
Abstract
Obesity is a global health concern, and one potential contributing factor is addictive-like eating behavior. Despite growing interest, the prevalence of food addiction (FA) in large community samples in Iran, and the potential sex-specific correlates of FA, remain unexplored. This study aimed to assess the prevalence of FA in a non-clinical Iranian population and to compare its sociodemographic correlates between males and females. This cross-sectional study, conducted from 2021 to 2022, included valid data from 9,345 adults (82.1% female, 17.9% male). Participants completed the Persian version of the modified Yale Food Addiction Scale 2.0 (mPYFAS 2.0) and demographic surveys. Univariable and multivariable logistic regression analyses were performed to identify FA correlates. Overall, 15.6% of participants met the diagnostic threshold for FA (8.7% males, 17.2% females). Regarding FA severity, 4.0% exhibited mild FA (males: 2.9%; females: 4.3%), 4.1% displayed moderate FA (males: 2.0%; females: 4.6%), and 7.5% demonstrated severe FA (males: 3.8%; females: 8.3%). Multivariable analyses revealed that younger age, female sex, overweight/obesity, and lower education were associated with higher FA prevalence in the overall sample. Sex-specific analyses showed that age and weight status were significant correlates for females, while weight status and education level were significant for males. Notably, underweight status was positively correlated with FA for males but was negatively associated with FA for females. Regarding FA symptoms, females reported higher endorsement of most symptoms except for situation and problems and activities where no sex differences were found. This study highlights the significant prevalence of FA in Iran, emphasizing sex differences in prevalence, symptomatology, and associated sociodemographic factors. These findings provide valuable insights for designing tailored, sex-specific interventions to mitigate FA severity.
Similar content being viewed by others

Introduction
Obesity, as a critical public health concern, is one important risk factor and comorbidity of a wide range of health conditions, such as major depressive disorders, anxiety disorders, sleep disorders, cardiovascular diseases, kidney diseases, diabetes, neoplasms, cancers, all leading to an increased mortality risk compared to the overall population1,2,3,4,5,6,7,8. As estimated by the latest data, the global prevalence of obesity has increased from 8.8% (4.8%) in 1990 to 18.5% (14%) in 2022 in women and men9. With the increasing number of people with obesity, it is imperative to identity the potential risk factors to inform effective interventions. Food addiction (FA), as a promising risk factor, has attracted much attention during recent years both in the academia10,11,12,13,14,15,16,17 and by clinicians18.
As a phenotype which proposes that some people may develop addictive-like symptoms towards specific foods high in sugar and/or fat (especially ultra-processed foods19, such as chocolate and ice cream), FA may increase the food intake and contribute too overweight or obesity ultimately20,21. This is supported by the significant association found between FA and obesity in both children22, adolescents23 and adults24 in recent meta-analyses. Moreover, FA is closely related to the obesity-related constructs (such as impulsivity, reward sensitivity, loss of control, craving, cognitive dysfunction, mental distress, psychiatric comorbidities, social and occupational impairment)25,26,27,28,29,30,31,32, which further supports its vital role in the development of obesity. According to the latest meta-analysis, the pooled prevalence of FA is 15% among children and adolescents23, 14% for non-clinical adults33 and 40% in clinical samples, which is especially high in patients with eating disorders (bulimia nervosa (84%), binge eating disorder (63%) and anorexia nervosa (53%))34. Thus, the identification of associated factors of FA might hold great practical implications for the development of interventions to manage and decrease FA symptoms. Sex is a critical, though frequently neglected, candidate for the prevalence and the number of symptoms and the type of symptoms endorsed of FA.
Sex differences on FA
Sex is a vital dimension35, which calls for much more research attention in the field of addictive disorders36,37,38,39,40, and FA is no exception41. The sex differences of FA might be reflected on the prevalence, number of symptoms, specific symptoms endorsed and comorbidity and correlates.
As for the prevalence of FA, sex differences were repeatedly reported, with higher prevalence in female than male was found in meta-analysis of studies using the (Yale Food Addiction Scale (YFAS)42, while the latest meta-analysis of research employing YFAS 2.0 revealed that the prevalence of male (27%) is higher than that of female (24%)33. Meanwhile, no sex difference was also mentioned in several investigations43,44,45,46,47.
For the symptoms of FA, by using YFAS, no sex difference was revealed on the symptom score48 while sex differences were revealed for specific symptoms endorsed. Female students scored higher than male counterpart on “use despite knowledge of adverse consequences”, “persistent desire or repeated unsuccessful attempts to cut down”, “tolerance”, “withdrawal” and “clinically significant impairment” symptom whereas no sex difference was reported on “loss of control”, “much time spent to obtain, use, recover”, and “important activities given up” symptom49. Since four more symptoms were added into YFAS 2.0 when compared to YFAS, thus, it remains unknown whether there are any sex differences on these four symptoms.
For the comorbidity of FA, sex differences were frequently reported as well. The co-occurring FA and post-traumatic stress disorder (PTSD) was found to be higher for male (RR = 8.54) compared to female (RR = 4.32) after controlling for potential covariates in the community sample50, whereas this sex difference was absent in veterans51.
Relatively little attention was paid to the sex difference on the correlates of FA. The sex differences identified in this line of research demonstrated that sex-specific considerations were warranted when developing the interventions to alleviate the severity of FA. Chronotype (natural preferences of the body for wakefulness and sleep)52 was found to be a correlate of FA for males but not for females53. Specifically, being evening type might increase the risk of having a FA diagnosis only for men but not for women. Plasma dopamine levels was revealed to be negatively associated with food addiction in males, and positively in females54. For the adolescents seeking treatment for obesity, the sex differences about the attitudinal correlates of FA symptoms were revealed as well55. More specifically, functional impairment due to FA symptoms was associated with anxiety about gaining weight for the boys and social pressure about eating among the girls. Dieting was positively linked to avoidance from important social, functional and interpersonal activities due to eating among the boys, whereas it was correlated with continuing to eat despite knowing negative consequences among the girls. The association between social pressure about eating and eating for longer duration and higher amount than intended was only found for the girls but not for boys. Moreover, some sex-specific correlates of FA was also identified in previous research, such as polycystic ovarian syndrome for women56.
FA in Iran
The prevalence of FA in Iran ranged from 6.3% to 31% depending on the samples investigated47,57,58,59,60,61. The sex difference was only revealed in children and adolescent sample, with boys tending to be more likely to meet FA diagnosis than girls60. However, this sex difference was absent in Iranian adult samples47,57,58. Whether there are any potential sex differences on the comorbidity and correlates of FA, especially in Iran, remain largely unknown.
The current study
The previous studies conducted in Iran were limited by the small sample sizes (222 ~ 473 participants)47,57,58,59,60,61 and the specific research groups with health conditions (e.g., adults with obesity47,59), visitors of family physician clinics58 and individuals undergone laparoscopic sleeve gastrectomy57), which hinders from getting the prevalence of FA from the community level. In addition, the inclusion of single sex (such as only women were investigated in59) also unable to analyze the potential sex differences.
Thus, the current investigation aimed to determine the prevalence of in community level with large adult sample size in Iran and to explore whether there maybe potential sex-specific factors related to FA to help to develop more sex-appreciate interventions for FA in the future.
Methods
Design and participants
This cross-sectional study, conducted between 2021 and 2022, collected data from 9664 participants through an online questionnaire. The link of this online questionnaire was distributed by various social media, such as Twitter (X), Instagram, Facebook, and Telegram. Digital consent was obtained for each participant before formal questionnaires.
Measurements
The online questionnaire includes two parts. The first part is about participants’ basic demographic information which was designed mainly by referring previous literature62, such sex, age, and self-reported height and weight. Additionally, expanding previous studies, educational level, marital status, season of birth and the gambling participation las year (yes or no) were also collected to examine whether they were potential correlates of FA.
In adapting the scale to the Iranian cultural context, we also revised the examples of “Certain foods” that appear at the beginning of the YFAS 2.0. The original examples based on Western diets were replaced with culturally relevant food and beverage items commonly consumed in Iran. These included local equivalents of high-sugar, high-fat, and high-salt items to maintain the conceptual consistency of “highly palatable foods” while improving cultural sensitivity. Participants were instructed to reflect on any food or drink they personally struggled to control over the past year, in line with the scale’s conceptual framework.
In terms of psychometric properties, recent large-scale studies have confirmed the reliability and validity of both the Persian YFAS 2.0 and the 13-item modified version (mPYFAS 2.0). A study involving 9606 participants reported excellent model fit (CFI > 0.95, RMSEA < 0.03) and high internal consistency (α = 0.83, ordinal α = 0.93, CR = 0.86) 63. The full Persian YFAS 2.0 also showed strong construct validity and internal consistency in a separate non-clinical sample (KR-20 = 0.99, ω = 0.91) 64.
These procedures and findings support the use of the mPYFAS 2.0 as a valid and culturally appropriate measure for assessing food addiction in Iranian populations.
The second part is about the prevalence of FA, which was measured by Persian version of the modified Yale Food Addiction Scale 2.0 (mPYFAS 2.0). In the mPYFAS 2.0, 13 items are included to measure the status of FA according to the extrapolation of the DSM-5 criteria for substance use disorder to the consumption of highly palatable foods. The participants were asked to answer on a 8-point Likert scale ranging from “0” (Never) to “7” (Daily). The mPYFAS 2.0 showed satisfactory reliability and the sex invariance was also confirmed.
Statistical analysis
Data were carefully checked and cleaned before formal analysis. Data with missing responses, incomplete responses and careless responses were treated as invaid data and discarded. Descriptive results, such as frequency, percentage and mean, were calculated. Multicollinearity test was conducted to see if the current dataset was suitable for regression analysis. The results revealed that the VIF value of all variables was less than 2 (see the supplementary material), indicating that no multicollinearity was found among variables and the current dataset fulfilled the assumptions of regression analysis. Univariable logistic regression model was used to determine the associated variables of food addiction, which were employed to construct a multivariable logistic regression model to determine the correlates of food addiction after adjusting associated variables. The SPSS version 22 software (IBM Corporation, Armonk, NY, USA) was used for all the analysis.
The current investigation was conducted in accordance with the Declaration of Helsinki and the Ethical Guidelines for Medical and Health research established by ministry of Health and Medical Education and Ministry of Science, Research and Technology, Iran. The approval was obtained from the Ethics Review Committee of Shahroud Medical University Iran (Registration No. IR.SHMU.REC.1399.161). Some parts of the data were used for the psychometrics test of mPYFAS 2.0, which was published elsewhere.
Results
Participant characteristics
The data from 9664 participants was collected and data from 319 participants (3.3%) was discarded due to either incomplete responses or careless responses, which leading to 9345 valid datasets. The mean age of the 9345 participants included in the formal analysis was 29.67 ± 9.02 years, ranging from 18 to 73 years. The majority of the participants were female (82.10%). Nearly half participants (48.5%) belong to the normal weight category. And over half participants were single (53.9%) and got university degree (64.0%). Most respondents (96.1%) did not made any kind of online and offline bets or any kind of gambling during the last year (see Table 1).
Prevalence of food addiction
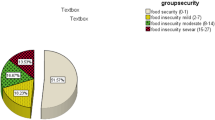
The diagnostic threshold for food addiction was met by 15.6% (95% CI [14.89%, 16.36%]) of participants (n = 1459), with 8.7% (95% CI [7.43%, 10.09%]) (n = 149) for male sample and 17.2% (95% CI [16.35%, 18.04%]) (n = 1310) for female sample. As for the food addiction severity, 4.0% (95% CI [3.62%, 4.42%]) met mild FA (male: 2.9% (95% CI [2.16%, 3.75%]); female: 4.3% (95% CI [3.83%, 4.74%])), 4.1% (95% CI [3.74%, 4.54%]) met moderate FA (male: 2.0% (95% CI [1.74%, 2.82%]); female: 4.6% (95% CI [4.14%, 5.08%])), and 7.5% (95% CI [6.97%, 8.04%]) met severe FA (male: 3.8% (95% CI [2.98%, 4.79%]); female: 8.3% (95% CI [7.73%, 8.97%])).
Symptoms of food addiction
The symptom score of female participants (1.58 ± 2.37) was significantly higher than that of male participants (1.16 ± 1.88), t = 7.79, Cohen’s d = 0.20. No sex difference was revealed on “important activities given up” symptom, and male participants endorsed more on “use in physically hazardous situations” and “continued use despite social or interpersonal problems” symptoms. Female participants endorsed more on the remaining symptoms and reported higher percentage to meet “clinical significant impairment” than male participants (see Table 2).
Correlates of food addiction
For the whole sample, the results of univariable logistic regression model showed that age, sex, weight status, education and marital status were associated with the FA diagnosis. However, only the associations with age, sex, BMI and education survived multivariable adjustment, while the association with marital status was rendered non-significant (see Table 3). Age (older than 30), being male, underweight/normal weight and high education level were negatively associated with FA.
To further explore the potential sex difference on correlates of FA, logistic regression was conducted for both females and males separately. For female sample, only age, weight status and marital status were identified as significant correlates of FA in univariable logistic regression model. After adjustment, age and weight status remained significant while marital status became insignificant (see Table 4). Age (22–25 years) and overweight and obesity were positively associated with FA for female participants.
For male sample, weight status, education and marital status were recognized as significant associates with FA in univariable logistic regression model while only weight status and education survived after adjustment in multivariable logistic regression model (see Table 5). Normal weight and high education level were negatively associated with FA for male participants.
Discussion
The present study represents the inaugural survey assessing the prevalence of food addiction and its associated demographic factors within a large non-clinical adult population of Iran. The sex differences were revealed on the prevalence, symptoms endorsed, and correlates of FA.
The prevalence of FA identified in the current study is 15.6%, which is exactly identical as Schulte and her colleagues’ finding during COVID-19 in USA64 and is also similar to the finding in Poland during COVID-19 (14.1%)65 and the latest meta-analysis data in non-clinical samples (14% around the world33 and 15% in in Latin America66). This prevalence is slightly lower than the prevalence (21%) of FA determined by a meta-analysis during COVID-1967, and much lower than the findings in Italy (46.9%)68 and Turkey (40.6%)69 while much higher than the prevalence in Bangladesh (7.5%)70. These inconsistencies might be due to several reasons. The YFAS version might be one of them. For example, Sultana et al.,70 used mYFAS, which might underestimate the prevalence of FA71. The sample characteristics might be another contributor. The current study recruited adult sample as Panno et al.,68 did, while Sultana et al.,70 and Kayaoğlu et al.,69 recruited only university students. However, even both employed university students as target sample69,70, noticeable difference of prevalence still was reported (40.6% vs. 7.5%). This is the same case for the current findings and Panno et al.68, which suggest that the prevalence of FA is heterogeneous across studies and some other variables might be more important than sample characteristics to lead to these discrepancies among previous studies, which warrant further investigations.
As for the sex difference on the prevalence of FA, we found that the prevalence of FA in Iran was more prevalent in women than men, which replicated previous findings42,62,72. More specifically, females got almost two-fold chance to get diagnosed as FA than males did (adjusted OR 2.94 (95%CI [2.43, 3.54]). The increased prevalence of FA in women as opposed to men may be associated with sex-related differences in hormonal profiles and/or dietary habits73,74.
Consistent with most previous findings24, individuals with overweight and obesity were susceptible to FA for both sex. Interestingly, the results for underweight represented opposite direction for females and males. Specifically, underweight was negatively associated with FA for females while positively associated with FA for males. These results suggested that the association between weight status and FA might be more complexed as previously assumed. In fact, Wiss75 summarized the previous studies about weight status and FA and found the heightened prevalence among the underweight population, which revealed a J-shaped relationship between BMI and FA prevalence43,76,77. We calculated the prevalence of FA for each status and found this J-shaped relationship was only revealed for male participants (see Table 6) but not female participants, which provides a more nuance insight about the linkage between weight status and FA prevalence and calls for special attention to underweight males.
Notably, sex-specific association with FA was identified in the current study, which extends previous studies53,54,55,56. More specifically, age range (22–25 years) was found to be positively associated with FA for females, while education level (≥ high school) was negatively associated with FA for males was reported. The interventions targeting FA are still on its infancy and much endeavor is warranted78,79,80, however, the sex-specific associations identified in both the current study and previous ones cannot be neglected when developing interventions in the future.
The findings of the current study indicate that individuals in the younger age group (< 30 years) are more susceptible to food addiction. Previous studies have also demonstrated that younger individuals tend to score higher on symptoms of FA compared to their older counterparts43,81. This result may be interpreted as a component of heightened vulnerability to addictive behaviors in younger individuals, possibly due to limitations in their risk assessment abilities and potential difficulties in controlling resistance to the consumption of high-fat/high-sugar foods. Additionally, lifestyle and dietary habits undergo more significant changes in younger individuals, potentially exposing them to a greater risk of emotionally driven eating and susceptibility to stress-related factors82.
Consistent with previous literature49, no sex difference was revealed on “important activities given up” symptom, females endorsed more on “use despite knowledge of adverse consequences”, “persistent desire or repeated unsuccessful attempts to cut down”, “tolerance”, “withdrawal” and “clinically significant impairment” symptoms than males. However, we found females also endorsed more on “loss of control” and “much time spent to obtain, use, recover” symptoms, which did not agree with Yu et al.49. Expanding Yu et al.49, we found males endorsed more on “use in physically hazardous situations” and “continued use despite social or interpersonal problems” symptoms than females and female endorsed more on “craving” and “impaired daily functioning (work, school, home)” symptoms than males.
This observed sex-specific symptom pattern where females more frequently reported withdrawal, craving, and clinically significant impairment may reflect underlying psychological and sociocultural mechanisms. Although these symptoms are part of the mYFAS 2.0 diagnostic structure based on DSM-5 criteria, their expression may be influenced by emotional vulnerability and gendered stress exposure. Prior studies suggest that women are more likely to experience internalizing symptoms such as anxiety and depression, which are linked to emotionally driven eating behaviors83. Sociocultural pressures related to caregiving, appearance, and dual work-family roles may further exacerbate this pattern, making females more prone to affectively charged food addiction symptoms84,85. In contrast, males may exhibit more externally oriented symptoms such as tolerance and increased time spent, reflecting reward-driven patterns83. These findings underscore the need for gender-sensitive interventions that address both the neurobehavioral and contextual stress factors contributing to food addiction.
The cultural context of food in Iran significantly shapes how food addiction symptoms are experienced, especially among women. Food is deeply embedded in social and familial roles often managed by women heightening its emotional significance and the distress linked to perceived loss of control85,86,87. At the same time, ideals of thinness and restraint, particularly in urban areas, often conflict with food-centric traditions, fostering guilt and shame around eating88. This tension is intensified by Iran’s nutrition transition, where ultra-processed foods increasingly coexist with traditional high-calorie dishes, creating mixed health messages86,89. Religious and moral values around moderation can further compound emotional eating and shame87. These culturally specific dynamics suggest that DSM-5-based food addiction symptoms may manifest differently across settings and call for more context-sensitive assessment and intervention strategies85.
Given the complex nature of food addiction, effective interventions must address both psychological factors and sociocultural influences. Evidence-based approaches such as impulse-control training, cognitive-behavioral therapy (CBT), and mindfulness techniques have shown promise in treating compulsive eating90,91. Our findings, which revealed higher symptom severity among women, highlight the need for gender-sensitive interventions focused on emotional regulation and shame resilience87,88,92. On a broader scale, public health strategies should address the food environment by regulating ultra-processed food marketing, promoting food literacy, and encouraging healthy traditional diets89. Community-based programs that reflect cultural values around caregiving, body image, and moral expectations are essential for reducing stigma and enhancing relevance85,87. Integrating clinical, cultural, and policy-level strategies offers a comprehensive framework for prevention and treatment aligned with the drivers identified in this study.
Limitations and future directions
This study has several limitations. First, the sample included a disproportionately high number of female participants (82.1%), which may limit the generalizability of the findings particularly the sex-stratified interpretations. Although this reflects broader trends in voluntary survey participation and food addiction studies, it remains a noteworthy limitation. Second, the use of self-report measures introduces the possibility of social desirability and recall biases, particularly for sensitive behavioral symptoms. Third, the cross-sectional design precludes causal inferences regarding the relationship between sex-specific variables and food addiction symptoms. Fourth, the 15.6% prevalence of food addiction observed in our study is comparable to the weighted average of 20% reported in a recent meta-analysis of 272 studies using the YFAS and mYFAS33, this suggests our estimate is within the expected global range for general population samples. However, given that the diagnosis was based on self-administered questionnaires, some overestimation cannot be ruled out. Future studies using structured clinical interviews are needed to validate these rates. Additionally, while recent events such as the COVID-19 pandemic may have influenced eating behaviors, our study did not collect relevant temporal data to examine this impact directly. Future longitudinal research could explore how such contextual factors affect food addiction symptoms over time. Lastly, because the study was conducted in an Iranian cultural setting, with its own food practices, gender roles, and religious or moral expectations surrounding eating, the findings may not be directly generalizable to other populations without cultural adaptation.
Future research should build on the current findings through longitudinal designs to better assess causal relationships between demographic and psychosocial variables and food addiction outcomes. For instance, the associations we observed between younger age, lower educational attainment, and food addiction cannot be interpreted causally due to the cross-sectional design. Incorporating structured diagnostic interviews alongside self-report tools could help improve the precision of prevalence estimates and symptom interpretation. Further investigation into unmeasured psychosocial variables such as mental health conditions, perceived stress, caregiving demands, or employment instability may provide a more comprehensive risk profile.
Given the observed sex-specific symptom patterns, future studies should also explore mechanisms underlying these differences using mixed methods and neurodevelopmental models. The “brain mosaic” framework suggests that symptom expression may result from a combination of biologically and socially influenced traits, regardless of assigned sex84. Exploring this heterogeneity, including underreported symptomatology in males, may improve the gender inclusivity of both diagnostic tools and treatment approaches. Finally, research should continue adapting and evaluating culturally responsive intervention models within Iranian and similar sociocultural settings ideally combining emotion-focused, community-based, and gender-informed components with public health strategies targeting food environments and cultural eating norms.
Conclusion
The prevalence of FA in Iran is 15.6%, with 8.7% for males and 17.2% for females. Weight status, and marital status are significant correlated with FA for both females and males, while sex-specific correlates of FA were also identified (younger age for females whereas lower education for males). Underweight is positively associated with FA for males while negatively associated with FA for females. Sex-specific considerations need to be taken into account when developing interventions of FA in the future.
Data availability
The datasets analyzed during the current study are available from the corresponding author upon reasonable request.
References
Chen, Y., Ma, L., Han, Z. & Xiong, P. The global burden of disease attributable to high body mass index in 204 countries and territories: Findings from 1990 to 2019 and predictions to 2035. Diabetes, Obes. Metab. https://doi.org/10.1111/dom.15748 (2024).
Tan, D. J. H. et al. Rising global burden of cancer attributable to high BMI from 2010 to 2019. Metabolism 152, 155744. https://doi.org/10.1016/j.metabol.2023.155744 (2024).
Steptoe, A. & Frank, P. Obesity and psychological distress. Phil. Trans. R. Soc. B: Biol. Sci. 378, 20220225. https://doi.org/10.1098/rstb.2022.0225 (2023).
Lopez-Jimenez, F. et al. Obesity and cardiovascular disease: mechanistic insights and management strategies. A joint position paper by the World Heart Federation and World Obesity Federation. European J. Prev. Cardiol. 29, 2218–2237 (2022).
Wiebe, N., Lloyd, A., Crumley, E. T. & Tonelli, M. Associations between body mass index and all-cause mortality: A systematic review and meta-analysis. Obes. Rev. 24, e13588. https://doi.org/10.1111/obr.13588 (2023).
Dong, Z. et al. Association of overweight and obesity with obstructive sleep apnoea: A systematic review and meta-analysis. Obes. Med. 17, 100185. https://doi.org/10.1016/j.obmed.2020.100185 (2020).
Chan, W. S., Levsen, M. P. & McCrae, C. S. A meta-analysis of associations between obesity and insomnia diagnosis and symptoms. Sleep Med. Rev. 40, 170–182. https://doi.org/10.1016/j.smrv.2017.12.004 (2018).
Lingvay, I., Cohen, R. V., Roux, C. W. I. & Sumithran, P. Obesity in adults. Lancet https://doi.org/10.1016/S0140-6736(24)01210-8 (2024).
Phelps, N. H. et al. Worldwide trends in underweight and obesity from 1990 to 2022: A pooled analysis of 3663 population-representative studies with 222 million children, adolescents, and adults. Lancet 403, 1027–1050. https://doi.org/10.1016/S0140-6736(23)02750-2 (2024).
Gearhardt, A. N. et al. Social, clinical, and policy implications of ultra-processed food addiction. BMJ 383, e075354. https://doi.org/10.1136/bmj-2023-075354 (2023).
Constant, A., Moirand, R., Thibault, R. & Val-Laillet, D. Meeting of minds around food addiction: Insights from addiction medicine, nutrition, psychology, and neurosciences. Nutrients 12, 3564. https://doi.org/10.3390/nu12113564 (2020).
Gearhardt, A. N. & Schulte, E. M. Is food addictive? a review of the science. Annu. Rev. Nutr. 41, 387–410. https://doi.org/10.1146/annurev-nutr-110420-111710 (2021).
LaFata, E. M. & Gearhardt, A. N. Ultra-Processed food addiction: An epidemic?. Psychother. Psychosom. 91, 363–372. https://doi.org/10.1159/000527322 (2022).
LaFata, E. M., Allison, K. C., Audrain-McGovern, J. & Forman, E. M. Ultra-Processed food addiction: A research update. Curr. Obes. Rep. 13, 214–223. https://doi.org/10.1007/s13679-024-00569-w (2024).
Schiestl, E. T., Rios, J. M., Parnarouskis, L., Cummings, J. R. & Gearhardt, A. N. A narrative review of highly processed food addiction across the lifespan. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 106, 110152. https://doi.org/10.1016/j.pnpbp.2020.110152 (2021).
Senol, E. & Mohammad, H. Current perspectives on brain circuits involved in food addiction-like behaviors. J. Neural Transm. 131, 475–485. https://doi.org/10.1007/s00702-023-02732-4 (2024).
Krupa, H., Gearhardt, A. N., Lewandowski, A. & Avena, N. M. Food addiction. Brain Sci. 14, 952. https://doi.org/10.3390/brainsci14100952 (2024).
Burrows, T. et al. Health professionals’ and health professional trainees’ views on addictive eating behaviours: A cross-sectional survey. Nutrients 12, https://doi.org/10.3390/nu12092860. 2860 (2020).
Ubbink, J. & Levine, A. S. From processed foods to ultraprocessed foods: Evolution of an industry model and impact on dietary quality, health, and society. Annu. Rev. Food Sci. Technol. https://doi.org/10.1146/annurev-food-111523-122028 (2024).
Tobore, T. O. Towards a comprehensive theory of obesity and a healthy diet: The causal role of oxidative stress in food addiction and obesity. Behav. Brain Res. 384, 112560. https://doi.org/10.1016/j.bbr.2020.112560 (2020).
Fazzino, T. L. The reinforcing natures of hyper-palatable foods: Behavioral evidence for their reinforcing properties and the role of the US food industry in promoting their availability. Curr. Addict. Rep. 9, 298–306. https://doi.org/10.1007/s40429-022-00417-8 (2022).
Bektaş, M., Demir, D., Demir, Ş & Bektaş, İ. The effect of food addiction in children on obesity: A systematic review and meta-analysis study. J. Pediatr. Res. 8, 414–423 https://doi.org/10.4274/jpr.galenos.2021.29963. (2021).
Yekaninejad, M. S. et al. Prevalence of food addiction in children and adolescents: A systematic review and meta-analysis. Obes. Rev. 22, e13183. https://doi.org/10.1111/obr.13183 (2021).
Bao, K., French, E. N., Schleyer, B., Khaikin, S. & Chen, E. Y. Food addiction is associated with greater objective binge eating and eating disorder psychopathology, and higher body mass index in youth, a meta-analysis. Psychiatry Res. Commun. 2, 100067. https://doi.org/10.1016/j.psycom.2022.100067 (2022).
Maxwell, A. L., Gardiner, E. & Loxton, N. J. Investigating the relationship between reward sensitivity, impulsivity, and food addiction: A systematic review. Eur. Eat. Disord. Rev. 28, 368–384. https://doi.org/10.1002/erv.2732 (2020).
Santiago, V. A. & Cassin, S. E. Social and occupational impairment among individuals with ultra-processed food addiction. Curr. Addict. Rep. 9, 307–317. https://doi.org/10.1007/s40429-022-00416-9 (2022).
Whatnall, M., Skinner, J. A., Leary, M. & Burrows, T. L. Food addiction: a deep dive into ‘loss of control’ and ‘craving’. Curr. Addict. Rep. 9, 318–325. https://doi.org/10.1007/s40429-022-00431-w (2022).
Iceta, S. et al. Cognitive function in binge eating disorder and food addiction: A systematic review and three-level meta-analysis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 111, 110400. https://doi.org/10.1016/j.pnpbp.2021.110400 (2021).
Piccinni, A. et al. Food addiction and psychiatric comorbidities: a review of current evidence. Eating Weight Disorders – Stud. Anorexia, Bulimia Obes. 26, 1049–1056. https://doi.org/10.1007/s40519-020-01021-3 (2021).
Wiss, D. A. & LaFata, E. M. Ultra-Processed foods and mental health: where do eating disorders fit into the puzzle?. Nutrients 16, https://doi.org/10.3390/nu16121955. 1955 (2024).
Skinner, J., Jebeile, H. & Burrows, T. Food addiction and mental health in adolescents: A systematic review. Lancet Child Adolescent Health 5, 751–766. https://doi.org/10.1016/S2352-4642(21)00126-7 (2021).
Burrows, T., Kay-Lambkin, F., Pursey, K., Skinner, J. & Dayas, C. Food addiction and associations with mental health symptoms: A systematic review with meta-analysis. J. Hum. Nutr. Diet. 31, 544–572. https://doi.org/10.1111/jhn.12532 (2018).
Praxedes, D. R. S. et al. Prevalence of food addiction determined by the yale food addiction scale and associated factors: A systematic review with meta-analysis. Eur. Eat. Disord. Rev. 30, 85–95. https://doi.org/10.1002/erv.2878 (2022).
Praxedes, D. R. S. et al. Correction to ‘Prevalence of food addiction determined by the yale food addiction Scale and associated factors: A systematic review with meta-analysis’. Eur. Eat. Disord. Rev. 32, 610–611. https://doi.org/10.1002/erv.3078 (2024).
Mauvais-Jarvis, F. et al. Sex and gender: Modifiers of health, disease, and medicine. Lancet 396, 565–582. https://doi.org/10.1016/S0140-6736(20)31561-0 (2020).
Davis, C. A. & Bonder, R. in Food and Addiction: A Comprehensive Handbook (eds A.N. Gearhardt, K.D. Brownell, M.S. Gold, & M.N. Potenza) 28–36 (Oxford University Press, 2024).
McKee, S. A. & McRae-Clark, A. L. Consideration of sex and gender differences in addiction medication response. Biol. Sex Differ. 13, 34. https://doi.org/10.1186/s13293-022-00441-3 (2022).
Zakiniaeiz, Y. & Potenza, M. N. Gender-related differences in addiction: A review of human studies. Curr. Opin. Behav. Sci. 23, 171–175. https://doi.org/10.1016/j.cobeha.2018.08.004 (2018).
Becker, J. B., McClellan, M. L. & Reed, B. G. Sex differences, gender and addiction. J. Neurosci. Res. 95, 136–147. https://doi.org/10.1002/jnr.23963 (2017).
Sanchis-Segura, C. & Becker, J. B. Why we should consider sex (and study sex differences) in addiction research. Addict. Biol. 21, 995–1006. https://doi.org/10.1111/adb.12382 (2016).
Römer, S. S., Bliokas, V., Teo, J. T. & Thomas, S. J. Food addiction, hormones and blood biomarkers in humans: A systematic literature review. Appetite 183, 106475. https://doi.org/10.1016/j.appet.2023.106475 (2023).
Pursey, K. M., Stanwell, P., Gearhardt, A. N., Collins, C. E. & Burrows, T. L. The prevalence of food addiction as assessed by the yale food addiction scale: a systematic review. Nutrients 6, https://doi.org/10.3390/nu6104552. 4552–4590 (2014).
Hauck, C., Weiß, A., Schulte, E. M., Meule, A. & Ellrott, T. Prevalence of ‘food addiction’ as measured with the yale food addiction scale 2.0 in a representative German sample and its association with sex, age and weight categories. Obes. Facts 10, 12–24. https://doi.org/10.1159/000456013 (2017).
Schankweiler, P., Raddatz, D., Ellrott, T. & Hauck Cirkel, C. Correlates of food addiction and eating behaviours in patients with morbid obesity. Obes. Facts 16, https://doi.org/10.1159/000531528. 465–474 (2023).
Lacroix, E. & von Ranson, K. M. Body image disturbance partially explains eating-related psychosocial impairment in food addiction. Eat. Behav. 41, 101512. https://doi.org/10.1016/j.eatbeh.2021.101512 (2021).
Piccinni, A., Marazziti, D., Cargioli, C., Mauri, M. & Stallone, T. Food addiction: Is it a nosological category or a psychopathological dimension? Preliminary results of an Italian study. Hormone Mol. Biol. Clin. Invest. 36, 20180021. https://doi.org/10.1515/hmbci-2018-0021 (2018).
Yousefi, R. et al. Food addiction and binge eating disorder in relation to dietary patterns and anthropometric measurements: A descriptive-analytic cross-sectional study in iranian adults with obesity. Behav. Med. 50, 37–46. https://doi.org/10.1080/08964289.2022.2092442 (2024).
Bonder, R. et al. Grazing and food addiction: Associations between varied patterns of overconsumption and addictive-like eating. Appetite https://doi.org/10.1016/j.appet.2024.107768 (2024).
Yu, Z. et al. Sex differences in disordered eating and food addiction among college students. Appetite 129, 12–18. https://doi.org/10.1016/j.appet.2018.06.028 (2018).
Hoover, L. V., Yu, H. P., Duval, E. R. & Gearhardt, A. N. Investigating gender differences in the co-occurrence of PTSD and food addiction. Appetite 187, 106605. https://doi.org/10.1016/j.appet.2023.106605 (2023).
Stojek, M. M. et al. Investigating sex differences in rates and correlates of food addiction status in women and men with PTSD. Nutrients 13, 1840. https://doi.org/10.3390/nu13061840 (2021).
Roenneberg, T. Having trouble typing? What on earth is chronotype?. J. Biol. Rhythms 30, https://doi.org/10.1177/0748730415603835. 487–491 (2015).
Amicis, R. D. et al. Sex differences in the relationship between chronotype and eating behaviour: A focus on binge eating and food addiction. Nutrients 15, https://doi.org/10.3390/nu15214580. 4580 (2023).
Mills, J. G., Thomas, S. J., Larkin, T. A. & Deng, C. Overeating and food addiction in Major Depressive Disorder: Links to peripheral dopamine. Appetite 148, 104586. https://doi.org/10.1016/j.appet.2020.104586 (2020).
Taş Torun, Y., İçen, S., Gül, H. & Döğer, E. A cross-sectional study on the correlates of food addiction symptoms in adolescents seeking treatment for obesity: Eating attitudes and gender differences. J. Addict. Dis. 40, 326–335. https://doi.org/10.1080/10550887.2021.1990638 (2022).
Derrigo, K. & LaFata, E. M. Examining the proportions of food addiction among women with and without polycystic ovarian syndrome who do and do not take hormonal birth control. Eat. Behav. 51, 101824. https://doi.org/10.1016/j.eatbeh.2023.101824 (2023).
Mousavi, M. et al. Food addiction disorder 2 years after sleeve gastrectomy; association with physical activity, body composition, and weight loss outcomes. Obes. Surg. 31, 3444–3452. https://doi.org/10.1007/s11695-021-05420-y (2021).
Haghighinejad, H. et al. Persian version of the yale food addiction scale 2.0: psychometric analysis and setting cutoff point for the food cravings questionnaire-trait-reduced. Psych. Invest. 18, 179–186. https://doi.org/10.30773/pi.2020.0198 (2021).
Moghaddam, S. A. P. et al. The prevalence of food addiction and its associations with plasma oxytocin level and anthropometric and dietary measurements in Iranian women with obesity. Peptides 122, 170151. https://doi.org/10.1016/j.peptides.2019.170151 (2019).
Naghashpour, M., Rouhandeh, R., Karbalaipour, M. & Miryan, M. Prevalence of food addiction among Iranian children and adolescents: Associations with sociodemographic and anthropometric indices. Med. J. Islam Repub. Iran 32, https://doi.org/10.14196/mjiri.32.8. 8 (2018).
Niroumand Sarvandani, M. et al. Validation and psychological properties of the Persian version of DSM 5 Yale food addiction Scale 2.0 (PYFAS 2.0) in non-clinical population. Addict. Health 14, https://doi.org/10.34172/ahj.2022.1283. 175 (2022).
Meule, A. & Gearhardt, A. N. Ten years of the yale food addiction scale: A review of version 2.0. Curr. Addict. Rep. 6, 218–228. https://doi.org/10.1007/s40429-019-00261-3 (2019).
Niroumand Sarvandani, M. et al. Confirmatory factor analysis and gender invariance of Persian version of the modified Yale food addiction scale (mPYFAS) 20: Insight from a large scale Iranian sample. J. Eating Disord. 12, https://doi.org/10.1186/s40337-023-00962-1. 14 (2024).
Schulte, E. M., Kral, T. V. E. & Allison, K. C. A cross-sectional examination of reported changes to weight, eating, and activity behaviors during the COVID-19 pandemic among United States adults with food addiction. Appetite 168, 105740. https://doi.org/10.1016/j.appet.2021.105740 (2022).
Zielińska, M., Łuszczki, E., Bartosiewicz, A., Wyszyńska, J. & Dereń, K. The prevalence of ‘“Food Addiction”’during the COVID-19 pandemic measured using the Yale Food Addiction Scale 20 (YFAS 20) among the adult population of Poland. Nutrients 13, https://doi.org/10.3390/nu13114115. 4115 (2021).
de Melo Barros, L. et al. Prevalence of food addiction determined by the Yale Food Addiction Scale in Latin America: A systematic review with meta-analysis. Int. J. Eat. Disord. 56, 677–690. https://doi.org/10.1002/eat.23909 (2023).
Alimoradi, Z., Lotfi, A., Lin, C.-Y., Griffiths, M. D. & Pakpour, A. H. Estimation of behavioral addiction prevalence during COVID-19 pandemic: A systematic review and meta-analysis. Curr. Addict. Rep. 9, 486–517. https://doi.org/10.1007/s40429-022-00435-6 (2022).
Panno, A., Carbone, G. A., Massullo, C., Farina, B. & Imperatori, C. COVID-19 related distress is associated with alcohol problems, social media and food addiction symptoms: Insights from the italian experience during the lockdown. Front. Psych. 11, 577135. https://doi.org/10.3389/fpsyt.2020.577135 (2020).
Kayaoğlu, K., Göküstün, K. K. & Ay, E. Evaluation of the relationship between food addiction and depression, anxiety, and stress in university students: A cross-sectional survey. J. Child Adolesc. Psychiatr. Nurs. 36, 256–262. https://doi.org/10.1111/jcap.12428 (2023).
Sultana, M. S. et al. Food addiction, orthorexia nervosa and dietary diversity among Bangladeshi university students: A large online survey during the COVID-19 pandemic. J. Eat. Disord. 10, 163. https://doi.org/10.1186/s40337-022-00680-0 (2022).
Silva Júnior, A. E. et al. Commentary on “Food addiction, orthorexia nervosa and dietary diversity among Bangladeshi university students: A large online survey during the COVID-19 pandemic”. J. Eat. Disord. 11, 78. https://doi.org/10.1186/s40337-023-00812-0 (2023).
Penzenstadler, L., Soares, C., Karila, L. & Khazaal, Y. Systematic review of food addiction as measured with the Yale Food Addiction Scale: Implications for the food addiction construct. Curr. Neuropharmacol. 17, https://doi.org/10.2174/1570159X16666181108093520. 526–538 (2019).
Lovejoy, J., Sainsbury, A. & Group, S. C. W. Sex differences in obesity and the regulation of energy homeostasis. Obes. Rev. 10, https://doi.org/10.1111/j.1467-789X.2008.00529.x. 154–167 (2009).
Marino, M. et al. Nutrition and human health from a sex–gender perspective. Mol. Aspects Med. 32, https://doi.org/10.1016/j.mam.2011.02.001. 1–70 (2011).
Wiss, D. Clinical considerations of ultra-processed food addiction across weight classes: An eating disorder treatment and care perspective. Curr. Addict. Rep. 9, 255–267. https://doi.org/10.1007/s40429-022-00411-0 (2022).
Meule, A. Food addiction and body-mass-index: A non-linear relationship. Med. Hypotheses 79, 508–511. https://doi.org/10.1016/j.mehy.2012.07.005 (2012).
Schulte, E. M. & Gearhardt, A. N. Associations of food addiction in a sample recruited to be nationally representative of the united states. Eur. Eat. Disord. Rev. 26, 112–119. https://doi.org/10.1002/erv.2575 (2018).
Reche-García, C. et al. Bariatric-Metabolic surgery is the most effective intervention in reducing food addiction symptoms: A systematic review and meta-analysis. Obes. Surg. https://doi.org/10.1007/s11695-024-07107-6 (2024).
O’Hea, E. L. et al. The food addiction clinical treatment (FACT) manual: A harm reduction treatment approach. Behav. Sci. 14, 557 (2024).
Leary, M., Pursey, K. M., Verdejo-Garcia, A. & Burrows, T. L. Current intervention treatments for food addiction: A systematic review. Behav. Sci. 11, 80 (2021).
Schulte, E. M. & Gearhardt, A. N. Development of the modified yale food addiction scale version 2.0. Eur. Eat. Disord. Rev. 25, 302–308. https://doi.org/10.1002/erv.2515 (2017).
Musharbash, R. M., Elsahoryi, N. A., McGrattan, A., Al-Alam, S. & Badawi, L. Prevalence of food addiction during COVID-19 pandemic in Amman, Jordan: A cross sectional study. J. Nutr. Food Proc. 4, 1–7 (2021).
Valente, S. et al. Sex-specific issues in eating disorders: A clinical and psychopathological investigation. Eat. Weight Disord.-Stud. Anorexia, Bulimia Obes. 22, 707–715 (2017).
Breton, É., Juster, R.-P. & Booij, L. Gender and sex in eating disorders: A narrative review of the current state of knowledge, research gaps, and recommendations. Brain Behav. 13, e2871. https://doi.org/10.1002/brb3.2871 (2023).
Lawson, J. L., Wiedemann, A. A., Carr, M. M. & Kerrigan, S. G. Considering food addiction through a cultural lens. Curr. Addict. Rep. 7, 387–394. https://doi.org/10.1007/s40429-020-00315-x (2020).
Haghighian Roudsari, A., Ajami, M., Davoodi, H. & Mohammadi-Nasrabadi, F. A Review of Evidence-Informed Policy Making in Sustainable Healthy Food and Nutrition Systems. J. Mazandaran Univ. Med. Sci. 29, 152–164 (2019).
Ebrahimi, E., Mardani-Hamooleh, M., Khezeli, M., Avatef-Fazeli, M. & Habibi-Asgarabad, M. Traces of social culture in the lived experiences of emotional eating among Iranian obese women. BMC Public Health 24, 1982. https://doi.org/10.1186/s12889-024-19501-x (2024).
Shoraka, H., Amirkafi, A. & Garrusi, B. Review of body image and some of contributing factors in Iranian population. Int. J. Prev. Med. 10, 19 (2019).
Amerzadeh, M., Takian, A., Pouraram, H., Sari, A. A. & Ostovar, A. Policy analysis of socio-cultural determinants of salt, sugar and fat consumption in Iran. BMC Nutr. 8, 26. https://doi.org/10.1186/s40795-022-00518-7 (2022).
Adams, R. C., Sedgmond, J., Maizey, L., Chambers, C. D. & Lawrence, N. S. Food addiction: Implications for the diagnosis and treatment of overeating. Nutrients 11, 2086 (2019).
Vasiliu, O. Current status of evidence for a new diagnosis: Food addiction-a literature review. Front. Psych. 12, 824936. https://doi.org/10.3389/fpsyt.2021.824936 (2022).
Gearhardt, A. N., Corbin, W. R. & Brownell, K. D. Development of the yale food addiction scale version 2.0. Psychol. Addict. Behav. 30, 113–121. https://doi.org/10.1037/adb0000136 (2016).
Acknowledgements
We would like to thank all the participants who made this study possible. We also extend our sincere gratitude to Shahroud University of Medical Sciences for their support of this project and to the university’s Ethics Review Committee for their valuable guidance and oversight.
Author information
Authors and Affiliations
Contributions
M.N.S. and M.A. contributed to the conceptualization and design of the study. M.N.S. was responsible for data acquisition. Data analysis and interpretation were conducted by Q.W.C., M.A., and M.N.S. The initial draft of the manuscript was prepared by M.N.S. and Q.W.C. M.N.S., Q.W.C., M.A., P.B., E.M.L., and T.L.B. reviewed and substantively revised the manuscript. Q.W.C. created the figures and visualizations. M.N.S. coordinated the project.
Corresponding author
Ethics declarations
Competing interests
Authors declare that they have no competing interests.
Ethics approval
The current study was conducted in accordance with the Declaration of Helsinki and the Ethical Guidelines for Medical and Health research established by ministry of Health and Medical Education and Ministry of Science, Research and Technology, Iran. We obtained the approval by the Ethics Review Committee of Shahroud Medical University Iran (Registration No. IR.SHMU. REC.1399.161).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Sarvandani, M.N., Chen, QW., Asadi, M. et al. Prevalence of food addiction and sex-specific correlates in a large sample of Iranian adults. Sci Rep 15, 41885 (2025). https://doi.org/10.1038/s41598-025-26203-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-26203-w
