
Abstract
Tinnitus is the perception of sounds without external stimuli, affecting 10%-15% of the general population and up to 25% of individuals over 70 years of age. While traditionally viewed as an auditory phenomenon, growing evidence highlights the role of the central nervous system in its pathophysiology. One of the proposed mechanisms, the “gating hypothesis” of tinnitus, suggests an alteration in the modulation of sensory activity by the frontostriatal network. Although structural changes in frontal areas support this idea, gray matter differences in subcortical regions—such as the auditory pathway and basal ganglia—remain poorly understood. Here, we examined subcortical structures and auditory function in older adults with mild presbycusis from the ANDES cohort, including 51 tinnitus patients and 40 age-matched controls. We analyzed brain volume via structural magnetic resonance imaging and subcortical auditory functionality via auditory brainstem responses (ABRs). We found non-significant differences in age, hearing loss, cognitive impairment, and ABR amplitudes between the groups. Notably, tinnitus patients presented a significant increase in the volume of basal ganglia structures (striatum and pallidum) but not in auditory areas. These findings reinforce the role of the basal ganglia in age-related tinnitus pathophysiology.
Similar content being viewed by others


Introduction
The perception of phantom sounds in the absence of external auditory stimuli, known as tinnitus, affects approximately 10% to 15% of the global population1,2,3. Tinnitus can manifest solely as a perceptual symptom with no other coexisting alterations, but for a subset of 1% to 3%, it becomes a distressing syndrome linked to emotional and cognitive alterations, such as anxiety, insomnia and depressive symptoms4,5. This difference has been identified as a key factor to consider in tinnitus research, highlighting the need to clearly define whether tinnitus corresponds to isolated tinnitus (sensory tinnitus) or to a tinnitus disorder with emotional and cognitive comorbidities6. Importantly, the differential pathophysiological mechanisms or neuroplasticity changes underlying these two tinnitus phenotypes (sensorial tinnitus vs. tinnitus disorder) are not well understood7. Elucidating the mechanisms of these two phenotypes of tinnitus can aid in the development of therapeutic strategies for alleviating the burden of tinnitus.
Several theoretical frameworks have been proposed to elucidate the neural mechanisms underlying tinnitus perception8,9,10. Nearly 50% to 80% of tinnitus patients have peripheral hearing loss due to inner ear damage, such as the loss of cochlear hair cells produced by acoustic trauma, ototoxicity, or age-related hearing loss11,12,13,14. The central gain hypothesis proposes that, owing to the diminished afferent activity in the cochlea and auditory nerve of individuals with hearing loss, there is an increase in neural activity within central auditory structures that could lead to tinnitus perception4,15,16. However, recent evidence suggests that the increased central gain activity in tinnitus patients may be more closely related to the presence of hyperacusis (intolerance to loud sounds) than to tinnitus itself10,17.
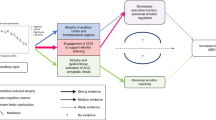
Another proposed mechanism in tinnitus involves an alteration in the top-down gating of auditory activity by frontostriatal and basal ganglia circuits18,19,20,21. In this sense, dysfunction in sensory gating could contribute to the persistence and distress associated with tinnitus21,22,23. Moreover, there are clinical reports showing that deep brain stimulation of the basal ganglia (caudate nucleus) can ameliorate tinnitus severity24; consequently, this subcortical structure has been proposed as a target for the neuromodulatory treatment of tinnitus25,26. However, the specific contribution of a basal ganglia gating mechanism in tinnitus in older adults is mostly unknown.
Aging and hearing loss are important factors to consider in older adults with tinnitus9,27,28,29. The incidence of tinnitus is known to increase with age and hearing loss30, affecting the quality of life in older adults30,31,32. In addition, hearing loss and aging are also associated with structural and functional brain changes33,34,35, making it difficult to determine structural brain changes that are specifically related to the presence of tinnitus in older adults36. In addition, although it is well established that aging and hearing loss are risk factors for cognitive decline and dementia37,38, whether tinnitus is associated with cognitive decline remains controversial39,40.
Importantly, a variety of functional and anatomical changes in different brain regions have been reported in MRI studies in tinnitus patients33,36,41,42,43,44. For example, previous studies have reported both volume reductions43 and increases42 in basal ganglia structures among tinnitus patients, making this a controversial issue. These differences could be explained by the clinical heterogeneity of tinnitus and its comorbidities, such as the presence/absence of hearing loss, the aging process or cognitive decline5,6. In this sense, it is important to study tinnitus characteristics and pathophysiological mechanisms in a specific group of older adults with tinnitus.
Here, we propose investigating structural and functional brain changes in subcortical nuclei in a subset of older adults with normal hearing to mild presbycusis who report tinnitus and do not use hearing aids. We hypothesize that the frontostriatal and basal ganglia networks play key roles in the pathophysiological mechanisms of the perception of sensory tinnitus in older adults. To test this hypothesis, we examined brain structural characteristics via MRI and auditory brainstem responses (ABRs) in the Chilean ANDES cohort of older adults45,46.
Results
A total of 91 older adults from the ANDES cohort were included (55 females), with an average age of 73.4 ± 5.1 years (ranging from 65 to 85 years), a mean hearing threshold of 30 ± 13.2 dB HL (PTA 0.5–4 kHz), and a mean education level of 9.5 ± 4.1 years. We identified 51 subjects who reported having tinnitus (T) and 40 subjects who were classified as non-tinnitus (NT). There were no significant differences in age or sex distribution between the tinnitus and non-tinnitus groups, whereas we detected a significant difference in educational level, which was lower in the tinnitus group (T: 8.7 ± 4.4 years of education; NT: 10.6 ± 3.6 years of education, Fig. 1a, p < 0.04). A summary of the demographic, audiological, cognitive, and emotional variables is presented in Table 1.
The presence of tinnitus disorder is usually accompanied by cognitive and emotional distress, whereas sensorial tinnitus is an isolated perceptual phenomenon. Using audiological, cognitive and mood surveys available in the ANDES cohort, we compared the tinnitus and non-tinnitus groups to determine the level of comorbidities in the tinnitus groups. We observed no significant differences in audiometric hearing levels, as measured by pure-tone average (PTA) (T: 30.8 \(\:\pm\:\) 13.8 dB HL; NT: 29.1\(\:\:\pm\:\:\)12.7 dB HL, p = 0.55), between the tinnitus and non-tinnitus groups. Similarly, analysis of the extended frequency range (0.125 Hz to 8 kHz) revealed no significant differences in hearing thresholds across all tested frequencies (Supplementary Figure S1). Additionally, Hearing Handicap Inventory for the Elderly–Screening (HHIE-S) scores, assessing the impact of hearing difficulties on quality of life, showed no significant differences between groups (T: 8.9 ± 9.1; NT:6.9 ± 7.5, p = 0.25) (Fig. 1b and c).

Educational level and audiological assessments. a) There were significant differences between groups in terms of years of education, being lower in tinnitus. b) The mean age and hearing levels of the tinnitus and non-tinnitus groups were similar. Significant correlations between PTA and age were found for both groups (T: Spearman rho = 0.48, p = 0.0003; NT: Spearman rho = 0.38, p = 0.013). c) The Hearing Handicap Inventory (HHIE-S) did not differ between the groups in terms of quality of life or emotional well-being with respect to hearing difficulties. d) Significant differences between groups were found in the loudness discomfort level (LDL), as the tinnitus group had a greater number of audiogram frequencies with detectable LDL, denoting a higher index for hyperacusis (T: 3.76 ± 4.1; NT: 1.92 ± 3.22, p = 0.02). * = statistically significant p < 0.05., ns = non-significant, p ≥ 0.05.
On the other hand, we found that the tinnitus group had a larger number of audiogram frequencies with detectable LDL than the non-tinnitus group did (T: 3.76 ± 4.1; NT: 1.92 ± 3.22, p = 0.02), indicating a greater presence of hyperacusis in the tinnitus group (Fig. 1d). The average LDL values for both groups across all tested frequencies are presented in Supplementary Figure S2.
There were no significant differences in the screening for cognitive decline, as evaluated by the MMSE score (T: 28.0 ± 1.33; NT: 28.1 ± 1.32, p = 0.75), or depressive symptoms, as assessed with the GDS (T: 3.5 ± 3.6; NT: 2.6 ± 2.4, p = 0.21) between the groups. Taken together, these results show that besides LDL and education, there were no significant differences in age, sex, hearing thresholds, MMSE scores or depressive symptoms between the groups with and without tinnitus in the ANDES cohort.

Functional evaluation of the central auditory pathway using suprathreshold ABR in the groups with and without tinnitus. a) The wave V/I ratio comparison revealed no difference between healthy controls and tinnitus patients. b) Non-significant difference in auditory-nerve (Wave I) amplitude. (c) Non-significant difference in wave V amplitude. ns = non-significant p ≥ 0.05.
We studied suprathreshold ABR responses to evaluate possible compensatory functional gains in the central auditory pathways of tinnitus patients16. We found non-significant differences in the amplitudes of wave I (t = 1.04, p = 0.3), wave V (t = 1.01, p = 0.31) and the V/I ratio (t = 1.46, p = 0.14) between the tinnitus and non-tinnitus groups (Fig. 2). Similarly, comparisons of ABR latencies for wave I (t = -0.07 ; p = 0.94) and wave V (t = 0.87; p = 0.38) yielded no significant differences between groups (Table 1). Next, we used volumetric MRI to evaluate possible structural changes in the central auditory pathway and in subcortical non-auditory brain structures of both groups. First, we calculated the volume of the nuclei of the central auditory pathway, including the cochlear nuclei, superior olivary complex, inferior colliculi, and the medial geniculate body and auditory cortex, by using an atlas of the human auditory pathway developed at 7-Tesla MRI47. There were no significant differences between the tinnitus and non-tinnitus groups in the intracranial volume (t = -0.75, p = 0.54), cochlear nuclei (t = -0.55, p = 0.94), superior olivary complex (t = 0.054, p = 0.94), inferior colliculi (t = -0.2, p = 0.94) and medial geniculate nucleus (t = 0.06, p = 0.94) or auditory cortex (t = -1.15, p = 0.94) (Fig. 3).

Volumetric MRI comparisons of the central auditory pathway in the groups with and without tinnitus. There were no significant differences between the groups in any of the structures measured. ns = non-significant p ≥ 0.05.

Basal ganglia volume comparisons. Volumetric comparisons of nonauditory subcortical structures revealed that tinnitus patients have larger pallidum (a), putamen (b), caudate (c), and nucleus accumbens (d) structures. *p < 0.05, **p < 0.01, ***p < 0.001.
Second, we evaluated structural changes in non-auditory brain subcortical structures, which are related to top-down gating mechanisms that could be altered in tinnitus patients15,23. To test this hypothesis, we calculated the gray matter volume of these subcortical nuclei and compared them between groups. We found that for basal ganglia structures, the tinnitus group had significantly larger volumes, (pallidum, t=-2.1, p = 0.03; Fig. 4a; putamen, t=-3.6, p = 0.0016; Fig. 4b; caudate, t=-2,8, p = 0.005; Fig. 4c; accumbens, t=-3.4, p = 0.0016; Fig. 4d). Figure 5 shows the anatomical reference for the striatum structures analyzed and their corresponding t values calculated for the comparisons between groups48.
We then calculated the striatum volume by summing the putamen, caudate, and accumbens volumes and found a significant difference in striatum volume between groups, even after controlling for the estimated total intracranial volume and age of the subjects (ANCOVA striatum, \(\:F\)=24.36, \(\:p\) value<0.001, \(\:\eta\:{p}^{2}\)=0.45).

Anatomical reference for the basal ganglia structures analyzed, along with their corresponding t-values calculated for the statistical comparisons.
To test frontal contributions to the top-down gating mechanism associated to tinnitus, we also examined key frontal cortical volumes involved in frontostriatal circuit between groups, including the anterior cingulate cortex (ACC) and dorsolateral prefrontal cortex (DLPFC) composites per hemisphere (covariates: age, eTIV). However, no group effects were significant across frontal ROIs (Left ACC p = 0.471, Right ACC p = 0.719, Left, DLPFC, p = 0.697, Right DLPFC, p = 0.316), suggesting that the effect is specific to striatal regions.
To explore the potential influence of the educational level on basal ganglia volumes, we conducted Pearson correlation analyses using years of education which has been proposed as a proxy for noise exposure50,51,52. No significant correlations were found between years of education and the volumes of basal ganglia structures (pallidum: r = – 0.09, p = 0.41; putamen: r = -0.16, p = 0.13; caudate: r = -0.10, p = 0.33; striatum: r = – 0.16, p = 0.13; accumbens: r = – 0.17, p = 0.10), indicating that education-related noise exposure is not associated with structural differences in these regions.
To assess whether brain volumes were associated with LDL presence within each group, we fitted separate ordinary least squares (OLS) regression models for the tinnitus and control groups. For the basal ganglia, the tinnitus group model showed no explanatory power (R2 = 0.051, p = 0.475) with no consistent significant associations after correction. In the control group, explanatory power was similarly low (R² = 0.086, p = 0.350) and no associations reached significance. Using composite volumes of the whole striatum yielded similar results (tinnitus group: R2 = 0.051; control group: R² = 0.086; no significant predictors). For the auditory pathway, the tinnitus group model had R² = 0.251 (p = 0.328) and the control group model had R2 = 0.196 (p = 0.794), with no individual ROI showing significant associations. Similar to the striatum, using a composite volume of the whole auditory pathway yielded consistent results (tinnitus group: R² = 0.082, p = 0.253; control group: R2= 0.004, p = 0.988). Thus, LDL presence is not associated with the striatal differences seen in tinnitus.
Afterwards, we conducted two robust linear regression models to examine whether the effect of tinnitus on basal ganglia volume was influenced by (i) age and (ii) hearing threshold (PTA). The interaction effect between tinnitus and age was statistically significant (β = 0.1451, p = 0.047), suggesting that the relationship between tinnitus and basal ganglia volume varies with age. However, the interaction effect between tinnitus and the PTA did not reach statistical significance (B = 0.0407, p = 0.186), indicating that the PTA does not strongly moderate this relationship (Fig. 6).

Interactions and effect of group (tinnitus vs. non-tinnitus) on striatum volume, with age (a) and PTA (b) as predictors. The striatum volume is the sum of the putamen, caudate, and accumbens volume structures.
Discussion
The present results show that older adults who reported having tinnitus in the past year have lower levels of education and a worse hyperacusis index (LDL) compared to age and hearing-matched non-tinnitus individuals. There were no significant differences in cognitive screening or depressive symptoms between the groups. Additionally, we found non-significant differences between groups in the structure and function of the central auditory pathway. However, we observed increased volumes in the basal ganglia structures, including the striatum and pallidum, of tinnitus patients. We propose that individuals with tinnitus in the ANDES cohort primarily experienced sensory tinnitus, as they did not actively complain about it but were instead asked about its presence during audiometric evaluations.
Tinnitus, far from being a single-stereotyped disorder, encompasses a wide array of maladaptive neural network configurations for sound processing9,28,49, ranging from sensorial or isolated tinnitus to tinnitus disorders with behavioral and emotional comorbidities6,28. In this study, we analyzed a specific group of tinnitus patients, which likely corresponded to sensorial tinnitus in older adults with normal to mild hearing loss and non-significant differences in age, hearing loss, cognition and depressive symptoms from non-tinnitus matched individuals. The educational level was worse in tinnitus patients, which could be explained by the reported greater exposure to acoustic injuries that can lead to tinnitus, such as acoustic trauma or ototoxicity, in less educated populations50,51. However, there was no correlation between years of education, used as a proxy for noise exposure, and basal ganglia volumes suggesting that noise exposure related to less education does not drive structural differences in our sample.
In this cohort, statistical comparisons revealed no significant differences in the degree of deafferentation (measured by pure-tone average, PTA; p = 0.55) or age (p > 0.05) between the tinnitus and non-tinnitus groups, indicating that neither factor was associated with the presence of tinnitus (Fig. 1b). Similarly, we did not find differences in electrophysiological (wave amplitudes and latencies in ABR) or morphological (size of key auditory nuclei in the brainstem) markers of central gain between the tinnitus and non-tinnitus groups. Our results are in agreement with reports showing a lack of compensatory central gain in tinnitus patients7,17.
Importantly, the tinnitus group did present significantly worse LDLs, potentially indicating a reduced dynamic range of the auditory system—a characteristic of hyperacusis, which several authors propose as a clinical marker of increased central gain7,10,17. Another explanation for the absence of central auditory gain increase in the tinnitus group of the ANDES cohort might be consequence of the slow progression of hearing loss and tinnitus in presbycusis patients. This slow progression may influence specific outcomes through better adaptation, such as the apparent lack of structural or electrophysiological markers of increased central gain in older adults with tinnitus.
In this specific cohort, the basal ganglia emerged as structures potentially linked to tinnitus. In recent decades, increasing evidence has shown that the basal ganglia play functional roles beyond movement control53. Basal ganglia circuits constitute highly conserved vertebrate structures receiving connections from diverse brain sources related to sensorimotor, visual, auditory, premotor, and emotional processing, among others54,55. Dysfunctions in the basal ganglia have been implicated in various conditions, including motor disorders (e.g., Parkinson’s disease, Huntington’s disease), psychotic disorders (e.g., schizophrenia), Tourette syndrome, obsessive‒compulsive disorder, and addictive behaviors56.
Research on the brain structure of tinnitus patients has reported contradictory results concerning structural changes in the basal ganglia, including decreases in volume43 and increases in volume42. In our case, we are in agreement with investigations reporting basal ganglia volume increases, which we propose for this specific subset of tinnitus individuals: that is, older adults with sensory tinnitus. In this sense, the results obtained in the group with tinnitus could be representative of beneficial neural adaptations to tinnitus in older adults without cognitive or depressive comorbidities.
The latter proposition can be supported by recent evidence obtained in patients treated with electroconvulsive therapy (ECT) for resistant depression. Brain MRI after ECT revealed gray matter volume increases in several regions, including the basal ganglia, suggesting that the increase in gray matter volume might be related to the clinical improvement of depressive symptoms57,58. Therefore, we propose that the increased volume changes that we found in the basal ganglia of the tinnitus group might have contributed to maintaining the phenotype of sensory tinnitus and preventing the emergence of tinnitus disorder syndrome.
The absence of significant group differences in frontal cortical volumes suggests that the volumetric alterations observed in our study are specific to the striatum. While both frontal and striatal structures participate in the frontostriatal gating hypothesis, their functional roles differ: frontal cortical areas are predominantly associated with top–down excitatory drive, whereas striatal regions also integrate inhibitory control via basal ganglia output pathways. These findings could support the hypothesis that the basal ganglia may play a specific role in the inhibition attempt to suppress tinnitus-related activity within auditory circuits rather than generating the tinnitus signal itself59. A speculative scenario could be that, in older adults with sensorial tinnitus, inappropriate signals generated in the auditory pathway are filtered by striatal circuits. This filtering interrupts a vicious cycle that might otherwise establish these changes as more permanent, preventing the emergence of tinnitus syndrome with cognitive and depressive comorbidities. However, the literature and our study (cross-sectional) do not allow for confirmation of a causal relationship between striatal function and top-down gating of tinnitus activity20,59.
Limitations
Among the limitations of this study, it is important to note that the primary methodology of the ANDES study did not focus specifically on tinnitus, nor did it include standard tinnitus intensity measures (e.g., tinnitus handicap inventory), which could provide insight into tinnitus severity and quality-of-life impacts. Future studies in this area would benefit from incorporating these parameters to explore potential correlations between basal ganglia volume and tinnitus severity in older adults.
Conclusion
In this specific group of older individuals with tinnitus, the only significant difference in brain structure between the tinnitus group and the non-tinnitus group was the volume enlargement of the basal ganglia nuclei. There were no significant differences in subcortical auditory volume, ABR response, cognition or depressive symptoms between the two groups. These results suggest that plastic changes in basal ganglia may be relevant for avoiding the cognitive and emotional comorbidities that constitute tinnitus syndrome. Future work could identify basal ganglia networks as potential targets for tinnitus mitigation.
Methods
Participants
Ninety-one older adults from the Auditory and Dementia Study (ANDES) cohort were recruited from Recoleta’s primary public health centers in Santiago de Chile. Importantly, these patients did not complain about tinnitus, as they were recruited from primary care adult health screening programs, representing a specific subset of “sensorial tinnitus” in older adults. The inclusion and exclusion criteria were as follows: (i) were over 65 years of age at the time of recruitment, (ii) had no history of neurological or psychiatric illness, (iii) had no cause of hearing loss other than presbycusis (e.g., conductive hearing loss), and (iv) did not use hearing aids. The Ethics Committee of the Clinical Hospital of the University of Chile approved all procedures (permission number OAIC752/15). The participants provided written informed consent in accordance with the Declaration of Helsinki.
Audiological assessment
Evaluations were carried out in the Department of Otolaryngology at the Clinical Hospital of the University of Chile. Audiometric hearing thresholds were evaluated from 0.125 to 8 kHz for each subject in both ears via a clinical audiometer (AC40, Interacoustics®). Conductive hearing loss was ruled out for each subject. The pure tone average (PTA) at 0.5, 1, 2, and 4 kHz was calculated for each subject in both ears.
Hyperacusis was estimated in dB (HL) using the loudness discomfort level (LDL) measured with an audiometer between 0.25 and 4 kHz. Owing to the frequent absence of LDL even at the maximum audiometer output (110 dB at 0.25 kHz and 115 dB between 0.5 and 4 kHz), group analyses for this variable focused on the detection or absence of a discomfort threshold at six frequencies (0.25, 0.5, 1, 2, 3 and 4 kHz) per ear, totaling twelve frequencies per subject. These analyses allowed us to use the whole sample of individuals, including those with no LDL, which have “0”, compared with subjects with LDL at all the evaluated frequencies, which yielded “12” summing both ears. Greater LDL values indicate more audiogram frequencies with hyperacusis.
Auditory brainstem response (ABR) waveforms were obtained by averaging with alternating clicks presented at suprathreshold levels (2000 repetitions, 80 dB nHL, bandpass 0.1–3 kHz, stimulus rate 21.1 Hz, EP25, Eclipse, Interacoustics®). The amplitudes of waves V and I were measured from peak to valley, and the latency times were calculated from the peaks of these waves. For the calculation of the V/I wave ratios, in situations where wave I was not detectable, the smallest amplitude value for wave I (0.02 µV) was utilized, as reported previously60.
Tinnitus
The audiologist of the ANDES cohort asked each participant during the audiometric evaluation about the presence or absence of tinnitus in the last year. The participants were divided into two categories: individuals experiencing tinnitus and those without tinnitus (non-tinnitus). The ANDES cohort does not include tinnitus intensity surveys.
Image acquisition
Imaging data collection was performed via a MAGNETOM Skyra 3 Tesla full-body MRI scanner (Siemens Healthcare GmbH, Erlangen, Germany), which employs a T1 MPRAGE sequence. We captured continuous images of the entire brain via specific parameters for a shorter acquisition time: time echo (TE) at 232 ms, time repetition (TR) at 2,300 ms, and a flip angle of 8 degrees, consisting of 26 slices, with a matrix size of 256 × 256 and a voxel dimension of 0.94 × 0.94 × 0.9 mm³. Additionally, T2-weighted turbo spin echo (TSE) imaging (4,500 TR ms, 92 TE ms) and fluid-attenuated inversion recovery (FLAIR) imaging (8,000 TR ms, 94 TE ms, 2,500 TI ms) were performed to evaluate structural irregularities. The total imaging process took approximately 30 min, resulting in 440 images per participant.
Image preprocessing and analysis
We employed two different morphometric approaches. First, we performed preprocessing with FreeSurfer, version 6, running under Centos 6. A single Linux workstation was used for the T1-weighted image analysis of individual subjects as suggested by previous research61. FreeSurfer processes cortical reconstruction62 through several steps: volume registration with the Talairach atlas, bias field correction, initial volumetric labeling, nonlinear alignment to the Talairach space, and final volume labeling. The automatic “recon-all” function produces representations of the cortical surfaces. It uses both intensity and continuity information from the entire three-dimensional MR volume in segmentation and deformation procedures. It creates gross brain volume extents for larger-scale regions (i.e., the total number of voxels per region): total gray and white matter, subcortical gray matter, brain mask volume, and estimated total intracranial volume (eTIV). The reliability between manual tracing and automatic volume measurements has been validated. The correspondence between manual tracings and automatically obtained segmentations was similar to the agreement between manual tracings63. All the volumes were visually inspected, and if needed, the volumes were edited by a trained researcher according to standard processes. With this approach, we calculated cortical and striatal volumes. Second, to analyze specific auditory pathway structures, we used a previously validated MNI mask47, which was created to filter central auditory pathway structures (Cochlear Nuclei, Superior Olivary Complex, Inferior Colliculi, and Medial Geniculate Nucleus). To use the mask, we preprocessed each T1-weighted image in SPM12 following the Voxel-Based Morphometry pipeline (VBM). Briefly, each T1-weighted image was tissue-segmented, followed by a study-specific DARTEL template where each image was iteratively aligned with DARTEL. To quantify the auditory regions of interest, only the resulting gray matter images were used.
Regions of interest
Regions of interest (ROIs) were selected a priori based on the hypothesis that tinnitus in older adults arises from altered frontostriatal gating of auditory information. In total, 11 bilateral ROIs were analyzed. Five ROIs corresponded to central auditory pathway structures—cochlear nuclei, superior olivary complex, inferior colliculi, medial geniculate body, and auditory cortex—quantified bilaterally using the 7T MRI atlas by Sitek et al. (2019)47 within the Voxel-Based Morphometry (VBM) pipeline. Two ROIs were cortical key structures to the frontostriatal circuit: anterior cingulate cortex and dorsolateral prefrontal cortex. The remaining four ROIs comprised basal ganglia structures—caudate, putamen, pallidum, and accumbens area—segmented bilaterally using FreeSurfer’s automated subcortical segmentation.
Clinical assessment
To obtain clinical information about general cognition, the presence of depression, hearing impairments, and general functionality, multiple scales were used. The subject’s general cognitive function was evaluated via the Mini-Mental State Examination (MMSE), a widely recognized and validated tool for assessing cognitive status64. Each participant self-assessed depression via the Geriatric Depression Scale (GDS)65. This test consists of 15 quick questions about various aspects of mental health and mood. Higher scores on the GDS indicate a greater likelihood of depression. The Hearing Handicap Inventory for the Elderly Screening (HHIE-S) was used as a self-assessment tool specifically designed to evaluate the impact of hearing loss on the quality of life of older adults66. It consists of 10 questions that focus on how hearing difficulties affect an individual’s daily life and emotional well-being. Higher scores indicate a greater impact of hearing loss on an individual’s life and well-being.
Statistical analysis
All the statistical analyses and graphs were generated via Python. Group differences between tinnitus controls and non-tinnitus controls were examined via independent-sample parametric and nonparametric tests for audiological, demographic, clinical and structural variables. Pearson correlation and Spearman rank correlation tests were used to evaluate relationships between variables such as pure tone average, age, years of education and structural volumes. Robust linear regression models were employed to investigate interactions between group, pure tone average, and age, assessing their combined effects on auditory and structural brain measures. Finally, analysis of covariance (ANCOVA) was used to control for confounders such as total intracranial volume and age in comparisons of gray matter volume across the auditory and striatal regions, which ensured that any observed group differences were independent of these covariates. To control for type I error inflation in ROI-based volumetric analyses, we applied False Discovery Rate (FDR) correction. Results are reported with group values or statistics, and all ROIs are FDR-corrected p-values, with a significance threshold set at p < 0.05.
Data availability
Data from this article are available from the corresponding author upon reasonable request.
Change history
20 January 2026
The original online version of this Article was revised: In the original version of this Article, the author Simón San-Martín was incorrectly indexed. The original Article has been corrected.
References
Bhatt, J. M., Bhattacharyya, N. & Lin, H. W. Relationships between tinnitus and the prevalence of anxiety and depression: tinnitus and mood disorders. Laryngoscope 127, 466–469 (2017).
Jarach, C. M. et al. Global prevalence and incidence of tinnitus: A systematic review and Meta-analysis. JAMA Neurol. 79, 888 (2022).
Shargorodsky, J., Curhan, G. C. & Farwell, W. R. Prevalence and characteristics of tinnitus among US adults. Am. J. Med. 123, 711–718 (2010).
Elgoyhen, A. B., Langguth, B., De Ridder, D. & Vanneste, S. Tinnitus: perspectives from human neuroimaging. Nat. Rev. Neurosci. 16, 632–642 (2015).
Langguth, B. et al. Different Types of Tinnitus, and Gender Aspects. in Textbook of Tinnitus (eds. Schlee, W. Springer International Publishing, Cham, 71–79 (2024). https://doi.org/10.1007/978-3-031-35647-6_7
De Ridder, D. et al. Tinnitus and tinnitus disorder: theoretical and operational definitions (an international multidisciplinary proposal). In: Progress in Brain Research vol. 260 1–25 (Elsevier, (2021).
Xie, J. et al. Neural mechanisms of tinnitus:an exploration from the perspective of varying severity levels. Brain Res. Bull. 111250 https://doi.org/10.1016/j.brainresbull.2025.111250 (2025).
Henton, A. & Tzounopoulos, T. What’s the buzz? The neuroscience and the treatment of tinnitus. Physiol. Rev. 101, 1609–1632 (2021).
Knipper, M. et al. The neural bases of tinnitus: lessons from deafness and cochlear implants. J. Neurosci. 40, 7190–7202 (2020).
Roberts, L. E., Salvi, R. & Overview Hearing loss, tinnitus, hyperacusis, and the role of central gain. Neuroscience 407, 1–7 (2019).
Haider, H. F. et al. Audiological biomarkers of tinnitus in an older Portuguese population. Front. Aging Neurosci. 14, 933117 (2022).
Khoza-Shangase, K. & Mkhize, S. P. Clinical and audiological characteristics in adults with tinnitus in South Africa. SAJCD 71, (2024).
Maihoub, S., Mavrogeni, P., Molnár, V. & Molnár, A. Tinnitus and its comorbidities: A comprehensive analysis of their relationships. JCM 14, 1285 (2025).
Xia, Q., Yang, S. & Ji, F. The characteristics of hearing loss in outpatients with tinnitus over the age of 60: an 11-year cross-sectional study. Acta Otolaryngol. 143, 753–758 (2023).
Rauschecker, J. P., Leaver, A. M. & Mühlau, M. Tuning out the noise: Limbic-Auditory interactions in tinnitus. Neuron 66, 819–826 (2010).
Schaette, R. & McAlpine, D. Tinnitus with a normal audiogram: physiological evidence for hidden hearing loss and computational model. J. Neurosci. 31, 13452–13457 (2011).
Hofmeier, B. et al. Functional biomarkers that distinguish between tinnitus with and without hyperacusis. Clin.Transl. Med. 11, (2021).
Chen, A. P. F. et al. Nigrostriatal dopamine pathway regulates auditory discrimination behavior. Nat. Commun. 13, 5942 (2022).
Hinkley, L. B. N. et al. Striatal networks for tinnitus treatment targeting. Hum. Brain. Mapp. 43, 633–646 (2022).
Rauschecker, J. P., May, E. S., Maudoux, A. & Ploner, M. Frontostriatal gating of tinnitus and chronic pain. Trends Cogn. Sci. 19, 567–578 (2015).
Wang, M. L. et al. Role of the caudate-putamen nucleus in sensory gating in induced tinnitus in rats. Neural. Regen Res. 16, 2250 (2021).
Hinkley, L. B., Mizuiri, D., Hong, O., Nagarajan, S. S. & Cheung, S. W. Increased striatal functional connectivity with auditory cortex in tinnitus. Front Hum. Neurosci. 9, (2015).
Leaver, A. M. et al. Dysregulation of limbic and auditory networks in tinnitus. Neuron 69, 33–43 (2011).
Cheung, S. W. & Larson, P. S. Tinnitus modulation by deep brain stimulation in locus of caudate neurons (area LC). Neuroscience 169, 1768–1778 (2010).
Basner, L. et al. Deep brain stimulation for primary refractory tinnitus: A systematic review. Brain Sci. 14, 452 (2024).
Cheung, S. W. et al. Phase I trial of caudate deep brain stimulation for treatment-resistant tinnitus. J. Neurosurg. 133, 992–1001 (2020).
De Ridder, D. et al. An integrative model of auditory Phantom perception: tinnitus as a unified percept of interacting separable subnetworks. Neurosci. Biobehav. Rev.. 44, 16–32 (2014).
Husain, F. T. & Khan, R. A. Review and perspective on brain bases of tinnitus. JAROhttps://doi.org/10.1007/s10162-023-00914-1 (2023).
Noreña, A. J. An integrative model of tinnitus based on a central gain controlling neural sensitivity. Neurosci. Biobehav. Rev.. 35, 1089–1109 (2011).
Reisinger, L. et al. Aging as risk factor for tinnitus and its complex interplay with hearing loss—evidence from online and NHANES data. BMC Med. 21, 283 (2023).
Malesci, R. et al. Tinnitus and neuropsychological dysfunction in the elderly: A systematic review on possible links. JCM 10, 1881 (2021).
Nondahl, D. M. et al. The impact of tinnitus on quality of life in older adults. J. Am. Acad. Audiol. 18, 257–266 (2007).
Husain, F. T. et al. Neuroanatomical changes due to hearing loss and chronic tinnitus: A combined VBM and DTI study. Brain Res. 1369, 74–88 (2011).
Husain, F. T. & Schmidt, S. A. Using resting state functional connectivity to unravel networks of tinnitus. Hear. Res. 307, 153–162 (2014).
Khan, R. A. et al. A large-scale diffusion imaging study of tinnitus and hearing loss. Sci. Rep. 11, 23395 (2021).
Yousef, A., Hinkley, L. B., Nagarajan, S. S. & Cheung, S. W. Neuroanatomic volume differences in tinnitus and hearing loss. Laryngoscope 131, 1863–1868 (2021).
Livingston, G. et al. Dementia prevention, intervention, and care: 2020 report of the lancet commission. Lancet 396, 413–446 (2020).
Livingston, G. et al. Dementia prevention, intervention, and care: 2024 report of the lancet standing commission. Lancet 404, 572–628 (2024).
Reisinger, L. & Weisz, N. Chronic tinnitus is associated with aging but not dementia. Hear. Res. 453, 109135 (2024).
Yang, D., Zhang, D., Zhang, X. & Li, X. Tinnitus-associated cognitive and psychological impairments: a comprehensive review meta-analysis. Front. Neurosci. 18, 1275560 (2024).
Boyen, K., Langers, D. R. M., de Kleine, E. & van Dijk, P. Gray matter in the brain: differences associated with tinnitus and hearing loss. Hear. Res. 295, 67–78 (2013).
Chen, X. et al. Depression, anxiety and brain volume after hearing loss and tinnitus: cohort study in the UK biobank. BJPsych open. 10, e37 (2024).
Cheng, S. et al. A multimodal Meta-Analysis of structural and functional changes in the brain of tinnitus. Front. Hum. Neurosci. 14, 28 (2020).
Yoo, H. B., De Ridder, D. & Vanneste, S. White matter changes in tinnitus: is it all age and hearing loss? Brain Connect. 6, 84–93 (2016).
Belkhiria, C. et al. Cingulate cortex atrophy is associated with hearing loss in presbycusis with cochlear amplifier dysfunction. Front. Aging Neurosci. 11, 97 (2019).
Medel, V. et al. Cochlear dysfunction as an early biomarker of cognitive decline in normal hearing and mild hearing loss. Alz Dem Diag Ass Dis. Mo. 16, e12467 (2024).
Sitek, K. R. et al. Mapping the human subcortical auditory system using histology, postmortem MRI and in vivo MRI at 7T. eLife 8, e48932 (2019).
Annie, G. Bryant. anniegbryant/subcortex_visualization: Initial Zenodo release. Zenodo https://doi.org/10.5281/ZENODO.15385315 (2025).
Knipper, M., Van Dijk, P., Nunes, I., Rüttiger, L. & Zimmermann U. Advances in the neurobiology of hearing disorders: recent developments regarding the basis of tinnitus and hyperacusis. Prog. Neurobiol. 111, 17–33 (2013).
Nondahl, D. et al. The use of hearing protection devices by older adults during recreational noise exposure. Noise Health. 8, 147 (2006).
Sanchez, V. A. et al. Comprehensive audiologic analyses after Cisplatin-Based chemotherapy. JAMA Oncol. 10, 912 (2024).
Prendergast, G. et al. Effects of age and noise exposure on proxy measures of cochlear synaptopathy. Trends Hear. 23, 2331216519877301 (2019).
Redgrave, P. et al. Goal-directed and habitual control in the basal ganglia: implications for parkinson’s disease. Nat. Rev. Neurosci. 11, 760–772 (2010).
Redgrave, P., Prescott, T. J. & Gurney, K. The basal ganglia: a vertebrate solution to the selection problem? Neuroscience 89, 1009–1023 (1999).
Tomioka, R. et al. The External Globus Pallidus as the Hub of the Auditory Cortico-Basal Ganglia Loop. eNeuro 11, (2024).
Howes, O. D. & Kapur, S. The dopamine hypothesis of schizophrenia: version III–The final common pathway. Schizophr. Bull. 35, 549–562 (2009).
Long, Z., Li, J. & Marino, M. Brain structural changes underlying clinical symptom improvement following fast-acting treatments in treatment resistant depression. J. Affect. Disord. 369, 52–60 (2025).
Ousdal, O. T. et al. The Neurobiological effects of electroconvulsive therapy studied through magnetic resonance: what have we Learned, and where do we go? Biol. Psychiatry. 91, 540–549 (2022).
Hullfish, J., Abenes, I., Yoo, H. B., De Ridder, D. & Vanneste, S. Frontostriatal network dysfunction as a domain-general mechanism underlying Phantom perception. Hum. Brain Mapp. 40, 2241–2251 (2019).
Delano, P. H. et al. Reduced suprathreshold auditory nerve responses are associated with slower processing speed and thinner Temporal and parietal cortex in presbycusis. PLoS ONE. 15, e0233224 (2020).
Gronenschild, E. H. B. M. et al. The effects of freesurfer version, workstation Type, and macintosh operating system version on anatomical volume and cortical thickness measurements. PLoS ONE. 7, e38234 (2012).
Fischl, B. & Dale, A. M. Measuring the thickness of the human cerebral cortex from magnetic resonance images. Proc. Natl. Acad. Sci. U.S.A. 97, 11050–11055 (2000).
Fischl, B. et al. Whole Brain Segmentation Neuron 33, 341–355 (2002).
Folstein, M. F., Folstein, S. E. & McHugh, P. R. Mini-mental state. J. Psychiatr. Res. 12, 189–198 (1975).
Yesavage, J. A. et al. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 17, 37–49 (1982).
Ventry, I. M. & Weinstein, B. E. The Hearing Handicap Inventory for the Elderly: a New Tool. Ear Hearing 3, 128–134 1. (1982).
Funding
This research work was supported by the National Agency for Research and Development of Chile (ANID), FONDECYT 1220607, FONDEF ID20I10371, FONDECYT 1221696, FONDEQUIP EQM210020, ANID - Basal Project AFB240002 to P. H. D, and Fundación Guillermo Puelma. Funding Scholarship ANID BECAS 2022-21221090 for San-Martín, S.
Author information
Authors and Affiliations
Contributions
C.D. and P.H.D. conceived the study design and oversaw cohort recruitment. S.S.M., V.M., H.B., C.D., and P.H.D. collected the experimental data and edited the manuscript. S.S.M., V.M., H.B., C.D., and P.H.D. conducted the statistical analyses and reported the results. S.S.M., V.M., H.B., C.D., and P.H.D. reviewed the manuscript. S.S.M., V.M., and P.H.D. Ensured that all the sections adhered to the journal guidelines.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
San-Martín, S., Medel, V., Breinbauer, H. et al. Increased basal ganglia volume in older adults with tinnitus. Sci Rep 15, 41303 (2025). https://doi.org/10.1038/s41598-025-25065-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-25065-6
