
Abstract
Hyperinflammation and extensive cell damage characterize both COVID-19-sepsis and bacterial sepsis, contributing to poor clinical outcomes. Cell-free DNA (cfDNA), a damage-associated molecular pattern (DAMP), reflects ongoing tissue injury and may predict mortality. We aimed to evaluate cfDNA as a prognostic biomarker for 30-day mortality in ICU patients with COVID-19- vs. bacterial sepsis, and its association with inflammatory markers and disease progression. In a prospective observational study (ethics approval: 2020–15,535; DRKS-ID: DRKS00025222), cfDNA was quantified in 64 ICU patients (COVID-19-sepsis n = 27, bacterial sepsis n = 37) at four time points using quantitative PCR targeting 90 bp and 222 bp fragments of LINE-1 elements. An Integrity Index (222/90 bp) was calculated to infer the predominant mode of cell death. Nineteen healthy individuals served as controls. Associations with mortality and clinical parameters were analyzed using adjusted Cox regression, time-dependent models, and correlation analyses. Higher cfDNA levels (90 bp) within the first 24 h were strongly associated with 30-day (p = 0.003) and 180-day mortality (p = 0.003) in COVID-19-sepsis, but not in bacterial sepsis. COVID-19 patients showed significantly higher cfDNA levels (p < 0.01), which correlated with CRP, PCT, LDH, and lactate. The Integrity Index increased over time in bacterial sepsis and remained stable in COVID-19-sepsis, but was not predictive of survival. Elevated cfDNA levels were associated with ECMO therapy but not with renal replacement therapy. cfDNA is a valuable early prognostic biomarker in COVID-19-sepsis. Its rapid dynamics and strong correlation with clinical outcomes highlight its potential for real-time monitoring and risk stratification in viral sepsis.
Similar content being viewed by others


Introduction
Cell-free DNA (cfDNA) is a recognized mediator of inflammation and tissue damage in sepsis syndromes, including both bacterial sepsis and coronavirus disease 2019 (COVID-19) sepsis. Elevated cfDNA levels reflect cellular injury, neutrophil activation, and uncontrolled immune responses, contributing to the amplification of systemic inflammation1.
Several conventional biomarkers of inflammation, such as C-reactive protein (CRP), procalcitonin (PCT), D-dimer, and ferritin2,3 correlate with adverse outcomes in sepsis. Inflammatory cytokines including interleukin (IL)-6, IL-8, and tumor necrosis factor-α (TNF-α), have also been linked to unfavorable disease trajectories4,5,6. However, cfDNA distinguishes itself as a damage-associated molecular pattern (DAMP), released from dead or damaged cells, or from activated immune cells such as neutrophils7 as a consequence of viral or bacterial infection. It plays a distinctive role in actively exacerbating inflammatory responses through pattern recognition receptors (PRRs). This amplification results in a vicious cycle of inflammation and cellular damage, contributing to disease severity8. In both COVID-19 and bacterial sepsis, cfDNA promotes the formation of neutrophil extracellular traps (NETs)9, a defensive mechanism that, when dysregulated, exacerbates organ injury and inflammation10 by releasing additional DAMPs and promoting cell death8. In COVID-19 sepsis, these processes can culminate in cytokine release syndrome (CRS) and multi-organ failure (MOF)11, mechanisms closely paralleling bacterial sepsis8.
Recent studies have identified cfDNA as a predictive biomarker for disease severity in both COVID-19 and bacterial sepsis12,13, based on its ability to reflect systemic inflammation, and tissue damage14. To further characterize the source and nature of cfDNA, the cfDNA Integrity Index—calculated as the ratio of longer (222 bp) to shorter (90 bp) fragments—has been proposed as an indicator of cfDNA origin. A higher Integrity Index is associated with NETosis and necrotic cell death, as seen in neutrophil activation, while a lower Integrity Index is typically reflective of apoptosis15. Importantly, the Integrity Index is not static and may change over time during the course of critical illness, potentially reflecting shifts in the dominant mechanisms of cell death and immune activation.
However, comparisons across studies are limited by heterogeneity in measurement techniques and clinical protocols. Consequently, the prognostic value of cfDNA in viral sepsis versus bacterial sepsis remains uncertain in the absence of a standardized, comparable study designs.
The primary endpoint of this study was to systematically evaluate whether cfDNA levels serve as a prognostic biomarker for 30-day mortality in patients with COVID-19-sepsis, and to compare this association to patients with bacterial sepsis. Additionally, we monitored cfDNA progression during the ICU stay, correlated cfDNA with inflammatory markers and clinical complications, and performed follow-up of patient mortality up to 180 days after ICU admission.
We hypothesized that cfDNA levels would be significantly higher in COVID-19-sepsis patients compared to bacterial sepsis, based on findings from our preceding pilot study, which demonstrated elevated cfDNA levels in COVID-19 patients compared to healthy controls12. Furthermore, we anticipated that cfDNA dynamics would correlate with short- and long-term mortality, as well as markers of disease progression, especially given the absence of specific therapeutic interventions for COVID-19-sepsis.
Methods
Study description
This prospective observational study was conducted at the Department of Anesthesiology, University Medical Center Mainz, Germany. Ethical approval (Landesärztekammer Rheinland-Pfalz; 2020–15,535) was obtained, following the Declaration of Helsinki and registered in the German Clinical Trial Register (DRKS-ID: DRKS00025222). The study recruited patients in the anesthesiologic ICU from February 2021 to May 2022. Additionally, a control group of 19 healthy individuals, generated in a preceding pilot study (Ethical approval No.: 2020–15,116-retrospective), was included to provide baseline cfDNA reference values.
Data collection
Patient data and test results were pseudonymized and collected from patients meeting inclusion criteria (Supplementary Table 1). Inclusion criteria were: diagnosis of bacterial or COVID-19 sepsis according to Sepsis-3 definitions16. Exclusion criteria comprised pre-existing conditions known to elevate cfDNA levels independently of infection, such as active malignancy or pregnancy. SARS-CoV-2 infection was confirmed by polymerase chain reaction (PCR) test. Patients were followed for 180 days post-ICU admission, with mortality assessed at 30 and 180 days.
Patients with COVID-19 received standardized treatment according to national recommendations of the RKI (Robert Koch Institut) and its STAKOB/COVRIIN group, including Remdesivir and corticosteroids. No deviations such as the interim use of acetylsalicylic acid, ACE inhibitors, or monoclonal antibody therapy occurred.
Power analysis and study size
Power analysis based on a pilot study12 indicated a cohort size of 60 patients per group. The calculation was based on cfDNA levels observed in moderately ill COVID-19 patients and healthy controls. In the current study, patients were more severely ill and showed substantially higher cfDNA levels, which exceeded pilot estimates. In the COVID-19 sepsis cohort, recruitment became increasingly difficult, and univariable Cox proportional hazards models had already demonstrated a highly significant association between cfDNA levels and 30- and 180-day mortality (p < 0.001); therefore, only 27 of the planned 60 patients were included. In the bacterial sepsis cohort, recruitment was stopped after 37 patients, as a sample size calculation based on these data indicated that at least 141 patients would be required to detect a significant association between cfDNA levels and mortality, at a significance level of 0.05 and a power of 80%, which was not feasible. Patient enrollment was thus terminated early due to declining ICU admissions and the robustness of the findings.
Sample collection and analysis
Blood samples were drawn into ethylenediaminetetraacetate (EDTA) tubes (Sarstedt®) at four defined time points: at ICU admission (0–24 h), between days 1–3, between days 7–10, and at day 14 (Supplementary Table 2). Samples were centrifuged at 3746 × g for 10 min at 20 °C within 3 h and stored at -80 °C. Quantitative real-time qPCR was performed for cfDNA determination as described by Neuberger et al.17. Amplicons of 90 and 222 base pairs (bp) of human long nuclear elements (LINE) of the L1PA2 family18 were analyzed, achieving ultra-low limit of quantification (LOQ) of 0.47 and 0.69 ng/mL, with repeatability ≤ 11.6% and intermediate precision ≤ 12.2%17. The cfDNA Integrity Index was calculated as the ratio of the concentration of 222 bp fragments to 90 bp fragments, reflecting the relative proportion of longer to shorter cfDNA fragments. CfDNA levels were determined without altering patient treatment.
The same blood collection tubes (EDTA, Sarstedt®), centrifugation scheme (3746 × g for 10 min, 20 °C, within 3 h of collection), storage conditions (− 80 °C), and identical qPCR assay (primer sets, reagents, platform, and calibration procedures) were used for both patients and controls. This approach minimized potential batch effects and ensured comparability between groups. The decision to use previously enrolled controls was based on ethical reasons, given that recruiting contemporaneous healthy volunteers during the COVID-19 pandemic was restricted.
Statistical analysis
Statistical analyses were conducted using R software (version 4.2.2, R Foundation for Statistical Computing, Vienna, Austria). Continuous variables are presented as mean ± standard deviation (SD) or median (interquartile range, IQR), and categorical variables as counts and percentages. For regression analyses, cfDNA values were used in their log-transformed form.
Primary endpoint
The primary endpoint was the association between cfDNA levels (90 bp and 222 bp), measured within 24 h of ICU admission, and 30-day mortality. This was assessed using Cox regression models adjusted for age and ASA classification. Survival curves were visualized using Kaplan–Meier estimates, with cfDNA levels dichotomized at median.
Secondary endpoints
Secondary endpoints focused on evaluating the relationship between cfDNA levels and (1) 180-day mortality, (2) inflammatory biomarkers (e.g., CRP, PCT, LDH, WBC, lactate), and (3) clinical complications such as the need for extracorporeal membrane oxygenation (ECMO) or renal replacement therapy.
-
(1)
Associations between cfDNA levels and 180-day mortality were analyzed using Cox regression models, adjusted for age and ASA classification. To further assess the prognostic value of cfDNA over time, extended Cox models with time-dependent covariates were applied.
-
(2)
Relationships between cfDNA levels and inflammatory markers at all four sampling time points were examined using Spearman’s rank correlation coefficient. These analyses were performed separately for COVID-19-sepsis and bacterial sepsis groups.
-
(3)
Associations between cfDNA concentrations and clinical complications, including the need for organ support therapies such as ECMO or renal replacement therapy, were analyzed using generalized estimating equations (GEE).
Additionally, cfDNA kinetics were evaluated using linear mixed models (ANOVA) to assess group differences and time trends across the four defined sampling points.
Comparison with healthy controls:
cfDNA concentrations and selected laboratory parameters were compared across COVID-19-sepsis, bacterial sepsis, and healthy control groups using the Kruskal–Wallis test.
Significant group differences were followed by Dunn’s post hoc test with Bonferroni correction for pairwise comparisons.
To ensure comparability, only cfDNA values from the first patient sampling (0–24 h after ICU admission) were used in comparisons with the single time-point data from healthy controls.
Results
Cohort characteristics
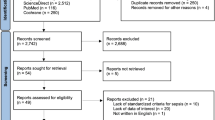
Enrollment included 27 patients with COVID-19-sepsis and 37 patients with bacterial sepsis (Fig. 1, Table 1). Among the COVID-19 patients, the majority were infected with the Delta variant (n = 16, 59.3%), while smaller numbers were observed for Alpha (n = 4, 14.8%), Beta (n = 1, 3.7%), and Omicron (n = 1, 3.7%). In 5 patients (18.5%) the viral variant was not determined. Additionally, a control group of 19 healthy individuals was included for comparison (Supplementary Table 3). Controls had a lower median age compared to patients and exhibited significantly lower cfDNA concentrations at baseline (p < 0.001) and significantly higher Integrity Indices (p < 0.001). Inflammatory markers such as CRP, WBC, and platelet counts were within normal ranges, with no signs of systemic inflammation.

Study cohort flow diagram detailing screening, eligibility, enrollment, and follow-up.
Patients with COVID-19-sepsis had similar 30-day (40% vs. 31%, p = 0.46) and 180-day mortality (58% vs. 55%, p = 0.78) rates compared to bacterial sepsis, but prolonged hospitalization (p = 0.002) and a higher prevalence of obesity (p = 0.02). Other comorbidities, including chronic cardiac disease and chronic renal disease, were more common in bacterial sepsis. Sequential Organ Failure Assessment (SOFA) scores were comparable between groups. Pulmonary complications, including ARDS and the need for ECMO therapy, were more frequent in COVID-19-sepsis, whereas other complications such as delirium and atrial fibrillation occurred more often in bacterial sepsis.
Primary endpoints
cfDNA levels as a prognostic marker for 30-day mortality
Despite similar 30-day mortality rates between COVID-19 sepsis (40%) and bacterial sepsis patients (31%) (p = 0.46; Table 1), cfDNA concentrations were significantly associated with survival outcomes, as illustrated in the Kaplan–Meier curves in Supplementary Fig. 1A–B. In COVID-19 sepsis patients, adjusted Cox regression analysis demonstrated that higher cfDNA levels within the first 24 h of ICU admission were strongly predictive of 30-day mortality (HR 5.02, 95% CI 1.75–14.43; p = 0.003; Table 2).
In contrast, in bacterial sepsis, cfDNA levels did not significantly correlate with 30-day mortality; only patient age was an independent predictor (HR 1.13, 95% CI 1.04–1.21; p = 0.002).
ROC analysis demonstrated promising discriminatory ability between survivors and non-survivors at hospital discharge among patients with COVID-19 sepsis (AUC = 0.99), but only moderate discrimination among those with bacterial sepsis (AUC = 0.68).
Secondary endpoints
cfDNA levels and 180-day mortality
Higher cfDNA levels measured within the first 24 h of ICU admission were similarly associated with increased 180-day mortality in COVID-19-sepsis patients (p = 0.003; Table 2).
Extended Cox models confirmed that elevated cfDNA concentrations strongly predicted long-term mortality (HR 2.66, 95% CI 1.59–4.45; p < 0.001), while in bacterial sepsis no significant relationship between cfDNA levels and 180-day mortality was observed (Supplementary Table 4).
In bacterial sepsis, higher LDH concentrations (p = 0.008) and lower WBC counts (p = 0.05) were associated with 30-day mortality.
cfDNA levels and disease progression over time and correlation with mortality
cfDNA levels at ICU admission were significantly higher in COVID-19-sepsis compared to bacterial sepsis for both 90 bp (p = 0.001) and 222 bp (p = 0.002) fragments (Fig. 2A–B). Over the course of ICU stay, 90 bp cfDNA levels decreased significantly in both groups (p = 0.006), while 222 bp levels remained relatively stable (p = 0.31).

Temporal dynamics and outcome association of log-transformed cfDNA levels in COVID-19 and bacterial sepsis. (a) 90 bp cfDNA progression over time for COVID-19-sepsis and bacterial sepsis patients. (b) 222 bp cfDNA progression over time for COVID-19-sepsis and bacterial sepsis patients. (c) individual courses of cfDNA levels for 90 bp for patients with COVID-19-sepsis and bacterial sepsis separated in survivors and non-survivors. (d) cfDNA levels of last measurement and association with hospital discharge and mortality for patients with COVID-19- sepsis and bacterial sepsis. Measurement timepoints:1 = 0–24 h after ICU admission; 2 = day 1–3; 3 = day 7–10; 4 = day 14.
In COVID-19-sepsis non-survivors showed consistently higher cfDNA levels over time than survivors, with diverging trajectories emerging early during the ICU course (Fig. 2C). This pattern was also visible at the final time point (day 14), where boxplots illustrate substantial differences in cfDNA distributions between survivors and non-survivors (Fig. 2D).
To assess the prognostic relevance of cfDNA kinetics, extended Cox regression models with time-dependent covariates were applied. These models account for dynamic changes in cfDNA levels over time rather than relying on static baseline values. In COVID-19-sepsis, cfDNA progression was independently associated with 30-day mortality (HR 1.45, 95% CI 1.12–1.87; p = 0.005; Supplementary Table 4), highlighting its value as a dynamic prognostic biomarker. In contrast, no such association was observed in bacterial sepsis.
The cfDNA Integrity Index (calculated as the ratio of 222 bp to 90 bp fragments) was not significantly associated with survival in either cohort.
Correlation of cfDNA with inflammatory markers
cfDNA levels correlated strongly with inflammatory and infection parameters at multiple time points (Supplementary Tables 5 and 6).
In COVID-19-sepsis, the highest correlation was found between cfDNA and LDH at baseline (Spearman’s Rho = 0.79; p < 0.0001) and persisted over time. Additionally a significant correlation was observed with CRP (p = 0.015) and PCT (p = 0.009).
In bacterial sepsis, cfDNA correlated significantly with LDH (p < 0.001) and PCT (p = 0.02) at baseline, and with lactate from the second time point onward.
Influence of pre-existing conditions on cfDNA levels
In COVID-19-sepsis, patients with pre-existing kidney disease (n = 5) exhibited significantly higher cfDNA levels compared to those without (p = 0.008) (Supplementary Fig. 2).
Importantly, patients with bacterial sepsis and pre-existing immunological disorders (n = 4) – including autoimmune diseases (systemic lupus erythematosus, rheumatoid arthritis) and heparin-induced thrombocytopenia (HIT) – exhibited significantly elevated baseline cfDNA levels (p < 0.001) (Supplementary Fig. 3).
To account for the overall comorbidity burden, outcome analyses were adjusted for ASA classification rather than for individual diseases, as ASA reflects a cumulative comorbidity risk. In these adjusted models, ASA classification itself was not significantly associated with mortality, whereas cfDNA levels in COVID-19-sepsis remained predictive (Table 2).
cfDNA and clinical complications
cfDNA concentrations were not significantly associated with acute kidney injury (AKI) or the need for renal replacement therapy (RRT).
However, ECMO therapy was significantly associated with higher cfDNA levels (p < 0.001) (Supplementary Table 7).
Discussion
This study contributes to the growing recognition of cfDNA as a critical biomarker in the pathophysiology of sepsis, particularly in distinguishing the inflammatory responses associated with COVID-19-sepsis and bacterial sepsis. While previous studies have reported its prognostic value in both types of sepsis 12,13, cross-group comparisons have been limited due to heterogeneous methods and patient cohorts. By applying a standardized study protocol, we evaluated whether cfDNA levels predict 30-day mortality in patients with COVID-19-sepsis and compared this with bacterial sepsis. Our hypothesis was based on findings from our pilot study in COVID-19 patients and cfDNA data from the literature. In addition, we assessed cfDNA kinetics, associations with inflammatory markers, and outcomes up to 180 days. We found that cfDNA levels were significantly elevated in COVID-19-sepsis, correlated strongly with both short- and long-term mortality, and tracked disease progression. No such prognostic association was observed in bacterial sepsis.
Primary Endpoints
cfDNA as a prognostic marker for 30-day and 180-day mortality
This study demonstrates that cfDNA levels within the first 24 h of ICU admission are strong and independent predictors of 30-day and 180-day mortality in patients with COVID-19-sepsis. These findings confirm and extend results from our earlier pilot study12, showing that elevated cfDNA levels are associated with poor outcomes in COVID-1919. In contrast, cfDNA concentrations in bacterial sepsis showed no significant association with mortality.
While the fundamental pathophysiological mechanisms of sepsis—such as immune activation, cytokine release, and NET-formation—are shared between bacterial and viral etiologies9,20, two key factors may explain the observed differences in cfDNA–mortality associations. First, COVID-19 appears to trigger a more sustained and dysregulated immune response, often characterized by excessive NETosis and delayed viral clearance21. This may lead to prolonged cfDNA release and amplified tissue damage. Second, the availability of effective and timely antibiotic treatment in bacterial sepsis likely attenuates the inflammatory cascade early in the disease course16, reducing cfDNA levels and their prognostic utility. In contrast, pathogen-specific therapies for COVID-19 were either unavailable or ineffective during the study period22, resulting in persistently elevated cfDNA in critically ill patients. These differences were observed despite comparable disease severity at ICU admission, as indicated by similar SOFA scores in both patient groups.
This combination—a stronger pathophysiological immune reaction in COVID-19 and the lack of effective early intervention—may help to explain the association between cfDNA and mortality observed in COVID-19-sepsis. Extended Cox models suggested that cfDNA dynamics over time were independently associated with both short- and long-term mortality in COVID-19 patients, but not in those with bacterial sepsis. The promising discrimination observed in ROC analysis (AUC = 0.99) and Kaplan–Meier survival differences underscore its potential for early risk stratification in viral sepsis. However, these results must be interpreted with caution due to small sample size and should be regarded as hypothesis-generating rather than definitive and require external validation before clinical application. In bacterial sepsis, by contrast, the impact of early treatment may obscure the prognostic relevance of cfDNA.
Previous studies showing prognostic associations in bacterial sepsis13,23,24,25 often lacked longitudinal sampling, standardized protocols, or clear exclusion criteria. Our findings emphasize that cfDNA should be interpreted in the context of both immune activation and therapeutic timing, and support its use as a dynamic, disease- and treatment-sensitive biomarker.
Secondary endpoints
cfDNA levels and disease progression over time
The temporal dynamics of cfDNA in our study provide insight into the evolving mechanisms of cell death during sepsis. While cfDNA concentrations were significantly elevated in COVID-19-sepsis compared to bacterial sepsis early after ICU admission, both groups exhibited a notable decline in 90 bp cfDNA over time, while 222 bp levels remained relatively stable in bacterial sepsis.
The Integrity Index is calculated as the ratio of 222 bp to 90 bp fragments. Short cfDNA fragments (~ 90 bp) are typically associated with apoptotic cleavage patterns, whereas longer fragments (~ 222 bp) may rise from necrosis or NETosis13,26. Thus, the observed decline of 90 bp levels over time, together with relatively stable 222 bp levels, is compatible with a shift toward NETosis or necrotic cell death in bacterial sepsis27.
In COVID-19-sepsis, both 90 bp and 222 bp levels decreased, resulting in a less pronounced rise of the Integrity Index. This may reflect ongoing apoptosis and less consistent NET-driven fragmentation, in line with prior findings of prolonged immune dysregulation and impaired viral clearance in severe COVID-1919.
Overall, these kinetic patterns suggest that cfDNA kinetics may provide information about disease severity as well as about qualitative changes in cell death pathways over time.
However, the Integrity Index was not independently predictive in our models, and its mechanistic interpretation remains speculative. Future studies should therefore combine cfDNA fragment analysis with direct markers of NETosis or nucleosome assays to validate and expand these exploratory findings.
Correlation with inflammatory markers
cfDNA showed consistent correlations with established inflammatory biomarkers including CRP, PCT, LDH, and lactate. In COVID-19-sepsis, the strongest association was observed between cfDNA and LDH—a marker of cellular damage—highlighting cfDNA’s ability to reflect active tissue injury. These results confirm earlier reports linking cfDNA to systemic inflammation and cell death24, and further establish its utility as a biomarker that integrates both immune activation and tissue damage signals.
Importantly, cfDNA appears to offer key advantages over conventional markers. Unlike CRP and PCT, which depend on hepatic synthesis and exhibit delayed kinetics, cfDNA is released immediately upon cellular damage and has a short half-life (5–120 min), allowing for earlier detection of dynamic inflammatory changes28. Furthermore, cfDNA is not affected by hepatic dysfunction or protein synthesis disorders, which can limit the reliability of CRP and PCT in critically ill patients. These properties position cfDNA as a potentially superior biomarker for early-phase disease monitoring and treatment response.
cfDNA and pre-existing medical conditions
We also observed that certain comorbidities were associated with altered cfDNA levels. In COVID-19-sepsis, patients with chronic kidney disease had significantly higher cfDNA, likely due to impaired renal clearance, consistent with prior studies29. In bacterial sepsis, elevated cfDNA was associated with pre-existing immunological disorders, such as autoimmune disease or HIT30, suggesting a possible link between immune dysregulation and enhanced cfDNA release. To account for the overall burden of comorbidities, outcome analyses were adjusted for ASA classification rather than individual diseases, since ASA reflects cumulative comorbidity risk. This approach was chosen because of the limited sample size and the low frequency of many single conditions, which would not allow stable statistical adjustment. In these models, ASA classification itself was not significantly associated with mortality, whereas cfDNA levels in COVID-19-sepsis retained prognostic significance. This indicates that the predictive value of cfDNA is not merely explained by comorbidity burden.
While group sizes were limited, these findings highlight the potential of cfDNA as a comorbidity independent prognostic marker and warrant confirmation in larger studies with detailed phenotyping.
cfDNA and clinical complications
Among critically ill patients, extracorporeal membrane oxygenation (ECMO) was significantly associated with elevated cfDNA levels. This may be attributed to the mechanical stress and exposure to artificial surfaces inherent to ECMO circuits, which can promote immune activation and cellular injury31. While earlier reports suggested only mild effects of ECMO on cfDNA, our findings indicate a more substantial impact in the context of severe viral sepsis. In contrast, no significant associations were observed between cfDNA and renal replacement therapy or dialysis dependence, possibly due to the use of continuous modalities (CRRT) in our ICU, which are associated with lower shear stress compared to intermittent hemodialysis32.
Limitations
This study provides valuable insights into cfDNA as a biomarker in sepsis; however, several limitations must be acknowledged. The healthy control group was substantially younger and was collected during an earlier study period compared to the patient cohorts. This could bias baseline cfDNA comparisons. To our knowledge, no specific age-stratified reference values for cfDNA are available in the literature; however, it is reasonable to assume that older individuals may exhibit higher cfDNA concentrations. Although identical sampling, processing, storage and qPCR quantification procedures were used to minimize batch effects, residual confounding related to sample handling cannot be excluded. Although regression models were adjusted for age and ASA class, residual confounding from baseline comorbidities cannot be excluded. Furthermore, no statistical adjustment was performed for therapies with antibiotics, antivirals, or corticosteroids, which may have influenced cfDNA levels and outcomes. A residual bias from these factors therefore cannot be excluded. The relatively small sample size, particularly in subgroup analyses, may limit statistical power and inflate effect estimates such as the very high AUC values. Moreover, due to the limited sample size, no internal validation procedures (such as bootstrapping or cross-validation) were performed for the ROC analyses; therefore, a potential risk of overfitting cannot be fully excluded and should be considered when interpreting the discriminatory performance of cfDNA. In addition, the single-center design restricts the generalizability of our findings. Furthermore, the predominance of Delta infections among COVID-19 patients in our cohort may limit the transferability of our results to other SARS-CoV-2 variants.
In addition, while cfDNA reflects systemic inflammation and tissue damage, it lacks cell-type specificity. Although the Integrity Index offers indirect insights into cell death mechanisms, more precise methods—such as methylation profiling or fragmentomics would be needed to determine cfDNA tissue origin and improve biological interpretation.
For future clinical translation, standardized, high-frequency cfDNA sampling and real-time quantification protocols are needed. Future studies should include methylated cfDNA analysis and more granular clinical documentation to enable sepsis subtyping and improve the biomarker’s diagnostic and prognostic utility.
Conclusions
cfDNA is a promising biomarker in sepsis, with significantly elevated levels in COVID-19-sepsis that were strongly associated with 30- and 180-day mortality. No such association was observed in bacterial sepsis, likely due to effective early treatment and different cfDNA kinetics. Fragment analysis revealed a shift from apoptosis to NETosis over time, particularly in bacterial sepsis, as reflected by the rising Integrity Index, however this interpretation requires further validation. cfDNA also correlated well with inflammatory markers and offers advantages over conventional biomarkers due to its rapid kinetics and independence from hepatic function. These findings support cfDNA’s potential for real-time risk stratification and disease monitoring in critically ill patients, especially in viral sepsis. However, the results should be regarded as hypothesis-generating and require confirmation in larger, multi-center studies with standardized sampling protocols and extended molecular analyses.
Data availability
The data used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
de Miranda, F. S. et al. Properties and application of cell-free DNA as a clinical biomarker. Int. J. Mol. Sci. 22(17), 9110 (2021).
Huang, I. et al. C-reactive protein, procalcitonin, D-dimer, and ferritin in severe coronavirus disease-2019: a meta-analysis. Ther. Adv. Respir. Dis. 14, 1753466620937175 (2020).
Wang, G. et al. C-reactive protein level may predict the risk of COVID-19 aggravation. Open Forum Infect. Dis. 7(5), offa153 (2020).
Del Valle, D. M. et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat. Med. 26(10), 1636–1643 (2020).
Herold, T. et al. Elevated levels of IL-6 and CRP predict the need for mechanical ventilation in COVID-19. J. Allergy Clin. Immunol. 146(1), 128-136.e4 (2020).
Zhang, X. et al. Viral and host factors related to the clinical outcome of COVID-19. Nature 583(7816), 437–440 (2020).
van der Poll, T., Shankar-Hari, M. & Wiersinga, W. J. The immunology of sepsis. Immunity 54(11), 2450–2464 (2021).
Denning, N. L. et al. DAMPs and NETs in Sepsis. Front Immunol 10, 2536 (2019).
Gillot, C. et al. NETosis and the immune system in COVID-19: mechanisms and potential treatments. Front. Pharmacol. 12, 708302 (2021).
Porto, B. N. & Stein, R. T. Neutrophil extracellular traps in pulmonary diseases: too much of a good thing?. Front. Immunol. 7, 311 (2016).
Tay, M. Z. et al. The trinity of COVID-19: immunity, inflammation and intervention. Nat. Rev. Immunol. 20(6), 363–374 (2020).
Hoeter, K. et al. Evidence for the utility of cfDNA plasma concentrations to predict disease severity in COVID-19: A retrospective pilot study. PeerJ 11, e16072 (2023).
Charoensappakit, A. et al. Cell-free DNA as diagnostic and prognostic biomarkers for adult sepsis: A systematic review and meta-analysis. Sci. Rep. 13(1), 19624 (2023).
Cheng, A. P. et al. Cell-free DNA tissues of origin by methylation profiling reveals significant cell, tissue, and organ-specific injury related to COVID-19 severity. Med 2(4), 411-422.e5 (2021).
Salvianti, F. et al. Integrity and quantity of total cell-free DNA in the diagnosis of thyroid cancer: Correlation with cytological classification. Int. J. Mol. Sci. 18(7), 1350 (2017).
Singer, M. et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA 315(8), 801–810 (2016).
Neuberger, E. W. I. et al. Validating quantitative PCR assays for cfDNA detection without DNA extraction in exercising SLE patients. Sci Rep 11(1), 13581 (2021).
Buzdin, A. et al. Genome-wide targeted search for human specific and polymorphic L1 integrations. Hum. Genet. 112, 527–533 (2003).
Stawski, R., Nowak, D. & Perdas, E. Cell-free DNA: potential application in COVID-19 diagnostics and management. Viruses 14(2), 321 (2022).
Zhu, C. L. et al. Dysregulation of neutrophil death in sepsis. Front Immunol 13, 963955 (2022).
Chen, X. et al. Risk factors for the delayed viral clearance in COVID-19 patients. J Clin Hypertens (Greenwich) 23(8), 1483–1489 (2021).
Stefan Kluge, U.J., Tobias Welte, Steffen Weber-Carstens, Gereon Schälte, Christoph D. Spinner, Jakob J. Malin, Petra Gastmeier, Florian Langer, Hendrik Bracht, Michael Westhoff, Michael Pfeifer, Klaus F. Rabe, Florian Hoffmann, Bernd W. Böttiger, Julia Weinmann-Menke, Alexander Kersten, Peter Berlit, Marcin Krawczyk, Wiebke Nehls, Reiner Haase, Oliver J. Müller, Christof Specker, Monika Nothacker, Nicole Skoetz, Gernot Marx, Christian Karagiannidis. S3-Leitlinie - Empfehlungen zur Therapie von Patienten mit COVID-19. AWMF online 2023 [cited 2023 05.04.2023]; Available from: https://register.awmf.org/de/leitlinien/detail/113-001LG.
Clementi, A. et al. The role of cell-free plasma DNA in critically Ill patients with sepsis. Blood Purif. 41(1–3), 34–40 (2016).
Hou, Y. Q. et al. Branched DNA-based Alu quantitative assay for cell-free plasma DNA levels in patients with sepsis or systemic inflammatory response syndrome. J. Crit. Care 31(1), 90–95 (2016).
Dadam, M. N. et al. Role of cell-free DNA levels in the diagnosis and prognosis of sepsis and bacteremia: A systematic review and meta-analysis. PLoS ONE 19(8), e0305895 (2024).
Umetani, N. et al. Increased integrity of free circulating DNA in sera of patients with colorectal or periampullary cancer: direct quantitative PCR for ALU repeats. Clin. Chem. 52(6), 1062–1069 (2006).
Chen, Z. et al. Review: The emerging role of neutrophil extracellular traps in sepsis and sepsis-associated thrombosis. Front. Cell. Infect. Microbiol. 11, 653228 (2021).
Avriel, A. et al. Admission cell free DNA levels predict 28-day mortality in patients with severe sepsis in intensive care. PLoS ONE 9(6), e100514 (2014).
Clementi, A. et al. Plasma cell-free DNA and caspase-3 levels in patients with chronic kidney disease. J. Clin. Med. 12(17), 5616 (2023).
Mondelo-Macía, P. et al. Circulating free DNA and its emerging role in autoimmune diseases. J. Personal. Med. 11(2), 151 (2021).
Lingel, M. P. et al. Clinical relevance of cell-free DNA during venovenous extracorporeal membrane oxygenation. Artif. Organs 47(11), 1720–1731 (2023).
Rumore, P. et al. Haemodialysis as a model for studying endogenous plasma DNA: oligonucleosome-like structure and clearance. Clin. Exp. Immunol. 90(1), 56–62 (1992).
Acknowledgements
The data shown in this manuscript are part of the doctoral thesis of the coauthors Vanessa Jochum and Maria Bergmann and the professional dissertation (habilitation) of Katharina Hoeter presented to the Johannes Gutenberg-University Mainz.
Funding
Open Access funding enabled and organized by Projekt DEAL. The study was supported by the Clinical Research Fellowship of the University Medical Center Mainz, Germany and the Federal Ministry of Research, Technology and Space; Funding-No.: 13GW0593E.
Author information
Authors and Affiliations
Contributions
KH, EWIN, PS, MKES, MB conceived and designed the study; KH, EWIN, VJ, KE, RK, MB, PS, MKES, MB acquisition, analysis; KH, EWIN, PS, MKES, MB the interpretation of data; KH, EWIN, RK, PS, MKES, MB have drafted the work or substantively revised it. All authors have approved the submitted version (and any substantially modified version that involves the author’s contribution to the study) and have agreed both to be personally accountable for the author’s own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The authors of this study confirm that the study was conducted to investigate a new biomarker for its prognostic value regarding the outcome of ICU patients with COVID-19-sepsis and bacterial sepsis.
The study was approved by the Ethics Committee (Landesärztekammer Rheinland-Pfalz; 2020–15535) and informed consent was obtained from participants. All methods involving human participants were performed in accordance with the ethical standards of the Declaration of Helsinki. This is an independent review board to which the institution University Medical Centre of the Johannes Gutenberg-University, Mainz, Germany is assigned.
Declaration of generative AI in scientific writing
During the preparation of this work the author used Deep L Write in order to improve readability and language. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hoeter, K., Neuberger, E.W.I., Jochum, V. et al. Prospective observational study of cell-free DNA as a prognostic biomarker in COVID-19 and bacterial sepsis: COVSEP-study. Sci Rep 15, 44144 (2025). https://doi.org/10.1038/s41598-025-32810-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-32810-4
