
Abstract
The aim of study was to evaluate the efficacy of the use of three-dimensional (3D) printing model for preoperative planning in treatment of tibial plateau fracture. Besides, we also investigated the effect of 3D printing technology on the communication between doctors and patients. Thirty-three patients with tibial plateau fractures were enrolled in the study from March 2022 to July 2023. A 3D digital model of each tibial plateau fracture was constructed, and the individual model was exported to a 3D printer for the construction of a full solid model. This 3D-printing model, along with the Three-Column classification, was utilized to plan the operation. During each operation, the operative time and amount of blood loss were recorded as primary outcome measures. Patients were followed to evaluate surgical outcomes using Rasmussen scores and radiological evaluation, which served as secondary outcome measures. Additionally, satisfaction for patients was assessed using questionnaires developed by Yiting Lou. Two-column fractures accounted for the highest proportion at 45.5%. Isolated posterior column fractures constituted 9.1%. The average 3D printing time was 7.1 ± 0.9 h; a material cost of 1 USD per model. Complex fracture cases had significantly longer 3D printing times (p = 0.001) and provided more information to the surgical team than simple fractures. Patient satisfaction with 3D models was rated at 7.4 ± 0.7 out of 10 points. Malalignment and gap width were not correlated with surgical time (p = 0.3 and 0.2). The infection rate was 3%, and the rate of secondary loss of reduction at six months was 25%, with no correlation with Rasmussen scores (P > 0.05, Fisher’s test). Our study revealed that 3D printing models effectively assist the surgeons in planning operations, especially in complex cases, and may enhances communication between surgeons and patients. Follow-up 6 months after surgery showed good knee function.
Similar content being viewed by others

Introduction
Tibial plateau fractures are peri-articular knee fractures of the proximal tibia. They comprise approximately 8% of all fractures among those aged over 55 years1 .The presentation is dependent on the mechanism of injury and is usually from either very high-energy trauma (typically younger men) or low-energy trauma (typically older women, as a fragility fracture)2. The treatment of tibial plateau fractures remains a challenge in many respects. Historically, the Schatzker and AO/OTA classifications, based on radiographic assessment of fracture patterns, have been widely used to guide treatment decisions. Limitations of these classifications include identifying the integrity of the posterior articular surface or posterior column. Therefore, Three-Column Classification based on CT imaging has been introduced for improved assessment of tibial plateau fracture, especially the posterior column which is higher rate than expected in complex tibial plateau fracture according to recent studies3,4. Nowadays, accurate and individualized surgery is becoming more and more essential in fracture fixations, so that, many studies have described the use of 3D printing model in the treatment of tibial plateau fracture. 3D printing technology allows clinicians to accurately design surgical approaches for fracture treatment to allow for more accurate surgical outcomes and to improve the quality of reduction and operational reliability. Thanks to 3D printing technology, the fracture morphology can be recreated as a physical model, allowing clinicians to observe the degree of tibial plateau injury and the planar fracture collapse position5. 3D modeling can allow surgeons to observe fracture morphology and collapse more intuitively, to design more accurate surgical approaches and reduction methods for internal fixation operation, which can avoid unnecessary soft tissue stripping and reduce wound complications6.
In 2023, Osma-Rueda found that the reproducibility was better when evaluating the classification using 3D printing than when using CT scans; 3D printing provided more information than CT and decreased measurement errors7. In addition, some authors have illustrated that 3D-assisted surgery reduces operation time, minimizes blood loss, and decreases the frequency of fluoroscopy6,8,9. However, the functional outcome remains unclear. Guidelines for medical 3D printing from the Radiological Society of North America (RSNA) 3D Printing Special Interest Group (SIG) suggest that 3D printing may be appropriate for acute complex intraarticular fractures5. Therefore, we conducted this study with the aim of using 3D printing models and the Three-Column classification to plan the operation and evaluate communication between doctors and patients.
Materials and methods
The study was conducted at the Department of Orthopedics, Hue University of Medicine and Pharmacy Hospital from March 2022 to July 2023. The study design is a descriptive cross-sectional analysis. The steps of conducting the research are described in Fig. 1.
Patients
Thirty-three patients with tibial plateau fracture were enrolled in the study. Of the admitted patients, there were 20 males and 13 females, with a mean age of 42.33 ± 12.7 years.

Flow diagram.
Printing the 3D model
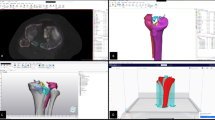
We received CT scans of tibial plateau fracture patients from the PACS system of our hospital. The original CT data were stored in Imaging and Communication in Medicine (DICOM) format, and the 3D model was created using Mimics software v10.01 (Materialise, Leuven, Belgium). The threshold value was set at “Bone (CT)” with a maximum of “226-Max,” which is optimal for bone reconstruction. This threshold may be adjusted based on the patient’s bone quality. Subsequently, we generated 3D digital images of the fracture in Mimics software, removing the femur and patella. Then, the data were imported into Ultimaker Cura 3D printing software in stereolithography (STL) format. After creating supports for the 3D digital model and calculating the printing time, we saved it in Gcode format and exported it to a 3D printer (Ender 5 Pro) to produce a full-scale physical model (1:1 ratio of the actual fracture) (Fig. 1).
The 3D printing time is calculated as the sum of the time spent on modeling in the software and the printing time of the 3D printer. Cases requiring emergency surgery (injuries to the neurovascular bundle, compartment syndromes, open fractures) still undergo 3D model printing before the surgery. If the 3D printing time doesn’t allow sufficient preparation for the operation, such cases will be excluded from the study.
Pre-operative planning based on 3D-printed model and three-column concept
Pre-operative planning with the application of the updated Three-Column Concept includes the traditional three-column classification and incorporates the mechanism of injury. Injuries were categorized into different fracture types based on the previously described Three-Column Concept. In this classification system, the tibial plateau is divided into three parts, specifically defined as the lateral, medial, and posterior columns as observed on axial plane CT images and 3D printing models. Additionally, the posterior column is further divided into the medial and lateral posterior columns (Fig. 2) A column is considered fractured if there is any disruption of the corresponding extra-articular cortical bone. Injuries are then further classified into zero and one-column fractures, which are relatively simple, and more complex two-column and three-column fractures.
The 3D printing model can also assist in providing crucial information about the mechanics of the injury itself (Fig. 2) A better understanding of the injury mechanics enables more effective reversal of the forces that led to the fracture. For instance, a hyperextension injury typically impacts the anterior columns with varus or valgus extension, affecting both the medial and lateral columns. On the other hand, flexion injuries usually involve the posterior column. Understanding the mechanics of the injury helps identify areas on the tibial plateau where damage is most likely to have occurred. In other words, comprehending the types and directions of the forces responsible for obvious damage allows for an exploration of less apparent damage that might lead to later complications.
Additionally, the flexion/extension position of the knee is assessed based on the posterior tibial slope angle (pTSA), measured on either the lateral radiographic plain film image or sagittal CT images. The varus/valgus force is determined by the medial tibial plateau angle (mTPA), measured on either the anterior-posterior (AP) radiographic plain film image or coronal CT images. A decreased (or negative) pTSA indicates the injured knee is in extension mode, while an increase indicates a flexion mode. A decreased mTPA indicates a varus force, whereas an almost normal value of mTPA indicates a valgus force.
Not all fractured columns require fixation, and there are differences in the functionality of the implants among these fractured columns. Primary plating with the main buttress function is applied to the compression side. If the tension side is comminuted or unstable, the application of a secondary supporting plate is recommended3.

These three columns are separated by three connecting lines, namely OA, OC, and OD. Point O is the center of the knee (midpoint of two tibial spines); Point A represents the anterior tibial tuberosity; Point D is the posteromedial ridge of proximal tibia; and Point C is the most anterior point of the fibular head. Point B is the posterior sulcus of the tibial plateau, which intersects the posterior column into the medial and lateral parts.
Computer-assisted surgical simulation: Using Mimics and 3-Matic software, we classified the fracture fragments and marked them with different colors. Subsequently, we tested reducing the fracture fragments, adjusting rotational and angulation deformities, while restoring the anatomical axis of the proximal tibia and joint surface. The plan for adjustments was annotated and communicated to the entire surgical team to be implemented in the actual surgical procedure (e.g., how to reduce the fragments in what sequence, which direction to rotate the fragments, which column to adjust first).
Surgical simulation in 3D printing model: Appropriate plates were selected to match the patient’s tibial plateau anatomy, adhering to the Three-Column and AO principles of fracture fixation. After completing the simulation on the model, the surgeon proceeded with the surgery following the preoperative plan (Fig. 3).

Surgical simulation before operation.
Postoperative management and follow-up
Postoperatively, early range of motion and non-weight bearing were emphasized. Passive range-of-motion exercises were initiated on the first post-operative day. Toe-touch weight bearing was initiated at 8 weeks. Full weight bearing was not permitted until radiographic signs of primary bone healing, usually present at 12 weeks postoperative. All patients were followed at one month, three months and six months postoperatively.
Evaluation
Standard AP and lateral radiographs were evaluated. mTPA, pTSA and articular step-off were measured at immediate postoperative and 6-month follow-up. Malreduction was defined as intraarticular step-off > 2 mm. Malalignment was defined as mTPA ≥ 90° or ≤ 80°; pTSA ≥ 15° or ≤-5°. Secondary loss of reduction was defined as an increase of 3° malalignment or an articular depression 2 mm when compared with the first post-operative radiograph10. Bony union was defined radiolographically by the treating surgeon as at least three cortical unions during the follow-up period. Nonunion was defined as no evidence of healing after 6 months.
Objective knee evaluation and patient reported functional outcomes were assessed at 18-month follow-up according to the Rasmussen score11 (see Appendix 1). Complications including infection, wound irritation and neurovascular injury were noted as well.
Statistical methods
SPSS Statistics 20.0 software (IBM SPSS Inc, Chicago, IL) was used for the statistical analyses. Descriptive statistics were expressed as frequencies and percentages for categorical variables, as mean and standard deviation for normally distributed continuous variables, and as median with interquartile range for non-normally distributed data. Analytical statistics included the Chi-square (χ2) test to assess associations between categorical variables, with Fisher’s exact test used when more than 25% of cells had expected counts < 5. The independent-samples T-test was applied to compare means between two normally distributed groups, and one-way ANOVA was used for comparisons among more than two independent groups with normal distributions. Pearson’s correlation coefficient was used to evaluate linear relationships between normally distributed continuous variables. A p-value < 0.05 was considered statistically significant.
Ethics approval
Approval was obtained from the ethics committee of Hue University of Medicine and Pharmacy (Date: 08 June 2022 / No: H2022/194). All procedures were performed in accordance with relevant guidelines and regulations, including the Declaration of Helsinki. Informed consent was obtained from all individual participants included in the study.
Result
Applying 3D printing models for classifying fractures according to the Three-Column classification and planning surgery, we obtained the following results:
Two-column fractures accounted for the highest proportion at 45.5%. Isolated posterior column fractures constituted 9.1%. (Table 1)
As shown in Table 2, The average 3D printing time is 7.1 ± 0.9 h. The average 3D printing time for patients with complex fractures (Schatzker IV, V, VI) is 7.5 ± 0.8 h, which is more than approximately 1 h longer than the average 3D printing time for the group of patients with simple fractures. The difference in 3D printing time between the two groups, simple and complex fractures, is statistically significant (p = 0.001, T-test). The complex fracture provided more information to the surgical team than simple fractures.
The satisfaction level regarding the use of 3D printed models for preoperative explanations by doctors to patients was assessed based on the Yiting Lou 2017 questionnaire8, which utilizes a 10-point scale (see Appendix 2). The results indicated an average score of 7.4 ± 0.7. There was no significant difference in satisfaction between the working-age group and the elderly group (p = 0.45, T-test).

The correlation between the articular step-off and GAP with the surgical time (n = 33).
There is no statistically significant correlation between preoperative joint surface displacement and surgical time (with p-values of 0.3 and 0.2, respectively) (Fig. 4).
The aggregate material expenditure for 3D printing, which encompassed both PLA and ABS plastics across 33 individual models, amounted to approximately 33 USD. Consequently, the average cost per model was calculated to be 1 USD.
We assessed factors influencing postoperative malalignment of the tibial plateau, such as age group, dislocation, Three-Column classification, Schatzker classification, time of surgery, and preoperative articular step-off. The results showed that the group of patients with postoperative malalignment of the tibial plateau had a statistically significantly higher preoperative step-off, with p = 0.03 (T-test) (Table 3).
Evaluating functional outcomes based on the Rasmussen scores at 3 months and 6 months, we observed that patients with a higher number of fractured columns tended to have lower functional scores (p < 0.01) (Table 4).
The average surgical time was 115.8 ± 34.2 min. The infection rate was 3%, and the rate of secondary loss of reduction at six months was 25%, with no correlation with Rasmussen scores (P > 0.05, Fisher’s test).
Case
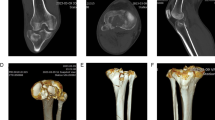
A 32-year-old male patient involved in a traffic accident presented with a tibial plateau fracture as revealed by X-ray and CT scan (Fig. 5). The fracture was classified as Schatzker VI, and all three columns fracture. A 3D printing technique was employed to create a 1:1 solid prototype of the fracture. Surgeons performed in vitro simulation of the surgery using the model as guidance. During the actual operation, the model aided in achieving satisfactory fracture reduction and fixation, with the plate and screws positioned correctly. An 8-month follow-up X-ray demonstrated a well-aligned tibial plateau with visible callus formation. The Rasmussen score at this point was 23, indicating a good outcome, and the patient did not experience any surgical complications during this period (Fig. 6).

X-ray and CT scan images before the surgery.

X-ray images at the 8-month follow-up, mTPA = 88.9°, PSA = 2.7°.
Discussion
The importance of accurate reduction and fixation in tibial plateau fractures is well recognized. Therefore, precise identification of tibial plateau fractures plays a pivotal role in the treatment process. Traditionally, physicians rely on two-dimensional images to confirm the fracture condition. However, the tibial plateau is a complex three-dimensional structure, and its anatomy is intricate. Reproducing the fracture accurately in planar images poses challenges, resulting in difficulties in diagnosis, classification, and surgical planning, especially for less experienced doctors.
Many studies have compared two groups and show results: Yiting Lou demonstrated that the group utilizing 3D printing models helped reduce surgical time, decrease blood loss, and lower the number of fluoroscopy during operation8. A systematic review and meta-analysis by Linzhen Xie illustrated that the 3D printing-assisted group exhibited a shorter operation time, less intraoperative blood loss, and faster union time for patients with tibial plateau fractures. Therefore, compared to conventional ORIF, ORIF assisted by 3D printing technology should be a more suitable treatment for tibial plateau fractures9.
We observed that complex fracture patterns are more beneficial for surgeons than simple fracture models. 3D printing models in cases of old fractures where there is existing callus formation also aid in planning the removal of the callus and reducing the fracture. Sheng Shen (2020) suggests that pre-operative simulation using a 3D printing model may be helpful for the treatment of old and complex tibial plateau fractures, contributing to pre-operative planning and ensuring accurate and personalized surgical procedures12. Wei-yong Wu show that using 3D printed models in combination with external fixation has more advantages for short-term treatment of complex tibial plateau fractures. It help external fixation to make up for the defect of not looking directly at the articular surface, improve the reduction quality of external fixation, and rationally plan the position of tibial half-pins6.
We have observed that the average 3D printing time using the Fused Deposition Modeling (FDM) method is 7.1 ± 0.9 h, so it should be considered not to print in cases requiring emergency surgery such as injuries to the neurovascular bundle, open fractures, or compartment syndromes. According to the study by Nicola Bizzotto, the printing time for a 3D model was approximately 4 h for distal radius fractures and 8 h for tibial plateau fractures13. In general, 3D printing of complex tibial plateau fracture models requires more time because additional supporting structures are needed, and both pre-printing and post-processing times are longer. It is necessary to estimate the printing time for each model to ensure that the 3D model can be completed before the scheduled surgery.
We had four cases that required emergency surgery but were still able to complete 3D model printing before the operation. All of these patients had already undergone CT scans at the referring hospitals, and their DICOM files were transferred to our center for 3D printing while they were being transported to the hospital. Cases that required emergency surgery but did not allow sufficient time for 3D model printing were excluded from the study. We recommend that in such situations, 3D printing should not be performed to avoid increasing the patient’s treatment costs.
The Three-Column classification has become a trend in current tibial plateau fracture management. Previously, this classification relied on CT scans and digital 3D reconstruction images. We perform the classification on 3D models as a supplementary method to CT scans to minimize errors in classification and surgery.
Based on our experience, we found that 3D-printed models help support and reduce classification errors compared with using conventional 2D imaging alone. This observation is consistent with the findings of Osma-Rueda et al., published in the Journal of the AAOS in 2023, which surveyed trauma surgeons and reported that the interobserver agreement for preoperative fracture classification using 3D-printed models (kappa = 0.81) was higher than that using conventional 2D CT images (kappa = 0.76). The 3D-printed models provide more comprehensive information than CT images and help reduce errors in measurement, classification, and preoperative surgical planning7.
On the other hand, the doctor-patient communication is also a key aspect of treatment. 3D printing model may become an innovative tool to improve the collaboration between doctors and patients, and improve the clinical outcome of the fractures. This finding was confirmed in the study by Yiting Lou, which compared groups with and without the use of 3D-printed models8. The mean patient satisfaction score in Yiting Lou’s study was 7.4 ± 0.7, whereas in our study, it was 7.3 ± 0.1.
Furthermore, we also utilize used 3D printed models for medical student education, providing learners with a visual and easily comprehensible insight into bone anatomy and the nature of fractures.
Our study has a small sample size and lacking comparison with a control group. Nevertheless, we performed an analysis of factors related to surgical outcomes. The average surgical time was 115.8 ± 34.2 min, consistent with other studies applying 3D models. Surgical time did not show a correlation with preoperative malalignment and gap width (p = 0.3 and 0.2). This can be attributed to various objective factors, including the benefits provided by the 3D model, aiding surgeons in better surgical planning. The 1:1 scale of the 3D model allows the surgical team to directly touch and feel the fracture lines, visually observe all angles of the tibial plateau, and prepare all necessary instruments with the assistance of the surgical scrub nurse based on the preoperative plan. All of these aspects may help improve operative time .
In our study, the consistency between the chosen fixation plates used before and after surgery indicates that the 3D printing model is a feasible imaging diagnostic method for surgical planning.
An analysis of the rate of loss of reduction (25%) identified several potential contributing factors, such as the fixation method, complexity of the fracture, and delayed rehabilitation among older patients. Additionally, it is noteworthy that none of the patients who experienced loss of reduction exhibited significant functional impairment at 6 months, as indicated by Rasmussen scores (p > 0.05).
Because of missing intraoperative data in some cases, blood loss and fluoroscopy counts were not always recorded. We will collect these metrics prospectively in future studies.
Regarding the cost of the 3D-printed model, we only calculated the cost of the printing material (plastic filament). The printers, software, and labor used in our study were provided free of charge by the laboratory of Hue University of Medicine and Pharmacy and the research team; therefore, we do not have an exact estimate of the total production cost of a 3D-printed model. The material cost was covered by the research team, and the patients in this study did not pay any fee for their 3D-printed models. According to the study by Nicola Bizzotto in 2016, the cost for each 3D-printed model ranges from 10 USD to 75 USD13.
Conclusion
Our study revealed that 3D printing models and the three-column concept effectively help surgeons plan accurate and personalized operative procedure, especially in complex cases. In addition, it may also enhance communication between surgeons and patients. Follow-up six months after surgery showed good knee function. However, its clinical effectiveness needs to be further assessed by a prospective randomized-controlled study.
Data availability
Data is provided within the manuscript or supplementary information files.
References
Rozell, J. C. et al. Tibial plateau fractures in elderly patients. Geriatric Orthop. Surg. Rehabilitation. 7 (3), 126–134 (2016).
Krause, M. et al. Intra-articular tibial plateau fracture characteristics according to the ten segment classification. Injury 47 (11), 2551–2557 (2016).
Wang, Y. et al. Updated three-column concept in surgical treatment for tibial plateau fractures–a prospective cohort study of 287 patients. Injury 47 (7), 1488–1496 (2016).
Luo, C-F. et al. Three-column fixation for complex tibial plateau fractures. J. Orthop. Trauma. 24 (11), 683–692 (2010).
Chepelev, L. et al. Radiological society of North America (RSNA) 3D printing special interest group (SIG): guidelines for medical 3D printing and appropriateness for clinical scenarios. 3D Print. Med. 4, 1–38 (2018).
Wu, W. et al. Preoperative plan with 3D printing in internal and external fixation for complex tibial plateau fractures. Orthop. Surg. 11 (4), 560–568 (2019).
Osma-Rueda, J., Mantilla-Angarita, F. & Lopez-Gualdron, C. Intraobserver and interobserver reproducibility of classifications of tibial plateau fractures and the surgical approaches chosen comparing 2D CT and 3D printing: reliability study. JAAOS Glob. Res. Rev. 7, 4 (2023).
Lou, Y. et al. Comparison of traditional surgery and surgery assisted by three dimensional printing technology in the treatment of tibial plateau fractures. Int. Orthop. 41 (9), 1875–1880 (2017).
Xie, L. et al. Three-dimensional printing assisted ORIF versus conventional ORIF for tibial plateau fractures: a systematic review and meta-analysis. Int. J. Surg. 57, 35–44 (2018).
Jiang, R. et al. A comparative study of less invasive stabilization system (LISS) fixation and two-incision double plating for the treatment of bicondylar tibial plateau fractures. Knee 15 (2), 139–143 (2008).
Shimizu, T. et al. Geriatric tibial plateau fractures: clinical features and surgical outcomes. J. Orthop. Sci. 21 (1), 68–73 (2016).
Shen, S. et al. Pre-operative simulation using a three-dimensional printing model for surgical treatment of old and complex tibial plateau fractures. Sci. Rep. 10 (1), 6044 (2020).
Bizzotto, N. et al. 3D printed replica of articular fractures for surgical planning and patient consent: a two years multi-centric experience. 3D Print. Med. 2 (1), 2 (2016).
Acknowledgements
This research was funded by Hue University through the Core Research Program (Grant No. NCM.DHH.2022.03), covering research expenses and publication fees.
Author information
Authors and Affiliations
Contributions
Dung Huu Tran and Nghi Thanh Nhan Le contributed to the conception and design of the study. Dung Huu Tran and Quoc Sang Nguyen performed the surgeries and data collection. Sang Quoc Nguyen was responsible for 3D modeling and printing of the tibial plateau before surgery, as well as data analysis and preparation of figures and tables. Dung Huu Tran wrote the main manuscript text. Nhan Nghi Thanh Le edited and critically revised the manuscript. All authors reviewed and approved the final version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Tran, H.D., Nguyen, Q.S. & Le, N.T.N. 3D printing and three column concept in surgical treatment of tibial plateau fracture. Sci Rep 16, 975 (2026). https://doi.org/10.1038/s41598-025-30475-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-30475-7
