
Abstract
Esophageal cancer patients often face various challenges in the perioperative period, and unplanned tracheal intubation is a serious complication that can significantly impact patient outcomes. Therefore, this study aimed to identify the risk factors for reintubation in esophageal cancer patients after surgery. A retrospective study was carried out on esophageal cancer patients who underwent surgery at Zhejiang Cancer Hospital in 2019. Data on patient demographics, surgical details, and anesthesia techniques were collected. We employed logistic regression analysis to explore the factors associated with the occurrence of unplanned tracheal intubation. The study encompassed a total of 463 patients. 7.8% (36/463) of the enrolled patients encountered unplanned reintubation during the postoperative phase. Notably, respiratory failure (9/49, 18.4%) and pulmonary infection (8/49, 16.3%) emerged as the primary drivers prompting patients to undergo reintubation in the postoperative period. The results of multivariable logistic analysis indicated that analgesic technique was the independent risk factor for reintubation and compared with general anesthesia (GA) combined with epidural anesthesia, GA combined with nerve block was significantly associated with reintubation. This study analyzed the incidence of unplanned tracheal intubation in esophageal cancer patients after surgery and determined the key independent risk factors.
Similar content being viewed by others

Introduction
Esophageal cancer, a common digestive tract malignancy worldwide, has a relatively high incidence and ranks seventh among the leading causes of cancer - related deaths1. Currently, although radiotherapy and chemotherapy have made rapid progress, surgery still plays a crucial part in the comprehensive treatment of esophageal cancer2,3. However, due to complex procedures involved in esophageal surgery, such as alterations to the intrathoracic environment, a series of severe complications often follow after the operation, posing a huge challenge to patients’ recovery4,5. Therefore, it is of utmost importance to meticulously manage the perioperative process to help patients avoid complications following esophageal surgery.
Reintubation, a severe postoperative complication6,7, refers to intubation after extubation of a patient initially tracheally intubated under general anesthesia or in combination with other analgesic techniques8. Numerous factors are related to postoperative reintubation, including the patient’s preoperative physical condition, surgical procedures, and perioperative anesthesia management. In clinical practice, when the topic of reintubation arises, it is often linked to serious respiratory disorders, such as acute hypoxemia, hypercapnia, respiratory failure and airway obstruction9,10,11. There is a strikingly correlation between reintubations and higher mortality rates, longer hospital stays, and greater costs12,13. These significant negative impacts highlight the importance of understanding this complication. However, despite its vital effect, the risk factors for reintubation after esophageal cancer surgery have not been fully elucidated. Since the esophageal cancer surgery can cause fluctuations in the intrathoracic environment, the occurrence probability of lung complications is relatively high14. It is predictable that the number of patients in need of second-time endotracheal intubation after esophageal cancer surgery will also rise.
At present, research findings have revealed that postoperative pulmonary complications after esophageal surgery are closely linked to senior age, preoperative lung function disorder, low albumin levels, perioperative blood transfusion and prolonged hospitalization15. Moreover, the surgical factors such as the duration of surgery, surgical technique, and the extent of lymph node dissection are also correlated16,17,18. It provides important references for subsequent studies, but the specific links between these factors and reintubation have not been thoroughly explored.
This study deeply explores the occurrence mechanisms of reintubation after esophageal cancer surgery to help surgeons and anesthesiologists conduct more accurate preoperative risk assessments. Based on these assessments, they can develop personalized prevention plans, optimize surgical and anesthesia management during the operation, and strengthen postoperative patient monitoring and care. By promptly identifying and addressing reintubation risk factors, we can reduce reintubation, improve patient prognosis, and minimize medical resource waste.
In this real-word research, we analyzed the reasons that patients accepted reintubation after esophageal cancer surgery and determined the risk factors associated with reintubation.
Methods
Study population
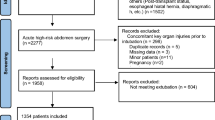
A total of 463 patients were enrolled in our research. Our research was approved by the Clinical Research Ethic Committee of Zhejiang Cancer Hospital. All the patients were diagnosed as esophageal cancer pathologically and accepted surgical treatment in Zhejiang Cancer Hospital in 2019. We designated 2019 as the time period for case recruitment in this study. This choice was grounded in the substantial increase in the number of esophageal cancer surgeries carried out in 2019, thereby affording an ample case volume to support comprehensive research. Moreover, during the subsequent period, the thoracic department underwent significant personnel turnover. Ultimately, we determined the timepoint to ensure the standardization and consistency of data collection. The cohort was actively followed up, and there were detailed records of their preoperative examinations, surgical procedures, and the postoperative nursing processes. The general demographic characteristics are displayed in Table 1, including gender, age, smoking history, history of hypertension, and preoperative lung function. Additionally, we collected the therapeutic regimes, covering preoperative chemotherapy, preoperative radiotherapy, surgical approaches, surgical technique and analgesic technique. Tumor staging is no exception.
The exclusion criteria for patients in this study are as follows: patients with severe preoperative respiratory function impairment, such as those with respiratory failure or active pulmonary tuberculosis within 1 month before surgery; patients who experienced severe intraoperative complications (e.g., massive hemorrhage, cardiac arrest, severe anesthetic accidents), as well as those who died within 24 h after surgery or discharged voluntarily leading to missing follow-up data; patients with severe missing follow-up information; patients with comorbid severe mental illness who were unable to cooperate with postoperative management.
Concrete procedures
As part of the clinical weaning protocol, patients were screened after surgery to assess their readiness for ventilator withdrawal. Eligibility for weaning was determined based on three core sets of criteria19: First, resolution of the underlying illness that initially required mechanical ventilation—a fundamental prerequisite to ensure the precipitating cause of respiratory failure no longer necessitated ventilatory support. Second, stable respiratory parameters, specifically a ratio of arterial oxygen partial pressure to fraction of inspired oxygen (PaO₂: FIO₂) greater than 150 mmHg (with FIO₂ ≤0.4) and a positive end-expiratory pressure (PEEP) setting below 8 cmH₂O, indicating adequate oxygenation with minimal ventilator assistance. Third, stable clinical status, which included: no electrocardiographic evidence of myocardial ischemia; no requirement for vasoactive medication; a heart rate below 140 beats per minute; presence of a spontaneous respiratory drive (respiratory stimulus); and an effective spontaneous cough reflex.
In line with previous research8, we defined reintubation as the need for patients to undergo endotracheal intubation again after meeting the standard criteria of extubation, either in the post-anesthetic care unit (PACU) or on the inpatient ward. In the cohort, the analgesic technique we chose was general anesthesia with diverse kinds of nerve block, such as epidural anesthesia, intercostal nerve block (INB), transversus abdominis plane block (TAP) and paravertebral nerve block. Analgesia was individualized based on the surgical approach, procedural feasibility, patient-specific factors, and patient preferences for pain management.
Statistical analysis
All the analysis in our study was performed with the software R version 4.4.1 (https://www.r-project.org/) and R Studio version 2024 (https://www.rstudio.com/). And the figures were generated by Graphpad prism version 9.5 (https://www.graphpad.com/). The differences of all variables between the two groups in Table 1 were reflected by the p-values. Inverse probability weighting (IPTW) was employed to balance the disparities between groups. The chi-square test was used for categorical variables, and the t-test was applied to continuous variables that did not follow a normal distribution. The median accompanied by the interquartile range (IQR) was used to present continuous variables. Additionally, utilizing the R package “autoreg”, we conducted univariate logistic regression analysis on all relevant variables and subsequently, variables with a p-value greater than 0.05 were screened out for multivariable analysis. The odds ratios (ORs) having 95% confidence intervals (CIs) of all the research factors were contrasted. Thereafter, we conducted collinearity diagnosis for all independent variables. After excluding some independent variables with high collinearity overlap, we reconstructed the logistic regression model and performed univariable and multivariable analyses on the remaining variables. Based on the analysis of risk factors for reintubation, we constructed a nomogram and calculated the cut-off value of the risk score.
Results
Patient characteristics
This study aimed to explore the potential factors related to reintubation in a cohort of 463 patients. Table 1 shows the analysis and comparison of the baseline characteristics between patients with reintubation (N = 36) and those without (N = 427). In terms of demographic characteristics, gender and age did not show significant differences between the two groups (p = .243; p = .251). Smoking history did not show a significant association with reintubation (p = .107), despite a slightly higher proportion of smokers in the reintubation group. Similarly, most of the tumor staging variables (T staging and N staging) did not show a significant relationship with reintubation (p = .078; p = .355). However, M staging (indicating distant metastasis status) was significantly associated with reintubation (p = .017). Patients with Mx or M1 staging (indicating unknown metastasis status or distant metastasis) had a higher proportion of reintubation compared to those with M0 staging (no distant metastasis). All tumor staging of esophageal cancer patients in our study was performed in accordance with the AJCC 8th Edition Esophageal Cancer Staging20. Moreover, analgesic technique was significantly related to reintubation (p = .003). In our study, we collected the cases following two analgesic techniques which includes GA combined with epidural anesthesia or other nerve block. The proportion of patients who experienced reintubation was much higher among those with GA combined with other nerve block (69.4%) than among those with GA combined with epidural anesthesia (30.6%). Interestingly, the rate of reintubation was significantly higher among patients whose catheters were removed immediately after surgery (72.2%) compared to those whose catheters were not removed immediately (27.8%). For those patients who were not extubated immediately in the operating room after the operation, the extubation was carried out in the PACU, which was specifically determined according to the condition of each patient. To achieve inter-group balance, we conducted IPTW; however, the resulting balancing effect did not meet our desired standard (Supplement Table 1).
The reason analysis of reintubation
This study thoroughly explored the causes of reintubation in 36 patients, and the pertinent details are presented in Table 2. Based on our statistical analysis, a considerable number of patients required reintubation for more than one reason. Thus, the final outcome presented in Table 2 summarizes the total frequency of 49 cases across different causes of reintubation. Respiratory-related problems were the primary drivers of reintubation, constituting 91.8% (45/49) of the cases. Specifically, respiratory failure was a prevalent cause, resulting in reintubation in 18.4% (9/49) of the patients. Among these cases, 3 patients developed respiratory failure due to isolated pulmonary complications. The secondary causes of respiratory failure included anastomotic leakage (2/9, 22.2%), aspiration (2/9, 22.2%), and recurrent laryngeal nerve injury (2/9, 22.2%). Pulmonary infection also emerged as a significant factor, with 16.3% (8/49) of the patients requiring reintubation because of it. This category encompassed diverse forms of pneumonia, such as inhalational pneumonia, which accounted for 4.1% (2/49) of the cases, interstitial pneumonia at 2.0% (1/49), and severe pneumonia at 6.1% (3/49). Other respiratory-related causes included low oxygen saturation and carbon dioxide retention, each contributing 10.2% (5/49) of the cases. Excessive sputum and laryngeal spasm each accounted for 8.2% (4/49) of the cases. Labored breathing and pulmonary edema accounted for 6.1% (3/49) and 2.0% (1/49) of the cases, respectively. In contrast, non-respiratory reasons for reintubation were less frequent, comprising 8.2% (4/49) of all cases.
The logistic analysis of risk factors for reintubation
We utilized univariable and multivariable logistic regression analyses to pinpoint the risk factors for reintubation in Supplement Table 2. During the univariable analysis, several variables exhibited trends that were close to attaining significance yet failed to reach the standard 0.05 threshold of statistical significance. Subsequently, we conducted collinearity diagnosis for all independent variables and excluded some independent variables with high collinearity overlap (Table 3). After accounting for confounding factors, we incorporated T staging, analgesic technique, and the timing of postoperative catheter removal into the multivariable analysis. The relationships between T staging and reintubation remained notably significant. In comparison to the T0-1 stage, T2-4 stage was not a significant factor (OR = 1.12, 95%CI: 0.50–2.53, p = .781), but Tx was a significant factor (OR = 10.48, 95%CI: 1.44–76.47, p = .020). Moreover, when contrasted with patients who underwent GA in combination with epidural anesthesia, those who received GA combined with nerve block (intercostal nerve block, transverse abdominis plane block, and paravertebral nerve block) had an odds ratio of 2.92 (95% CI: 1.38–6.18, p = .005), thereby validating a strong association between this analgesic technique and reintubation.
The timepoints of the second intubation and extubation
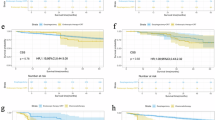
Further, in Figs. 1 and 2, we analyzed the patients who underwent reintubation, including the time of the second intubation and the time of extubation after the second intubation. Considering the limitations of the number of included patients, we merely counted the cases where the frequency of the same reintubation cause was greater than or equal to 3. The second intubation due to pulmonary infection occurred 48–96 h after the first extubation. Laryngeal spasm and carbon dioxide retention, the severe postoperative perioperative complications, mostly occurred in the early postoperative period. The second intubation caused by respiratory failure had a relatively large time span. Patients who underwent second endotracheal intubation due to respiratory failure and pulmonary infection had a relatively long time for the second extubation, with an average of 522 and 546 h respectively. In contrast, for patients with carbon dioxide retention and laryngeal spasm, the average time for the second extubation was approximately 16 h and 78 h, respectively.

The timepoint of second intubation. This box plot displays the distribution of the time from operation until reintubation for each specific reason.

The timepoint of catheter removal of second intubation. This box plot presents the distribution of the time from operation until the removal of the reintubation tube for each cause.
Nomogram predicting risk factors of reintubation
Figure 3 presents the nomogram developed to quantify individual esophageal cancer patients’ risk of unplanned tracheal intubation, including its scoring system and risk conversion scale. The nomogram incorporates three core predictors with specific point assignments: for T staging, T0-1 scores 0 points, T2-4 scores 5 points, and Tx scores 100 points; for analgesic technique, GA combined with epidural anesthesia scores 0 points, while GA combined with other nerve blocks scores 46 points; for postoperative catheter removal time, extubation immediately after operation scores 0 points, while extubation in PACU based on individual conditions scores 51 points. It allows clinicians to calculate a patient’s total score by summing the points of each predictor and then determine the associated reintubation risk via the integrated risk conversion scale. To further stratify patients, we calculated the optimal cutoff value for the risk score across the entire cohort, which was determined to be 48.5 points. Based on this cutoff, patients were divided into two groups: 188 patients were classified as the High-risk group (risk score ≥ 48.5), and 275 patients were categorized as the Low-risk group (risk score < 48.5). This stratification enables a more nuanced assessment of unplanned tracheal intubation risk and supports tailored perioperative management strategies.

Construct a nomogram based on the risk factors and calculate the risk score. (A) Scoring rubric of nomogram. (B) Nomogram predicts the reintubation.
Discussion
By conducting the retrospective analysis of the clinical data of 463 esophageal cancer patients who underwent surgery at Zhejiang Cancer Hospital in 2019, and applying methods including the chi-square test, t-test, as well as univariable and multivariable logistic regression analyses, this study made a meticulous exploration of the risk factors for reintubation following esophageal cancer surgery. The study found that 7.8% of the patients experienced unplanned reintubation after surgery. Respiratory system-related problems were the predominant cause of reintubation, constituting 91.8% of the total cases. Among these, respiratory failure and pulmonary infection emerged as the most prominent factors. This is consistent with the findings of previous studies21,22. Multivariable logistic analysis showed that the analgesic technique was an independent risk factor for reintubation. Compared with GA combined with epidural anesthesia, GA combined with other nerve block was significantly associated with reintubation. This study has clarified the incidence of reintubation after esophageal cancer surgery and the key risk factors, offering valuable reference to surgeons and anesthesiologists. Consequently, it’s capable of reducing the rate of reintubation and improving the prognosis of patients by the accurate prediction of high-risk factors and subsequent optimization of anesthesia protocols represent key strategies.
The probability of reintubation after surgery varies depending on the surgical site23,24,25. The reasons for reintubation are mostly respiratory problems9,11. There have been few previous studies reporting the incidence of reintubation after esophageal cancer surgery. By means of this study, we determined the incidence of the reintubation of postoperative esophageal cancer patients and analyzed the risk factors. In our study, the analgesic technique is an important independent risk factor for reintubation. The reintubation rate of patients who received GA combined with other nerve block was significantly higher than that of patients who received general anesthesia combined with epidural anesthesia. As is commonly believed, nerve block and epidural anesthesia can both reduce respiratory complications and lower the incidence of unplanned tracheal intubation in different degree26. The nerve block involved in our study including intercostal nerve block (INB), transversus abdominis plane block (TAP) and paravertebral nerve block, still carries the potential of causing respiratory system-related complications. If INB affects the intercostal muscles innervated by the T1-T12 nerves, it may weaken the chest wall movement. Especially in the case of bilateral block or high-level block, it may aggravate the restrictive ventilation disorder. Equally, epidural block also stands a chance to affect the breathing muscles accidently which might give rise to the pulmonary atelectasis following surgery26. When low-concentration local anesthetics (such as 0.25%-0.375% ropivacaine) are used, it only blocks sensory nerves and sympathetic nerves, with minimal impact on motor nerves that innervate respiratory muscles. This ensures that the contraction function of intercostal muscles and diaphragms remains basically normal, and the reduction in lung ventilation volume (MV) and minute ventilation volume (VE) can be controlled within an acceptable range, thus effectively protecting respiratory function. In contrast, other nerve blocks have obvious limitations in protecting respiratory function: INB directly blocks the sensory and motor fibers of intercostal nerves. TAP mainly acts on the anterior abdominal wall nerves, and its analgesic range is limited. Since postoperative pain after esophageal cancer is mainly in the chest and back, TAP cannot provide sufficient analgesia. Patients may be afraid to take deep breaths and cough effectively due to pain, leading to sputum retention, which increases the risk of pulmonary infection and respiratory failure. Although paravertebral nerve block can achieve a relatively definite blocking effect on thoracic pain, its clinical application remains relatively limited. Besides, epidural block effectively reduces the intraoperative stress response, improves visceral blood flow by blocking the sympathetic nerve chain and lowers the use of postoperative opioid medications27. On one hand, this improves pulmonary perfusion and prevents ventilation/perfusion (V/Q) ratio imbalance; on the other hand, it inhibits the release of inflammatory factors such as IL-6 and TNF-α, alleviates pulmonary interstitial edema and alveolar epithelial injury, and thereby indirectly reduces the risk of pulmonary infection. We can reasonably infer that general anesthesia combined with thoracic epidural anesthesia (TEA) significantly reduces the risk of reintubation after esophageal cancer surgery by virtue of its precise protection of respiratory function, effective inhibition of stress response, optimized pain control, and low risk of procedural complications. In contrast, general anesthesia combined with other nerve blocks constitutes an independent risk factor for reintubation due to respiratory function impairment, insufficient stress regulation, analgesic deficiencies, and the risk of procedural complications.
Currently, the analgesia concept of enhanced recovery after surgery (ERAS) advocates multimodal analgesia combined with local anesthetic techniques in clinical practice. This approach can reduce the use of opioids and avoid related side effects5,28. And in the multimodal analgesia for esophageal cancer surgery, thoracic epidural anesthesia, which is regarded as one of the optimal analgesic methods for thoracoabdominal surgeries and should be considered as a first-line option for postoperative analgesia, can minimize the risk of motor block while providing good analgesic effects. However, the exact mechanisms regarding the impact of two analgesic techniques on reintubation after esophageal cancer surgery remain unclear and further research is needed.
As an indicator significantly associated with clinicopathological outcomes, T stage also showed a clear association with the risk of postoperative reintubation in this study, and this association was verified by multivariable logistic regression analysis (Table 3). stage, which is significantly associated with clinical pathological outcomes, also shows a strong correlation with reintubation. Specifically, the risk of reintubation showed significant stratified differences among subgroups with different T stages: Taking T0-T1 stage as the reference group, patients with Tx stage (unknown primary tumor stage) had a significantly increased risk of reintubation, with an adjusted OR of 10.48 (95% CI: 1.44–76.47, p = .020). This suggests that patients with unknown T stage may have insufficient preoperative disease assessment, leading to imprecise surgical plan formulation and thus an increased risk of postoperative reintubation. However, there was no statistically significant difference in the risk of reintubation between patients with T2-T4 stage and those with T0-T1 stage (OR = 1.12, 95% CI: 0.50–2.53, p = .781), and this result is slightly different from our initial hypothesis. It is hypothesized that this may be related to the more detailed preoperative assessment and greater emphasis on protecting respiratory function during surgery for patients with T2-T4 stage disease, which thus offsets the potential increase in reintubation risk that would otherwise be associated with tumor progression. Further analysis of the univariate analysis results shows that patients with Tx stage already exhibited an increasing trend in reintubation risk in the univariate analysis (OR = 8.81, 95% CI: 1.30-59.72, p = .026), and this trend remained statistically significant after multivariate adjustment. This indicates that unknown T stage is an independent risk factor for reintubation, separate from analgesic methods and postoperative extubation timing. This finding also receives indirect support from previous studies, Tanigawa’s research has proven that patients with T3/T4 esophageal cancer have an increased risk of postoperative pulmonary infection and respiratory failure due to the extensive surgical scope29. Unknown T stage may lead to insufficient or excessive surgical resection range. The former may increase the risk of postoperative infection due to residual tumor, while the latter may exacerbate respiratory function damage due to excessive surgical trauma. Both scenarios may indirectly increase the risk of reintubation by inducing complications such as pulmonary infection and respiratory failure. Although the specific mechanism leading to reintubation is not clear, we can reasonably speculate that the T stage is an important risk factor for reintubation. This suggests that in clinical practice, emphasis should be placed on the completeness of preoperative T stage assessment. Through accurate staging, surgical plans and perioperative management can be optimized, thereby reducing the risk of reintubation.
Previous studies30,31,32 have shown that the core triggering factor for unplanned reintubation is the patient’ inability to maintain respiratory function, which is consistent with the findings of our study. Its pathophysiological mechanisms focus on disorders of pulmonary ventilation or gas exchange, respiratory muscle abnormalities, and impaired airway secretion clearance, among others, and are influenced by patients’ underlying diseases. Regrettably, as this study did not focus on the pathophysiological changes in patients, it was unable to further explore the specific mechanisms underlying unplanned reintubation in patients after radical esophagectomy.
In our research, the timepoints of reintubation and extubation after reintubation provide valuable insights. For example, reintubation related to pulmonary infection occurs 48 to 96 h after the first extubation. This may be on account of the incubation period of the infection and the time required for the symptoms to become severe enough to necessitate reintubation. The former research findings revealed that in the infection group, the serum inflammatory markers (such as IL-6 and TNF-\(\:\alpha\:\)) and white blood cell count were significantly elevated seven days after surgery. Meanwhile, the pulmonary function indices declined33. However, the timepoints recognized in our study are earlier. This may be attributed to the differences in the age of the patient groups under consideration and their preoperative pulmonary function. Besides, the time span of reintubation related to respiratory failure is quite large, which indicates that it may be caused by diverse causes. Here are some of the contributing factors: postoperative anastomotic leakage, the effect of anesthesia, compromised preoperative lung function, and a smoking history34,35,36,37. Undoubtably, comprehensively mastering the hazard elements of pulmonary failure and making a preoperative preparation will make sense.
IPTW was applied to balance baseline characteristics between the two groups (unplanned tracheal intubation vs. non-intubation). Yet, the outcome did not meet expectations, with the SMD of certain key variables (analgesia technique) failing to reach the desired balance after weighting. While IPTW can regulate observable confounding variables, our study likely includes unaccounted potential confounders that have further undermined the effectiveness of weighting. Furthermore, the choice of analgesic approaches is not entirely random; their distribution is linked to various preoperative factors in patients that are not fully quantifiable. This form of allocation bias, derived from clinical decision-making, exceeds what IPTW can adjust for.
Notably, this study still has some limitations. Initially, as a retrospective study, it may be subject to inherent selection bias. The data were sourced from a single center, namely Zhejiang Cancer Hospital, which may limit the generalizability of the research findings. Secondly, despite our adjustment for multiple factors in the multivariable analysis, there might still exist unmeasured confounding variables. These might encompass, for instance, the experience level of anesthesiologists and the degree of proficiency in performing analgesic procedures. Moreover, the number of cases included in our research was restricted, thereby reducing the persuasiveness of our findings. Additionally, we failed to categorize the methods of nerve block in detail, resulting in only a general comparison of the differences between epidural block and other nerve blocks. Lastly, due to limitations in the study design, this study was unable to incorporate the Numerical Rating Scale (NRS) score or other objective indicators for evaluating postoperative pain in patients. Future research will further investigate the association between postoperative pain and reintubation when opportunities arise.
In a word, our study has identified analgesic techniques and T stage as important risk factors for reintubation after esophageal cancer surgery. Prospective, multi-center investigations are required in the forthcoming period to validate these findings and explore the underlying mechanisms, aiming to formulate more efficacious preventive strategies.
Conclusions
This study investigated the incidence of reintubation in postoperative esophageal cancer patients and pinpointed the crucial independent risk factors. Respiratory-related problems were identified as the primary cause of reintubation, with respiratory failure and pulmonary infection being the most prominent factors. And analgesic technique was an important independent risk factor. The reintubation rate was significantly higher in patients who received general anesthesia combined with nerve block compared to those with general anesthesia combined with epidural anesthesia.
Data availability
Any researchers interested in this study could contact corresponding author for requiring data.
Abbreviations
- GA:
-
General anesthesia
- OR:
-
The odds ratio
- CI:
-
Confidence interval
- IQR:
-
The interquartile range
- PACU:
-
Post-anesthetic care unit
- INB:
-
Intercostal nerve block
- TAP:
-
Transversus abdominis plane block
- MV:
-
Ventilation volume
- VE:
-
Minute ventilation volume
- V/Q:
-
Ventilation/perfusion
- TEA:
-
Thoracic epidural anesthesia
- ERAS:
-
Enhanced recovery after surgery
- IPTW:
-
Inverse probability weighting
References
Yang, H., Wang, F., Hallemeier, C. L., Lerut, T. & Fu, J. Oesophageal cancer. Lancet (London England). 404(10466), 1991–2005 (2024).
Xue, M. et al. Robotic assisted minimally invasive esophagectomy versus minimally invasive esophagectomy. Front. Oncol. 13, 1293645 (2023).
Wu, L-L. et al. Postoperative survival effect of the number of examined lymph nodes on esophageal squamous cell carcinoma with pathological stage T1–3N0M0. BMC Cancer 22(1). (2022).
Rutegård, M., Lagergren, P., Rouvelas, I. & Lagergren, J. Intrathoracic anastomotic leakage and mortality after esophageal cancer resection: a population-based study. Ann. Surg. Oncol. 19(1), 99–103 (2012).
Zhang, S. W. et al. Effect of the active cycle of breathing technique on perioperative outcome in individuals with esophagectomy: A Quasi-experimental study. Front. Surg. 8, 735947 (2021).
Caplan, R. A., Posner, K. L., Ward, R. J. & Cheney, F. W. Adverse respiratory events in anesthesia: a closed claims analysis. Anesthesiology 72(5), 828–833 (1990).
Fasting, S. & Gisvold, S. E. Serious intraoperative problems–a five-year review of 83,844 anesthetics. Can. J. Anaesth. = J. Canadien D’anesthesie. 49(6), 545–553 (2002).
Rujirojindakul, P. et al. Risk factors for reintubation in the post-anaesthetic care unit: a case-control study. Br. J. Anaesth. 109(4), 636–642 (2012).
Kindgen-Milles, D., Buhl, R., Gabriel, A., Böhner, H. & Müller, E. Nasal continuous positive airway pressure: A method to avoid endotracheal reintubation in postoperative high-risk patients with severe nonhypercapnic oxygenation failure. Chest 117(4), 1106–1111 (2000).
Qian, J. Y. et al. A clinical risk model for assessing the survival of patients with stage IA-IIA non-small cell lung cancer after surgery. J. Thorac. Disease. 14(11), 4285–4296 (2022).
Brown, K. A. et al. Urgent adenotonsillectomy: an analysis of risk factors associated with postoperative respiratory morbidity. Anesthesiology 99(3), 586–595 (2003).
Tillquist, M. N., Gabriel, R. A., Dutton, R. P. & Urman, R. D. Incidence and risk factors for early postoperative reintubations. J. Clin. Anesth. 31, 80–89 (2016).
Rudolph, M. I. et al. Association of reintubation and hospital costs and its modification by postoperative surveillance: A multicenter retrospective cohort study. J. Clin. Anesth. 91, 111264 (2023).
Mariette, C. et al. Hybrid minimally invasive esophagectomy for esophageal cancer. N. Engl. J. Med. 380(2), 152–162 (2019).
Li, S., Su, J., Sui, Q. & Wang, G. A nomogram for predicting postoperative pulmonary infection in esophageal cancer patients. BMC Pulm. Med. 21(1), 283 (2021).
Qiu, M. L. et al. Current state of esophageal cancer surgery in china: a national database analysis. BMC Cancer. 19(1), 1064 (2019).
Szakó, L. et al. Network meta-analysis of randomized controlled trials on esophagectomies in esophageal cancer: the superiority of minimally invasive surgery. World J. Gastroenterol. 28(30), 4201–4210 (2022).
Law, S., Wong, K. H., Kwok, K. F., Chu, K. M. & Wong, J. Predictive factors for postoperative pulmonary complications and mortality after esophagectomy for cancer. Ann. Surg. 240(5), 791–800 (2004).
Boles, J. M. et al. Weaning from mechanical ventilation. Eur. Respir. J. 29(5), 1033–1056 (2007).
Rice, T. W. et al. Cancer of the esophagus and esophagogastric junction-major changes in the American Joint Committee on Cancer eighth edition cancer staging manual. Cancer J. Clin. 67(4), 304–317 (2017).
Schussler, O. et al. Postoperative pneumonia after major lung resection. Am. J. Respir. Crit Care Med. 173(10), 1161–1169 (2006).
Masaki, H. et al. Risk markers for postoperative reintubation of intensive care unit patients: A retrospective multicentre study of the National Intensive Care Registry. Intensive Crit. Care Nurs. 87, 103956 (2025).
Wang, F. et al. Effect of nasal high-flow oxygen humidification on patients after cardiac surgery. Heliyon 9(11), e20884 (2023).
He, Q. et al. Postoperative pulmonary complications after major abdominal surgery in elderly patients and its association with patient-controlled analgesia. BMC Geriatr. 24(1), 751 (2024).
Schmutz, A. et al. Protocol based evaluation for feasibility of extubation compared to clinical scoring systems after major oral cancer surgery safely reduces the need for tracheostomy: a retrospective cohort study. BMC Anesthesiol. 18(1), 43 (2018).
Rodgers, A. et al. Reduction of postoperative mortality and morbidity with epidural or spinal anaesthesia: results from overview of randomised trials. BMJ (Clinical Res. ed). 321(7275), 1493 (2000).
Kingma, B. F., Visser, E., Marsman, M., Ruurda, J. P. & van Hillegersberg, R. Epidural analgesia after minimally invasive esophagectomy: efficacy and complication profile. Diseases Esophagus: Official J. Int. Soc. Dis. Esophagus 32(8). (2019).
Low, D. E. et al. Guidelines for perioperative care in esophagectomy: enhanced recovery after surgery (ERAS(®)) society recommendations. World J. Surg. 43(2), 299–330 (2019).
Tanigawa, Y., Nakamura, K., Yamashita, T., Nakagawachi, A. & Sakaguchi, Y. Changes in respiratory mechanics of artificial pneumothorax two-lung ventilation in video-assisted thoracoscopic esophagectomy in prone position. Sci. Rep. 11(1), 6978 (2021).
De Jong, A. et al. Effect of non-invasive ventilation after extubation in critically ill patients with obesity in france: a multicentre, unblinded, pragmatic randomised clinical trial. Lancet Respiratory Med. 11(6), 530–539 (2023).
Tan, D. et al. High-flow nasal cannula oxygen therapy versus non-invasive ventilation for chronic obstructive pulmonary disease patients after extubation: a multicenter, randomized controlled trial. Crit. Care. (London, England). 24(1), 489 (2020).
Jaber, S. et al. Noninvasive ventilation on reintubation in patients with obesity and hypoxemic respiratory failure following abdominal surgery: a post hoc analysis of a randomized clinical trial. Intensive Care Med. 50(8), 1265–1274 (2024).
Wang, W., Yang, T., Xie, J. & Huang, S. Impact of pulmonary infection after radical esophagectomy on serum inflammatory markers, pulmonary function indices, and prognosis. Saudi Med. J. 45(1), 40–45 (2024).
Uchihara, T. et al. Risk factors for pulmonary morbidities after minimally invasive esophagectomy for esophageal cancer. Surg. Endosc. 32(6), 2852–2858 (2018).
Kuwano, H. et al. Relationship between preoperative assessment of organ function and postoperative morbidity in patients with oesophageal cancer. Eur. J. Surg. = Acta Chir. 164(8), 581–586 (1998).
Verstegen, M. H. P. et al. Outcomes of patients with anastomotic leakage after Transhiatal, McKeown or Ivor Lewis esophagectomy: A nationwide cohort study. World J. Surg. 45(11), 3341–3349 (2021).
Veelo, D. P. & Geerts, B. F. Anaesthesia during oesophagectomy. J. Thorac. Disease. 9(Suppl 8), S705–s712 (2017).
Funding
This work was supported by Zhejiang Provincial Medical Health Science and Technology Project (No. 2021KY103, and No. 2024KY845). The design of the study, the collection, analysis, and interpretation of data, and the writing of the manuscript were not influenced by the funding bodies in any way.
Author information
Authors and Affiliations
Contributions
Shunv Cai: Methodology, Validation, Investigation, Writing - Original Draft. Xinyi Liu : Writing - Review & Editing, Supervision. Yimin Wu: Methodology, Validation, Investigation, Writing - Original Draft. Junbo Yuan: Formal analysis, Writing - Review & Editing. Yun Cheng: Formal analysis, Writing - Review & Editing. Weikang Zhang: Formal analysis, Writing - Review & Editing. Zewu Ding: Formal analysis, Writing - Review & Editing. Man Fang: Formal analysis, Writing - Review & Review & Editing.
Corresponding authors
Ethics declarations
Consent for publication
All the authors had consented to the publication in Scientific Reports.
Ethics statement and consent to participate
The Clinical Research Ethic Committee of Zhejiang Cancer Hospital, which approved this study (approval number: IRB-2025-327 (IIT)), waived the need for informed consent for this retrospective study. All procedures were in accordance with the Declaration of Helsinki.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yuan, J., Wu, Y., Cheng, Y. et al. The risk analysis of unplanned tracheal intubation after radical esophagectomy. Sci Rep 15, 45635 (2025). https://doi.org/10.1038/s41598-025-30531-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-30531-2
