
Abstract
People living with a rare disease can wait months to years for a confirmed diagnosis after symptom onset, mainly due to low prevalence, lack of awareness of primary healthcare professionals, heterogeneous clinical presentation and/or peculiar inheritance patterns. This consensus paper aims to establish a set of guidelines to assist healthcare professionals—also without a specialized expertise in rare diseases—in optimizing the diagnostic pathway for these conditions. During Phase 1 of a real-time Delphi study, ten experts defined 26 statements addressing the identification of clinical features (“red flags”, domain 1) and non-clinical tools/conditions (“clinical gateways”, domain 2) that could trigger/support the diagnostic suspect of a rare disease. During Phase 2, the survey was extended to a multidisciplinary panel of 55 experts to reach a consensus on statements. Consensus was reached on 22 out of 26 statements across the two domains. Family history, clusters of birth defects, unusual presentations of common disease, neurodevelopmental delays or decline, and severe pathology emerged as key indicators to improve the identification and referral of cases of rare disease and should be integrated into primary care practices. Education, increased awareness in the community and use of technology are possible gateways to facilitate early diagnosis in rare disease.
Similar content being viewed by others

Introduction
Rare diseases are defined as chronic and debilitating conditions occurring in < 1 every 2000 people in Europe and in < 200,000 people in USA. Although each rare disease affects a small number of individuals, when viewed globally, they involve more than 300 million people worldwide, with high medical, psychological and financial burdens to patients, caregivers and healthcare systems1. Many rare diseases are progressive and exhibit symptoms at birth or during childhood. Moreover, a significant proportion of rare diseases are severe, multisystem disorders2, substantially affecting life quality and expectancy3.
Despite rare diseases are increasingly being recognized as a global health priority4, people living with a rare disease can still wait months to years for a confirmed diagnosis after symptom onset.
The diagnosis of rare diseases can be quite complex and challenging due to the rarity of each condition and the heterogeneous clinical presentation and/or peculiar patterns of inheritance, in addition to a general lack of awareness, training and education among physicians5. To counteract these difficulties at informative level, the 11th revision of the International Classification of Diseases and Related Health Problems (ICD-11), issued by the World Health Organization in 2024, has a greater focus on rare disease vs. the previous versions, and, in particular, it now includes the Orphanet terminology to improve the classification and understanding of rare diseases6,7.
Primary care is the initial point of contact of a subject in the healthcare system, and general practitioners (GPs), pediatricians and emergency physicians should have a broad medical knowledge to be able to recognize problems and make decisions, rather than provide a definitive diagnosis. Recognition and evaluation of red flags, i.e. signs and symptoms of disorders in patient’s medical history, is essential in primary care, playing a crucial role in ensuring that potentially serious conditions, such as rare diseases, are not overlooked and patients are referred to specialists or centers for further clinical and genetic investigation8. Of note, referral of an undiagnosed patient to a center for rare diseases in Europe reduces the total diagnosis time (TDT) from 5.4 (interquartile range: 0.1–6.2) to 4.3 years (interquartile range: 0.1–4.2), underlying the need for more centers of expertise and increased referrals9.
Healthcare professionals often lack clear information and guidelines on when to suspect the presence of a rare disease. Information about the existence and the activity of centers for rare diseases and the access procedures is often inadequate as well10. The present study is based on a real-time Delphi (RTD) method and has been developed in the setting of the Argo project to reach a consensus on a series of statements defining the general clinical and non-clinical signals and circumstances that should trigger the diagnostic suspect of a rare disease, with the aim of supporting primary healthcare professionals, including those lacking a specific experience/background in the setting of these disorders. The Delphi panel was intentionally composed of a multidisciplinary group of professionals (including clinicians from various specialties, public health experts, and healthcare coordinators) reflecting the real-world complexity of rare disease care. This approach aimed to ensure that the identified red flags would be applicable not only in specialized settings but also across broader healthcare contexts, enhancing their relevance and potential for implementation.
Methods
Study design and development
The Argo project (https://helaglobe.com/argo/) takes its name from Argo, Ulysses’ faithful dog, who, recognizing his master beyond any disguise, embodies the essence of vigilance and instinct. Inspired by this symbolism, the initiative promotes a culture of diagnostic awareness, encouraging healthcare professionals to look beyond appearances and identify the often subtle and overlooked signs of rare diseases.
The Delphi method is a reliable measurement instrument commonly used in different settings, including health-related areas, to reach a consensus on a topic by a structured group of experts11. The conventional Delphi method is based on multiple rounds of questionnaires aimed at collecting and synthesizing opinions, and has four main characteristics: anonymity, iteration, controlled feedback and statistical aggregation of group responses12. However, this multi-round Delphi (MRD) is characterized by some shortfalls, including the length of the process. Recently, the concept of RTD as an efficiency-centered approach has emerged. It allows an enhancement of the overall process, as it is characterized by a greater efficiency, does not require iterative rounds of an online survey and the responses are recorded and updated in “real-time”. Of interest, recent studies revealed comparable outcomes for the MRD and the RTD surveys and highlighted the advantages of RTD in terms of time saving and achievement of better convergence on final scoring13.
This RTD survey was led and administered in the setting of the Argo project by Helaglobe (Florence, Italy) as a team of experts in Consensus methodologies that was responsible, in collaboration with the Campania Region—Coordinator Center for Rare Diseases (Naples, Italy), for literature review, organization and coordination of the experts’ groups, development and analysis of questionnaires, and drafting of the final report of the survey.
All methods were carried out in accordance with relevant guidelines and regulations. All panelists provided written informed consent for their participation in the RTD study. No human patients or animals were involved in the study.
The study and the RTD survey were organized as detailed below and in Fig. 1:

Overall design of the study.
Step 1, Desk analysis: a working group from the Argo project administrator (Campania Region—Coordinator Center for Rare Diseases and Helaglobe) drafted a preliminary list of principles and research questions following the literature review on rare diseases, diagnostic odyssey and potential general red flags. Predefined keywords were used for literature search in the main biomedical PubMed/Medline database, and the search string was as follows: (((rare diseases[Title/Abstract]) AND (red flags[Title/Abstract]) AND ((diagnosis[Title/Abstract]) OR (suspect[Title/Abstract])))) OR ((rare disease[Title/Abstract]) AND (early diagnosis[Title/Abstract]) AND ((late diagnosis[Title/Abstract]) OR (delayed diagnosis[Title/Abstract]))) OR ((rare disease[Title/Abstract]) AND ((diagnosis[Title/Abstract]) OR (suspect[Title/Abstract])) AND ((pedigree[Title/Abstract]) OR (genetics[Title/Abstract]) OR (familial[Title/Abstract]))).
The following selection/inclusion criteria were used during literature review:
-
Reference period: January 1, 2014-August 31, 2024;
-
Studies in English;
-
Major publications with greater scientific evidence (meta-analysis, systematic reviews, clinical trials, clinical studies, guidelines, reviews, real-world data) relevant for the topic of the RTD study.
Step 2, meetings of the expert board, literature review and statement definition: a board composed by a panel of 10 experts in rare diseases reviewed, discussed and revised during two virtual meetings the outputs of the desk analysis, including a list of draft statements. Overall process allowed the generation of 26 survey items about general “red flags” (domain 1) and the non-clinical circumstances and tools (“clinical gateways”, domain 2) that should trigger and support a diagnostic suspect of rare disease in healthcare professionals, with particular reference in those involved in primary care and without a well-defined expertise in rare diseases. Red flags and clinical gateways differ not only in their content but also in their relationship with time and clinical action. Red flags represent signals that may require immediate action—when more than one of them appear, rare disease suspicion should be raised, and the patient should be promptly referred for further diagnostic investigations. In contrast, clinical gateways do not indicate an immediate emergency but represent factors that should be integrated into medium- and long-term planning.
Step 3, Delphi panel composition and online voting: 67 experts in the field of rare diseases were invited by email to participate to the RTD survey and 45 accepted. All materials, including the survey, were in English. The 45 experts included as members of the Delphi voting panel, together with the board of 10 experts (n = 55 total panelists), were asked to express their judgment on the 26 statements defined during the Step 2 described above. Overall, participants to the RTD survey included experts in rare diseases, representatives from Rare Disease Coordination Centers (CCMRs), pediatricians and specialists from various fields with experience in specific rare diseases. The RTD survey was conducted on a proprietary platform by Helaglobe. Participants were provided with personal access to the online portal for four weeks between December 2024 and January 2025. On accessing the portal during the process, panelists were able to vote and comment each statement and to view aggregated responses from other responders in real-time. They were also able to revise their responses as many times as they wished within the set timeframe, with a simultaneous calculation of agreement and feedback. Single answers and comments were anonymous and only visible by the moderators.
Step 4, voting and analysis of consensus: Voting was undertaken by the Delphi panelists using a 5-point Likert scale to indicate the level of agreement on each statement: 1 = absolutely disagree, 2 = disagree, 3 = neither agree nor disagree, 4 = agree, 5 = strongly agree. The answers were expressed as a percentage response for each statement. A total cumulative agreement was defined as the sum of response percentages in items 4 (‘agree’) and 5 (‘strongly agree’).
Final data analysis: The consensus for each statement was reached if at least 75% of Delphi panelists ranked the statement ≥ 4 on the 5-point Likert scale described above. This level of total cumulative agreement has been set as median threshold to define the consensus consistently with several other studies in the healthcare setting14.
Results
Participation in the survey
We recruited in this RTD study a panel of experts selected among the major stakeholders in the field of rare diseases, representing a variety of medical specialties, with the aim of achieving the greatest possible range of opinions in this setting. Forty-five out of the 67 experts we contacted agreed to participate in the RTD and joined the board of 10 experts, thus reaching a remarkable total of 55 voting panelists. Physicians and researchers belonged to one, or a combination of, the areas of expertise listed in Table 1. Pediatrics (n = 12) and medical genetics (n = 5) were the most frequent specialties among panelists, followed by nephrology and human genetics (n = 4/each), cardiology, immunology, hematology, rheumatology, and internal medicine (n = 3/each). A group of 20 panelists were also representatives of regional centers for rare diseases located in 18 Italian regions. UNIAMO, the Italian Federation of Rare Diseases, which also serves as the Italian National Alliance within the European Organization for Rare Diseases (EURORDIS) represented people with rare diseases and their families.
Overview of results
The 26 final statements defined by a panel of 10 experts in rare diseases during the Phase 2 of the study were split in two domains (defined as red flags and clinical gateways of rare disease, respectively) as described in Methods section, and spanned the following areas:
Red flags (n = 16 statements):
-
Involvement of multiple systems
-
Multiple specialist referrals
-
Genetic inheritance pattern
-
Delayed diagnosis or single/multiple misdiagnosis or prolonged hospital stay
-
Failure to standard therapies
-
School concerns
-
Puberty and transition to adult care
-
Peculiar emotional phenomena
-
Disease presentation at any age
-
Functional impairment
-
Wait and see strategy
Clinical gateways (n = 10 statements):
-
Healthcare professional education
-
Information to increase awareness and knowledge about rare diseases
-
Implementation of technological tools
-
Healthcare system planning
At the end of RTD, the statements’ review was highly favorable, with 84.6% of them achieving a consensus (Table 2). The four statements that did not reached a consensus were all included among the potential red flags of rare disease, and concerned the failure to standard therapies (statement #9), the prolonged length of hospital stay (statement #10), school concerns (statement #11) and the peculiar emotional phenomena associated with other signs or symptoms and with failure to respond to standard therapies (statement #13) (Table 2).
Of note, 43.7% and 60% of the statements reached a 90–100% consensus in the red flags and clinical gateways domains, respectively. The statements reaching a 98–100% consensus in domain of potential red flags of rare disease confirmed the importance of patient’s family history, possibly suggesting a genetic inheritance pattern to be further investigated (statement #6, 100.0% degree of consensus), and recommended to carefully consider a potential manifestation of a rare disease at any age, considering a different intensity of signs and symptoms that could make the diagnosis even more complicated (statement #14, 98.2% degree of consensus). Other potential red flags of rare disease that reached a high degree of consensus following the RTD process included the multiorgan or multisystem involvement, to be evaluated through a comprehensive and multispecialty approach (statement #1, 94.6% degree of consensus) and the delayed diagnosis, implying a persistent health issue for at least one year (statement #7, 96.3% degree of consensus) (Table 2).
Some of the initial red flag statements such as “Failure to Standard Therapies”, “Prolonged Length of Hospital Stay”, and “Peculiar Emotional Phenomena” did not reach a sufficient level of agreement. According to our own interpretation, this is potentially due to several reasons. First, many common conditions present with similar symptoms or signs, leading to ambiguity in differentiating them from rare diseases. Second, different clinical experiences, diagnostic approaches, and cultural factors that may influence how these symptoms are perceived and managed across healthcare settings.
In line with this, the items multiple specialist referrals and specific red flags derived from hospital administrative data monitoring, and “invisibility” diagnostic challenges reached a borderline level of agreement (statement #5: 75.0% and statement #19 among the “clinical gateways”: 75.9%). According to our own interpretation, the uncertainty among panelists is likely to reflect the same underlying challenges, such as overlap with more common diagnostic pathways, variable and incomplete knowledge of atypical disease presentation, and negative or uncertain perception regarding the potential usefulness of hospital records and notes as source for diagnostic red flags.
The statements reaching a 100% consensus in the domain of potential clinical gateways underlined the importance of healthcare professional education to learn systematic methods aimed at excluding common conditions and focusing on the diagnostic suspect of rare disease (statement #17), the importance of an increased awareness of rare diseases among healthcare professionals, leading to a possible re-evaluation of subjects in light of a diagnostic suspect of rare disease (statement #20), and the relevance of the economic burden of a delayed diagnosis of rare disease for healthcare systems, patients and their families (statement #26). Other clinical gateways that reached a high degree of consensus following the RTD process included a comprehensive and updated electronic medical record as a tool to summarize the patient’s journey and identify potential red flags of rare disease, avoiding data dispersion and redundant tests (statement #23, 96.3% degree of consensus) (Table 2).
Discussion
A prompt identification of general signs and symptoms of rare disease is an urgent issue in healthcare policies, as late diagnosis or misdiagnosis can deeply affect the quality of life of patients and their caregivers, with a relevant psychological burden and a financial impact to individuals and healthcare systems15.
The diagnostic delay in rare disease
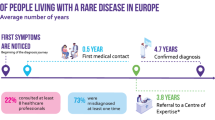
A recent retrospective patient survey conducted within the Rare Barometer programme, an initiative of EURORDIS-Rare Diseases Europe, revealed that the average TDT is 4.7 years, with 50% of people living with a rare disease waiting at least 9 months for a confirmed diagnosis after symptom onset, and 25% waiting more than 5 years9. The survey also revealed that the average time from symptom onset to first medical contact in Europe is approximately 5 months, while the average time from first medical contact to a confirmed diagnosis of rare disease is 4.3 years9. Another study conducted in Poland and collecting the responses from 925 caregivers of children with a rare disease revealed that the duration of the diagnostic journey spanned from 0 to 18 years, with an average time of 1.7 years, while the average number of physicians consulted before receiving the correct diagnosis was 4.816. A survey recently conducted in China and involving almost 2000 patients and caregivers, representing 104 different rare diseases, revealed a diagnostic delay of 1.4 ± 3.0 years. Patients experienced 1.6 ± 3.8 misdiagnoses between 3.2 ± 2.4 hospitals. Diagnoses of rare disease were concentrated in 10 large hospitals and 5 big cities, indicating a significant heterogeneity of medical resources in the Country. Patients also reported that the rare disease often led to difficulty in their education and employment, as well as to a significant financial burden. A battery of standardized tests demonstrated poor health status, depression, somatization, anxiety, and sleeping issues among both patients and caregivers17.
The main determinants of diagnostic delays in Europe are gender and age, and in particular symptom onset before 30 years of age and being a woman, in addition to living in Northern or Western Europe, the number of healthcare professionals consulted, misdiagnosis, referral to a center of expertise, unmet needs for psychological and financial support, having a genetic disease and a family history of rare disease9.
The Argo study
Multiple factors can affect a timely diagnosis of rare disease, and healthcare professionals need clear information and guidelines on when to suspect the presence of this kind of disorder. The Delphi methods assumed a central role in the latest years to develop guidance in healthcare practice using collaborative insight where data are limited or evidence is conflicting18. In particular, the RTD method selected for this study maximized the participation of experts from different areas, reduced the amount of time required to panelists, and enabled a real-time presentation of results, so that experts were able to perform multiple assessments and modify their opinion12.
This RTD study identified and recommended a series of clinical and non-clinical signals, tools and circumstances (red flags and clinical gateways) that should be considered by primary care professionals during the journey towards a diagnosis of rare disease (Table 2).
Recently, the International Rare Diseases Research Consortium (IRDiRC) assembled a global, multistakeholder task force to identify barriers and opportunities that could support primary healthcare professionals in addressing challenges posed by rare diseases19. The Argo RTD study identified some key indicators that were consistent with the outcomes of the IRDiRC task force, such as family medical history, clusters of birth defects, unusual presentations of common illnesses, neurodevelopmental delays or decline, and severe pathology that should be integrated into primary care practices to improve the identification and referral of cases of rare disease. Of interest, a range of red flags of rare disease initially identified by 79 different patient groups based in UK through a non-medical audience questionnaire, reached a consensus also in this experts’ opinion RTD study, thus leading to a convergence of common experiences and recommendations shared by both patients and physicians, even if based in different Countries20. In particular, a common consensus was reached on red flags across physical and psychosocial domains, with reference to the involvement of three or more organs or systems (statement #1), the pattern of genetic inheritance (statement #6), the continued presentation during childhood and adulthood (statement #14), multiple specialist referrals (statement #4), delayed diagnosis (statement #7) and misdiagnosis (statement #8)20. Of note, school concerns, reported as a potential red flag of rare disease by patient groups in UK, did not reach a significant expert consensus in this study (statement #11), suggesting that difficulties in the educational setting are not considered a typical challenge of young subjects with a rare disease. It is interesting to note that the role of schools in identifying potential indicators of a rare disease may vary significantly across these two different educational systems. In UK, the school system is structured to identify and separate students with specific difficulties, assigning them to distinct educational pathways. Conversely, in Italy, the guiding principle is educational inclusion, aiming to integrate students with difficulties into the standard education system while avoiding early categorization. This cultural difference may explain the lower consensus reached for statement # 11, since the concern that school involvement could lead to stigmatization or misdiagnosis may have influenced how this aspect was perceived by the Italian panelists.
A two-step Delphi survey involving all German centers for rare diseases and patient groups as experts of their rare disease highlighted the need to improve the diagnostic process in individuals with rare diseases, with a particular focus on metabolic and autoimmune diseases21.
Overall consistency of results about red flags of rare diseases obtained in this RTD study and in other surveys or questionnaires summarized above highlights homogeneous circumstances in the setting of the diagnostic suspect of a rare disease in different Countries and healthcare systems that require a global call to action.
For what concerns the “clinical gateways”, filling the gap in knowledge about rare diseases through education of healthcare professionals, focused meetings and scientific publications, is highly recommended by the experts (statements #17–20, Table 2). An increased awareness of rare diseases and the typical pattern of a diagnostic journey faced by patients and their families should also be increased among the general population and the stakeholders, as well as among schoolteachers and educators, for an effective collaboration between the community and the healthcare professionals (statements #21–22, 25). These recommendations are supported by other recently published indications. Among them, a survey involving 165 medical doctors taking their specialization courses in Poland revealed that most physicians lacked basic knowledge about the etiology, epidemiology and estimated prevalence of rare diseases, and many of them lacked preparation and training to distinguish rare diseases from more common conditions5. According to the authors, initiatives should be taken by the Academia to train physicians about rare diseases, regardless of medical specialization, and with a principle-based approach. Although it is impossible to be aware of every identified rare disease, physicians should still be equipped to recognize the so called “zebras” among the “horses”5. Consistently with these results, physicians from different hospitals in China revealed through a questionnaire that lack of rare disease awareness and inappropriate education in medical schools are a major issue in diagnostic delay and/or misdiagnosis of these disorders22. A similar urgent information need for emergency physicians about rare diseases came up from a large survey conducted by Zhou et al. in the same Country23. Of note, a lack of guidelines or consensus was indicated as the most important reason for the diagnostic delay of rare diseases by the emergency physicians involved in the survey23. Of interest, Medics4RareDiseases, a charity based in UK, created the online course “Rare Disease 101” to try to address the gap in formal education in the field of rare disease medicine using a disease-agnostic approach, obtaining encouraging early results24.
Centers for rare diseases concentrate expertise and knowledge about these disorders and play a major role worldwide in supporting diagnosis and treatment approaches25. In particular, centers for rare diseases could play a major role for genetic assessment in case of a diagnostic suspect. Actually, about 80% of rare diseases have a genetic basis, and several of them follow a pattern of inheritance indicative of a monogenic origin. Recent advancements in sequencing technologies revealed the genetic causes for newly identified rare diseases and helped identify new variants responsible for previously known disorders2. In addition, when exome or whole genome sequencing are unrevealing, different novel technological approaches can be applied to support the diagnosis and elucidate the molecular mechanism of rare diseases26. Actually, the low incidence, and/or the limited knowledge of the pathogenetic mechanisms, are responsible for the lack of EMEA or FDA-approved treatments for about 95% of the estimated 6000–10,000 rare diseases4. Nonetheless, even when an approved therapy is unavailable, an accurate diagnosis of rare disease can lead to symptomatic treatments and medical intervention, improving patients’ quality of life and extending their lifespan2. In addition, a diagnosis of rare disease can allow the participation in relevant clinical trials, prevent potentially ineffective and harmful treatments and allow the support of specific patient advocacy groups4,19. GPs and other healthcare professionals should be aware of the operations and goals of centers for rare disease in their area and refer to them when necessary. On the other hand, the centers for rare diseases should improve their visibility and access also through the implementation of user-friendly websites and providing timely feedback to physicians (statement #24)10.
Finally, panelists involved in this RTD study highlighted the importance of constantly updated and comprehensive electronic medical records as a tool to facilitate the identification of potential red flags of rare disease (statement # 23, Table 2). This aspect is of particular interest in the perspective of recent advances in the use of artificial intelligence (AI) and machine learning, as these tools could assist physicians and expedite the diagnosis of rare diseases27,28,29. In particular, algorithms can automate and systematize the clinical suspicion of a genetic disease by analyzing the information stored in electronic health records and creating predictive models to accelerate the identification of patients with a clinical profile representative of receiving a genetic test. The combination of targeted education and new technologies could help the population of rare disease patients (around 50%) affected by significant diagnostic delay, lowering the costs and finally improving patient outcomes30,65.
Limitations
We would like to highlight that the high level of consensus on red flags among panelists does not imply that these indicators should be automatically used as standalone screening tools for rare disease suspicion. The identification of a red flag should always be interpreted within a broader clinical context, taking into account sociodemographic variables and additional diagnostic factors. For example, a high number of emergency department visits may be an alert for a potential rare disease but could also reflect limited access to primary care services or socioeconomic disadvantage. The isolated use of red flags as a diagnostic filter could lead to an excessive number of false positives. Further validation is required and encouraged to confirm their ability to discriminate effectively the patients at higher risk while avoiding unnecessary diagnostic procedures or misclassification.
Other study limitations possibly relate to the composition of the voting panel of experts and to the subjectivity in initial selection of literature and statements. In particular, the panel is limited to Italian professionals and cultural or healthcare system differences might limit applicability elsewhere. Delphi is an opinion-based consensus process, so potentially different outcomes with different panels are intrinsically part of this procedure. We acknowledge that the inclusion of non-clinical experts may have influenced the level of agreement on certain items more closely related to direct patient interaction. For instance, red flag items such as “failure to standard therapies”, “length of stay”, “school concerns”, and “peculiar emotional phenomena”, which require a high degree of intimate knowledge of rare diseases and close contact with the families, did not achieve final degree of consensus due to the broad and heterogenous composition of the panel. However, their participation was considered essential to incorporate systemic, organizational, and policy-level perspectives, which are crucial for ensuring that clinical insights can be effectively translated into sustainable, real-world implementation strategies.
Conclusions
To the best of our knowledge, this is the first RTD study providing a consensus by a relatively large panel of experts about red flags and clinical gateways to be considered by primary care professionals in the troubled journey towards a diagnosis of rare disease. The multidisciplinary expertise and the multiplicity of voting panelists in this RTD study benefit the consensus process. Moreover, the constantly high response rate throughout the RTD study indicated that experts’ knowledge and opinions were well represented throughout the whole survey, and anonymity minimized the possibility of introducing bias in the consensus process, thus strengthening its validity.
The recommendations emerging from this survey represent a basis to reshape, adjust and optimize the process leading to an early recognition of rare diseases in the primary care setting and respond at least in part to the unmet needs of affected individuals and their families. This could improve the patient experience, optimize the use of available healthcare, financial and technological resources and reduce the challenges of the diagnostic odyssey. As Argo project evolves, future phases will intend to focus on disease-specific consensus-building and the extension of the methodology to a European context, with the aim of promoting cross-national alignment on early recognition strategies for rare diseases. In addition, a retrospective validation study is under evaluation to assess whether the proposed red flags are identifiable in clinical documentation preceding diagnosis, to evaluate their potential to support earlier suspicion and reduce diagnostic delay in real-world settings.
Data availability
The data sets generated and analyzed during the current study are available from the corresponding author on reasonable request.
References
Tisdale, A. et al. The IDeaS initiative: pilot study to assess the impact of rare diseases on patients and healthcare systems. Orphanet. J. Rare Dis. 16, 429 (2021).
Vaisitti, T. et al. The frequency of rare and monogenic diseases in pediatric organ transplant recipients in Italy. Orphanet. J. Rare Dis. 16, 374 (2021).
Schieppati, A., Henter, J. I., Daina, E. & Aperi, A. Why rare diseases are an important medical and social issue. Lancet 371, 2039–2041 (2008).
Baynam, G. et al. Global health for rare diseases through primary care. Lancet Glob. Health 12, e1192–e1199 (2024).
Walkowiak, D. & Domaradzki, J. Are rare diseases overlooked by medical education? Awareness of rare diseases among physicians in Poland: an explanatory study. Orphanet J. Rare Dis. 16, 400 (2021).
Chute, C. G. The rendering of human phenotype and rare diseases in ICD-11. J. Inherit. Metab. Dis. 41, 563–569 (2018).
Baxter, M. F., Hansen, M., Gration, D., Groza, T. & Baynam, G. Surfacing undiagnosed disease: consideration, counting and coding. Front. Pediatr. 11, 1283880 (2023).
Ramanayake, R. P. J. C. & Basnayake, B. M. T. K. Evaluation of red flags minimizes missing serious diseases in primary care. J. Fam. Med. Prim. Care 7, 315–318 (2018).
Faye, F. et al. Time to diagnosis and determinants of diagnostic delays of people living with a rare disease: Results of a Rare Barometer retrospective patient survey. Eur. J. Hum. Genet. 32, 1116–1126 (2024).
Druschke, D. et al. Potentials and current shortcomings in the cooperation between German centers for rare diseases and primary care physicians: results from the project TRANSLATE-NAMSE. Orphanet. J. Rare Dis. 16, 494 (2021).
Jones, J. & Hunter, D. Consensus methods for medical and health services research. BMJ 311, 376–380 (1995).
Varndell, W., Fry, M. & Elliott, D. Applying real-time Delphi methods: development of a pain management survey in emergency nursing. BMC Nurs. 20, 149 (2021).
Quirke, F. A. et al. Multi-round versus real-time Delphi survey approach for achieving consensus in the COHESION core outcome set: a randomised trial. Trials 24, 461 (2023).
Diamond, I. R. et al. Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies. J. Clin. Epidemiol. 67, 401–409 (2014).
Yang, G. et al. The national economic burden of rare disease in the United States in 2019. Orphanet. J. Rare Dis. 17, 163 (2022).
Domaradzki, J. & Walkowiak, D. Invisible patients in rare diseases: parental experiences with the healthcare and social services for children with rare diseases. A mixed method study. Sci. Rep. 14, 14016 (2024).
Li, X. et al. A questionnaire-based study to comprehensively assess the status quo of rare disease patients and care-givers in China. Orphanet. J. Rare Dis. 16, 327 (2021).
Nasa, P., Jain, R. & Juneja, D. Delphi methodology in healthcare research: How to decide its appropriateness. World J. Methodol. 11, 116–129 (2021).
Adams, D. R. et al. Addressing diagnostic gaps and priorities of the global rare diseases community: Recommendations from the IRDiRC diagnostics scientific committee. Eur. J. Med. Genet. 70, 104951 (2024).
Al-Attar, M., Butterworth, S. & McKay, L. A quantitative and qualitative analysis of patient group narratives suggests common biopsychosocial red flags of undiagnosed rare disease. Orphanet. J. Rare Dis. 19, 172 (2024).
Blöß, S. et al. Diagnostic needs for rare diseases and shared prediagnostic phenomena: Results of a German-wide expert Delphi survey. PLoS ONE 12, e0172532 (2017).
Li, X. et al. Rare disease awareness and perspectives of physicians in China: a questionnaire-based study. Orphanet. J. Rare Dis. 16, 171 (2021).
Zhou, L., Xu, J. & Yang, J. Poor education and urgent information need for emergency physicians about rare diseases in China. Orphanet. J. Rare Dis. 17, 211 (2022).
Dunne, T. F., Jeffries, D. & Mckay, L. Rare disease 101: an online resource teaching on over 7000 rare diseases in one short course. Orphanet. J. Rare Dis. 19, 275 (2024).
Salvatore, M. et al. Improving diagnosis for rare diseases: the experience of the Italian undiagnosed rare diseases network. Ital. J. Pediatr. 46, 130 (2020).
Marwaha, S., Knowles, J. W. & Ashley, E. A. A guide for the diagnosis of rare and undiagnosed disease: beyond the exome. Genome Med. 14, 23 (2022).
Wojtara, M., Rana, E., Rahman, T., Khanna, P. & Singh, H. Artificial intelligence in rare disease diagnosis and treatment. Clin. Transl. Sci. 16, 2106–2111 (2023).
Visibelli, A., Roncaglia, B., Spiga, O. & Santucci, A. The impact of artificial intelligence in the odyssey of rare diseases. Biomedicines 11, 887 (2023).
Schaefer, J., Lehne, M., Schepers, J., Prasser, F. & Thun, S. The use of machine learning in rare diseases: a scoping review. Orphanet. J. Rare Dis. 15, 145 (2020).
Morley, T. J. et al. Phenotypic signatures in clinical data enable systematic identification of patients for genetic testing. Nat. Med. 27, 1097–1104 (2021).
Faviez, C. et al. Objectivizing issues in the diagnosis of complex rare diseases: lessons learned from testing existing diagnosis support systems on ciliopathies. BMC Med. Inform. Decis. Mak. 24, 134 (2024).
Yahia, R., Rafi, I. & Evans, W. Implementing a digital rare disease case-finding tool in UK primary care: a qualitative study of health professionals’ experience. Br. J. Gen. Pract. 74, (2024).
Tahani, N. et al. Consensus clinical management guidelines for Alström syndrome. Orphanet. J. Rare Dis. 15, 253 (2020).
Vandeborne, L., van Overbeeke, E., Dooms, M., De Beleyr, B. & Huys, I. Information needs of physicians regarding the diagnosis of rare diseases: A questionnaire-based study in Belgium. Orphanet. J. Rare Dis. 14, 99 (2019).
Kaski, J. P. et al. Cardiomyopathies in children and adolescents: aetiology, management, and outcomes in the European Society of Cardiology EURObservational Research Programme Cardiomyopathy and Myocarditis Registry. Eur. Heart J. 45, 1443–1454 (2024).
Merker, V. L. et al. Understanding barriers to diagnosis in a rare, genetic disease: Delays and errors in diagnosing schwannomatosis. Am. J. Med. Genet. A 188, 2672–2683 (2022).
Germain, D. P. et al. The benefits and challenges of family genetic testing in rare genetic diseases-lessons from Fabry disease. Mol. Genet. Genomic Med. 9, e1666 (2021).
Howard, J. F. et al. Safety and efficacy of zilucoplan in patients with generalised myasthenia gravis (RAISE): a randomised, double-blind, placebo-controlled, phase 3 study. Lancet Neurol. 22, 395–406 (2023).
Goto, S. et al. Artificial intelligence-enabled fully automated detection of cardiac amyloidosis using electrocardiograms and echocardiograms. Nat. Commun. 12, 2726 (2021).
Porcari, A. et al. Diagnostic-therapeutic care pathways for patients with cardiac amyloidosis - SIC/ANMCO Consensus document. Edited by the Italian Cardiac Amyloidosis Network (RIAC). G Ital. Cardiol. 25, 900–920 (2024).
Emdin, M. et al. Approach to the diagnosis and management of patients with cardiac amyloidosis. A consensus document by the Tuscan section of the Italian Association of Hospital Cardiologists (ANMCO) and the Tusco-Umbrian section of the Italian Society of Cardiology (SIC). G Ital. Cardiol. 22, 621–634 (2021).
Lim, S., Halandras, P. M., Bechara, C., Aulivola, B. & Crisostomo, P. Contemporary management of acute mesenteric ischemia in the endovascular era. Vasc. Endovascular Surg. 53, 42–50 (2019).
Ferreira, G. C. et al. Iron Hack - A symposium/hackathon focused on porphyrias, Friedreich’s ataxia, and other rare iron-related diseases. F1000Res 8, 1135 (2019).
Diab, N. S. et al. Molecular genetics and complex inheritance of congenital heart disease. Genes 12, 1020 (2021).
Jean, F., Stuart, A. & Tarailo-Graovac, M. Dissecting the genetic and etiological causes of primary microcephaly. Front. Neurol. 11, 570830 (2020).
Bhatia, N. S. et al. Singapore undiagnosed disease program: Genomic analysis aids diagnosis and clinical management. Arch. Dis. Child 106, 31–37 (2021).
Ward, A. J. et al. Genetic services survey-experience of people with rare diseases and their families accessing genetic services in the Irish Republic. J. Community Genet. 14, 583–592 (2023).
Mendoza-Alvarez, A. et al. A catalog of the genetic causes of hereditary angioedema in the Canary Islands (Spain). Front. Immunol. 13, 997148 (2022).
Graf, J. et al. Misdiagnoses and delay of diagnoses in Moyamoya angiopathy-a large Caucasian case series. J. Neurol. 266, 1153–1159 (2019).
Zhang, L. et al. Diagnosing relapsing polychondritis remains a common challenge: experience from a Chinese retrospective cohort. Clin. Rheumatol. 39, 2179–2184 (2020).
Lodhia, J. et al. Case series of high-grade soft tissue sarcoma of the lower limb with delayed diagnosis: Experience at a tertiary hospital in northern Tanzania. Int. J. Surg. Case Rep. 97, 107475 (2022).
Cappello, M. et al. Identification and management of gastrointestinal manifestations of hereditary transthyretin amyloidosis: Recommendations from an Italian group of experts. Dig. Liver Dis. 56, 1014–1020 (2024).
Smeets, N. et al. Congenital myasthenic syndromes in Belgium: Genetic and clinical characterization of pediatric and adult patients. Pediatr. Neurol. 158, 57–65 (2024).
Salvatore, M. et al. The Italian registry for patients with Prader-Willi syndrome. Orphanet. J. Rare Dis. 18, 28 (2023).
Gordon, D., Watson, A., Desurkar, A., Cowley, L. & Hiemstra, T. F. Assessing the role of ketogenic dietary therapy in ring chromosome 20 syndrome: A patient-led approach. Epilepsia Open 5, 295–300 (2020).
Mazzucato, M. et al. A population-based registry as a source of health indicators for rare diseases: the ten-year experience of the Veneto Region’s rare diseases registry. Orphanet. J. Rare Dis. 9, 37 (2014).
Miravitlles, M. et al. Clinical and functional characteristics of individuals with alpha-1 antitrypsin deficiency: EARCO international registry. Respir. Res. 23, 352 (2022).
Kohlschütter, A. & van den Bussche, H. Early diagnosis of a rare disease in children through better communication between parents, physicians and academic centers. Z. Evid. Fortbild. Qual. Gesundhwes. 141–142, 18–23 (2019).
Kaywanga, F. et al. Rare diseases in Tanzania: a National Call for Action to address policy and urgent needs of individuals with rare diseases. Orphanet. J. Rare Dis. 17, 343 (2022).
Chong-Neto, H. J. et al. Are pediatricians familiar with hereditary angioedema?. World Allergy Organ J. 16, 100783 (2023).
Grzybowski, J. et al. Diagnosis and treatment of transthyretin amyloidosis cardiomyopathy: A position statement of the Polish Cardiac Society. Kardiol. Pol. 81, 1167–1185 (2023).
Caruana, M. et al. HTAD patient pathway: Strategy for diagnostic work-up of patients and families with (suspected) heritable thoracic aortic diseases (HTAD). A statement from the HTAD working group of VASCERN. Eur. J. Med. Genet. 66, 104673 (2023).
Aldharee, H. Duchenne muscular dystrophy in Saudi Arabia: A review of the current literature. Front. Neurol. 15, 1392274 (2024).
Nurchis, M. C. et al. Bayesian cost-effectiveness analysis of whole genome sequencing versus whole exome sequencing in a pediatric population with suspected genetic disorders. Eur. J. Health Econ. 25, 999–1011 (2024).
Cirillo, C. et al. Diagnostic delay in rare diseases in the Campania region: addressing ageing, gender disparities, and the “postcode lottery effect” to reduce the patient odyssey. Eur. J. Public Health. ckaf088 (2025).
Acknowledgements
Elena Caproni, PhD and Enrico Nello, AI-Engineer of Helaglobe, provided support in RTD development and set-up.
Funding
The publication was supported by Helaglobe (Florence, Italy), which has no commercial interest in selling health related products.
Author information
Authors and Affiliations
Consortia
Contributions
G.L. had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: G.L, F.D.I., M.M., L.Pecchia, G.Piccinocchi, L.S., M. S., D.C., L.Politi, I.S., A.S., P.F.; Statements voting and commenting: G.A., A.A., M.A., P.A.A., S.B., R.B., F.B., C.B., S.B., A.B., P.C., M.C., T.C., E.D., F.D.I., S.D.M., P.F., M.G., L.G., M.G., G.L., L.M., B.M., M.M., G.M., G.Parenti, L. Pecchia, G.Piccinocchi,, M.P., A.P., R.P., A.R., L.R., D.R., E.Rossi, E. Rozzi, M.R., L.S., S.S., I.S., C.S., M. S., R. S., A.S., C.S., S. Sica, F.S., P.S., G.T., A.T., R.T., M.T., A.V., R.V.; Acquisition, analysis, or interpretation of data: G.L., F.D.I., M.M., L.Pecchia, G.Piccinocchi, L.S., M. S., D.C., L.Politi, F.T., A. Forte, M.C., C.D.S., A.Fusco, I.S., A.S., P.F.; Drafting of the manuscript: G.L., L.Politi, A. Forte, P.F.; Critical review of the manuscript for important intellectual content: G.L., F.D.I., M.M., L.Pecchia, G.Piccinocchi, L.S., M. S., I.S., A.S., P.F.. Statistical analysis: F.T.; Obtained funding: None; Administrative, technical, or material support: G.L., D.C., L.Politi, F.T., M.C., C.D.S., A.Fusco; Supervision: G.L., P.F. All authors critically reviewed, edited, and added to the manuscript, as well as approved the final version of the manuscript and its submission.
Corresponding author
Ethics declarations
Ethical approval
Ethical approval was waived by the Azienda dei Colli-Vanvitelli (Campania 2) Ethics Committee (Italy) for this study, as it did not involve clinical trials or patient data.
Competing interests
M.C., F.D.I., C.D.S., P.F., A. Fusco, G.L., B.M., L. Pecchia, L.S., I.S., A.S., report no competing interests. D.C., L.Politi, A.Forte and F.T. work for Helaglobe which served as consultant for Abiogen, Alexion, AOP health, Apellis, Convatec, Daichii-sankyo, Doctolib, Fidia, Gore, GSK, Hologic, Lilly, Mirum, Molteni, Orphalan, Recordati rare diseases, SOBI, Theramex, Tillotts, UCB, Uriach, Visufarma. G.P. reported receiving a Research grant from Zambon, Spark tx. He also received fees for participation in Clinical Studies sponsored by Synageva, Biomarin, Amicus tx, as a speaker from Takeda Shire, Sanofi Genzyme, Amicus tx, Biomarin and for Travel reimbursements from Shire Takeda, Sanofi Genzyme, Medifood, Vitaflo, Recordati, Piam farmaceutici. M.M. reported receiving honoraria as Advisor or speaker for AstraZeneca, Abbvie, GSK, Lilly, UCB, Biogen, BMS, Idorsia, Molteni, Otsuka, Roche, Novartis. M.S. reported fee for advisory boards and research grants from Alexion, Biomarin, Chiesi, Denali, Ultragenix, Sanofi, Takeda.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Limongelli, G., De Iaco, F., Mosca, M. et al. Argo Delphi consensus statement on red flags and clinical gateways towards rare disease diagnosis. Sci Rep 15, 39411 (2025). https://doi.org/10.1038/s41598-025-23081-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-23081-0
