
Abstract
In the population of patients with hepatitis B virus (HBV)-associated hepatocellular carcinoma (HCC) experiencing postoperative recurrence and undergoing subsequent transarterial chemoembolization (TACE), a comprehensive model for outcome prediction and risk stratification remains lacking. Between 2016 and 2021, a total of 189 eligible patients from two centers were allocated into training, internal validation, and external validation cohorts. Key factors such as extrahepatic metastasis, prior anti HBV treatment status, Child-Pugh classification, and pre-TACE systemic immune-inflammation response index (SIRI) score were utilized to construct a nomogram via multivariate Cox regression analyses and supported by scientific rationale. The nomogram’s predictive performance and discriminative capability were evaluated and compared with the Barcelona Clinic Liver Cancer (BCLC) recurrence staging system. The nomogram consistently demonstrated superior performance over the BCLC system across the training (C-index: 0.76 vs. 0.66), internal validation (C-index: 0.76 vs. 0.76), and external validation datasets (C index: 0.73 vs. 0.65). Furthermore, the nomogram effectively stratified patients into low-, medium-, and high-risk categories, each characterized by distinct median post-recurrence survival (PRS) times: 51.2 months (95% CI: 27.7, 60.2), 18.6 months (95% CI: 13.9, 35.0), and 6.0 months (95% CI: 3.8, 8.0), respectively. The nomogram can be used to stratify the risk of HBV-associated HCC that recurs after curative resection and experiences further TACE and predicts individual survival with reliable performance and discrimination.
Similar content being viewed by others
Introduction
Globally, liver cancer ranks as the sixth most common cancer and the third leading cause of cancer-related mortality1. In China, primary liver cancer is the fourth most prevalent cancer and the second leading cause of cancer-related deaths2. Liver cancer is projected to affect over 1 million individuals worldwide by 20253. Hepatocellular carcinoma (HCC) is the predominant type of liver cancer, representing approximately 90% of cases3. In China, about 80% of liver cancer cases are attributed to infections with hepatitis B virus (HBV) or hepatitis C virus (HCV), in contrast to Western countries where alcohol consumption and metabolic dysfunction-associated steatotic liver disease (MASLD) are more prevalent causes4. Currently, liver transplantation is considered the optimal treatment for tumors unsuitable for local resection. However, the global shortage of liver donors and insufficient funding continue to constrain the advancement of liver transplantation. Hepatic resection is the primary curative intervention for patients with HCC. Nevertheless, the substantial recurrence rate of 60% to 70% within five years post-surgery remains a significant impediment to long-term survival5,6,7. For patients experiencing recurrence following curative resection, the principal therapeutic strategies include tyrosine kinase inhibitors (TKIs), thermal ablation, and transarterial chemoembolization (TACE), with a minority undergoing reoperation. Recent advancements in therapeutic approaches are highlighted by the introduction of immune checkpoint inhibitors (ICIs), such as PD-1/L1 and anti-CTLA-4 inhibitors8,9,10. In several regions of China, TACE and TKIs continue to be the predominant treatments for patients with recurrent HCC. Nomograms were used to evaluate survival and recurrence following surgery11,12; however, these tools do not account for post-recurrence survival (PRS), as they are constructed using variables limited to primary tumor characteristics and initial resection. Wang and colleagues13 previously developed a nomogram for predicting survival following TACE; however, their study lacked a comprehensive analysis of survival outcomes specifically within the HBV-associated HCC subgroup and did not account for recurrent HCC. This omission may have resulted in the exclusion of other significant prognostic factors, such as alpha-fetoprotein (AFP). Consequently, there is a clinical imperative to establish a specialized prognostic model to predict survival outcomes after TACE in patients with HBV-associated HCC who experience recurrence following curative resection, particularly in regions with high HBV prevalence. In this study, we created a web-based calculator (https://idoctorzlyy.shinyapps.io/DynNomapp/) and a prognostic nomogram model for these patients.
Patients and methods
Patients
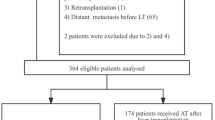
Clinical records were collected from patients with HBV-associated HCC who experienced recurrence post-curative resection and underwent TACE between October 2016 and October 2021 at the Second Affiliated Hospital of Chongqing Medical University and Yunnan Cancer Hospital. The inclusion criteria for the study were as follows: (1) pathological confirmation of HCC post-curative surgery with imaging-confirmed recurrence; (2) presence of at least one detectable liver recurrence lesion; (3) history or current infection with HBV; (4) Eastern Cooperative Oncology Group performance status score of ≤ 1; and (5) Child-Pugh classification of A or B. Patients were excluded from the study if they had other malignant conditions, had received treatment prior to TACE and after recurrence, or if they lacked sufficient clinical information. A total of 354 patients were screened, of whom 189 met the eligibility criteria and were subsequently enrolled in the study. From the Chongqing cohort, 122 patients were randomly allocated in a 3:1 ratio to either the training cohort (n = 91) or the internal validation cohort (n = 31). Additionally, 67 patients from the Yunnan cohort were assigned to the external validation cohort. Figure 1 provides an overview of the study population. TACE was selected as the treatment modality for patients at Barcelona Clinic Liver Cancer (BCLC) stage A who were either unsuitable for reoperation or opted against it. These patients presented with large tumor volumes and small standard residual liver volumes.

Flow chart of study design. HBV, hepatitis B virus; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; ICIs, immune checkpoint inhibitors; TACE, transarterial chemoembolization; TKIs, tyrosine kinase inhibitors.
We reviewed the Practice Guideline of TACE for HCC in China and Korea14,15. We included patients who adhered to the guideline-recommended TACE procedures and endpoints, as verified through operative records and imaging data, while excluding those who underwent hepatic arterial infusion chemotherapy (HAIC).
TACE procedures: A Rosch Hepatic catheter is cannulated into the celiac trunk using percutaneous Seldinger technique for catheterization through the femoral artery. For conventional TACE (c-TACE), the iodized oil and aqueous solution and chemotherapeutic drugs should be mixed, forming a “water in oil” emulsion to improve the stability of the solution. The volume ratio of iodized oil to aqueous solution is usually 2:1. For drug-eluting beads TACE (DEB-TACE), Pirarubicin is usually loaded on microspheres. The iodinated oil or microspheres are slowly embolized through a microcatheter into the tumor artery, followed by embolization with larger diameter particles to bring the blood supply to a “stasis” or “near-stasis” state, i.e. contrast agents are slowly flushed out within 2–5 heartbeats. Angiography is performed 5 min after blood stasis. If tumor staining is still observed, further chemoembolization should be considered to achieve stasis or near-stasis.
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and received ethical approval from the ethics committee of the Second Affiliated Hospital of Chongqing Medical University, which included a waiver of informed consent. (No. 2019-60).
Data collection
The clinical data encompasses gender, age, ECOG PS score, serum AFP concentration, HBV immunology and DNA levels, prior anti-HBV therapy, total bilirubin, albumin, major vascular invasion, extrahepatic metastasis, BCLC recurrence staging, Child-Pugh classification, tumor size and count, times of TACE procedures, additional adjuvant therapies post-TACE, targeted therapy, immunotherapy, high intensity focused ultrasound, percutaneous ethanol injection, radiation, radiofrequency ablation, etc. Data on neutrophil, lymphocyte, monocyte, and platelet counts within the 3 days before and after the each TACE, along with calculating neutrophil-lymphocyte ratio (NLR), platelet-lymphocyte ratio (PLR), monocyte-lymphocyte ratio (MLR), and systemic inflammatory response index (SIRI = neutrophil count * monocyte count / lymphocyte count) of the first TACE were collected16.
Follow-up
Patients were monitored until either their death or October 1, 2024. During the first two years following discharge, each patient participated in outpatient follow-up appointments, which included CT or MRI scans and serum tumor marker assessments every three months, transitioning to biannual evaluations thereafter. The date of recurrence was identified as the date on which the initial positive imaging test was obtained. PRS was defined as the duration of survival following the detection of the initial cancer recurrence.
Statistical analysis
Continuous variables were presented as medians with interquartile ranges (IQRs), and differences between multiple groups were analyzed using Kruskal-Wallis H test. Binary and ordinal categorical variables were expressed as case counts with corresponding percentages. Differences among multiple groups were analyzed using the chi-square test or Fisher’s exact test for binary variables, and the Kruskal-Wallis test for ordinal variables. Determine the optimal cut point for continuous variables (NLR, MLR, PLR, and SIRI) using the maximum selected rank statistics from the R package “maxstat”17. Kaplan-Meier survival curves were generated and analyzed using the log-rank test. Significant variables identified through univariate Cox regression and log-rank tests were incorporated into a multivariate Cox regression model to ascertain risk factors affecting the prognosis of HBV-associated HCC following TACE. The prognostic nomogram was developed based on previously identified predictors, existing scientific evidence, and clinical relevance. The model’s performance was assessed using the Harrell’s concordance index (C-index), which serves as a measure of calibration analogous to the area under the receiver operating characteristic curve. Calibration curves were generated using 1,000 bootstrap samples. Discrimination was evaluated using Kaplan-Meier survival curves of tertile predictions and Decision Curve Analysis (DCA)18,19,20. Each patient’s prognostic score was calculated from the nomogram, and the optimal cut-off value for patient categorization was determined using X-tile version 3.6.121. The performance and discrimination were compared with the Barcelona recurrence staging system. Calculations were conducted using Stata/SE 15.0 (Stata Corp, College Station, TX) and R software (version 4.4.1; www.r-project.org), utilizing the ‘rms’ package for nomogram construction, and the ‘survminer’ and ‘survival’ packages for survival analyses. A two-tailed P-value less than 0.05 was deemed statistically significant.
Results
Patient characteristics
Table 1 details the clinical and pathological characteristics of patients in both the training and validation cohorts, revealing no significant differences between the baseline data of the three cohorts. The median PRS time for the overall cohort was 14 months, with 1-, 2-, 3-, and 5-year PRS rates of 55.6%, 39.2%, 26.7%, and 12.3%, respectively. The median PRS times were 16.1 months for the training cohort, 14 months for the internal validation cohort, and 14.3 months for the external validation cohort. PRS rates at 1, 2, 3, and 5 years were 54.8%, 39.6%, 28.8%, and 14.4% for the training cohort; 61.3%, 38.7%, 21.3%, and 14.2% for the internal validation cohort; and 52.2%, 38.8%, 25.6%, and 6.5% for the external validation cohort. After TACE, 183 patients (96.8%) received TKIs, 9 of 70 with severe vascular invasion were eligible for radiotherapy, 12 (6.3%) received ICIs, and 2 (1.1%) received ICIs plus TKIs.
Prognostic factors in the training cohort
We performed log-rank tests and univariate Cox regression on 27 factors in the training cohort, detailed in Supplementary Table S1 online. Statistically significant factors like AFP, major vascular invasion, extrahepatic metastasis, BCLC recurrence staging, Child-Pugh classification, TACE times, pre-TACE NLR, pre-TACE MLR, pre-TACE PLR, pre-TACE SIRI score, and post-TACE NLR. Figure 2 presents these results, showing TACE times, extrahepatic metastasis, and Child-Pugh classification as survival risk factors after TACE for recurrent HBV-associated HCC.

Multivariate analysis and forest plot of the hazard ratio of PRS in the training cohort. BCLC, Barcelona Clinic Liver Cancer; HBV, hepatitis B virus; MLR, monocyte-lymphocyte ratio; NLR, neutrophil-lymphocyte ratio; PLR, platelet-lymphocyte ratio; PRS, post-recurrence survival; SIRI, systemic inflammatory response index; TACE, transarterial chemoembolization.
The study focused on patients with HBV-associated HCC, highlighting the impact of “prior anti-HBV therapy” on survival and the SIRI value’s reflection of the tumor’s immune-inflammatory microenvironment on TACE efficacy and patient survival. Consequently, both metrics were included.
In conclusion, we constructed this nomogram based on five key dimensions: tumor burden, treatment intensity or tolerance, liver reserve function, systemic inflammatory or immune status, and management of the underlying etiology (HBV).
Nomogram for post-recurrence survival
The nomogram was developed incorporating variables such as extrahepatic metastasis, prior anti-HBV therapy, Child-Pugh classification, TACE times, and pre-TACE SIRI score. These factors, identified as significant through the Cox regression model and corroborated by existing predictors, scientific literature, and clinical relevance, are intended to predict 2- and 3-year PRS rates after TACE in patients with recurrent HBV-associated HCC (see Fig. 3). The nomogram enables the calculation of survival probability by summing the values assigned to each variable on the scale. A lower overall prognostic score indicates a higher likelihood of achieving 2- and 3-year PRS rates. However, due to the limited number of 5-year survivors, the model does not predict 5-year outcomes.

Nomogram for predicting the 2- and 3-year PRS rates after TACE in patients with postoperative recurrence of hepatitis B virus-associated hepatocellular carcinoma. HBV, hepatitis B virus; PRS, post-recurrence survival; SIRI, systemic inflammatory response index; TACE, transarterial chemoembolization.
Evaluation of the prognostic nomogram
In the training cohort, the C-index for PRS prediction was 0.76 (95% CI: 0.70, 0.81), which was significantly superior to that of the BCLC recurrence staging system (0.66; 95% CI: 0.60, 0.72; P = 0.014). The calibration curve for 2- and 3-year PRS probabilities exhibited excellent agreement between the nomogram predictions and the actual observations (see Fig. 4a). In the internal validation cohort, the C-index for PRS prediction was 0.76 (95% CI: 0.66, 0.83), which did not differ significantly from the BCLC recurrence staging system (0.76, 95% CI: 0.69, 0.83; P = 0.864). In the external validation cohort, the C-index for PRS prediction was 0.73 (95% CI: 0.67, 0.79), which exceeded that of the BCLC recurrence staging system (0.66; 95% CI: 0.58, 0.72; P = 0.086). The calibration curves for the 2- and 3-year PRS aligned with the training cohort (see Fig. 4b and c). Additionally, the calibration curves for 2- and 3-year PRS, based on the BCLC recurrence staging system, demonstrated consistency across the training and both validation cohorts (see Supplementary Fig. S1 online).

The calibration curves for predicting the 2- and 3-year PRS in the training (a), internal validation (b) and external validation (c) cohort. PRS, post-recurrence survival.
Discrimination of prognostic nomogram
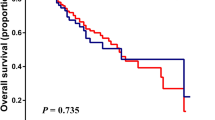
The discriminatory power of the nomogram in predicting PRS was evaluated by dividing predicted probabilities into three risk groups and plotting Kaplan-Meier curves for the training cohort (see Fig. 5). Supplementary Table S2 online shows baseline data for risk groups across three cohorts. In the training cohort, the nomogram categorized patients into low-, medium-, and high-risk groups with 1-year PRS rates of 82.4%, 47.6%, and 6.7%, 2-year rates of 70.6%, 28.6%, and unavailable, and 3-year rates of 31.0%, 6.2%, and unavailable (all P < 0.001). In the internal validation cohort, 1-year PRS rates were 85.7%, 35.7%, and 33.3%, and 2-year rates were 57.1%, 28.6%, and unavailable (P = 0.037). In the external validation cohort, 1-year PRS rates were 85.7%, 35.5%, and 12.5%, and 2-year rates were 67.9%, 22.6%, and unavailable (P < 0.001). Kaplan-Meier curves for the BCLC recurrence staging of HBV-associated HCC were also generated for all cohorts (see Supplementary Fig. S2 online). We also further evaluated the discriminatory power through DCA and compared it with the BCLC recurrence staging system. The PRS prediction model demonstrated superior net benefit rates compared to the BCLC recurrence staging system at equivalent risk threshold and a larger area under the curve (see Supplementary Fig. S3 online).

Kaplan-Meier curves of post-recurrence survival for subgroups of patients. Patients were stratified by the prognostic score in the training (a), internal validation (b) and external validation (c) cohort.
Discussion
We developed a nomogram based on liver function, tumor biologic behavior, hepatitis infection and systemic inflammation. This nomogram utilized cohort data to assess the prognosis of patients with HBV-associated HCC who experienced recurrence following curative resection and underwent TACE. It effectively stratified patients into prognostic subgroups with distinct PRS outcomes.
HBV infection significantly increased the risk of developing HCC. Current treatment strategies for HBV-associated HCC patients emphasized the importance of continuous antiviral therapy. Effective anti-HBV therapy not only reduces viral load but also plays a pivotal role in preserving liver function, which is essential for the management of HCC as it directly influences patients’ eligibility for ongoing treatment and follow-up post-disease progression22. Our multivariable Cox regression analyses suggested the necessity of chronic antiviral therapy in HBV-associated HCC patients, emphasizing the interaction between antiviral therapy and maintenance of liver function status. Growing evidence supports incorporating antiviral agents and maintaining liver function in HCC treatment, potentially improving patient prognosis and survival outcomes22,23.
Although extrahepatic recurrent metastases are indicative of an advanced tumor stage, liver failure resulting from intrahepatic tumor growth remains the predominant cause of mortality in the majority of patients with HCC. Empirical evidence suggested that patients exhibiting extrahepatic metastases demonstrated inferior overall survival (OS) and progression-free survival (PFS) compared to those with intrahepatic metastases24,25. For surgically resected patients, extrahepatic recurrences also had worse OS than intrahepatic recurrences25. Our study incorporated extrahepatic metastases into the nomogram after recognizing it as a prognostic risk factor following TACE in patients with recurrent HBV-associated HCC. TACE not only blocked the tumor’s blood supply and nutritional sources but also treated intrahepatic lesions through perfusion chemotherapy. However, extrahepatic lesions are not amenable to direct treatment via TACE and instead necessitate a therapeutic regimen comprising TKIs, chemotherapy, or ICIs. Despite the rapid advancements in research and the widespread adoption of ICIs in clinical practice in recent years, by the end of 2020, only a small percentage of patients in China with adequate financial resources had access to ICI treatment. Furthermore, a lack of familiarity with ICIs among some physicians led to adverse events. Given that only 12 patients in our cohort received ICI treatment, a comprehensive evaluation of its efficacy was not feasible.
We categorized patients into three groups based on the number of TACE: 1, 2, and ≥ 3. The baseline profiles of patients in the three groups were compared and the results are attached in Table S3 of the Supplementary Material. We found that baseline information such as age, gender, and ECOG PS scores were balanced, but indicators that responded to tumor load, such as extrahepatic metastases, tumor diameter, and number were different for these baseline indicators. The differences in these metrics are consistent with the clinical reality that patients tend to be in more advanced stages the more times they receive TACE. Although patients who underwent more TACE are often considered to be at a more advanced stage clinically (selection bias), our multifactorial analysis, after adjusting for extrahepatic metastases and hepatic function grading, still found the number of TACEs to be an independent protective factor against recurrence. This seemingly contradictory result may reflect two key points: (1) patients who are able to tolerate and complete multiple on-demand TACE, in and of themselves, represent a prognostically superior subgroup with a good response to treatment and more stable liver function reserve; and (2) more importantly, in patients with comparable tumor loads and liver function, sustained and effective TACE therapy does provide additional tumor control benefits and delays recurrence progression. This emphasizes the importance of aggressive implementation of an on-demand, multiple TACE strategy in eligible patients. However, the nature of residual confounding and observational studies means that causality needs to be interpreted with caution and could be further validated in future studies using methods such as time-dependent analysis.
The findings from recent studies underscore the critical role of the SIRI as a prognostic biomarker in liver cancer, particularly HCC26,27. Elevated SIRI values suggested an increased inflammatory state, which may contribute to tumor development and adverse clinical outcomes. This connection is explained by the complex interplay between inflammation and cancer biology. Chronic inflammation is associated with tumor cell evasion of the immune system, increased angiogenesis, and carcinogenesis28,29. In addition, the ability of SIRI to stratify patients based on risk suggests its potential integration into clinical practice for guiding treatment decisions and monitoring disease progression. A more comprehensive understanding of prognosis can be achieved by combining SIRI with traditional prognostic factors such as liver function and tumor stage30. Future studies should seek to confirm these results in larger groups and investigate interventions to mitigate systemic inflammation, thereby improving outcomes for liver cancer patients.
The BCLC staging system was initially designed to connect staging with treatment recommendations for primary HCC, not recurrent HCC. Researches indicated a correlation between the BCLC recurrence staging system and PRS7. Previous studies have used BCLC staging for risk stratification after TACE13. Our nomogram had a higher C-index of 0.76 than the BCLC recurrence staging system of 0.66, indicating better discriminatory power. Although the recommended first-line treatment options for BCLC stage C include TKIs, ICIs, or a combination of both, there remains global controversy, with many patients undergoing TACE. Treatment recommendations by doctors are based on tumor burden, liver function, and the anticipated prognosis of different treatments. Nevertheless, patient factors, such as financial cost, also impact the final decision. Our study mirrors real-world clinical settings, thereby augmenting the practical applicability of our nomogram.
The integration of TKIs and ICIs with other systemic therapies has markedly advanced clinical practice, becoming the primary treatment for BCLC stage C patients9,10,31,32,33. For BCLC stage B, TACE is the recommended therapy34. TACE has remained the standard treatment for moderate to advanced HCC and recurrent HCC following curative resection in China and most developing countries due to its accessibility, reproducibility and affordability. Kudo and colleagues35 suggested that combining TACE with Sorafenib improved median survival, OS and PFS compared to Sorafenib alone for unresectable HCC. The CHANCE001 study36 demonstrated that the combination of TACE with PD-(L)1 inhibitors and molecular targeted therapies is more efficacious than TACE alone in the treatment of unresectable HCC, extending median survival by 3.5 months. Furthermore, the LEAP-012 study37 reported that TACE combined with Lenvatinib and pembrolizumab for unresectable non-metastatic HCC significantly improved objective response rate (ORR 47% vs. 33%) and progression-free survival (median PFS 14.6 vs. 10.0 months) compared to dual placebo. The GUIDANCE001 study38 suggested that a triple therapeutic regimen comprising TACE, TKIs, and ICIs may enhance the surgical conversion rate (hepatic resection rate of 36.4% compared to 23.5%) relative to TACE alone in patients with intermediate to advanced HCC. However, this potential benefit must be carefully balanced against the risk of adverse events.
Tumor diameter and tumor number were excluded from the Cox regression analysis. However, the tumor burden was crucial for the patient’s prognosis. Our model also needed to be validated on larger samples, and rather than relying solely on the model, it needed to be considered in the context of clinical reality. The reason for this situation may be that TACE was different from surgery, and TACE cannot achieve radical resection in either a single tumor or multiple tumors. However, the accessibility of TACE for single and multiple tumors was similar, and simultaneous embolization of multiple vessels can be performed at the same time, which of course may affect the liver function for a short period. Alternatively, our target population was recurrent HCC after curative resection, and it was likely that the tumor had infiltrated into the microenvironment.
Our research has limitations. First, selection bias is a risk in observational studies, though minimized by including all consecutive patients. Second, despite strong predictive performance, our model’s small sample size and lack of extensive validation require further testing with larger datasets. Additionally, the model focused on recurrent HBV-associated HCC in a Chinese population, which may limit its generalizability to other races and regions. Third, the study didn’t include all prognostic factors, like genomic data, which could affect the model’s completeness and should be addressed in future research.
Inclusion of additional clinical variables and biomarkers in the prognostic model could be explored to improve the accuracy of prediction. The utility of the nomogram in informing clinical treatment decisions, such as the modification of TACE treatment strategies based on score results, could also be investigated. In addition, the use of the model can be explored in combination with other therapeutic methods (e.g., targeted therapy and immunotherapy) to optimize the comprehensive treatment plan.
In summary, this study has developed an effective tool for predicting recurrence in patients with HBV-associated HCC following TACE. By incorporating multiple clinically relevant factors, the nomogram offers precise survival predictions for individual patients, thereby aiding clinicians in formulating more informed treatment plans and prognostic evaluations. Moreover, the processes of model construction and validation offer valuable insights and guidance for the development of other tumor prognosis models, thereby contributing to the advancement of personalized medicine.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Bray, F. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 74, 229–263 (2024).
Han, B. et al. Cancer incidence and mortality in China, 2022. J. Natl. Cancer Cent. 4, 47–53 (2024).
Llovet, J. M. et al. Hepatocellular carcinoma. Nat. Rev. Dis. Primer. 7, 6 (2021).
Lin, J. et al. Epidemiological characteristics of primary liver cancer in Mainland China from 2003 to 2020: a representative multicenter study. Front. Oncol. 12, 906778 (2022).
Hsiao, C. Y. et al. Risk factors, patterns, and outcome predictors of late recurrence in patients with hepatocellular carcinoma after curative resection: a large cohort study with long-term follow-up results. Surgery 176, 2–10 (2024).
European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinoma. J. Hepatol. 69, 182–236 (2018).
Tabrizian, P., Jibara, G., Shrager, B., Schwartz, M. & Roayaie, S. Recurrence of hepatocellular cancer after resection: patterns, treatments, and prognosis. Ann. Surg. 261, 947–955 (2015).
Cheng, A. L. et al. Updated efficacy and safety data from IMbrave150: atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J. Hepatol. 76, 862–873 (2022).
Gao, X. et al. Safety and antitumour activity of cadonilimab, an anti-PD-1/CTLA-4 bispecific antibody, for patients with advanced solid tumours (COMPASSION-03): a multicentre, open-label, phase 1b/2 trial. Lancet Oncol. 24, 1134–1146 (2023).
Qin, S. et al. Camrelizumab plus Rivoceranib versus Sorafenib as first-line therapy for unresectable hepatocellular carcinoma (CARES-310): a randomised, open-label, international phase 3 study. Lancet 402, 1133–1146 (2023).
Lin, W. P. et al. Development and validation of a model including distinct vascular patterns to estimate survival in hepatocellular carcinoma. JAMA Netw. Open. 4, e2125055 (2021).
He, Y. et al. Development and validation of a nomogram for predicting postoperative early relapse and survival in hepatocellular carcinoma. J. Natl. Compr. Canc Netw. 22, 1–7e42 (2024).
Wang, Q. et al. Development of a prognostic score for recommended TACE candidates with hepatocellular carcinoma: a multicentre observational study. J. Hepatol. 70, 893–903 (2019).
Zhu, H. D. et al. Transarterial chemoembolization for hepatocellular carcinoma: treatment algorithm proposed by Chinese college of interventionalists (CCI). EngMedicine 1, 100037 (2024).
Cho, Y. et al. Transarterial chemoembolization for hepatocellular carcinoma: 2023 expert consensus-based practical recommendations of the Korean liver cancer association. Clin. Mol. Hepatol. 29, 521–541 (2023).
Cui, S., Cao, S., Chen, Q., He, Q. & Lang, R. Preoperative systemic inflammatory response index predicts the prognosis of patients with hepatocellular carcinoma after liver transplantation. Front. Immunol. 14, 1118053 (2023).
Zhang, L. K. et al. Effects of tumor marker regression load score on long-term prognosis of gastric cancer patients undergoing radical surgery after neoadjuvant chemotherapy. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 50, 108367 (2024).
Harrell, F. E., Califf, R. M., Pryor, D. B., Lee, K. L. & Rosati, R. A. Evaluating the yield of medical tests. JAMA 247, 2543–2546 (1982).
Iasonos, A., Schrag, D., Raj, G. V. & Panageas, K. S. How to build and interpret a nomogram for cancer prognosis. J. Clin. Oncol. Off J. Am. Soc. Clin. Oncol. 26, 1364–1370 (2008).
Zhao, L. et al. Understanding decision curve analysis in clinical prediction model research. Postgrad. Med. J. 100, 512–515 (2024).
Camp, R. L., Dolled-Filhart, M. & Rimm, D. L. X-tile: a new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin. Cancer Res. 10, 7252–7259 (2004).
Kim, S. K. et al. Hepatitis B virus treatment and hepatocellular carcinoma: controversies and approaches to consensus. Liver Cancer. 11, 497–510 (2022).
Shelat, V. G. Improving clinical outcomes of patients with hepatocellular carcinoma: role of antiviral therapy, conversion therapy, and palliative therapy. World J. Gastrointest. Oncol. 16, 4037–4041 (2024).
Lee, J. I. et al. Prognosis of hepatocellular carcinoma patients with extrahepatic metastasis and the controllability of intrahepatic lesions. Clin. Exp. Metastasis. 31, 475–482 (2014).
He, W. et al. Nomogram to predict survival of patients with recurrence of hepatocellular carcinoma after surgery. Clin. Gastroenterol. Hepatol. 16, 756–764e10 (2018).
Wenpei, G. et al. Predictive value of preoperative inflammatory indexes for postoperative early recurrence of hepatitis B-related hepatocellular carcinoma. Front. Oncol. 13, 1142168 (2023).
Gavriilidis, P. & Pawlik, T. M. Inflammatory indicators such as systemic immune inflammation index (SIII), systemic inflammatory response index (SIRI), neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) as prognostic factors of curative hepatic resections for hepatocellular carcinoma. Hepatobiliary Surg. Nutr. 13, 509–511 (2024).
Maiuri, A. R. & O’Hagan, H. M. Interplay between inflammation and epigenetic changes in cancer. Prog Mol. Biol. Transl Sci. 144, 69–117 (2016).
Greten, F. R. & Grivennikov, S. I. Inflammation and cancer: triggers, mechanisms, and consequences. Immunity 51, 27–41 (2019).
Xu, L. et al. Systemic inflammation response index (SIRI) predicts prognosis in hepatocellular carcinoma patients. Oncotarget 8, 34954–34960 (2017).
Finn, R. S. et al. IMbrave150: updated overall survival (OS) data from a global, randomized, open-label phase III study of Atezolizumab (atezo) + bevacizumab (bev) versus Sorafenib (sor) in patients (pts) with unresectable hepatocellular carcinoma (HCC). J. Clin. Oncol. 39, 267–267 (2021).
Finn, R. S. et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl. J. Med. 382, 1894–1905 (2020).
Lau, G. et al. Outcomes in the Asian subgroup of the phase III randomised HIMALAYA study of Tremelimumab plus durvalumab in unresectable hepatocellular carcinoma. J. Hepatol. S0168-8278 (24), 02424–02423 (2024).
Ding, Y. J. et al. Survival benefit of sequential curative treatment for TACE suitable BCLC stage B HCC patients. Sci. Rep. 14, 22588 (2024).
Kudo, M. et al. Randomised, multicentre prospective trial of transarterial chemoembolisation (TACE) plus Sorafenib as compared with TACE alone in patients with hepatocellular carcinoma: TACTICS trial. Gut 69, 1492–1501 (2020).
Zhu, H. D. et al. Transarterial chemoembolization with PD-(L)1 inhibitors plus molecular targeted therapies for hepatocellular carcinoma (CHANCE001). Signal. Transduct. Target. Ther. 8, 58 (2023).
Kudo, M. et al. Transarterial chemoembolisation combined with lenvatinib plus pembrolizumab versus dual placebo for unresectable, non-metastatic hepatocellular carcinoma (LEAP-012): a multicentre, randomised, double-blind, phase 3 study. Lancet 405, 203–215 (2025).
Yang, D. L. et al. Multicenter, retrospective GUIDANCE001 study comparing transarterial chemoembolization with or without tyrosine kinase and immune checkpoint inhibitors as conversion therapy to treat unresectable hepatocellular carcinoma: survival benefit in intermediate or advanced, but not early, stages. Hepatology (2025).
Acknowledgements
We would like to thank Prof. Yin-shan Yang and colleagues for providing external validation cohorts data.
Funding
This study was supported by the Yunnan Fundamental Research Project (Grant No.202201AY070001-158) and the Science Research Fund Project of Education Department of Yunnan Province (Grant No. 2023J0369).
Author information
Authors and Affiliations
Contributions
Zhang-you Guo: Data curation, Conceptualization, Supervision, Writing-review and editing, Manuscript-revised; Mu-yang Tu: Formal analysis, Methodology, Writing-original draft; Yin-shan Yang: Data curation, Funding acquisition **;** Ling-xiang Xu: Data curation, Methodology, Visualization; Dan-dan Fan: Funding acquisition, Supervision **.** All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects/patients were approved by the Ethics Committee of the Second Hospital Affiliated with Chongqing Medical University (No. 2019-60).
Informed consent
This was a retrospective study, and the investigators requested a waiver of informed consent, which was formally approved by the Ethics Committee of the Second Affiliated Hospital of Chongqing Medical University (No. 2019-60).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Guo, Zy., Tu, My., Yang, Ys. et al. Nomogram for predicting post-transarterial chemoembolization survival in recurrent patients with hepatitis B virus-associated hepatocellular carcinoma. Sci Rep 15, 42367 (2025). https://doi.org/10.1038/s41598-025-26375-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-26375-5
