
Abstract
Metagenomic next-generation sequencing (mNGS) has been widely used in infectious diseases. However, reports on mNGS for lower respiratory tract infection (LRTI) diagnosis remain limited, potentially offering significant value for improving pathogen identification. This study evaluates the diagnostic performance and clinical value of mNGS compared to traditional methods in LRTI. We analyzed traditional and mNGS detection results from 165 patients with suspected LRTI using different specimens including bronchoalveolar lavage fluid (BALF), blood, tissue samples, and pleural effusion. We compared diagnostic differences and characteristics between mNGS and traditional methods, and evaluated the effect of mNGS results on antibiotic treatment.
Among 165 cases, 146 (88.48%) patients with LRTI had microbial etiology finally identified. Compared with traditional diagnostic methods, mNGS showed significantly higher positive rate (143/165, 86.7% vs 69/165, 41.8%, P < 0.05). The diagnostic performance of mNGS was not affected by sample types. mNGS demonstrated significant advantage in detecting poly-microbial infections and rare pathogens. Twenty-nine kinds of pathogens were detected only by mNGS, including non-tuberculous mycobacteria (NTM), Prevotella, anaerobic bacteria, Legionella gresilensis, Orientia tsugamushi, and viruses. The pathogen spectrum differed between immunocompetent and immunocompromised individuals. mNGS resulted in treatment changes in 119 patients (72.13%), with 54 patients (32.73%) having reduced antibiotics. mNGS has obvious advantages over traditional detection methods with results unaffected by sample types. mNGS demonstrates significant value for pathogen detection and may provide guidance in clinical practice.
Similar content being viewed by others

Introduction
Lower respiratory tract infections (LRTIs), commonly categorized as community-acquired pneumonia (CAP) or hospital-acquired pneumonia (HAP), represent a significant global health concern due to high adult mortality, despite widespread antibiotic use1. LRTI diagnosis typically involves a combination of clinical assessment, laboratory tests, radiological findings, and microbial culture/molecular results2. Identifying the causative pathogen is crucial for effective LRTI treatment. However, in China, traditional diagnostic methods fail to identify the pathogen in over half of LRTI cases3. Given that these traditional methods are time-consuming and exhibit low positivity rates, antibiotic use often remains empiric, based on suspected pathogens and clinical presentation4. Culture-negative infections, defined as clinically suspected infectious conditions where conventional culture methods fail to identify causative pathogens, represent a significant diagnostic challenge in LRTI management. Accurate pathogen identification is paramount for targeted treatment, emphasizing the critical need for rapid and precise pathogen identification in LRTI to enable effective infection control and minimize inappropriate antibiotic use.
Metagenomic next-generation sequencing (mNGS) is an advanced method for pathogen diagnosis that sequences all nucleic acids present in clinical specimens without prior amplification of specific targets. Wilson’s 2014 Leptospira diagnosis using mNGS pioneered its use in infectious disease5, and subsequent studies confirm its value in detecting pathogens across infections like encephalitis6, skin infections7, and pneumonia8. Chen specifically highlighted mNGS’s utility in severe pneumonia diagnosis, often revealing pathogens missed by conventional culture and PCR. Traditional pneumonia diagnostics are limited by sputum collection challenges and the low sensitivity of blood cultures9. In contrast, mNGS offers a broader detection range, identifying bacteria, viruses, fungi, and atypical pathogens often missed by standard methods. While mNGS can analyze diverse fluid specimens, bronchoalveolar lavage fluid (BALF), tissue, blood, and pleural effusion are most commonly used for mNGS-based diagnostics. Though often reserved for complex cases in developed nations, particularly among immunocompromised patients or those with central nervous system infections10,11, mNGS serves as a crucial supplement, especially in settings with limited PCR and reliance on culture, addressing PCR’s limited scope and constrained hospital testing capacity. In China, traditional molecular diagnostics are primarily limited to targeted PCR assays for common respiratory pathogens and culture-based methods. Many hospitals lack comprehensive multiplex PCR panels available in developed countries, creating diagnostic gaps that mNGS can potentially address. This limited molecular diagnostic infrastructure, combined with the high burden of complex respiratory infections including tuberculosis and atypical pathogens, highlights the particular need for mNGS implementation in this setting11,12.
Despite growing evidence supporting mNGS utility, several critical gaps remain in our understanding of its clinical application in LRTI diagnosis. Most previous studies have been limited by small sample sizes, single-center designs, or focus on specific patient populations. Furthermore, comprehensive comparisons across different specimen types and systematic evaluation of clinical impact on antibiotic management remain incomplete. The influence of prior antibiotic exposure on comparative diagnostic performance between mNGS and traditional methods has not been adequately addressed.
Nevertheless, to our knowledge, the impact of mNGS for etiological detection in LRTI were still limited and not comprehensive. Identifying the pathogen of LRTI plays a vital role in the initial antimicrobial therapy. A total of 204 adult patients suspected with LRTI, with complete clinical data of mNGS and traditional results, were reviewed in our study. Only 165 patients were finally investigated and evaluated the effect and clinical performance of mNGS in etiological diagnosis at last. The present study addresses these knowledge gaps through a systematic evaluation of mNGS diagnostic performance compared to traditional methods in a large cohort of LRTI patients, with comprehensive analysis across multiple specimen types and detailed assessment of clinical impact on antimicrobial therapy. This investigation seeks to systematically evaluate the diagnostic performance of mNGS compared to conventional methods. It aims to address critical clinical questions regarding: the potential of mNGS to improve pathogen detection rates, particularly in diagnostically challenging scenarios such as culture-negative infections or opportunistic infections in immunocompromised hosts; the capacity of mNGS to decrease time-to-diagnosis, thereby enabling earlier initiation of targeted therapeutic interventions; the constraints associated with mNGS, including financial expenditures, bioinformatic complexities, and the prevalence of false-positive results stemming from contamination, which could influence its clinical adoption; and the extent to which mNGS yields measurable improvements in patient prognoses, encompassing reduced mortality rates, shortened lengths of hospitalization, or a decrease in the inappropriate utilization of antimicrobial agents.
Experimental materials and methods
Patients and study design
The study was produced in Ningbo medical center of Lihuili hospital between January 2018 and December 2020. The study was conducted in accordance with the ethical standards of the institutional and national research committees and with the 1964 Helsinki Declaration and its later amendments. We included 204 cases of suspected LTRI if they presented with at least two of the following symptoms: fever (temperature > 38.0°C), cough with sputum production, dyspnea, or chest pain, in conjunction with radiographic evidence of pulmonary infiltrates on chest X-ray or CT scan. The Inclusion criteria refer to the following points: (1) presence of the aforementioned symptoms and radiologic evidence of LRTI; (2) Consent to undergo mNGS testing at patient’s own expense (3) patients ≥ 14 years of age. (4)availability of paired conventional microbiological tests(culture, PCR, or antigen testing).The exclusion criterion was the final diagnosis with non-infectious and incomplete clinical/microbiological data. Patients were excluded if they had received more than 7 days of targeted antimicrobial therapy prior to specimen collection, to minimize potential bias in traditional culture results.
Diagnostic criteria
The final pathogen diagnosis was determined by a multidisciplinary team, including infectious disease specialists, microbiologists, and radiologists, through a comprehensive analysis of mNGS results (pathogen-specific reads, genomic coverage, and confidence thresholds), traditional methods such as culture (bacterial/fungal), PCR, antigen testing (e.g., Legionella urinary antigen), and microscopy (e.g., acid-fast staining for Mycobacterium). Clinical correlation involved imaging progression (e.g., chest CT lesion resolution) and host factors (e.g., immunosuppression, travel history)13. When multiple traditional methods were used to detect the same pathogen type, positive results from any method were considered positive for that pathogen category. Discordant results between traditional methods were resolved through clinical correlation and repeat testing when possible.
Data collection and variables
For each patient, we analyzed the following parameters: demographics, including age and sex, and comorbidities such as COPD and diabetes; imaging manifestations, including CT findings such as lobar consolidation and cavitation; lesion size changes measured Pre-therapy and post-therapy by radiologists; clinical conditions, encompassing immunocompromised status (e.g., due to HIV or chemotherapy) and complications (e.g., septic shock and ARDS); and antibiotic adjustments, including initial empirical therapy and subsequent targeted therapy guided by mNGS/traditional results (e.g., de-escalation from meropenem to penicillin for S. pneumoniae). Additional variables collected included timing and duration of antibiotic pre-treatment, specific antimicrobial agents used, and interval between antibiotic initiation and specimen collection.
We analyzed the following parameters for each patient: Demographics, including age and sex, as well as comorbidities such as COPD and diabetes. Imaging manifestations, including CT findings like lobar consolidation and cavitation. Lesion size changes were measured Pre-therapy and post-therapy by radiologists. Clinical conditions encompassed immunocompromised status, for example, due to HIV or chemotherapy, and complications such as septic shock and ARDS. Antibiotic adjustments included empirical therapy, which is the initial regimen before diagnostics, and targeted therapy, which is the post-mNGS/traditional results, such as de-escalation from meropenem to penicillin for S. pneumoniae.
Clinical Efficacy: Firstly, symptomatic improvement includes the resolution of fever, cough, and dyspnea within 7 days, as well as a CRP/PCT decline of more than 50% from baseline. Radiologic improvement is defined as a reduction of at least 30% in lesion size on follow-up CT, according to RECIST-like criteria. Secondary outcomes encompass the duration of hospitalization and 30-day mortality.
The definition of hypoimmunity was met when more than one of the following risk factors were found: (1) diabetes; (2) neutropenia; (3) accept the immunosuppressive regimen; (4) Chronic lung diseases; (5) Patients with hematology or solid cancer received chemotherapy during the last 3 months; (6) Cerebrovascular diseases patients of high risk with pneumonia; (7) Chronic and long-term Glucocorticoids or biological drug use for autoimmune diseases; (8) other immunocompromised state not including above all.
Quality Control and Contamination Prevention: To minimize contamination risk, all specimens were collected using sterile techniques and processed within 4 h of collection. Negative controls (sterile water) were included in each mNGS sequencing batch. Laboratory personnel followed strict aseptic protocols, and dedicated equipment was used for each specimen type. Environmental monitoring was performed regularly in the mNGS laboratory.
Specimen collection
Samples were collected from patients suspected with pulmonary infection, including BALF, tissue, blood and pleural effusion. BALF was obtained through the bronchoscopy (K201/K203, Olympus, Tokyo, Japan) conducted by the operation technician of the Respiratory Endoscopy Center. Tissue samples were obtained by CT-guided lung puncture biopsy, precisely locate the region of the lesion, and then obtained by the needle in all patients. And the sample tissue was ground with a tissue homogenizer to use. Blood samples were collected by the nurse when the patient has the fever (T > 38.0℃). Pleural effusion obtained through closed thoracic drainage, about 10ml. Average number of BALF was 20 ml, tissue samples was were obtained from lung biopsy and divided into 4 pieces. Each sample were equally divided into two parts for traditional pathogens detection and mNGS analysis. We choose the appropriate method to collect the specimen according to the clinical experience.
The traditional method. Traditional diagnostic methods included standardized protocols for bacterial/fungal culture, molecular testing, antigen detection, and microscopic examination. The traditional method include pathology, pathogen culture and serum antigen detection. The culture was identified according to the operating procedures for national clinical testing.It mainly refers to culture for Bacterial/Fungal Culture(BioMérieux, ,Marcy-l'Étoile, France; Cat. No. 43041;SDA; Thermo Fisher Scientific, Waltham, MA, USA;Cat. No. R454602),Smear Microscopy(Sigma-Aldrich, St. Louis, MO, USA; Cat. No. CS0003, Sigma-Aldrich, Cat. No. GMS1;Solarbio, Beijing, China;Cat. No. G1281),Nucleic Acid Test for virus(e.g.,Influenza A/B,SARS-CoV-2)or Atypical Pathogen (Altona Diagnostics GmbH, Hamburg, Germany; Cat. No. 711011)., Antigen Detection Test(Galactomannan:Bio-Rad Laboratories, Hercules, CA, USA; Cat.No.62794) and Cryptococcus Determination of Capsular Polysaccharide Antigen(Immuno-Mycologics, Inc., Norman, OK, USA; Cat. No. CrAg3001) on serum samples, Acid-Fast Staining(Sigma-Aldrich, St. Louis, MO, USA; Cat. No. HT50) detect mycobacterium. All traditional methods were performed according to standard operating procedures with appropriate positive and negative controls. Quality assurance protocols were implemented for each testing modality.
And the pathology method detected as follows. The lung biopsy specimens were fixed with 4% formaldehyde (Cat. No. F0030;Sunbio, Ningbo, China) and sent to the pathology laboratory within 2 h, where they were dehydrated, paraffin-coated (Cat. No. HT-PW100;Hao Tian, Suzhou, China), sliced and stained with hematoxylin and eosin (Cat. No. G1120; Solarbio, Beijing, China ) according to the operation guide. Check for the visible pathogens (fungal hyphae) and inflammatory cell infiltration under microscope. In addition, in order to distinguish the bacteria, fungi, Mycobacterium tuberculosis and Pneumocystis carinii, the samples were stained with Ziel Nielsen acid resistant, silver hexamine, Schiff base periodate (PAS) et al.14.
Metagenomic next-generation sequencing analysis
All samples were stored in sterile containers in a timely manner and took to the mNGS laboratory to ensure samples were placed at 4°C prior to analysis. Nucleic acid detection and sequencing were carried out through the platform of BGISEQ-50/MGISEQ-2000 (BGI-Nanjing, NANJING, China). The current mNGS protocol focused on DNA sequencing only and did not include RNA sequencing, which may limit detection of RNA viruses such as influenza, respiratory syncytial virus, and rhinovirus. DNA sequence in the sample compared it with the microbial nucleic acid sequence in the database, and identify the pathogenic microorganisms in combination with clinical manifestations. The minimum detection limit of this technology is 5–50 copies/M, and the detection including 6350 kinds of bacteria, 1064 kinds of fungi, 4945 kinds of viruses and 234 kinds of parasites, but the detection without including Ribonucleic Acid (RNA) sequencing. After that, we obtained accurate and fast short read alignment with Burrows-Wheeler transform (BWA: https://bio-bwa.SourceForge.Net) in order to get the high-quality data15. The possible pathogens are finally identified based on the sequence number or other clinical method. Bioinformatics analysis included removal of human DNA sequences, alignment to microbial databases, and application of stringent thresholds to minimize false-positive results. Contamination assessment was performed by comparing results with negative controls and environmental monitoring data.
Statistical analyses
Statistical analysis SPSS v20 (IBM Corp., Armonk, NY, USA)was used to analyze all data. Continuous variables are expressed as the mean ± standard error of the mean (SD) and categorical variables are expressed as numbers (percentage). We used A2 × 2 contingency table to detect the sensitivity and specificity of mNGS and traditional method in different samples. The difference of continuous variables was detected by T test, while the categorical variables was conducted by one-way. Subgroup analyses were performed to assess the impact of prior antibiotic treatment on diagnostic performance. Stratified analyses compared results between patients with and without prior antibiotic exposure. P < 0.05 was considered to indicate a statistically significant difference.
Results
Characteristics of the patients
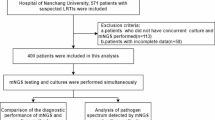
This study enrolled patients between January 2018 and December 2020 (Table 1). From an initial cohort of 204 patients, 165 were ultimately diagnosed with LRTI and included in the final analysis. This cohort comprised 58 females and 107 males, with ages ranging from 16 to 83 years (mean ± SD, 57.58 ± 13.10 years) (Table 1). Specimens were classified as bronchoalveolar lavage fluid (BALF) (n = 87, 52.7%), tissue (n = 42, 25.5%), pleural effusion (n = 16, 8.2%), and blood (n = 20, 12.1%). A significant proportion of patients (93.4%) had received antimicrobial therapy prior to specimen collection. Approximately half of the patients (76 of 165) had underlying medical conditions, including immune system diseases (n = 10), diabetes mellitus (n = 10), malignant neoplasms (n = 9), and chronic lung diseases (n = 22) such as chronic obstructive pulmonary disease, asthma, pulmonary fibrosis, interstitial lung disease, and bronchiectasis. Other conditions included severe pneumonia (n = 8), sequelae of cerebral infarction (n = 6), and acquired immunodeficiency syndrome (AIDS, n = 2). Cough (64.2%) and fever (39.4%) were the most common presenting clinical symptoms. All patients exhibited stable vital signs upon enrollment (Table 1 and Fig. 1). Among the 149 patients who received prior antibiotic treatment, mNGS maintained higher sensitivity compared to traditional methods (85.2% vs 38.9%, P < 0.05), while in antibiotic-naive patients, the difference remained significant (92.3% vs 50.0%, P < 0.05).

Flow diagram of the study. Abbreviations: ID, infectious disease; NID, noninfectious disease.
Compare and concordance of mNGS relative to traditional methods
In this study, a likely pathogen was identified in 83.6% (138/165) of LRTI patients when mNGS results were combined with those from traditional etiological detection methods (Table 1). The overall sensitivity of mNGS was 86.7% (143/165 patients), significantly higher than the 41.8% (69/165 patients) sensitivity of traditional methods (Fig. 2A, P < 0.05). Concordance between mNGS and traditional methods in identifying LRTI etiology was only 32.3% (20 cases). Among the patients with double-positive results, the pathogens were completely matched in only 20 cases (32.3%), while 21 cases (33.9%) showed inconsistencies (Fig. 2B). This discrepancy may be attributed to the detection of RNA viruses by respiratory virus antigen assays and Cryptococcus by the Cryptococcal Antigen Latex Agglutination System, both of which were missed by mNGS. Another possible explanation is that normal flora species were considered suspected pathogens when sequence reads were near the established threshold in double-positive patients.

(A) Comparison of sensitivity between mNGS and traditional method in patients with LRTI. (B) Consistency between traditional and mNGS were showing in the Composite pie. The double-positive result between traditional and mNGS results was 62 (37.6%); of the double-positive patients 32.3% (20 cases) were completely matched, while 33.9% (21 cases) were inconsistent.
Difference of mixed infection and pathogen spectrum between different immune status individuals
As shown in Fig. 3B, the positive rate for identifying multiple potential pathogens was significantly higher with mNGS than with traditional methods (P < 0.05). mNGS identified one potential pathogen in 57 patients (34.5%) and more than one pathogen in 96 patients (55.2%) out of the 165 patients. The sensitivity of mNGS for detecting polymicrobial infections (55.2%) was significantly higher than that of traditional methods (7.3%) (Fig. 3B, P < 0.05).

(A) Bar graph showing common combinations of mixed infections among immunocompetent and immunocompromised patients. (B) The proportion of multiple microorganism in LRTI patients conducted by traditional and mNGS showing in the B Bar graph.
Bacterial-bacterial co-infections were the most frequent in immunocompetent patients, whereas bacterial-fungal and single bacterial infections were the predominant combinations in immunocompromised patients (Fig. 3A). This suggests that patients with different immune statuses may be susceptible to different forms of pathogen involvement.
Pathogen detection between mNGS and traditional method detecting
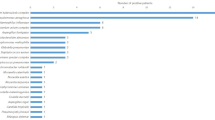
Traditional methods detected 18 types of pathogens in positive patients, primarily bacteria (72.22%), followed by fungi (22.22%) and viruses (5.6%). In contrast, mNGS identified 47 types of pathogens in positive patients, with a similar bacterial prevalence (72.82%), but higher viral detection (12.5%) and lower fungal detection (14.6%). Overall, mNGS demonstrated a higher detection rate for bacteria (123 vs 55), fungi (42 vs 18), and viruses (36 vs 1) compared to traditional methods (Fig. 4A).

(A) Pathogen Species distribution detected by mNGS and traditional method.A NTM, non-tuberculous mycobacteria; Mycobacterium Tuberculosis ,MTB; A.baumannii,Acinetobacter baumannii; EBV, Epstein-Barr virus; CMV, Human cytomegalovirus; HSV, Herpes simplex virus; H1N1, Hemagglutinin 1 Neuraminidase 1. P.jirovecii, Pneumocystis jirovecii. (B) Pathogen Species distribution in different patients.
mNGS detected bacterial infections in 123 patients (74.55%), significantly more than traditional methods (55 patients, 33.33%). The most common bacteria identified by mNGS were non-tuberculous mycobacteria (NTM, 13.94%),Pseudomonas aeruginosa (13.33%), Mycobacterium tuberculosis (MTB, 12.73%),Prevotella (12.73%), anaerobic bacteria (6.06%), and Enterococcus (6.06%). Traditional methods most frequently detected MTB (10.30%), Streptococcus pneumoniae (4.85%), Pseudomonas aeruginosa (4.24%), Acinetobacter baumannii (3.03%), Klebsiella pneumoniae (3.03%), Enterococcus (2.42%), and Stenotrophomonas maltophilia (2.42%).
mNGS detected fungal infections in 42 patients (24.45%), compared to 18 patients (10.91%) by traditional methods. The most common fungi identified by mNGS were Aspergillus (8.48%), Pneumocystis jirovecii (7.27%), Candida (6.67%), Cryptococcus neoformans (1.82%), Penicillium marneffei (0.61%), and Schizophyllum commune (0.61%) (Fig. 4A).
mNGS detected viral infections in 26 patients (15.76%), while traditional methods identified only one case (6.06%). The viruses detected by mNGS were all DNA viruses, including EBV (16 cases), HSV (9 cases), CMV (7 cases), and single cases of human herpesvirus types 5 and 7, and Human adenovirus 7 (Fig. 4A). While mNGS detected a broader range of pathogens, a single H1N1 case was identified by antigen serology but missed by mNGS.
mNGS exhibited higher sensitivity than traditional methods for detecting NTM, Prevotella, anaerobic bacteria, Enterococcus, Streptococcus, Actinomyces, Stenotrophomonas maltophilia, Mycoplasma pneumoniae, Streptococcus constellatus, Legionella gresilensis, Orientia tsutsugamushi, and viruses (Fig. 4A).
Pathogen spectra varied based on immune status (Fig. 4B). In immunocompetent patients, frequent pathogens included MTB (13.5%), NTM (11.5%), Pseudomonas aeruginosa (8.8%), Aspergillus (4.1%), Streptococcus (2.7%), Streptococcus constellatus (2.7%), Klebsiella pneumoniae (2.7%), anaerobic bacteria (2.0%), Acinetobacter baumannii (2.0%), Cryptococcus neoformans (1.4%), and Chlamydia psittaci (1.4%). In immunocompromised patients, frequent pathogens included P. jirovecii (20.0%), NTM (11.7%), Pseudomonas aeruginosa (10.0%), MTB (10.0%), Aspergillus (10.0%), coinfections (8.3%), anaerobic bacteria (8.3%), Escherichia coli (5.0%), Haemophilus influenzae (3.3%), Streptococcus constellatus (3.3%), Acinetobacter baumannii (1.7%), Cryptococcus neoformans (1.7%), Candida (1.7%), and Penicillium marneffei (1.7%).
Comparison of diagnostic performance in different specimen type
To assess potential differences in pathogen detection across sample types, we compared results from BALF, tissue, pleural effusion, and blood. mNGS exhibited higher positivity rates than traditional methods for all specimen types (Fig. 5A). mNGS sensitivity was highest in BALF samples (95.4%), followed by tissue (78.6%), blood (75%), and pleural effusion (75%). Culture sensitivity was also highest in BALF samples (49.4%) compared to pleural effusion (31.3%), blood (25%), and tissue (21.4%). However, statistical analysis revealed no significant differences in pathogen detection between the four sample types (Fig. 5B), indicating that the overall positivity rates of mNGS and traditional methods were not significantly influenced by sample origin.

(A) The sensitivity of mNGS and traditional methods to different sample types in LRTI cases were showed. The positive rate of mNGS of BALF, tissue, pleural effusion and blood specimens were higher than the traditional method (p < 0.05). (B) Bsut without statistical differences among the subtypes (p > 0.05) were showed.
Antibiotic Changes according to mNGS results
As shown in Table 1, 149 patients (91.3%) received antibiotic treatment during hospitalization before sample collection. Based on mNGS results, 119 patients (72.13%) had their anti-infective regimens modified (Table 2). This included de-escalation of antimicrobial agents in 54 patients (32.73%) and escalation in 65 patients (39.39%) (Table 2). Escalation of antibiotic treatment was primarily driven by the detection of specific pathogens by mNGS, such as Aspergillus, P. jirovecii, anaerobic bacteria, Orientia tsutsugamushi, Cryptococcus neoformans, or the identification of co-infections.
Discussion
Given the crucial role of etiology in the diagnosis and treatment of LRTIs, research has increasingly focused on improving microbiological diagnosis. Traditional approaches are often time-consuming, have low pathogen detection rates (below 40%), and involve complex steps16. mNGS offers a promising alternative by enabling broad detection of microorganisms, strain analysis, virulence assessment, resistance gene identification, and diagnosis of infections with unknown causes17. Leveraging short-read sequencing, mNGS rapidly analyzes microbial communities in patient samples, providing unbiased detection, faster turnaround times, and potential for semi-quantitative monitoring. Direct nucleic acid screening of respiratory specimens (sputum, BALF, lung tissue, pleural effusion) enables comprehensive analysis. Therefore, we compared traditional methods and mNGS for LRTI diagnosis by analyzing BALF, blood, tissue, and pleural fluid samples from 165 patients, focusing on detection efficiency and discrepancies.
A significant limitation of our study is that 91.3% of patients had received antimicrobial therapy prior to specimen collection. This factor may substantially bias the comparison between mNGS and traditional methods, particularly affecting culture-based diagnostics. Culture sensitivity is known to decline dramatically after antibiotic initiation, potentially creating an unfair advantage for mNGS, which can detect non-viable organisms and nucleic acid fragments. While this reflects real-world clinical scenarios where patients often receive empirical antibiotics before definitive diagnosis, it may overestimate the relative superiority of mNGS compared to traditional methods. Future studies should include larger cohorts of antibiotic-naive patients to provide more balanced comparisons.
mNGS demonstrated a significantly higher positivity rate (86.7%) than traditional methods (41.8%) (P < 0.05), consistent with prior studies18,19. Discrepancies between mNGS and traditional methods in these cases likely stemmed from mNGS’s superior sensitivity20, broader detection capability21,22, and ability to detect non-viable organisms 23,24. The clinical impact of metagenomics in infection diagnosis continues to expand, with mNGS showing particular advantages in complex cases where traditional methods fail22. Additionally, mNGS’s ability to detect antimicrobial resistance genes provides valuable information for treatment decisions21. The comprehensive nature of metagenomic approaches in clinical microbiology allows for identification of polymicrobial infections and biofilm-associated pathogens that may be missed by conventional methods23,25. While mNGS positivity was higher across all specimen types, the overall positivity rate was not significantly influenced by specimen type, contrasting with Duan et al.26, who hold the opposite view that the sensitivity of mNGS in specimen of blood, BALF and sputum samples. We acknowledge that the smaller sample sizes for blood and sputum specimens could have introduced bias into our results.
Fang27 and Xie19 covered it that mNGS could significantly increase the detecting of the mixed infection. In our mNGS-positive cases, more than one kind of pathogen was detected in 55.2% of patients. mNGS can directly identify various types of pathogens (bacteria, viruses, fungi, mycoplasma, chlamydia, leptospires, parasites, and unknown organisms) because it extracts all nucleic acids from the specimen. Although Streptococcus pneumoniae is typically the dominant pathogen in CAP28, our routine bacterial testing revealed a comparable incidence of NTM. This finding warrants careful interpretation, as it likely reflects the specialized nature of our tertiary referral center, which manages a disproportionate number of patients with chronic lung conditions, bronchiectasis, and other NTM-predisposing factors29. The high prevalence of NTM may not be representative of general LRTI populations and could introduce selection bias into our pathogen spectrum analysis. This finding underscores the advantage of mNGS in detecting multiple pathogens within a single sample, potentially enhancing the diagnosis of mixed infections relative to traditional methods.
The spectrum of pathogens varied significantly between immunocompetent and immunocompromised patients, providing important clinical insights. In immunocompetent patients, bacterial-bacterial co-infections were most common, while bacterial-fungal combinations predominated in immunocompromised patients. This differs from Wu30, who reported bacterial-viral and bacterial-bacterial co-infections as most frequent in immunocompetent patients. These differences may reflect variations in patient populations, geographic factors, and local epidemiology. The predominance of P. jirovecii (20.0%) in our immunocompromised cohort aligns with expected opportunistic infection patterns, while the high frequency of NTM in both groups suggests endemic presence in our region.
While mNGS offers enhanced detection, false positives remain a significant concern due to potential misidentification of contaminants or normal respiratory flora, such as Neisseria mucosa, Roxella roxella, Candida albicans, Malassezia globosa, Prevotella, Acinetobacter, Corynebacterium, HSV, and EBV, which were detected in our mNGS reports31. Given the lack of standardized criteria for distinguishing contamination from true infection, clinicians should carefully evaluate patient presentation, risk factors, and other data when mNGS identifies pathogens missed by traditional methods. Conversely, negative mNGS with positive traditional results should prompt investigation into potential mNGS limitations. To improve interpretation, Marsh32 suggest establishing bacterial load thresholds, and Zhou33 emphasize integrating mNGS with clinical and concurrent lab findings.
A critical limitation of our study is the exclusive focus on DNA sequencing, which precluded detection of important RNA viruses commonly associated with LRTI, including respiratory syncytial virus, influenza virus, rhinovirus, and coronaviruses. This technical limitation may have underestimated the true burden of viral infections in our cohort and reduced the comprehensive diagnostic value of mNGS. The single H1N1 case identified by traditional antigen testing but missed by mNGS exemplifies this limitation. Future studies should incorporate both DNA and RNA sequencing to provide complete pathogen detection coverage, though this would significantly increase costs.
Diagnosing LRTI etiology requires comprehensive clinical and laboratory assessment, and future guidelines are needed to refine mNGS data interpretation and differentiate contamination from true pathogens.
Our study demonstrated that mNGS offered superior detection of NTM, Prevotella, Streptococcus, and anaerobes compared to traditional methods. This is likely due to several factors. Isolating, culturing, and identifying NTM strains is time-consuming and often yields low positivity rates, hindering timely clinical diagnosis and treatment34, leading to infrequent NTM detection in our hospital using traditional methods. Prevotella, a black-pigmented anaerobic species and a component of the oral microbiome, is linked to oral diseases35 and is easily detected in patients with chronic pulmonary infections and compromised immunity. However, Prevotella identification via traditional methods requires culture isolation followed by identification using the rapid ID 32A system, a lengthy and costly process36. Anaerobic bacteria detection necessitates a strict anaerobic environment during sample collection and analysis, often leading to these organisms being missed by routine clinical microbiology laboratories.
For mycobacterial infections, mNGS can rapidly identify the Mycobacterium species, whereas conventional tests require more time. However, mNGS may sometimes miss Mycobacterium tuberculosis (MTB) or NTM. As Li14 noted, the detection of MTB and NTM can be lower with mNGS because MTB is an intracellular bacterium, making it difficult to detect its extracellular nucleic acids. Our results also showed that pathology confirmed 6 out of 20 MTB cases missed by mNGS, highlighting the value of combining mNGS with pathology or culture for MTB diagnosis. Other research8 also suggests integrating mNGS with culture or Xpert assays for tuberculosis diagnosis. Furthermore, mNGS was advantageous for detecting rare pathogens like O. tsutsugamushi, Chlamydia, and Legionella, which were only detected by mNGS in our study. mNGS also aids in Cryptococcus identification, which, in combination with culture and CrAg assays, significantly improves diagnostic accuracy and guides appropriate antifungal treatment selection37. In our research, we identified three cases of Pneumocystis jirovecii by both mNGS and traditional methods.
The consistency rate between traditional methods and mNGS for pathogen identification was only 32.3% in LRTI, with 20 cases (32.3%) showing inconsistencies. This included 5 missed cases of NTM, 4 of MTB, 2 of Enterococcus, 2 of Pseudomonas aeruginosa, and single cases of Staphylococcus hemolyticus, Paragonimus, H1N1, Haemophilus influenzae, anaerobic bacteria, Klebsiella, Myxococcus aureus, and Cryptococcus, all missed by either mNGS or traditional methods. The antigen test detected H1N1 and Paragonimus, and the Cryptococcal Antigen Latex Agglutination System detected Cryptococcus, which were missed by mNGS. Another possibility is that we may have considered normal flora as suspected pathogens when sequence reads were near the set threshold for mNGS in traditional-positive patients. Furthermore, incomplete disruption of the Mycobacterium cell wall during DNA extraction for mNGS might have resulted in missed MTB cases. Regardless of downstream molecular methods, effective sample pretreatment remains essential for pathogen recovery.
mNGS’s speed and accuracy in identifying infectious pathogens significantly reduces diagnostic turnaround time, providing valuable clinical guidance for subsequent diagnosis and treatment38. In our study, 72.13% of patients who were receiving antibiotics during hospitalization had their anti-infective regimens modified based on mNGS results. This high rate of treatment modification demonstrates the substantial clinical impact of mNGS on antimicrobial stewardship. The ability to de-escalate therapy in 32.73% of patients not only reduces unnecessary antibiotic exposure but also helps combat antimicrobial resistance—a critical global health concern. The escalation of therapy in 39.39% of patients, driven by detection of specific pathogens such as Aspergillus, P. jirovecii, or polymicrobial infections, highlights mNGS’s value in identifying complex infections requiring specialized treatment.
Despite the promising results, several barriers must be addressed before routine clinical implementation of mNGS. Cost remains a significant limitation, with mNGS testing typically costing 5–10 times more than traditional methods. The requirement for specialized bioinformatics expertise and infrastructure may limit accessibility in resource-constrained settings. Turnaround time, while faster than culture, still requires 24–48 h, which may not meet the needs for urgent clinical decisions. Additionally, the interpretation of results requires clinical expertise to distinguish pathogenic organisms from colonizers or contaminants, necessitating specialized training for clinicians.
Future research should focus on developing standardized interpretation guidelines, cost-effectiveness analyses, and identification of optimal patient populations for mNGS testing. Integration with rapid point-of-care diagnostics and development of simplified reporting systems could enhance clinical utility. Furthermore, studies incorporating both DNA and RNA sequencing, larger sample sizes stratified by antibiotic exposure, and long-term patient outcome data would strengthen the evidence base for mNGS implementation.
Moving forward, several strategies can be implemented in clinical practice to enhance LRTI diagnosis and address the limitations identified in this study. Firstly, supplementing DNA sequencing with RNA sequencing will broaden the scope of pathogen detection, particularly for RNA viruses. Secondly, expanding sample sizes, especially for blood, tissue, and pleural fluid specimens, will increase the statistical power and sensitivity of pathogen identification. Crucially, establishing standardized criteria for interpreting mNGS results is essential for differentiating between true infections and the presence of contaminants or colonizing organisms. Finally, validating positive mNGS findings with confirmatory testing methods, such as cultures, immunological assays, or PCR, will improve the accuracy and reliability of LRTI diagnoses.
Conclusions
In summary,our results indicate that mNGS offers significant advantages over traditional methods, demonstrating a more than twofold higher positivity rate (86.7% vs. 41.8%). Notably, mNGS exhibited superior sensitivity in detecting anaerobes, Aspergillus, Mycobacterium tuberculosis, and NTM. Furthermore, mNGS facilitated the detection of multiple pathogens within a single sample more readily. While mNGS displayed a higher overall positivity rate compared to traditional methods, its diagnostic performance was not significantly affected by sample type. Additionally, we observed distinct pathogen spectra in patients with varying immune statuses. Moreover, mNGS findings can inform and optimize antibiotic usage. Overall, mNGS has demonstrated significant value in pathogen detection and offers valuable implications for clinical practice. Future research should focus on identifying the optimal patient populations and sample types for mNGS, refining methods for distinguishing pathogenic from contaminating bacteria based on mNGS reports, and expanding the application of mNGS in drug resistance profiling and RNA virus detection.
Data availability
Date will be made available on reasonable request from corresponding author.
References
Corrêa, R. A. et al. Recommendations for severe community-acquired pneumonia treatment. J Bras Pneumol. 44(5), 405–423 (2018).
Olson, G. & Davis, A. M. Diagnosis and treatment of adults with community-acquired pneumonia. JAMA 323(9), 885–886. https://doi.org/10.1001/jama.2019.21118 (2020).
Zhu, Y. G., Tang, X. D., Lu, Y. T., Zhang, J. & Qu, J. M. Contemporary situation of community-acquired pneumonia in china: a systematic review. J Transl Int Med. 6(1), 26–31. https://doi.org/10.2478/jtim-2018-0006 (2018).
Wunderink, R. G. & Waterer, G. (2017) Advances in the causes and management of community acquired pneumonia in adults. BMJ 358, 2471. https://doi.org/10.1136/bmj.j2471 (2017).
Wilson, M. R. et al. Actionable diagnosis of neuroleptospirosis by next-generation sequencing. N Engl J Med. 370(25), 2408–2417. https://doi.org/10.1056/NEJMoa1401268 (2014).
Brown, J. R., Bharucha, T. & Breuer, J. Encephalitis diagnosis using metagenomics: application of next generation sequencing for undiagnosed cases. J Infect. 76(3), 225–240. https://doi.org/10.1016/j.jinf.2017.12.014 (2018).
Cai, Y. et al. Metagenomic next generation sequencing improves diagnosis of prosthetic joint infection by detecting the presence of bacteria in periprosthetic tissues. Int J Infect Dis. 96, 573–578. https://doi.org/10.1016/j.ijid.2020.05.125 (2020).
Chen, P., Sun, W. & He, Y. Comparison of metagenomic next-generation sequencing technology, culture and GeneXpert MTB/RIF assay in the diagnosis of tuberculosis. J Thorac Dis. 12(8), 4014–4024. https://doi.org/10.21037/jtd-20-1232 (2020).
Lansky, J. A., Litvin, J., Nadjm, B., Myint, K. S. Improving the diagnosis of pneumonia with host biomarkers and machine learning. The Lancet Digit. Health 3 (10), e611–e612. https://doi.org/10.1016/S2589-7500(21)00199-4
Liu, Y. et al. Effectiveness of metagenomic next-generation sequencing in the diagnosis of infectious diseases: a systematic review and meta-analysis. Int J Infect Dis. 142, 106996. https://doi.org/10.1016/j.ijid.2024.106996 (2024).
Miller, S. et al. Laboratory validation of a clinical metagenomic sequencing assay for pathogen detection in cerebrospinal fluid. Genome Res. 29(5), 831–842. https://doi.org/10.1101/gr.238170.118 (2019).
Graf, E. H. et al. comparative evaluation of the verigene respiratory pathogens nucleic acid test and conventional methods for the diagnosis of respiratory tract infections. J Clin Microbiol. 59(8), e0053121. https://doi.org/10.1128/JCM.00531-21 (2021).
Fu, Z. F. et al. Evaluations of clinical utilization of metagenomic next-generation sequencing in adults with fever of unknown origin. Front Cell Infect Microbiol. 11, 745156. https://doi.org/10.3389/fcimb.2021.745156 (2022).
Li, H. et al. Detection of pulmonary infectious pathogens from lung biopsy tissues by metagenomic next-generation sequencing. Front Cell Infect Microbiol. 8, 205. https://doi.org/10.3389/fcimb.2018.00205 (2018).
Li, H. & Durbin, R. Fast and accurate short read alignment with burrows-wheeler transform. Bioinformatics 25(14), 1754–1760. https://doi.org/10.1093/bioinformatics/btp324 (2009).
Zheng, Y., Qiu, X., Wang, T. & Zhang, J. The diagnostic value of metagenomic next-generation sequencing in lower respiratory tract infection. Front Cell Infect Microbiol. 11, 694756. https://doi.org/10.3389/fcimb.2021.694756 (2021).
Gu, W., Miller, S. & Chiu, C. Y. Clinical metagenomic next-generation sequencing for pathogen detection. Annu Rev Pathol. 14, 319–338. https://doi.org/10.1146/annurev-pathmechdis-012418-012751 (2019).
Huang, J. et al. Metagenomic next-generation sequencing versus traditional pathogen detection in the diagnosis of peripheral pulmonary infectious lesions. Infect Drug Resist. 13, 567–576. https://doi.org/10.2147/IDR.S235182 (2020).
Xie, G. et al. exploring the clinical utility of metagenomic next-generation sequencing in the diagnosis of pulmonary infection. Infect Dis Ther. 10(3), 1419–1435. https://doi.org/10.1007/s40121-021-00476-w (2021).
Diao, Z., Han, D., Zhang, R. & Li, J. Metagenomics next-generation sequencing tests take the stage in the diagnosis of lower respiratory tract infections. J Adv Res. 38, 201–212. https://doi.org/10.1016/j.jare.2021.09.012 (2021).
Guidicelli, G., Renvoise, A., Heyndrickx, L., Djossou, F. & Descamps, V. Next-generation sequencing in clinical bacteriology: a practical review for the detection of antimicrobial resistance genes. J Glob Antimicrob Resist. 30, 248–258. https://doi.org/10.1016/j.jgar.2022.07.006 (2022).
Hong, N. T. et al. The landscape of clinical metagenomics in infection diagnosis. J Clin Med. 10(16), 3565. https://doi.org/10.3390/jcm10163565 (2021).
Simner, P. J., Beo, T. H. & Patel, R. Metagenomics and its role in clinical microbiology. Clin Microbiol Rev. 31(2), e00059-e117. https://doi.org/10.1128/CMR.00059-17 (2018).
Naccache, S. N. & Chiu, C. Y. Metagenomics and other advanced diagnostic methods for infectious diseases. Cold Spring Harb Perspect Med. 9(8), a036764. https://doi.org/10.1101/cshperspect.a036764 (2019).
Peters, B. M., Jabra-Rizk, M. A., O’May, G. A., Conlan, J. V. & Harriott, M. M. Microbial interactions and community structures in polymicrobial biofilms. Microbiology 166(2), 85–103. https://doi.org/10.1099/mic.0.000877 (2020).
Duan, H. et al. The diagnostic value of metagenomic next⁃generation sequencing in infectious diseases. BMC Infect Dis. 21(1), 62. https://doi.org/10.1186/s12879-020-05746-5 (2021).
Fang, X. et al. Diagnostic value of metagenomic next-generation sequencing for the detection of pathogens in bronchoalveolar lavage fluid in ventilator-associated pneumonia patients. Front Microbiol. 11, 599756. https://doi.org/10.3389/fmicb.2020.599756 (2020).
Ruiz-Giardin, J. M. et al. Etiology of community-acquired pneumonia in adults: a systematic review and meta-analysis. J. Infect. 83(1), 1–12 (2021).
Loebinger, M. R. et al. risk factors for nontuberculous mycobacterial pulmonary disease: a systematic literature review and meta-analysis. Chest 164(5), 1115–1124. https://doi.org/10.1016/j.chest.2023.06.014 (2023).
Wu, X. et al. Etiology of severe community-acquired pneumonia in adults based on metagenomic next-generation sequencing: a prospective multicenter study. Infect Dis Ther. 9(4), 1003–1015. https://doi.org/10.1007/s40121-020-00353-y (2020).
Dickson, R. P., Erb-Downward, J. R., Martinez, F. J. & Huffnagle, G. B. The Microbiome and the respiratory tract. Annu Rev Physiol. 78, 481–504. https://doi.org/10.1146/annurev-physiol-021115-105238 (2016).
Marsh, R. L. et al. How low can we go? The implications of low bacterial load in respiratory microbiota studies. Pneumonia (Nathan). 10, 7. https://doi.org/10.1186/s41479-018-0051-8 (2018).
Zhou, H. et al. Clinical impact of metagenomic next-generation sequencing of bronchoalveolar lavage in the diagnosis and management of pneumonia: a multicenter prospective observational study. J Mol Diagn. 23(10), 1259–1268. https://doi.org/10.1016/j.jmoldx.2021.06.007 (2021).
Huang, M., Lin, Y., Chen, X. & Wu, D. The value of gene chip detection of bronchoalveolar lavage fluid in the diagnosis of nontuberculous mycobacterial lung disease. Ann Palliat Med. 10(6), 6438–6445. https://doi.org/10.21037/apm-21-1205 (2021).
Riggio, M. P. & Lennon, A. development of a novel pcr assay for detection of prevotella oris in clinical specimens. FEMS Microbiol Lett. 276(1), 123–128. https://doi.org/10.1111/j.1574-6968.2007.00926.x (2007).
Webb, K. et al. Porphyromonas pasteri and Prevotella nanceiensis in the sputum microbiota are associated with increased decline in lung function in individuals with cystic fibrosis. J Med Microbiol. 71(2), 001481. https://doi.org/10.1099/jmm.0.001481 (2022).
Xing, X. W. et al. Apparent performance of metagenomic next-generation sequencing in the diagnosis of cryptococcal meningitis: a descriptive study. J Med Microbiol. 68(8), 1204–1210. https://doi.org/10.1099/jmm.0.000994 (2019).
Tao, Y. et al. Diagnostic performance of metagenomic next-generation sequencing in pediatric patients: a retrospective study in a large children’s medical center. Clin Chem. 68(8), 1031–1041. https://doi.org/10.1093/clinchem/hvac067 (2022).
Acknowledgements
We would like to thank all the patients who donate their biological samples and thank to BGI for the help. Mingjun Dong was supported by the foundations and was responsible for designed the experiments and collecting the data and statistical analysis in our study.
Funding
The present study was supported in part by the grant from Guangxi Key Laboratory of Molecular Medicine in Liver Injury and Repair. (No. GXLIRMMKL-201916) and The Medical and Health Science and Technology Program of Zhejiang Province (2024KY294) .
Author information
Authors and Affiliations
Contributions
D.M.J, W.R, W.H, J.J.B, X.S.G designed the experiments. W.R and D.M.J collected data, analyzed and interpreted the data. W.H and W.R drafted the manuscript. X.S. G and J. JB revised the manuscript and put forward constructive suggestions. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The written informed consent from each patient and the approval of Ethics Committee of Ningbo Medical Center Lihuili Hospital. The study was conducted in accordance with the ethical standards of the institutional and national research committees and with the 1964 Helsinki Declaration and its later amendments.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, R., Wang, H., Jiang, J. et al. Diagnostic value of metagenomic next-generation sequencing in the etiological diagnosis of lower respiratory tract infection. Sci Rep 15, 39987 (2025). https://doi.org/10.1038/s41598-025-23695-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-23695-4
