
Abstract
Background Aggressive fluid therapy has been standard in acute pancreatitis management, but recent data favor a conservative approach. We evaluated fluid administration practices in adult acute pancreatitis patients in IMUs and ICUs from 2018 to 2022. Methods Retrospective cohort study of adult patients with acute pancreatitis admitted to multidisciplinary IMUs and ICUs in the Capital Region of Denmark (January 2018 to December 2022). Primary outcome was the total volume of fluids administered within 72 h of admission to the IMU/ICU. Secondary outcomes included the volume of intravenous (IV) IV crystalloids, non-crystalloid and non-iv fluid, as well as annual changes in fluid administration over the study period. Changes were evaluated using linear regression, adjusted for age, sex, department type, admission Ranson score, and admission creatinine level. Results A total of 382 patients were included. Over 72 h, median total fluid was 9,608 mL (IQR 6,166–12,752), comprising 3,341 mL (IQR 1,723–5,400) of IV crystalloids, 2,108 mL (IQR 1,050–3,763) of IV non‑crystalloids, and 2,450 mL (IQR 1,190–4,125) of non‑IV fluids. Fluid peaked in the first 24 h (2,000 mL crystalloid; IQR 1,000–3,200) and fell to 0 mL (IQR 0–1,000) between 48 and 72 h. From 2018 to 2022, total volumes fell non‑significantly by 345 mL/year (95% CI − 707 to 18; P = 0.062), while crystalloids declined significantly by 244 mL/year (95% CI − 482 to − 6.4; P = 0.044). Other fluid types were stable. Volume varied by vasoactive use, ventilation, etiology, and admission timing. Conclusion Patients with acute pancreatitis in the ICU/IMU receive large volumes of fluids—mainly IV crystalloids—especially during the first 24 h. While the overall fluid volume has not significantly decreased over five years, a modest reduction in crystalloid use was observed.
Similar content being viewed by others


Introduction
In Scandinavia the incidence rate of acute pancreatitis is around 40 per 100.000 persons1. Severe disease develops in approximately one third of these patients2. The mortality rate is reported to be up to 17%3. Early aggressive fluid resuscitation has been widely recommended for the management of acute pancreatitis, but evidence for this practice is limited2,4. The practice is based on the theory that pancreatic inflammation and massive release of activated pancreatic enzymes results in systemic inflammation and endothelial damage with loss of fluid to the interstitial space leading to hypovolemia. This results in decreased perfusion of the pancreas which increases the risk of pancreatic necrosis5. Fluid resuscitation is thought to correct tissue hypoperfusion by counteracting the pancreatic and systemic microcirculation impairment6. However, this comes at a cost with increased risk of fluid accumulation and overhydration, that has been associated with organ failure and death7.
Over the recent years there has been a trend towards more restrictive fluid administration strategies based on observations of no difference between liberal versus standard fluid strategies, and more recently standard versus restrictive fluid strategies8,9. Further, it has recently been demonstrated that a more restrictive fluid approach to patients with pancreatitis may also be beneficial10. It is however unknown how the current fluid administration strategy is among patients admitted with acute pancreatitis to ICU/IMU units, and what the potential for improvement in care is for this population.
The aim of the present study was to determine the current standard of care with regards to administration of fluid in adult patients with acute pancreatitis admitted to intermediate care units (IMUs) and intensive care units (ICUs), and whether this has changed during the past five years.
Methods
Study design
The present study was a retrospective cohort study. The study was approved by the Regional Board of Health in the Capital Region of Denmark (no.: R-22074321 on the 27th January 2023) and submitted to the Danish Agency for data protection. Due to the retrospective nature of the study, it had no consequences for the involved patients and the need for individual patient consent was therefore waived by the Regional Health Research Ethics Committee in the Capital Region of Denmark Journal no.: F-25,011,203. All methods were carried out in accordance with relevant guidelines and regulations. The study protocol followed the STROBE statement11.
Setting
Patient data were collected from all multidisciplinary IMUs and ICUs in the Capital Region of Denmark from January 2018 to December 2022. This includes five hospitals with ICUs and three with IMUs.
Patients
Patients who were ≥ 18 years and registered with the diagnosis of acute pancreatitis (ICD-10 DK85.x) upon or during admission to the IMU or ICU were included. Patients transferred from other regions to the Capital Region for continued or more specialized treatment of acute pancreatitis were excluded. The diagnosis of acute pancreatitis was at the discretion of the attending physicians and the common guideline in the Capital region defined this according to the Revised Atlanta Classification which requires meeting two of the following three criteria: typical abdominal pain, serum amylase or lipase level higher than 3 times the upper limit of the normal range, or signs of acute pancreatitis on imaging12.
Data sources
Patient characteristics and volumes of fluid administration were collected from the electronic health record (Sundhedsplatformen by EPIC). All data were entered as a part of daily clinical practice. The data of administered fluids was entered directly into the electronic patients charts primarily by nursing staff, except medicine administered via pumps where the volume data was transferred directly from the pump.
Outcomes
All outcomes and analyses were defined a priori. The primary outcome was the total volume of fluids administered from admission to 72 h after admission to the IMU or ICU in patients with acute pancreatitis from 2018 to 2022 and whether this changed over the corresponding five years. The total fluid volume included all IV fluids (crystalloids, colloids, glucose, blood products, medicine water and nutrition), enteral medicine and water and oral liquids. We collected all available data from 0 to 72 h of ICU/IMU admission independently of whether patients were transferred to another unit or ward.
The secondary outcomes included the total volumes of IV crystalloid, non-crystalloid and non-iv administered between 0 and 72 h of IMU or ICU admission, the total volume of all fluid categories, IV crystalloid and non-crystalloid fluids and non-iv fluid administered between 0 and 24 h, 24–48 h and 48–72 h after IMU or ICU admission.
Statistical analysis
Categorical variables are presented as numbers (n) and percentages (%) and differences between strata were compared with the Chi-Square test or nonparametric tests as appropriate. Continuous variables are presented as mean ± standard deviation (SD) if normally distributed or as median (interquartile range, IQR) if skewed and differences between strata were compared with the Student’s t-test or the Mann-Whitney U test as appropriate. Baseline characteristics include predictors of severity with a CRP > 150 mg/L or Glasgow score > 2 after 48 h indicating complication13,14. Changes in volumes over time were analyzed in a linear regression model with fluid volume as the dependent variable and year as the explanatory variable. These were adjusted for the confounding factors age, sex, department type, admission component of Ranson score and creatinine concentration. Prespecified exploratory subgroup analyses of the primary outcome were performed to determine the influence of: severity (defined as severe if Ranson score > 2)12, etiology (most commonly gallstones and alcohol), age > 65 years, Body Mass Index (BMI) > 30, respiratory support (non-invasive and invasive mechanical support), treatment with vasoactive medicine (norepinephrine or/and dopamine), acute kidney injury (defined as stage 3 or more on a modified Kidney Disease: Improving Global Outcomes)15, unit type stay (IMU or ICU), cumulative fluid volume more or less than 5 L (L) before IMU/ICU admission and IMU/ICU admission in or after 5 days from hospital admission. The subgroups were analyzed by including an interaction term between year and subgroup variable, and also adjusted for confounding factors age, sex, department type, admission component of Ranson score and creatinine concentration. All tests were two-sided with a significance level of 0.05. Statistical analyses were done with the newest version (4.4.2.) of R.
Results
A total of 382 patients were included in the study. The median age was 64 years (IQR 50–75), and 60% were men, Table 1. A total of 193 (51%) patients were admitted to the IMU and 130 (34%) to the ICU, with the remainder having a combined unit stay within the first three days. The primary cause of IMU/ICU admission was respiratory distress. The primary causes of acute pancreatitis were gallstones in 28% of patients and alcohol in 25%. Mild disease, corresponding to a Ranson score of less than 3, was observed in 52% of patients upon ICU/IMU admission, while the remainder had moderate or severe disease. In 86% of patients, the Glasgow score was greater than 2, indicating a high risk of developing severe acute pancreatitis, Table 1. The median time from hospital admission to IMU/ICU admission was two days (IQR 1–7). During this period, patients received a median of 2,482 mL of fluid (IQR 1,000–3,875 mL), of which intravenous crystalloid constituted a median 1,000 mL (IQR 0–2,837 mL), Fig. 1 and supplemental Table 1.

The volumes of total fluid, iv fluids and iv crystalloids across different time periods of admission.
Upon arrival at the ICU/IMU, the median total volume of fluid administered within the first 72 h was 9,608 mL (IQR 6,166–12,752 mL). Of this, IV crystalloids accounted for a median of 3,341 mL (IQR 1,723–5,400 mL), IV non-crystalloid fluids for a median of 2,108 mL (IQR 1,050–3,763 mL), and non-IV fluids for a median of 2,450 mL (IQR 1,190–4,125 mL), Fig. 1 and supplemental Table 1.
Most of the fluid was administered during the first 24 h. The peak IV crystalloid administration occurred during the first 24 h, with a median of 2,000 mL (IQR 1,000–3,200 mL), decreasing to a nadir between 48 and 72 h at a median of 0 mL (IQR 0–1,000 mL) (Fig. 1). Likewise, although less pronounced, IV non-crystalloid fluid decreased from a median of 800 mL (IQR 400–1,517 mL) during the first 24 h to a median of 522 mL (IQR 0–1,226 mL) between 48 and 72 h. However, there was no difference in non-IV fluid administration (Fig. 1) and (supplemental Table 1).
In exploratory subgroup analyses, we found heterogeneity in the total volume of fluid administration during the first 72 h with more fluid administered to patients treated with vasoactive medication (P for interaction = 0.004) and those with less than five days from hospital admission to ICU admission (P for interaction = 0.012), supplemental Fig. 1. Likewise, we found substantial heterogeneity for IV crystalloid volumes with more fluid administered to patients not treated with mechanical ventilation (P for interaction = 0.030) and those with less than five days from hospital admission to ICU admission (P for interaction < 0.001). We also found heterogeneity in those treated with and without vasoactive medication (P for interaction < 0.001) and with different pancreatitis etiologies (P for interaction = 0.035), but the fluid administration patterns within these subgroups were more complex, supplemental Fig. 2. For the IV non-crystalloid volume, we found that more fluid was administered to patients treated with mechanical ventilation (P for interaction < 0.001) and with vasoactive medication (P for interaction < 0.001), supplemental Fig. 3. For the non-IV volumes, we only found that more fluid was administered to patients not treated with mechanical ventilation (P for interaction = 0.023), supplemental Fig. 4.

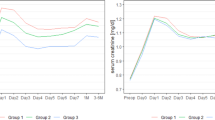
The volumes of total fluid, iv fluids and iv crystalloids across the years 2018-2022
During the years 2018–2022, the median total volume of fluid administered did not decrease (change of − 345 mL per year [95% CI − 707 to 18; P = 0.062]). However, there was a decrease in IV crystalloid administration (change of − 244 mL per year [95% CI − 482 to − 6.4; P = 0.044]), Fig. 2; Table 2. There was no change in non-IV fluid or IV non-crystalloid fluid administration, Table 2; Fig. 2. We observed no heterogeneity between subgroups regarding the change in fluid administration over the period for total fluid, non-IV fluid, IV crystalloid, or IV non-crystalloid fluids (Supplemental Figs. 5–8).
In exploratory analyses we consistently found that increased intravenous fluid was associated with decrease survival, supplemental Table 2.
Discussion
In this study of patients with acute pancreatitis, patients received large fluid volumes—primarily intravenous crystalloids—within the first 72 h of IMU/ICU admission, with the highest volumes given during the first 24 h. Fluid administration practice varied according to disease severity, the use of vasoactive medication or mechanical ventilation, and the timing of IMU/ICU admission, although the results from these analyses should be considered exploratory due to the limited sample size. Over the study period (2018–2022), total fluid volumes did not decrease, although there was a modest decline in intravenous crystalloid use.
Despite lacking evidence for benefit, aggressive fluid resuscitation has been a cornerstone of pancreatitis treatment for many years16. Unsurprisingly fluid overload is a common complication in this population17. The consequences of fluid overload are well described and include global edema involving all organs, and has been proposed to be a leading cause of organ dysfunction and increased mortality in critical illness in general and pancreatitis specifically18. It is however notoriously difficult to determine the causality based on observational data. Nevertheless, recent studies in septic shock indicate that a conservative fluid strategy may be beneficial especially in ventilated patients, but whether this translate into a reduced mortality is unclear8,9,19. Likewise, in patients with pancreatitis a more conservative strategy seem to improve outcome10. Although there are no available data to support this claim, we speculate that a more conservative approach to fluid therapy is emerging - especially resuscitation fluid in the critically ill patients. Although we did not find a decline in the overall fluid administration, the reduction in crystalloid use – the primary resuscitation fluid - is in line with this.
The variation in subgroups should be interpreted with caution due to the modest sample size. However, it is worth noticing that within patients with pancreatitis admitted to ICU/IMU there is substantial variation in severity and that this seems to affect decisions regarding fluid administration. When designing trials of shock treatment that include these patients this variation should be taken into account, i.e. separate protocol for patients with and without need for vasoactive medication and for early vs. late admission during hospitalisation.
Based on the data from the present study, it would seem that there is still potential for a more rational use of fluid in pancreatitis patients with organ failure, and that the majority of fluid is still administered after ICU/IMU admission. Especially, crystalloid administration should be considered, but also other fluid types not administered as resuscitation fluids are administered in large quantities. In a recent multicenter randomized study, protocolized reduction of non-resuscitation fluids in patients with septic shock resulted in a large decrease in fluid administration compared with usual care20. They define non-resuscitation fluids as all other fluids, such as vehicles for nutrition and medication, as well as fluids given to correct electrolyte disturbances and to ensure adequate hydration. A trial using this design to test if reducing non-resuscitation fluids improves outcomes is missing.
Strengths and limitations
A strength of the study is the access to data from electronic health records, which reduces the possibility of missed/incorrect data. There is however always a risk of information bias in both identification of cases as well as missing data or erroneous data entry into the EHR. To further minimize accidental inclusion of patients, who did not meet the inclusion criteria, the extracted patient list was manually screened for exclusion criteria and primary IMU/ICU admission cause. A limitation in using extracted data from Sundhedsplatformen, is that registration of fluid may differ between departments and staff members, which poses a certain degree of result uncertainty. Another limitation is that not all the included hospitals have an IMU, which contributes to selection bias. Finally, we used total fluid volume as the primary outcome. Fluid balance may have been a more relevant primary outcome seen from a daily clinical perspective. However, this approach would likely have been more prone to influence by the above uncertainty that comes with potential differing fluid registration.
Taken together there is evidence to support a randomized controlled trial of restricted fluid therapy in pancreatitis, that focuses not solely on resuscitation fluids but at a more general approach to fluid therapy.
Conclusion
Patients with acute pancreatitis in the ICU/IMU receive large volumes of fluids—mainly IV crystalloids—especially during the first 24 h. While the overall fluid volume has not decreased over five years, a reduction in crystalloid use was observed.
Data availability
The data for the present analysis is avaliable from the corresponding author upon reasonably request and subject to national and international law and data protection.
References
Halvorsen, F. A. & Ritland, S. Acute pancreatitis in Buskerud County, Norway. Incidence and etiology. Scand. J. Gastroenterol. 31, 411–414 (1996).
Gardner, T. B. Fluid resuscitation in acute pancreatitis - going over the WATERFALL. N Engl. J. Med. 387, 1038–1039 (2022).
Whitcomb, D. C. Clinical practice. Acute pancreatitis. N Engl. J. Med. 354, 2142–2150 (2006).
Zhou, S. et al. Comprehensive meta-analysis of randomized controlled trials of lactated ringer’s versus normal saline for acute pancreatitis. Pancreatology 21, 1405–1410 (2021).
Gardner, T. B., Vege, S. S., Pearson, R. K. & Chari, S. T. Fluid resuscitation in acute pancreatitis. Clin. Gastroenterol. Hepatol. 6, 1070–1076 (2008).
Garg, P. K. & Singh, V. P. Organ failure due to systemic injury in acute pancreatitis. Gastroenterology 156, 2008–2023 (2019).
Di Martino, M. et al. Systematic review and meta-analysis of fluid therapy protocols in acute pancreatitis: type, rate and route. HPB (Oxford). 23, 1629–1638 (2021).
Meyhoff, T. S. et al. Restriction of intravenous fluid in ICU patients with septic shock. N Engl. J. Med. 386, 2459–2470 (2022).
Angus, D. C. et al. A systematic review and meta-analysis of early goal-directed therapy for septic shock: the ARISE, process and promise investigators. Intensive Care Med. 41, 1549–1560 (2015).
de-Madaria, E. et al. Aggressive or moderate fluid resuscitation in acute pancreatitis. N Engl. J. Med. 387, 989–1000 (2022).
von Elm, E. et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 370, 1453–1457 (2007).
Banks, P. A. et al. Classification of acute pancreatitis–2012: revision of the Atlanta classification and definitions by international consensus. Gut 62, 102–111 (2013).
Working Party of the British Society of Gastroenterology. Association of surgeons of great Britain and Ireland, pancreatic society of great Britain and Ireland & association of upper GI surgeons of great Britain and Ireland. UK guidelines for the management of acute pancreatitis. Gut 54 (Suppl 3), iii1–9 (2005).
Jones, M. J., Neal, C. P., Ngu, W. S., Dennison, A. R. & Garcea, G. Early warning score independently predicts adverse outcome and mortality in patients with acute pancreatitis. Langenbecks Arch. Surg. 402, 811–819 (2017).
Kellum, J. et al. KDIGO clinical practice guideline for acute kidney injury. Kidney Int. Supplements. 2, 1–138 (2012).
Haydock, M. D. et al. National survey of fluid therapy in acute pancreatitis: current practice lacks a sound evidence base. World J. Surg. 37, 2428–2435 (2013).
de-Madaria, E. et al. Influence of fluid therapy on the prognosis of acute pancreatitis: a prospective cohort study. Am. J. Gastroenterol. 106, 1843–1850 (2011).
Wang, N. et al. Fluid balance and mortality in critically ill patients with acute kidney injury: a multicenter prospective epidemiological study. Crit. Care. 19, 371 (2015).
National Heart, Lung, and Blood Institute Prevention and Early Treatment of Acute Lung Injury Clinical Trials Network. Early restrictive or Liberal fluid management for sepsis-induced hypotension. N Engl. J. Med. 388, 499–510 (2023).
Lindén, A. et al. Protocolized reduction of non-resuscitation fluids versus usual care in septic shock patients (REDUSE): a randomized multicentre feasibility trial. Crit. Care. 28, 166 (2024).
Author information
Authors and Affiliations
Contributions
T.S.I. and J.L. Designed the study. T.S.I. and J.L. and M.I. ascertained and validated data. T.S.I. and J.L. and M.I. analysed and drafted the main manuscript. All authors critically revised and approved the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study was retrospective and proved by the health board the capital region of Denmark. Nr. R-22074321 The need for individual patient consent was waived.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.








Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Lacoppidan, J., Tholin, M.W., Kristiansen, K.T. et al. Fluid resuscitation practice in patients with acute pancreatitis in Danish intermediate and intensive care units - a retrospective cohort study. Sci Rep 16, 4006 (2026). https://doi.org/10.1038/s41598-025-34038-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-34038-8

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}