
Abstract
To identify risk factors associated with the necessity of bronchoalveolar lavage (BAL) in children with Mycoplasma pneumoniae pneumonia (MPP) and pulmonary consolidation, and to develop and validate a predictive model to support clinical decision-making. A retrospective study was conducted on 323 children diagnosed with MPP and pulmonary consolidation at our hospital from September 2020 to October 2023. Patients were divided into BAL group (n = 163) and non-BAL group (n = 160). Clinical data, laboratory findings, and imaging features (including quantified pulmonary consolidation volume) were collected. Univariate and multivariate logistic regression analyses were employed to identify independent predictors for BAL intervention. A nomogram was constructed based on significant factors. The model’s performance was assessed using the receiver operating characteristic (ROC) curve, concordance index (C-index), calibration plot, and internal validation via bootstrap resampling. Multivariate logistic regression identified lung atelectasis, older age, greater pulmonary consolidation volume (percentage of total lung volume), and longer hospital stay as independent risk factors for BAL. Corticosteroid treatment emerged as a protective factor. The nomogram developed from these variables yielded an area under the ROC curve (AUC) of 0.87 (95% CI: 0.83–0.91), with good calibration. Internal validation confirmed the robustness of the model. Lung atelectasis, pulmonary consolidation extent, length of hospitalization, age, and corticosteroid therapy are key determinants for BAL necessity in MPP children with consolidation. The proposed nomogram demonstrates strong discrimination, calibration, and clinical applicability, facilitating personalized evaluation of BAL indication.
Similar content being viewed by others


Introduction
Mycoplasma pneumoniae (MP) is one of the major pathogens responsible for community-acquired pneumonia (CAP) in children. Although Mycoplasma pneumoniae pneumonia (MPP) is generally self-limiting, the incidence of refractory MPP (RMPP) and severe cases has been increasing in recent years, accompanied by more complications and a heavier disease burden1,2. MP infection can trigger a strong immune response and mucosal injury, leading to excessive mucus secretion, impaired ciliary function, and airway obstruction3. Radiologically, pulmonary consolidation is a common manifestation of MPP. However, complications within the airway—such as plastic bronchitis, mucus plug obstruction, or severe mucosal damage—are often difficult to detect by chest X-ray or CT alone, making bronchoscopy a valuable diagnostic tool in such cases4.
Bronchoalveolar lavage (BAL), as an adjunctive treatment for MPP, can effectively remove airway secretions and mucus plugs, promote resolution of inflammation and lung re-expansion, and reduce complications4. However, as an invasive and high-cost procedure, BAL is not suitable for all MPP patients with pulmonary consolidation. At present, there is a lack of objective criteria to determine which patients truly require BAL intervention.
This study aimed to retrospectively analyze the clinical, laboratory, and radiological data (including quantitative pulmonary consolidation volume) of 323 children with MPP and pulmonary consolidation (BAL group: 163 cases; non-BAL group: 160 cases) in order to identify independent risk factors for BAL intervention and to develop and validate a predictive model. The model is expected to enhance clinical decision-making accuracy, promote individualized management, minimize unnecessary procedures, and optimize the allocation of healthcare resources.
Methods
Study population
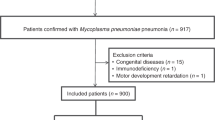
This was a retrospective cohort study involving 323 children with MPP and radiologically confirmed pulmonary consolidation, admitted to the Department of Pediatrics at the Second Affiliated Hospital of Guangxi Medical University between September 2020 and October 2023. Eligible patients ranged in age from 1 month to 15 years and met the following criteria: (1) diagnosed with Mycoplasma pneumoniae pneumonia (MPP) according to the 2023 Chinese guideline (Expert consensus on the diagnosis and treatment of Mycoplasma pneumoniae pneumonia in children)5. Specifically, in addition to clinical symptoms and signs, all patients had a confirmed MP infection evidenced by at least one of the following laboratory criteria: (i) a positive nucleic acid amplification test (NAAT) for MP-DNA or MP-RNA, or (ii) a single serum particle agglutination test titer of anti-MP antibody ≥ 1:160, or a demonstrated fourfold or greater increase in antibody titer during the course of the illness; (2) pulmonary consolidation confirmed by chest CT; (3) BAL evaluated or performed based on the 2018 Chinese guidelines for pediatric flexible bronchoscopy6. Exclusion criteria included: (1) severe underlying diseases; (2) allergy to macrolides; (3) contraindications for bronchoscopy; (4) withdrawal from treatment or lack of consent; and (5) incomplete clinical data.
Data collection
Participants were divided into the BAL group (n = 163) and the non-BAL group (n = 160) based on whether they underwent BAL. Data extracted from electronic medical records included: (1) demographic and clinical characteristics (age, sex, hospital stay, fever peak/duration, lung auscultation findings, corticosteroid therapy); (2) laboratory tests: White blood cell (WBC), Neutrophil Percentage (NEU%), Lymphocyte Percentage (LYM%), High-sensitivity C-reactive protein (hsCRP), Procalcitonin (PCT), Lactic dehydrogenase (LDH), Creatine kinase isomer-MB (CK-MB), D-Dimer (D-D), Fibrinogen (FIB), Erythrocyte Sedimentation Rate (ESR), Alanine Aminotransferase (ALT), Immunoglobulin A (IgA), Immunoglobulin M (IgM), Immunoglobulin G (IgG); (3) imaging features (atelectasis, pleural effusion, consolidation extent). Pulmonary consolidation volume was quantified using Vitrea® Advanced Visualization software (Canon Medical Systems).
Statistical analysis
The normality of continuous variables was assessed using the Shapiro-Wilk test. Data conforming to a normal distribution were expressed as mean ± standard deviation (\({ {\bar {\rm x}}}\) ± s), and comparisons between groups were performed using the independent samples t-test. Non-normally distributed data were presented as median and interquartile range [M (P25–P75)], and the Mann–Whitney U test (rank-sum test) was used for group comparisons. Categorical variables were expressed as frequencies and percentages, and comparisons between groups were conducted using the chi-square test or Fisher’s exact test, as appropriate. Variables with statistically significant differences in univariate analysis were included in a multivariate logistic regression model using a backward stepwise selection method to identify independent predictors of BAL intervention. A nomogram was then constructed based on the final logistic regression model. The predictive performance of the model was assessed using the area under the receiver operating characteristic (ROC) curve (AUC) and calibration plot. Statistical analyses were performed using SPSS version 26.0 and R software version 4.3.2. A two-tailed P value ≤ 0.05 was considered statistically significant.
Results
Clinical characteristics
There were no significant differences in sex between the BAL and non-BAL groups (P > 0.05). The BAL group had a significantly longer hospital stay [7 (6,8) vs. 5 (4,7) days, P < 0.001]. BAL cases were more frequent in summer (38.7%), whereas non-BAL cases peaked in winter (51.3%) (P < 0.001). The BAL group also had higher fever peaks, longer fever duration, and longer macrolide use (all P < 0.05), but lower glucocorticoid use and wheezing incidence (P < 0.05), as shown in Table 1.
Laboratory findings
The BAL group showed significantly higher neutrophil percentage, hsCRP, and D-dimer levels, and lower WBC and CK-MB levels compared to the non-BAL group (P < 0.05), as shown in Table 2.
Radiological characteristics
Atelectasis (9.82% vs. 1.25%), pleural effusion (9.20% vs. 3.75%), proportion of lung consolidation (1.36% vs. 0.28%) and Consolidation volume (9620.00 mm3 vs. 2035.90 mm3) were significantly higher in the BAL group (P < 0.05). Single-lobe consolidation was more common in the non-BAL group (P < 0.05), as shown in Table 3.
Predictive model development
Variables with statistically significant differences in univariate analysis were included in a multivariate logistic regression model using a backward stepwise method. The analysis identified pulmonary consolidation proportion (OR = 2.10), age (OR = 1.01), length of hospital stay (OR = 1.61), and atelectasis (OR = 6.49) as independent risk factors for undergoing BAL. In contrast, corticosteroid use was found to be a protective factor (OR = 0.25), as shown in Table 4.
Based on the identified independent predictors, a nomogram model was constructed to estimate the probability of undergoing BAL (Fig. 1). ROC curve analysis demonstrated good discriminatory power, with an area under the curve (AUC) of 0.87 (95% CI: 0.83–0.91) (Fig. 2). The calibration plot indicated satisfactory agreement between predicted and observed probabilities (Fig. 3). For instance, in a child with MPP and pulmonary consolidation—aged 4 years, hospitalized for 6 days, not treated with corticosteroids, with a consolidation proportion of 2%, and no atelectasis—the corresponding scores for each variable were as follows: 24 points for hospitalization duration, 8 points for age, 24 points for absence of corticosteroid use, and 0 points for absence of atelectasis, yielding a total of 56 points. The predicted probability of requiring BAL was approximately 75%.

Nomogram prediction model for undergoing BAL in pediatric patients.

ROC curve of the nomogram prediction model.

Calibration curve of the nomogram prediction model.
Discussion
The incidence of MPP has increased among pediatric CAP cases, with a rising proportion of RMPP among those with pulmonary consolidation7. MP infection can disrupt immune homeostasis and provoke a robust cellular immune response, damaging ciliary function and impeding mucus clearance—factors that contribute to airway obstruction, consolidation, and atelectasis8. Early identification and appropriate intervention are critical to preventing disease progression and serious complications.
BAL has become increasingly utilized in the diagnosis and management of pediatric MPP due to its ability to dilute and remove viscous secretions and necrotic tissue, visualize airway pathology, and collect representative pathogen samples4,9,10.
In this study, the median age of children in the BAL group was higher than that in the non-BAL group, which may be attributed to the more mature immune systems in older children, making them more prone to excessive inflammatory responses to Mycoplasma pneumoniae (MP) infection. In addition, increasing age has been associated with a higher risk of macrolide resistance11,12,13. Correspondingly, children in the BAL group exhibited higher peak temperatures, longer durations of fever and hospitalization, and significantly prolonged courses of macrolide and tetracycline antibiotic therapy. These findings suggest that persistent high fever reflects a stronger inflammatory response, and a prolonged disease course may further trigger complications such as plastic bronchitis and atelectasis, thereby increasing disease severity14.
Interestingly, the non-BAL group had higher rates of glucocorticoid use and wheezing, possibly reflecting a younger age and higher prevalence of wheezing disorders or allergic tendencies in this subgroup15. Glucocorticoids suppress pro-inflammatory cytokines (e.g., IL-1β, IL-2, IL-6, MIP-1β, IL-8) and may reduce the need for BAL in patients with milder disease or those with an allergy-related inflammatory phenotype16,17.
Inflammatory markers such as neutrophil percentage, D-dimer, and hsCRP were elevated in the BAL group, indicating more severe systemic inflammation, which markers have been previously associated with RMPP11,13,16,18,19. Although other parameters like LDH, ALT, and immunoglobulins have been proposed as severity indicators, they did not reach significance in this study, possibly due to sample or site limitations.
Bronchoscopic findings in the BAL group commonly included mucosal hyperemia, edema, follicular hyperplasia, mucus plugs, and bronchial narrowing—85% had mucus plugs and 38% had follicular changes—consistent with characteristic airway pathology of MPP4,20,21. These changes are linked to MP’s P1 protein-mediated adherence and subsequent epithelial damage and immune infiltration.
CT imaging further revealed that BAL group patients had higher rates of atelectasis and pleural effusion. Quantitative consolidation analysis using Vitrea® confirmed a significantly higher proportion of lung consolidation in the BAL group, aligning with clinical and inflammatory severity. Prior studies have successfully used CT-derived parameters in predictive models for RMPP22,23, supporting their utility in clinical assessment.
Several studies have developed models to predict the need for BAL in MPP, incorporating variables such as D-dimer, ALT, fever duration, CRP, and consolidation volume12,23,24. In this study, age, proportion of lung consolidation, hospital stay, and atelectasis were identified as risk factors, while glucocorticoid use was protective. The resulting nomogram had strong predictive power (AUC 0.86; sensitivity 0.83; specificity 0.74), and offers an intuitive tool for bedside application.
Conclusions
In a nutshell, BAL plays a crucial diagnostic and therapeutic role in children with MPP and pulmonary consolidation. The predictive model developed in this study offers a practical reference for identifying candidates for BAL, facilitating timely and individualized treatment.
Data availability
The datasets generated and/or analysed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Abbreviations
- MP:
-
Mycoplasma pneumoniae
- MPP:
-
Mycoplasma pneumoniae pneumonia
- BAL:
-
Bronchoalveolar lavage
- hsCRP:
-
hypersensitive C-reactive protein
- WBC:
-
White blood cell
- NEU%:
-
Neutrophil percentage
- Lym%:
-
Peripheral: lymphocyte percentage
- D-D:
-
D-Dimer
- ESR:
-
Erythrocyte sedimentation rate
- IgG:
-
Immunoglobulin G
- IgA:
-
Immunoglobulin A
- IgM:
-
Immunoglobulin M
- PCT:
-
Procalcitonin
- LDH:
-
Lactic dehydrogenase
- FIB:
-
Fibrinogen
- ALT:
-
Alanine aminotransferase
- OR:
-
Odd ratio
- CI:
-
Confidence interval
- ROC:
-
Receiver operating characteristic
- AUC:
-
Area under the ROC curve
References
Zhao, X. et al. Clinical characteristics and risk factors for Mycoplasma pneumoniae pneumonia in children. Front. Pead. 12, 1438631. https://doi.org/10.3389/fped.2024.1438631 (2024).
Wang, L. et al. Comparative study of diagnostic efficacy of sputum and Bronchoalveolar lavage fluid specimens in community-acquired pneumonia children treated with fiberoptic bronchoscopy. BMC Infect. Dis. 23 (1), 565. https://doi.org/10.1186/s12879-023-08522-3 (2023).
Wang, W. et al. Correlation of DNA load, genotyping, and clinical phenotype of Mycoplasma pneumoniae infection in children. Front. Pead. 12, 1369431. https://doi.org/10.3389/fped.2024.1369431 (2024).
Ling, Y. et al. Bronchoscopy improves short-term imaging improvement in segmental/lobar pneumonia: a single-center retrospective cohort study. Respir. Med. 242, 108088. https://doi.org/10.1016/j.rmed.2025.108088 (2025).
Guidelines for the diagnosis and treatment of Mycoplasma pneumoniae pneumonia in children (2023 edition). In National Health Commission of the People’s Republic of China 2023, vol. 50 79–85 (2023). https://doi.org/10.3760/cma.j.cn331340-20230217-00023.
Pediatric Respiratory Endoscopy Diagnosis and Treatment Technology Expert Group of Talent Exchange Service Center of National Health and Health Commission,Endoscopy Professional Committee of Pediatricians Branch of Chinese Physicians Association,Pediatric Respiratory Endoscopy Professional Committee of Endoscopists Branch of Chinese Physicians Association. et al. Guidelines for pediatric bendable bronchoscopy in China (2018 edition). Chin. Clin. J. Practical Pediatr. 33 (13), 983–989. https://doi.org/10.3760/cma.j.issn.2095-428X.2018.13.006 (2018).
Ding, G. et al. Challenges in the treatment of pediatric Mycoplasma pneumoniae pneumonia. Eur. J. Pediatrics. 183 (7), 3001–3011. https://doi.org/10.1007/s00431-024-05519-1 (2024).
Xue, Y., Wang, M. & Han, H. Interaction between alveolar macrophages and epithelial cells during Mycoplasma pneumoniae infection. Front. Cell. Infect. Microbiol. 13, 1052020. https://doi.org/10.3389/fcimb.2023.1052020 (2023).
Pápai-Székely, Z., Grmela, G. & Sárosi, V. Novel diagnostic processes and challenges in bronchoscopy. Pathol. Oncol. Res. 30, 1611774. https://doi.org/10.3389/pore.2024.1611774 (2024).
Hu, M. et al. Efficacy of Bronchoalveolar lavage in treating Mycoplasma pneumonia and bacterial pneumonia with atelectasis in children. Transl. Pediatr. 14 (3), 432–441. https://doi.org/10.21037/tp-2024-593 (2025).
Zhu, Y. et al. Immune response plays a role in Mycoplasma pneumoniae pneumonia. Front. Immunol. 14, 1189647. https://doi.org/10.3389/fimmu.2023.1189647 (2023).
Wang, S. Y., Zhang, W. B. & Wan, Y. Construction of a predictive model for performing Bronchoalveolar lavage in children with Mycoplasma pneumoniae pneumonia and pulmonary consolidation. Zhongguo Dang Dai Er Ke Za Zhi = Chinese. J. Contemp. Pediatr. 25 (10), 1052–1058. https://doi.org/10.7499/j.issn.1008-8830.2305113 (2023).
Cao, B. et al. Overview of antimicrobial options for Mycoplasma pneumoniae pneumonia: focus on macrolide resistance. Clin. Respir. J. 11 (4), 419–429. https://doi.org/10.1111/crj.12379 (2017).
Wen, J. et al. The combination of initial markers to predict refractory Mycoplasma pneumoniae pneumonia in Chinese children: a case control study. Respir. Res. 22 (1), 89. https://doi.org/10.1186/s12931-020-01577-9 (2021).
Chiang, L. C. et al. Prevalence and severity of symptoms of asthma, allergic rhinitis, and eczema in 10- to 15-year-old schoolchildren in central Taiwan. Asian Pac. J. Allergy Immunol. 25 (1), 1–5 (2007).
Al-Qahtani, A. A., Alhamlan, F. S. & Al-Qahtani, A. A. Pro-inflammatory and anti-inflammatory interleukins in infectious diseases: a comprehensive review. Trop. Med. Infect. Dis. 9 (1), 13. https://doi.org/10.3390/tropicalmed9010013 (2024).
Li, H. P. et al. Therapeutic agents rounding up the immunopathology of COVID-19. Therapeut. Clin. Risk Manage. 17, 657–668. https://doi.org/10.2147/TCRM.S313003 (2021).
Huang, J. J. et al. Clinical characteristics of plastic bronchitis in children: a retrospective analysis of 43 cases. Respir. Res. 23 (1), 51. https://doi.org/10.1186/s12931-022-01975-1 (2022).
Shen, F. et al. Development of a nomogram for predicting refractory Mycoplasma pneumoniae pneumonia in children. Front. Pead. 10, 813614. https://doi.org/10.3389/fped.2022.813614 (2022).
Wang, L. et al. Efficacy of fiberoptic bronchoscopy and bronchoalveolar lavage in childhood-onset, complicated plastic bronchitis. Pediatr. Pulmonol. 55 (11), 3088–3095. https://doi.org/10.1002/ppul.25016 (2020).
Ma, R. et al. Risk factor analysis of plastic bronchitis among 126 children with macrolide-resistant Mycoplasma pneumoniae pneumonia with mutations at the A2063G site after bronchoscopy examination: a nomogram prediction model. Front. Pead. 13, 1521954. https://doi.org/10.3389/fped.2025.1521954 (2025).
Cheng, Z. et al. Quantitative computed tomography of the coronavirus disease 2019 (COVID-19) pneumonia. Radiol. Infect. Dis. 7 (2), 55–61. https://doi.org/10.1016/j.jrid.2020.04.004 (2020).
Tian, H. U. et al. Study on predictive value of refractory Mycoplasma pneumonia based on quantitative CT. J. Clin. Radiol. 42 (12), 1918–1921 (2023).
Meihong, J. I. A. N. G. & Chen, Y. U. A. N. Clinical observation of fiberoptic bronchoscopy bronchoalveolar lavage in the treatment of refractory Mycoplasma pneumonia pneumonia in children. Chin. J. Gen. Pract. 23 (2), 269–272. https://doi.org/10.16766/j.cnki.issn.1674-4152.003883 (2025).
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
Ming Liang: Conceptualization, Methodology, Software, Writing - original draft, Review, & Editing. Haihong Zhang: Data curation, Writing- Original draft preparation. Yanning Li: Software, Writing- Original draft preparation. Li Li: Software, Writing- Original draft preparation. Hong Zhen: Writing- Original draft preparation. Liqin Tan: Software. Linzhen Huang: Writing- Original draft preparation. Yujun Chen: Writing- Reviewing and Editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
This was a retrospective study and thus, an ethical approval and written informed consent was waived by the Ethic Committee of the Second Affiliated Hospital of Guangxi Medical University. The study was conducted in accordance with the declaration of Helsinki.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Liang, M., Zhang, H., Li, Y. et al. A prediction model for bronchoalveolar lavage in children with Mycoplasma pneumoniae pneumonia and consolidation. Sci Rep 16, 3152 (2026). https://doi.org/10.1038/s41598-025-32941-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-32941-8
