AUC, area under the curve: The AUC of the ROC curve is 0.833, indicating a high discriminatory power of the model. An AUC of 1 represents perfect discrimination, while an AUC of 0.5 suggests no discriminative ability. Sensitivity and Specificity: The curve shows the trade-off between sensitivity and specificity. Sensitivity, or the true positive rate, is plotted on the y-axis, while specificity, or the true negative rate, is plotted on the x-axis. Model Performance: The model demonstrates a balance between sensitivity and specificity, with a notable sensitivity of 0.704 (95% CI: 0.714 to 0.850) at a given threshold.
The sensitivity of the model, indicated on the y-axis, is 0.704, and the specificity, indicated on the x-axis, is 0.665 at the point where the curve intersects the dashed line representing the threshold probability. The curve illustrates the trade-off between sensitivity and specificity across various threshold settings.
The AUC under the ROC curve of a random subset (65%) of the data
The ROC curve analysis of the 28-day survival rate prediction model was performed using a random subset comprising 65% of the dataset. The model demonstrated an AUC of 0.851, signifying excellent discriminatory ability. This indicates a 70.4% probability of correctly identifying patients who will survive, with a high level of confidence in this estimation. The ROC curve, positioned significantly above the diagonal line that represents a random guess (AUC = 0.5), indicates an excellent performance. Its proximity to the left upper corner of the plot signifies the model’s superior ability to discriminate between survivors and non-survivors compared to random assumptions.
Clinical Implications: The high AUC value, combined with the balance between sensitivity and specificity, makes this model a potentially valuable tool in clinical settings. It can assist healthcare providers in making informed decisions regarding patient care and optimize resource allocation by predicting the likelihood of survival within the first 28 days of treatment or hospital admission.
Statistical Significance: The 95% CI for sensitivity further supports the statistical significance of the model’s predictive accuracy. This interval provides a range within which the true sensitivity of the model is likely to fall, adding to the reliability of the model’s predictions. The ROC curve analysis of the 28-day survival rate prediction model, with an AUC of 0.851, presents a strong case for its implementation in clinical practice. The model’s ability to accurately predict survival rates can significantly impact patient outcomes and guide treatment strategies (Fig. 6).

ROC Curve Analysis for the 28-day survival rate prediction model of a random subset (65%) of the data. This model’s performance was internally validated using a random subset of 65% of the data. AUC (area under the curve): The AUC of the ROC curve is 0.851. Sensitivity, which is the model’s ability to correctly identify patients who will survive, is plotted on the y-axis. Specificity, which is the model’s ability to correctly identify patients who will not survive, is plotted on the x-axis. At a given threshold, the model demonstrates a sensitivity of 0.704 with a 95% CI ranging from 0.714 to 0.850.
Discussion
In this study, we aimed to identify and validate significant predictive factors affecting 28-day survival rates by analyzing data from 303 patients and developing a predictive model based on these factors. The results indicated that six major predictive factors affected the 28-day survival rates: age, consciousness level, acid–base balance (pH), AST levels, myoglobin concentrations, and the need for mechanical ventilation.
The investigation revealed that the mean age of non-survivors (67.0 ± 12.1 years) exceeded that of survivors (61.6 ± 14.2 years), a finding that corresponds with previous research and reinforces that age plays a crucial role in determining patient survival rates19. We further highlighted age as a critical factor influencing the 28-day survival rates20. This finding is consistent with multiple studies suggesting that older patients have a higher likelihood of adverse clinical outcomes21. Physiological reserves and responsiveness to illness tend to diminish with advancing age, which may result in prolonged recovery and lower survival rates22. Additionally, older patients frequently present with chronic health issues that may further affect their survival outcomes23. Notable differences were also observed in the sex distribution; however, the influence of sex on survival rate prediction remains ambiguous.
Consciousness is a crucial marker for predicting prognosis, highlighting the significance of neurological assessment in critically ill patients24.Variations in consciousness can indicate early neurological impairment and are closely linked to neurological injury and unfavorable outcomes25. In clinical settings, evaluating consciousness levels enables rapid assessment of illness severity, facilitating timely interventions26.
Marked discrepancies in the acid–base balance (pH levels) and lactate concentrations illustrate the harmful effects of metabolic disturbances on patient prognosis27. Irregularities in these metrics may indicate the extent of tissue hypoxia and metabolic acidosis, which are strongly associated with patient survival rates. An irregular acid–base balance (pH) is a powerful indicator of adverse prognosis in critically ill individuals. Severe metabolic acidosis, related to tissue hypoxia and cellular impairment, may result in lower pH levels. Therefore, preserving a balanced acid–base environment is essential for optimal cellular activities and organ function.Disruptions in this balance can result in multiple organ dysfunction syndrome, negatively influencing patient survival outcomes28.
AST is a vital marker for assessing liver function and was shown to be useful for predicting 28-day survival rates in this study. High AST levels may indicate damage to liver cells, which is often considered a negative prognostic factor in critically ill patients29.Furthermore, elevated AST levels reflect not only liver impairment but may also be associated with muscle injury. In patients with severe illness, increased AST levels may be related to the severity of inflammation and tissue damage, both of which can affect recovery and overall survival.
Similarly, elevated myoglobin levels emerged as a significant prognostic indicator closely related to muscle injury. The presence of myoglobin in the bloodstream can influence survival outcomes, as it correlates with the patient’s inflammatory response and degree of tissue damage30. Myoglobin is a protein predominantly located in cardiac and skeletal muscles, and its concentration in the blood often correlates directly with the extent of muscle damage. In critically ill patients, elevated myoglobin levels may indicate severe myocardial injury, which can result in cardiac dysfunction that adversely affects systemic hemodynamics and oxygen delivery31. Given the heart’s essential role in sustaining life, any substantial decline in its function can significantly affect a patient’s survival rate32.
The need for mechanical ventilation support in critically ill patients is frequently correlated with diminished survival rates, a pattern that corresponds to markers indicating the severity of the critical illness33. The requirement for mechanical ventilation may be a crucial factor affecting survival rates, particularly the degree of respiratory function impairment. Patients requiring mechanical ventilation generally exhibit more severe ailments and a less favorable prognosis34. Thus, mechanical ventilation functions not only as a form of respiratory assistance but also as an indicator of the patient’s respiratory capacity and overall chances of survival.
In this study, we developed a predictive model that identified six important predictive elements through LASSO regression analysis35, resulting in the creation of a nomogram designed to estimate the 28-day survival rate in patients with diabetes and sepsis.The model achieved a C-index of 0.833, indicating strong discriminative capability36. Bootstrap validation further established the model’s stability and discriminative efficacy, reinforcing the reliability of the findings and providing a solid foundation for clinical implementation37. Internal validation is essential for evaluating the performance of predictive models, as it confirms consistent efficacy across different samples and conditions. This model is a vital resource for healthcare professionals, allowing them to consider several key factors when making treatment choices. By integrating these factors, the model supports the assessment of patient outcomes and modification of treatment strategies accordingly. This personalized approach to treatment can enhance therapeutic outcomes and improve survival rates for patients.
Decision curve analysis revealed that the predictive model yields a greater net benefit within a patient survival probability threshold ranging from 20% to 80%, compared to simplified scenarios considering only complete survival or non-survival38. This highlights the potential utility of the model in clinical decision-making. Moreover, ROC curve analysis showed an AUC value of 0.833 for the model, indicating strong predictive capabilities. The balance between sensitivity and specificity observed in the ROC analysis further supports the model’s clinical relevance. With its high AUC and equilibrium between sensitivity and specificity, this predictive model is a valuable asset for healthcare professionals to assist them in making informed evaluations of patients’ 28-day survival probabilities and guiding the development of treatment strategies.
Limitation
Although the model developed in this study demonstrated notable predictive accuracy, certain limitations must be acknowledged. The model does not fully integrate all potential factors affecting survival rates, such as genetic predisposition, socioeconomic conditions, and lifestyle factors. Future investigations should examine how these variables influence the model’s predictive capabilities and aim to incorporate them to improve accuracy. While the model showed outstanding performance in internal validation, its effectiveness in various populations and clinical environments needs validation through further external assessments. Future research should evaluate the model’s application across patient demographics and geographic locations to confirm its wide-ranging clinical relevance.
Conclusion
The predictive model developed in this study for the 28-day survival rate of patients with diabetes and sepsis demonstrates high predictive accuracy and serves as an effective clinical decision-making tool for healthcare professionals. Although the model showed commendable effectiveness in internal validation, its consistency and applicability across various populations remains to be verified through external validation. Future investigations should aim to identify more predictive factors and incorporate them into the model to enhance its accuracy and clinical relevance.
Data availability
The datasets generated and analysed during the current study are available in the [Date.xlsx].
References
Agudelo-Ochoa, G. M. et al. Gut microbiota profiles in critically ill patients, potential biomarkers and risk variables for sepsis. Gut Microbes. 12, 1707610. https://doi.org/10.1080/19490976.2019.1707610 (2020).
Ahn, S. Y. et al. In vivo monitoring of dynamic interaction between neutrophil and human umbilical cord blood-derived mesenchymal stem cell in mouse liver during sepsis. Stem Cell. Res. Ther. 11, 44. https://doi.org/10.1186/s13287-020-1559-4 (2020).
Al Zoubi, S. et al. Linagliptin attenuates the cardiac dysfunction associated with experimental sepsis in mice with Pre-existing type 2 diabetes by inhibiting NF-κB. Front. Immunol. 9, 2996. https://doi.org/10.3389/fimmu.2018.02996 (2018).
Singer, M. et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). Jama 315, 801–810. https://doi.org/10.1001/jama.2016.0287 (2016).
Cai, S. et al. Association between glucose-to-lymphocyte ratio and in-hospital mortality in intensive care patients with sepsis: A retrospective observational study based on medical information Mart for intensive care IV. Front. Med. (Lausanne). 9, 922280. https://doi.org/10.3389/fmed.2022.922280 (2022).
Costantini, E., Carlin, M., Porta, M. & Brizzi, M. F. Type 2 diabetes mellitus and sepsis: state of the art, certainties and missing evidence. Acta Diabetol. 58, 1139–1151. https://doi.org/10.1007/s00592-021-01728-4 (2021).
Holt, R. I. G., Cockram, C. S., Ma, R. C. W. & Luk, A. O. Y. Diabetes and infection: review of the epidemiology, mechanisms and principles of treatment. Diabetologia 67, 1168–1180. https://doi.org/10.1007/s00125-024-06102-x (2024).
Han, H. F. et al. Duodenal-jejunal bypass increases intraduodenal bile acids and upregulates duodenal SIRT1 expression in high-fat diet and streptozotocin-induced diabetic rats. World J. Gastroenterol. 28, 4338–4350. https://doi.org/10.3748/wjg.v28.i31.4338 (2022).
Mao, H. et al. Loss of bone morphogenetic protein-binding endothelial regulator causes insulin resistance. Nat. Commun. 12, 1927. https://doi.org/10.1038/s41467-021-22130-2 (2021).
Souza, M. C. et al. Chronic Toxoplasma gondii infection exacerbates secondary polymicrobial sepsis. Front. Cell. Infect. Microbiol. 7, 116. https://doi.org/10.3389/fcimb.2017.00116 (2017).
Su, C. H., Chen, W. M., Chen, M., Shia, B. C. & Wu, S. Y. Association of diabetes severity and mortality with lung squamous cell carcinoma. Cancers (Basel). 14. https://doi.org/10.3390/cancers14102553 (2022).
Uckun, F. M. et al. RJX improves wound healing in diabetic rats. Front. Endocrinol. (Lausanne). 13, 874291. https://doi.org/10.3389/fendo.2022.874291 (2022).
Xu, L. et al. Protective effect of melatonin against polymicrobial sepsis is mediated by the Anti-bacterial effect of neutrophils. Front. Immunol. 10, 1371. https://doi.org/10.3389/fimmu.2019.01371 (2019).
Zhang, J. et al. Global transcriptional regulation of STAT3- and MYC-mediated sepsis-induced ARDS. Ther. Adv. Respir Dis. 13, 1753466619879840. https://doi.org/10.1177/1753466619879840 (2019).
Zhang, L. et al. Construction and evaluation of a sepsis risk prediction model for urinary tract infection. Front. Med. (Lausanne). 8, 671184. https://doi.org/10.3389/fmed.2021.671184 (2021).
Zhu, X. et al. Conjunctival microbiota in patients with type 2 diabetes mellitus and influences of perioperative use of topical Levofloxacin in ocular surgery. Front. Med. (Lausanne). 8, 605639. https://doi.org/10.3389/fmed.2021.605639 (2021).
Manjappachar, N. K. et al. Outcomes and predictors of 28-Day mortality in patients with hematologic malignancies and septic shock defined by Sepsis-3 criteria. J. Natl. Compr. Canc Netw. 20, 45–53. https://doi.org/10.6004/jnccn.2021.7046 (2022).
Zhang, X., Yuan, W., Li, T., Sha, H. & Hui, Z. The association between body mass index and 28-day mortality in patients with sepsis: A retrospective cohort study. Am. Surg. 91, 494–504. https://doi.org/10.1177/00031348241304040 (2025).
Cadrin-Tourigny, J. et al. A new prediction model for ventricular arrhythmias in arrhythmogenic right ventricular cardiomyopathy. Eur. Heart J. 43, e1–e9. https://doi.org/10.1093/eurheartj/ehac180 (2022).
de Vries, V. A. et al. Long-Term outcome of patients with a hematologic malignancy and multiple organ failure admitted at the intensive care. Crit. Care Med. 47, e120–e128. https://doi.org/10.1097/ccm.0000000000003526 (2019).
Feng, K. et al. Identification of biomarkers and the mechanisms of multiple trauma complicated with sepsis using metabolomics. Front. Public. Health. 10, 923170. https://doi.org/10.3389/fpubh.2022.923170 (2022).
Gershon, R. R. et al. Psychosocial influences on disaster preparedness in San Francisco recipients of home care. J. Urban Health. 94, 606–618. https://doi.org/10.1007/s11524-016-0104-3 (2017).
Gill, P. S., Ozment, T. R., Lewis, N. H., Sherwood, E. R. & Williams, D. L. Trained immunity enhances human monocyte function in aging and sepsis. Front. Immunol. 13, 872652. https://doi.org/10.3389/fimmu.2022.872652 (2022).
Gonçalves, B. et al. Incidence and impact of sepsis on long-term outcomes after subarachnoid hemorrhage: a prospective observational study. Ann. Intensive Care. 9 https://doi.org/10.1186/s13613-019-0562-3 (2019).
Guo, L. et al. Platelet MHC class I mediates CD8 + T-cell suppression during sepsis. Blood 138, 401–416. https://doi.org/10.1182/blood.2020008958 (2021).
Hu, J. et al. Siglec15 shapes a non-inflamed tumor microenvironment and predicts the molecular subtype in bladder cancer. Theranostics 11, 3089–3108. https://doi.org/10.7150/thno.53649 (2021).
Karagiannidis, C. et al. Case characteristics, resource use, and outcomes of 10 021 patients with COVID-19 admitted to 920 German hospitals: an observational study. Lancet Respir Med. 8, 853–862. https://doi.org/10.1016/s2213-2600(20)30316-7 (2020).
Lewis, J. M. et al. Population incidence and mortality of sepsis in an urban African Setting, 2013–2016. Clin. Infect. Dis. 71, 2547–2552. https://doi.org/10.1093/cid/ciz1119 (2020).
Li, Y. et al. Role of eotaxin-1/CCL11 in sepsis-induced myocardial injury in elderly patients. Aging (Albany NY). 12, 4463–4473. https://doi.org/10.18632/aging.102896 (2020).
Mankowski, R. T. et al. Older sepsis survivors suffer persistent disability burden and poor Long-Term survival. J. Am. Geriatr. Soc. 68, 1962–1969. https://doi.org/10.1111/jgs.16435 (2020).
Metkus, T. S. et al. Myocardial injury in severe COVID-19 compared with Non-COVID-19 acute respiratory distress syndrome. Circulation 143, 553–565. https://doi.org/10.1161/circulationaha.120.050543 (2021).
Nunes, M. C. P. et al. Incidence and predictors of progression to Chagas cardiomyopathy: Long-Term Follow-Up of trypanosoma cruzi-Seropositive individuals. Circulation 144, 1553–1566. https://doi.org/10.1161/circulationaha.121.055112 (2021).
Opondo, C., Allen, E., Todd, J. & English, M. Association of the paediatric admission quality of care score with mortality in Kenyan hospitals: a validation study. Lancet Glob Health. 6, e203–e210. https://doi.org/10.1016/s2214-109x(17)30484-9 (2018).
Quispe Cornejo, A. et al. The use of automated pupillometry to assess cerebral autoregulation: a retrospective study. J. Intensive Care. 8 https://doi.org/10.1186/s40560-020-00474-z (2020).
Wang, X., Jehi, L., Ji, X. & Mazzone, P. J. Phenotypes and subphenotypes of patients with COVID-19: A latent class modeling analysis. Chest 159, 2191–2204. https://doi.org/10.1016/j.chest.2021.01.057 (2021).
Wright, S. W. et al. Enhanced bedside mortality prediction combining point-of-care lactate and the quick sequential organ failure assessment (qSOFA) score in patients hospitalised with suspected infection in Southeast asia: a cohort study. Lancet Glob Health. 10, e1281–e1288. https://doi.org/10.1016/s2214-109x(22)00277-7 (2022).
Yu, H. et al. Identification of CFHR4 as a potential prognosis biomarker associated with Lmmune infiltrates in hepatocellular carcinoma. Front. Immunol. 13, 892750. https://doi.org/10.3389/fimmu.2022.892750 (2022).
Yuan, Y. et al. The transcription factor KLF14 regulates macrophage Glycolysis and immune function by inhibiting HK2 in sepsis. Cell. Mol. Immunol. 19, 504–515. https://doi.org/10.1038/s41423-021-00806-5 (2022).
Author information
Authors and Affiliations
Contributions
Rulin Wang conceived the study design, summarized the data and performed the statistical analysis and drafted the manuscript. Zhaxi Dunzhu conceived the study design, summarized the data. Zhixin Tan collected the data.Zhendong Niu summarized the data, performed the statistical analysis and drafted the manuscript. Haowen Tan collected the data. Yongli Gao conceived the study design and revised the manuscript. Yu Cao conceived the study design and revised the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, R., Dunzhu, Z., Tan, Z. et al. Development and validation of an interpretable machine learning model for early prediction in patients with diabetes and sepsis. Sci Rep 15, 38546 (2025). https://doi.org/10.1038/s41598-025-22488-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-22488-z
