
Abstract
Despite the potential of pembrolizumab and lenvatinib combination therapy in treating metastatic renal cell carcinoma (mRCC), real-world evidence on its efficacy and safety remains limited. We retrospectively analyzed data from 118 patients with mRCC who initiated pembrolizumab plus lenvatinib as first-line therapy between August 2022 and March 2024. Patient characteristics, treatment outcomes, and adverse events were evaluated. Oncological outcomes were stratified following the International Metastatic RCC Database Consortium risk classification. The objective response and disease control rates were 69.5% and 98.5%, respectively. Median progression-free survival (PFS) was 26.8 months (95% confidence interval (CI), 23.5–27.8)), whereas the median overall survival (OS) was not reached (95%CI, 20.5– not reached). Grade ≥ 3 treatment-related adverse events occurred in 39.8% of all patients. Clinical outcomes were also compared between patients aged ≥ 75 and < 75 years. Median age was 70 years; 70.3% and 29.7% aged < 75 and ≥ 75 years, respectively. No significant differences were observed in PFS and OS between the two groups (p = 0.14 and p = 0.44, respectively). Pembrolizumab plus lenvatinib demonstrated favorable efficacy and manageable safety in a real-world cohort of patients with mRCC, including older adults.
Similar content being viewed by others
Introduction
Renal cell carcinoma (RCC) is the seventh most common cancer globally, accounting for approximately 2–3% of all adult malignancies and leading to over 170,000 deaths annually1. At the time of initial diagnosis, approximately 30% of patients present with distant metastases, necessitating systemic therapy2,3. Owing to the distinct hypervascular characteristics of RCC tissues, tyrosine kinase inhibitors have played a central role in metastatic RCC (mRCC) treatment over the past two decades4. In addition, immune checkpoint inhibitors (ICIs) such as antibodies targeting programmed cell death protein-1 (PD-1) or the PD-1 ligand 1 (PD-L1), which block immunosuppressive PD-1/PD-L1 signaling pathways, have become standard therapeutic options in the management of mRCC5.
ICI-based combination therapies have been recently developed, significantly improving clinical outcomes for patients with mRCC, as evidenced in several clinical trials6,7,8,9. Among these, the combination of pembrolizumab and lenvatinib has shown particularly durable antitumor activity, with an objective response observed in 71.3% of patients10,11. Updated data from the second interim analysis of progression-free survival (PFS), with a median follow-up of 49.8 months, revealed that pembrolizumab plus lenvatinib significantly improved PFS and nearly doubled the objective response rate (ORR) compared to sunitinib. However, real-world evidence regarding the clinical efficacy of this combination therapy remains limited.
In the present study, we aimed to evaluate the real-world efficacy and toxicity of pembrolizumab plus lenvatinib in patients with mRCC across all risk categories as defined by the International Metastatic RCC Database Consortium (IMDC). Clinical outcomes were also compared between patients aged < 75 and ≥ 75 years since individuals aged ≥ 75 years are classified as late-stage elderly in Japan.
Results
Baseline characteristics
The clinical characteristics of all patients are summarized in Table 1. The median patient age was 70 years (range: 35–86 years). The most prevalent histological subtype was clear cell carcinoma, observed in 106 patients (89.8%). The number of metastatic sites ranged from one to six, with 50 (42.4%) patients presenting with multiple metastatic sites (≥ 2 metastatic lesion) at diagnosis. The most frequent site of distant metastasis was the lungs (63.6%), followed by the lymph nodes (28.8%). Based on the IMDC risk classification, 22.9% of patients were categorized as favorable risk, 50.8% as intermediate risk, and 26.3% as poor risk. Prior to study enrollment, 76 patients (64.4%) underwent nephrectomy, and 37 patients (31.4%) underwent tissue biopsies. The most common treatment administered immediately after pembrolizumab plus lenvatinib was cabozantinib (9.3%).
Clinical outcomes of pembrolizumab plus lenvatinib
The median follow-up duration was 16.4 months (range: 5.3–33.8). At data cutoff, 57 (48.3%) and 66 (55.9%) patients discontinued pembrolizumab and lenvatinib therapy, respectively, mainly due to the AE (29.7%) and disease progression (14.4%). During the observation period, cancer-related mortality occurred in 15 (12.7%) patients. The median PFS was 26.8 months (95% confidence interval (CI), 23.5–27.8), whereas the median OS was not reached (NR) (95%CI, 20.5–NR, Fig. 1). Of the 118 patients, 13 achieved CR (11.0%), 69 achieved PR (58.5%), 31 achieved SD (26.3%), and 5 achieved PD (4.2%), resulting in an ORR and disease control rate (DCR) of 69.5% and 95.8%, respectively (Table 2).

Kaplan–Meier survival curve for all patients with mRCC treated with pembrolizumab plus lenvatinib. (A) Progression-free survival (PFS) and (B) overall survival (OS). NR; not reached.
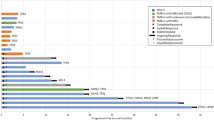
The ORRs stratified by IMDC risk were: favorable 0 (70.4%), intermediate (71.7%), and poor (64.5%), respectively. When we evaluated the ORRs by IMDC score, the ORR with score 1, 2, 3, and 4–6, were 71.3%, 73.1%, 65.0%, and 53.8%, respectively (Fig. 2A). PFS and OS in each IMDC risk group was shown in Fig. 2B and C. While there was no statistically significant difference in ORR between the intermediate- and poor-risk groups (p = 0.226), patients with favorable/intermediate-risk showed significantly longer PFS (hazard ratio (HR), 0.344; 95% CI, 0.137–0.862, p = 0.023, Fig. 3A) and OS (HR, 0.0809; 95% CI, 0.0264–0.247, p < 0.0001, Fig. 3B) than those with poor risk. Moreover, median CRP levels were significantly lower in the IMDC favorable/intermediate-risk than in the poor- risk groups (Fig. 3C). Although patients in the favorable-risk group did not exhibit a significantly longer PFS compared with those in the intermediate- or poor-risk groups (HR, 0.671; 95% CI, 0.262–1.718; p = 0.406; Supplementary Fig. S1A), they demonstrated a significantly longer OS (HR, 0.271; 95% CI, 0.0851–0.856; p = 0.027; Supplementary Fig. S1B).

Survival analysis for patients according to the International Metastatic RCC Database Consortium (IMDC) risk classification. (A) Objective response rates stratified by the number of IMDC risk factors. (B) Progression-free survival (PFS) by IMDC risk group: favorable- (n = 27), intermediate- (n = 60), and poor-risk (n = 31) groups. (C) Overall survival (OS) by IMDC risk group. (D) Comparative analysis of baseline C-reactive protein levels between IMDC poor- and favorable/intermediate risk-groups.

Survival analysis for patients with International Metastatic RCC Database Consortium (IMDC) favorable/intermediate- and those with poor- risk. Kaplan-Meier curve of (A) progression-free survival (PFS) and (B) overall survival (OS) in patients with IMDC favorable/intermediate- (n = 87) and poor-risk (n = 31) groups. (C) Comparative analysis of baseline C-reactive protein levels between IMDC poor- and favorable/intermediate risk-groups.
In this cohort, 83 (70.3%) and 35 (29.7%) patients were aged < 75 and ≥ 75 years, respectively (Supplementary Table S1). ORRs were 71.4% in the < 75-year group and 62.7% in the ≥ 75-year group, with CR rates of 14.3% and 9.6%, respectively. However, no significant differences were observed in PFS (HR, 0.553; 95% CI, 0.228–1.45; p = 0.14) or OS (HR, 1.032; 95% CI, 0.361–2.952; p = 0.44) between the two age groups (Fig. 4).
AEs leading to pembrolizumab discontinuation occurred in 44.6% of patients aged < 75 years and 57.1% of patients aged ≥ 75 years. For lenvatinib, discontinuation occurred in 48.1% and 74.3% of patients aged < 75 and ≥ 75 years, respectively. The frequency of AEs leading to discontinuation of pembrolizumab or lenvatinib was not significantly different between the two groups (p = 0.785, Supplementary Table S1).
Influence of upfront cytoreductive nephrectomy for synchronous mRCC
Next, we assessed the efficacy of nephrectomy in patients with synchronous metastatic disease (M1) at mRCC diagnosis who subsequently received pembrolizumab plus lenvatinib. Among 61 patients (51.7%) with M1 disease, 19 patients (31.1%) underwent cytoreductive nephrectomy (CN). To align the clinical background, patients with M1 disease were divided into the IMDC intermediate- and poor-risk groups, and PFS and OS were evaluated. As a result, there was no statistically significant difference of PFS (HR, 0.764; 95% CI, 0.148–3.953; p = 0.748, HR, 1.355; 95% CI, 0.221–8.313; p = 0.743, respectively) and OS between patients with and without CN in both IMDC groups (HR, 1.871; 95% CI, 0.096–10.370; p = 0.679, HR, 1.419; 95% CI, 0.240–8.397; p = 0.700) (Supplementary Fig. S2 and S3).
Safety analysis
Treatment related AEs are summarized in Table 3. Overall, treatment-related AEs occurred in 84.7% of patients, with hypertension (39.8%), hypothyroidism (22.9%), and Palmer-plantar erythrodysesthesia syndrome (18.6%) being the most common AEs. Grade ≥ 3 AEs occurred in 39.8% of patients, with the most frequent being hypertension (8.5%), followed by proteinuria (6.8%) and diarrhea (6.8%). Eighteen (18.0%) patients required steroid treatment for immune-related AEs.
Discussion
The therapeutic landscape for mRCC has undergone considerable transformation with the advent of ICIs. Over the past seven years, five ICI-based combination therapies have been approved and are now preferred as first-line treatments for advanced clear cell RCC (ccRCC) by the National Comprehensive Cancer Network12. Among them, the combination of pembrolizumab and lenvatinib showed substantial efficacy in patients with ccRCC as well as in non-ccRCC patients, showing consistent benefit across various metastatic sites, including the lungs, lymph nodes, liver, and bones13,14,15. However, real-world evidence regarding this combination therapy remains limited, highlighting the need for data that can guide treatment decisions in clinical practice. Accordingly, in this study, we aimed to evaluate the real-world efficacy and safety of pembrolizumab plus lenvatinib in patients with mRCC to explore factors influencing clinical outcomes.
First, our findings confirmed favorable clinical efficacy of pembrolizumab plus lenvatinib, as reflected by a high ORR of 69.5% and prolonged PFS and OS (Fig. 1; Table 2). Lenvatinib is a multi-target TKI that selectively inhibits several receptor pathways, including vascular endothelial growth factor receptor (VEGFR), fibroblast growth factor receptor (FGFR), platelet-derived growth factor receptor α (PDGFR α), RET, and KIT molecules16. Our findings are consistent with those observed in the pivotal CLEAR trial (including a subgroup analysis of patients enrolled in Japan), although the CR rate in the present study was lower than that in previous reports (11.0% vs. 16.1–19.0%)10,14. We speculated that this discrepancy may be attributed to a higher proportion of patients with IMDC poor-risk status (26.3%) in our cohort, who likely had higher baseline tumor burden than those in the favorable- or intermediate-risk groups17. In addition, baseline CRP levels were significantly elevated in the poor-risk group, which may reflect a more immunosuppressive tumor microenvironment and systemic inflammation that impair ICI efficacy (Fig. 2D)18,19.
Second, to the best of our knowledge, this is the first study to demonstrate comparable efficacy of pembrolizumab plus lenvatinib in patients aged ≥ 75 and < 75 years in terms of PFS and OS (Fig. 4). Despite growing use of ICIs in mRCC, data on their safety and efficacy in elderly patients remain limited in real-world settings. Several clinical trials reported PFS and OS for the subgroup aged ≥ 65 years7,9,10,20,21, whereas three trials performed the subgroup analysis among patients aged ≥ 75 years7,20,22 since geriatric oncology guidelines recommend patients ≥ 75 years should routinely undergo comprehensive geriatric assessment before treatment decisions23. Additionally, clinical trial participants tend to be younger than the general patient population by a median age of 64.9 years24. Importantly, in our study, discontinuation rates due to AEs were not significantly different between the two age groups (≥ 75 and < 75 years), suggesting that this ICI-based combination therapy is feasible and tolerable in elderly patients. Nonetheless, prospective studies are warranted to better define the risk-benefit profile of pembrolizumab and lenvatinib in elderly patients with mRCC.

Survival analysis by age group. (A) Progression-free survival (PFS) and (B) overall survival (OS) in patients aged < 75 (n = 83) and aged ≥ 75 (n = 35). NR; not reached.
Third, in patients with synchronous metastatic disease at diagnosis, we observed there was no significant difference between patients with and without CN in terms of PFS and OS when patients were stratified into the IMDC intermediate- and poor-risk groups for evaluation (Supplementary Fig. S2 and 3). The relevance of upfront CN in mRCC remains controversial25,26. Bakouny et al. reported that upfront CN was associated with significantly better OS in ICI-treated patients (HR,0.72; 95%CI, 0.67–0.78; p < 0.001) using IMDC database27. Singla et al. also showed improved OS in patients receiving CN before ICI therapy compared to those who did not undergo CN28. Previous reports demonstrated that primary RCC tumors secrete pro-inflammatory cytokines that drive inflammation and suppress T-cell activity, potentially limiting the effectiveness of systemic immunotherapy29,30. On the other hand, Li et al. reported that the deferred CN was observed to be correlated with superior OS compared to the upfront CN in patients with ICI-based combination subgroup analysis31. However, these findings are retrospective, observational, and subject to selection bias, which underscores the need to conduct randomized controlled trials with ICI-based regimens.
Finally, we found that the percentage of grade ≥ 3 AEs was lower in our study population when compared to that in general population treated with pembrolizumab plus lenvatinib (39.8% vs. 82.4%). As an additional example, in patients with avelumab plus axtinib therapy, grade ≥ 3 AEs occurred in 17.1% of Japanese patients, whereas 71.2% of global population experienced grade ≥ 3 AEs6,32. Differences in the incidence and severity of drug-related AEs between Asian and global (primarily Western) populations may arise from a combination of genetic, physiological, environmental, and clinical factors33,34. On the other hand, Asian populations frequently experience higher rates of hematologic or hepatic toxicities but sometimes lower rates of gastrointestinal or fatigue-related events33. These differences highlight the importance of intense monitoring while receiving treatment.
This study has some limitations. First, the retrospective and observational study design with a small sample size introduces potential selection bias. Second, data were limited to those available in medical records, which may have resulted in an underestimation of disease burden and treatment-related AEs. Third, this report is based on a Japanese population, and therefore these findings cannot be directly generalized to all racial or ethnic groups. Fourth, short median follow-up might underscore the incidence of AEs and clinical prognosis. Finally, due to the low number of events such as disease progression or death, we were unable to perform multivariate analyses of PFS and OS.
Despite these limitations, to the best of our knowledge, this is the first real-world study to demonstrate that pembrolizumab plus lenvatinib offers promising clinical outcomes in patients with mRCC. Our findings validate the efficacy and tolerability of this combination therapy across all age groups, including patients aged ≥ 75 years. These results support the use of pembrolizumab plus lenvatinib as a viable first-line treatment option for mRCC in routine clinical practice.
Materials and methods
Patients
We conducted a multicenter retrospective study involving 118 patients with mRCC who received pembrolizumab plus lenvatinib as first-line therapy between August 2022 and March 2024. For each patient, data were collected on age, Karnofsky Performance Status (KPS), sex, IMDC risk group, tumor histology, comorbidities, and sites of metastasis.
Tumor response was evaluated using imaging modalities such as computed tomography (CT) or magnetic resonance imaging (MRI), according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1, every 2–3 months. We evaluated tumor responses (complete response [CR], partial response [PR], stable disease [SD], or progressive disease [PD]), PFS, and overall survival (OS). PFS was defined as the time from initiation of pembrolizumab plus lenvatinib treatment to either documented disease progression or death from any cause. OS was defined as the time from treatment initiation to death from any cause or last follow-up. Adverse events (AEs) during treatment were collected and graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE) version 5.035.
This multicenter study was conducted in accordance with the ethical standards of the Declaration of Helsinki and approved by the Institutional Review Board of each participating institution (approval number 018 − 0003 at Osaka University Hospital). The institutional review board of Osaka University Hospital approved that this research was properly conducted in an opt-out format. All methods were performed in accordance with the relevant guidelines and regulations by including a statement.
Informed consent
was obtained from all patients for data collection.
Treatment and assessment
All patients received at least one dose of pembrolizumab (200 mg intravenously every three weeks) and lenvatinib (20 mg orally once daily). Treatment was continued until disease progression, clinical deterioration, unacceptable toxicity, or patient withdrawal.
Patients continued to receive pembrolizumb or lenvatinib until disease progression in the present study.
Statistical analysis
Categorical variables were compared using Fisher’s exact test or the chi-square test. The Mann–Whitney U test (two-tailed) was performed to evaluate differences in CRP between patients in the IMDC favorable/intermediate- and poor-risk groups. PFS and OS were estimated using the Kaplan–Meier method and compared using the log-rank test. Statistical significance was set at p < 0.05. All statistical analyses were conducted using the JMP software (version 17.0; SAS Institute, Cary, NC, USA).
Data availability
The data that support the findings of this study are available from the corresponding author, TK, upon reasonable request.
References
Bukavina, L. et al. Epidemiology of renal cell carcinoma: 2022 update. Eur. Urol. 82, 529–542 (2022).
Ljungberg, B. et al. European association of urology guidelines on renal cell carcinoma: the 2022 update. Eur. Urol. 82, 399–410 (2022).
Gupta, K., Miller, J. D., Li, J. Z., Russell, M. W. & Charbonneau, C. Epidemiologic and socioeconomic burden of metastatic renal cell carcinoma (mRCC): a literature review. Cancer Treat. Rev. 34, 193–205 (2008).
Choueiri, T. K. & Motzer, R. J. Systemic therapy for metastatic Renal-Cell carcinoma. N Engl. J. Med. 376, 354–366 (2017).
Carlo, M. I., Voss, M. H. & Motzer, R. J. Checkpoint inhibitors and other novel immunotherapies for advanced renal cell carcinoma. Nat. Rev. Urol. 13, 420–431 (2016).
Motzer, R. et al. Avelumab plus axitinib versus Sunitinib for advanced Renal-Cell carcinoma. N Engl. J. Med. 380, 1103–1115 (2019).
Motzer, R. et al. Nivolumab plus ipilimumab versus Sunitinib in advanced Renal-Cell carcinoma. N Engl. J. Med. 378, 1277–1290 (2018).
Choueiri, T. K. et al. Nivolumab plus Cabozantinib versus Sunitinib for advanced Renal-Cell carcinoma. N Engl. J. Med. 384, 829–841 (2021).
Rini, B. I. et al. Pembrolizumab plus axitinib versus Sunitinib for advanced Renal-Cell carcinoma. N Engl. J. Med. 380, 1116–1127 (2019).
Motzer, R. et al. Lenvatinib plus pembrolizumab or everolimus for advanced renal cell carcinoma. N Engl. J. Med. 384, 1289–1300 (2021).
Motzer, R. et al. Lenvatinib plus pembrolizumab versus Sunitinib in First-Line treatment of advanced renal cell carcinoma: final prespecified overall survival analysis of CLEAR, a phase III study. J. Clin. Oncol. 42, 1222–1228 (2024).
Motzer, R. et al. NCCN Guidelines® insights: kidney Cancer, version 2.2024. J. Natl. Compr. Canc Netw. 22, 4–16 (2024).
Motzer, R. et al. Lenvatinib plus pembrolizumab or everolimus for advanced renal cell carcinoma. N Engl. J. Med 384 1289–1300 (2021).
Eto, M. et al. Lenvatinib plus pembrolizumab versus Sunitinib for advanced renal cell carcinoma: Japanese patients from the CLEAR study. Cancer Med. 12, 6902–6912 (2023).
Motzer, R. et al. Characterization of responses to lenvatinib plus pembrolizumab in patients with advanced renal cell carcinoma at the final prespecified survival analysis of the phase 3 CLEAR study. Eur. Urol. 86, 4–9 (2024).
Adachi, Y. et al. Inhibition of FGFR reactivates IFNγ signaling in tumor cells to enhance the combined antitumor activity of lenvatinib with Anti-PD-1 antibodies. Cancer Res. 82, 292–306 (2022).
Tannir, N. M. et al. Nivolumab plus ipilimumab versus Sunitinib for first-line treatment of advanced renal cell carcinoma: extended 8-year follow-up results of efficacy and safety from the phase III checkmate 214 trial. Ann. Oncol. 35, 1026–1038 (2024).
Fukuda, S. et al. Impact of C-reactive protein flare-response on oncological outcomes in patients with metastatic renal cell carcinoma treated with nivolumab. J Immunother Cancer 9, e001564 (2021).
Schüttke, V. et al. Early kinetics of C-reactive protein as prognosticator for survival in a real-world cohort of patients with metastatic renal cell cancer under first-line therapy with immune checkpoint inhibitors. Clin. Transl Oncol. 26, 1117–1128 (2024).
Motzer, R. et al. Nivolumab plus Cabozantinib versus Sunitinib in first-line treatment for advanced renal cell carcinoma (CheckMate 9ER): long-term follow-up results from an open-label, randomised, phase 3 trial. Lancet Oncol. 23, 888–898 (2022).
Choueiri, T. K. et al. Updated efficacy results from the JAVELIN renal 101 trial: first-line avelumab plus axitinib versus Sunitinib in patients with advanced renal cell carcinoma. Ann. Oncol. 31, 1030–1039 (2020).
Tomita, Y. et al. Efficacy and safety of avelumab plus axitinib in elderly patients with advanced renal cell carcinoma: extended follow-up results from JAVELIN renal 101. ESMO Open. 7, 100450 (2022).
Bergerot, C. D. et al. Geriatric assessment: ASCO global guideline. JCO Glob Oncol. 11, e2500276 (2025).
Ludmir, E. B. et al. Factors associated with age disparities among cancer clinical trial participants. JAMA Oncol. 5, 1769–1773 (2019).
Stellato, M. et al. Impact of previous nephrectomy on clinical outcome of metastatic renal carcinoma treated with Immune-Oncology: A Real-World study on behalf of Meet-URO group (MeetUro-7b). Front. Oncol. 11, 682449 (2021).
Yildirim, H. et al. A nationwide Real-world evaluation of upfront cytoreductive nephrectomy in patients with synchronous metastatic renal cell carcinoma in the immunotherapy era. Eur. Urol. Oncol. 8, 623–631 (2025).
Bakouny, Z. et al. Upfront cytoreductive nephrectomy for metastatic renal cell carcinoma treated with immune checkpoint inhibitors or targeted therapy: an observational study from the international metastatic renal cell carcinoma database consortium. Eur. Urol. 83, 145–151 (2023).
Singla, N. et al. Improved survival after cytoreductive nephrectomy for metastatic renal cell carcinoma in the contemporary immunotherapy era: an analysis of the National cancer database. Urol. Oncol. 38, 604e609–604e617 (2020).
Flanigan, R. C. Debulking nephrectomy in metastatic renal cancer. Clin. Cancer Res. 10, 6335s–6341s (2004).
Lahn, M. et al. Pro-inflammatory and T cell inhibitory cytokines are secreted at high levels in tumor cell cultures of human renal cell carcinoma. Eur. Urol. 35, 70–80 (1999).
Li, K. P. et al. Comparison of upfront versus deferred cytoreductive nephrectomy in patients with metastatic renal cell carcinoma receiving systemic therapy: a systematic review and meta-analysis. Int. J. Surg. 109, 3178–3188 (2023).
Nonomura, N. et al. Final analysis of Post-Marketing surveillance for Avelumab + Axitinib in patients with renal cell carcinoma in Japan. Cancer Med. 14, e70275 (2025).
Hasegawa, Y. et al. Ethnic difference in hematological toxicity in patients with non-small cell lung cancer treated with chemotherapy: a pooled analysis on Asian versus non-Asian in phase II and III clinical trials. J. Thorac. Oncol. 6, 1881–1888 (2011).
Poon, D. M. C. et al. Ethnic Pharmacogenomic differences in the management of Asian patients with metastatic prostate cancer. Cancers (Basel) 14, 407 (2022).
National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE). Version 5.0 https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm
Templeton, A. J. et al. Change in Neutrophil-to-lymphocyte ratio in response to targeted therapy for metastatic renal cell carcinoma as a prognosticator and biomarker of efficacy. Eur. Urol. 70, 358–364 (2016).
Ishihara, H. et al. Predictive impact of an early change in serum C-reactive protein levels in nivolumab therapy for metastatic renal cell carcinoma. Urol. Oncol. 38, 526–532 (2020).
Yano, Y. et al. Serum C-reactive protein level predicts overall survival for clear cell and Non-Clear cell renal cell carcinoma treated with ipilimumab plus nivolumab. Cancers (Basel) 14, 5659 (2022).
Acknowledgements
We would like to thank all the patients, family members and staff from all the units that participated in the study.
Funding
The study is based on retrospective data analysis. The authors did not receive support from any organization for the submitted work. No funds, grants, or other support was received.
Author information
Authors and Affiliations
Contributions
T. K. was responsible for the study conception and design, conducted the study, collected and analyzed the data, and drafted the manuscript. Y. N., M. S., T. T., T. I., S. T., H. O., M. T., K. O., K. K., H. H., Y. I., T. H., Y. Y., K. H., A. K., Y. O., K. N., S. T., K. F., H. T., O. M., M. N., and N. N. conducted the study, collected and analyzed the data, drafted the study, and revised the manuscript. All authors have read and approved the final manuscript for submission.
Corresponding author
Ethics declarations
Competing interests
The other authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Kato, T., Nakai, Y., Sato, M. et al. Real-world efficacy and safety of pembrolizumab plus lenvatinib in patients with metastatic renal cell carcinoma: a multi-institutional retrospective study. Sci Rep 15, 43676 (2025). https://doi.org/10.1038/s41598-025-27578-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-27578-6
