
Abstract
This paper develops a scale to measure the healing tourism experiences, drawing on grounded theory and extant relevant literature. In Study 1, 30 in-depth interviews with purposive sampling were conducted to establish a conceptual model comprising four dimensions: anticipated healing, embodied healing, interactive healing, and reminiscence healing. Study 2 applied multivariate statistical analyses to refine the scale, and based on 280 valid questionnaires, developed a 13-item instrument representing the four dimensions. Study 3 further tested the validity and applicability of the scale using data from Study 2, confirming its reliability and predictive power. Study 4 was subsequently conducted to validate the model’s predictive utility by testing the relationship between healing tourism experiences and tourists’ willingness to revisit, thereby confirming the criterion-related validity of the scale. The findings contribute both theoretically and practically: the scale offers a robust measurement standard for scholars to investigate the healing tourism experiences in greater depth, and it provides a theoretical reference for practitioners seeking to evaluate and enhance the restorative value of tourism products and services.
Similar content being viewed by others

Introduction
Tourism can enhance harmony in interpersonal relationships, satisfy the pursuit of freedom and tranquility, and thus deepen one’s understanding of life1,2. The Global Wellness Institute (GWI) has identified 11 principal categories within the healing economy, including wellness tourism, sports and fitness, spas, mental health, and more. As reported by the GWI, the healing tourism market accounted for 18% of the global tourism industry in 2019, and it’s expected that the global healing economy will expand by approximately 10% annually, reaching a market size of US$7 trillion by 2025. Several countries and regions are proactively capitalizing on this growth opportunity, pursuing innovative avenues for the advancement of healing tourism. This phenomenon reflects the continued rise in the pursuit of health and well-being3,4.
In recent years, there has been a growing body of research examining the healing effects of tourism activities, encompassing a diverse range of topics such as wellness tourism, health tourism, and medical tourism. Prior research has indicated that tourism can enhance perceptions of health, facilitate emotional healing, promote physical relaxation, relieve psychological stress, and ultimately contribute to feelings of emotional well-being and inner peace5,6. Furthermore, the healing experience serves as a significant motivator for tourists to temporarily detach from their daily lives and alleviate stress, thereby enhancing their well-being and influencing their behavioral intentions7,8. Although both qualitative explorations and several scale-based studies have examined tourism’s restorative outcomes, the conceptualization of the healing tourism experiences remain fragmented. Prior scales often focus on wellness or resort-specific contexts, without providing a comprehensive framework that integrates psychological, emotional, and embodied aspects across the entire travel process. Moreover, existing models rarely clarify the structural relationships among these dimensions, limiting their explanatory and practical applicability.
To address these gaps, this paper employs a mixed-methods approach to conceptualize and measure the healing tourism experiences, which is defined as the psychological, emotional, sensory, and social restorative processes occurring before, during, and after travel. This definition positions healing not as a vague effect but as a structured, multidimensional construct embedded in the tourist journey.
The objectives of this study are threefold. First, it aims to develop a theoretically grounded scale that captures the multidimensional structure of the healing tourism experiences. Second, it seeks to empirically validate the reliability and validity of the proposed dimensions. Third, it explores the relationship between healing tourism experiences and behavioral outcomes, particularly revisit intention. These objectives give rise to the following research questions: What are the key dimensions of healing tourism experiences? How can they be validly measured? And how do they influence tourists’ behavioral intentions?
Literature review
Conceptualizing tourist experiences
Essence and definitions
The tourist experiences constitute the conceptual foundation of tourism studies and have been examined through multiple disciplinary perspectives9. Early research emphasized behavioral aspects, viewing tourism as a sequence of activities and responses shaped by tourists’ participation and perceptions10,11. With the emergence of the experience economy, scholars began to highlight affective, cognitive, and sensory elements, framing tourism as an authentic, meaningful, and transformative encounter12,13,14. Definitions vary from describing tourism as “enjoyable, memorable, and engaging” to positioning it as a search for authentic, multisensory, and transformative experiences15,16.
Four core dimensions
The tourist experiences are typically conceptualized through four interrelated dimensions: affective, cognitive, behavioral, and sensory17,18,19. Affective experiences involve emotional responses such as joy, surprise, or nostalgia20. Cognitive experiences refer to the intellectual engagement with destinations, including knowledge acquisition and cultural understanding21,22. Behavioral experiences encompass concrete actions such as sightseeing or shopping23. Sensory experiences encompass the full range of sensations-sight, sound, smell, taste, and touch-that shape perceptions of place24. Collectively, these dimensions provide a framework for understanding how tourists construct and evaluate their experiences.
Conceptualizing healing in interdisciplinary contexts
Healing is a multidimensional construct that has been examined across psychology, medicine, environmental research, and the arts. Each discipline emphasizes different pathways and mechanisms of recovery, yet they converge on several core processes that are transferable to tourism contexts.
In psychology, therapeutic models such as dialectical behavior therapy, compassion-focused therapy, and mindfulness-based interventions highlight the role of emotional regulation, cognitive reframing, and resilience building25,26. These approaches demonstrate that healing is not merely the reduction of symptoms but a process of regaining balance, reframing negative experiences, and cultivating adaptive coping strategies.
In the field of medicine, complementary and alternative therapies such as yoga, meditation, acupuncture, and energy-based healing emphasize the integration of mind and body. These practices illustrate how embodied engagement-through breathing, movement, or energy flow-can alleviate stress, improve physical vitality, and foster holistic well-being27,28. Such insights underline that healing involves both physiological recovery and psychological renewal.
Environmental psychology contributes through attention restoration theory and biophilia perspectives, emphasizing that natural environments reduce stress, restore directed attention, and promote relaxation29,30. Mechanisms such as sensory immersion and restorative attention explain why forests, oceans, and mountains are frequently described as therapeutic spaces, offering both immediate psychological relief and longer-term benefits to mental health.
Art and narrative therapies further expand the scope of healing by underscoring the importance of symbolic expression and meaning-making. Engagement with music, painting, literature, or storytelling provides opportunities for individuals to externalize emotions, reconstruct identity, and generate new perspectives on life challenges31,32. Healing here emerges from the process of creative expression and reflective interpretation.
Synthesizing across these fields, healing can be understood as a dynamic process encompassing emotional regulation, cognitive reframing, embodied practices, sensory immersion, and symbolic expression. While these mechanisms originate in clinical or therapeutic contexts, they are equally relevant to tourism, where immersive environments, embodied practices, and reflective encounters can generate both short-term psychological restoration and long-term well-being outcomes.
Healing in tourism research
Wellness tourism
Wellness tourism encompasses activities such as spa treatments, yoga retreats, meditation programs, and other holistic health services that explicitly target physical and psychological well-being. Scholars argue that wellness tourism is often motivated by the desire to reduce stress, improve vitality, and restore inner balance in response to the demands of modern life33. Empirical studies show that such experiences provide immediate relief, including lowered physiological stress levels, enhanced relaxation, and improved mood5. However, most research in this area is context-specific, focusing on particular facilities or retreat settings. As a result, wellness tourism is often framed in terms of short-term benefits, and limited attention has been given to how such experiences may contribute to long-term behavioral change or sustained well-being. The emphasis on relaxation and bodily restoration, while important, represents only one facet of healing in tourism.
Nature therapy and ecotourism
Nature-based tourism has been widely studied for its restorative properties, particularly through the lenses of attention restoration theory and stress recovery frameworks29,30. Experiences such as forest bathing, mountain hiking, and coastal ecotourism have been shown to reduce mental fatigue, improve concentration, and promote feelings of tranquility. These activities immerse tourists in natural environments, engaging multiple senses and encouraging a state of mindfulness. In the short term, exposure to nature reduces stress and enhances positive affect, offering compelling evidence for tourism’s therapeutic value. Yet, the literature tends to emphasize momentary psychological restoration rather than exploring how nature-based experiences may foster deeper lifestyle changes, environmental values, or sustained improvements in well-being. Consequently, the longitudinal effects of ecotourism remain underexplored.
Pilgrimage and spiritual tourism
Pilgrimage and spiritual tourism foreground the symbolic, ritualistic, and existential aspects of travel. Participation in religious journeys or sacred site visits is often linked to processes of meaning-making, ritual engagement, and identity transformation34. Such experiences provide not only immediate relief from personal struggles but also a sense of spiritual renewal, forgiveness, or transcendence that can endure long after the journey has ended. Research suggests that spiritual tourism contributes to sustained psychological well-being by fostering a sense of belonging, connectedness, and existential clarity35. However, despite the rich theoretical insights, empirical research in this domain often remains descriptive. Few validated measurement instruments exist to systematically assess the healing outcomes of pilgrimage, making it difficult to compare across contexts or to integrate these insights with broader models of tourism experiences.
Transformative and liminal tourism
Transformative tourism frames healing as part of broader processes of personal growth, identity reconstruction, and value reorientation. Central to this perspective is the notion of liminality-an in-between state where ordinary roles and routines are suspended, enabling reflection and experimentation with new ways of being36. Travel in liminal contexts, such as retreats, adventure expeditions, or volunteer tourism, can catalyze profound shifts in worldview and self-concept14. These experiences highlight healing not merely as symptom relief but as a deeply transformative process that shapes personal narratives and future life trajectories. Despite its conceptual richness, however, research in this area remains largely theoretical. There is a lack of empirically validated tools to measure how transformative or liminal experiences translate into sustained healing outcomes, leaving this stream of literature underdeveloped in practical terms.
Gaps and contributions
Existing research across psychology, medicine, environmental studies, and tourism has provided valuable insights into the multifaceted nature of healing. Interdisciplinary studies highlight key mechanisms such as emotional regulation, cognitive reframing, embodied practices, sensory immersion, and symbolic expression, while tourism research demonstrates how these processes manifest in wellness retreats, nature-based experiences, pilgrimages, and transformative journeys (see Table_1).
Importantly, these streams of research are not fully aligned. For example, Attention Restoration Theory30 conceptualizes healing primarily as a short-term recovery of directed attention through exposure to restorative environments, whereas transformative experience theory36 emphasizes long-term processes of identity reconstruction and existential growth. The temporal gap between momentary psychological restoration and enduring personal transformation has rarely been addressed in an integrative framework. By situating healing tourism experiences as a continuum that bridges these temporal dimensions, this study addresses a fundamental theoretical tension rather than merely proposing a novel construct.
Despite these contributions, several gaps remain. First, current conceptualizations of healing in tourism are fragmented across wellness, ecological, spiritual, and transformative domains, resulting in a lack of integrative theoretical frameworks. Second, the majority of empirical work focuses on short-term outcomes such as stress relief or mood enhancement, while sustained healing processes linked to identity change, meaning-making, or lifestyle reorientation remain underexplored. This imbalance further underscores the need for a model that incorporates both immediate restoration and long-term transformation within a single conceptual continuum. Third, while prior research has employed descriptive or context-specific scales, few studies have anchored measurement development in established psychometric traditions. Classic works on construct development37 and item purification38 emphasize systematic item generation, content validity assessment, and iterative refinement. By explicitly aligning with these methodological standards, the present study not only introduces a new construct but also situates its measurement within a recognized scholarly tradition, thereby strengthening both rigor and credibility. Finally, existing scales are typically context-specific and descriptive, offering limited capacity to measure the structural interrelations among healing dimensions across diverse tourism settings. Few studies combine qualitative and quantitative methods in a way that allows both theory building and robust validation of measurement instruments.
This study addresses these gaps by developing and validating a multidimensional scale of the healing tourism experiences. Drawing on grounded theory and interdisciplinary insights, the scale integrates both immediate and enduring healing outcomes and captures their interrelationships. Methodologically, it advances beyond descriptive accounts by combining qualitative conceptualization with rigorous quantitative testing. Theoretically, it clarifies the structure of healing experiences within tourism. Practically, it provides a diagnostic tool that can guide destination managers and practitioners in designing and evaluating health-oriented products and services.
Conceptual boundary of healing tourism experiences
Although “healing tourism” has often been discussed interchangeably with wellness, restorative, and transformative tourism, its conceptual boundaries remain insufficiently defined. To clarify these distinctions, this study positions healing tourism experiences as a temporally extended and psychologically integrated process that unfolds across three sequential phases-anticipation (pre-tourism), embodied and interactive engagement (in-tourism), and reminiscence (post-tourism). This perspective emphasizes healing as an ongoing trajectory of emotional regulation, sensory immersion, social connectedness, and reflective meaning-making that collectively contribute to sustained well-being.
In contrast, wellness tourism primarily centers on service-based treatments (e.g., spas, yoga retreats, and detox programs) designed to improve physical or psychological health within bounded temporal settings. Restorative tourism focuses on short-term psychological and sensory recovery, often through contact with natural environments or leisure contexts that replenish depleted cognitive and emotional resources. Transformative tourism, meanwhile, underscores identity change and value reorientation through deeply reflective or liminal experiences that catalyze long-term personal growth.
Therefore, while wellness and restorative tourism emphasize immediate relief or bodily restoration, and transformative tourism stresses self-transcendence and existential change, healing tourism experiences integrate these outcomes within a continuous, multidimensional process that bridges transient recovery and enduring psychological balance.
Methodology and results
In this study, the healing tourism experiences are defined as the comprehensive psychological process in which tourists, throughout the entire travel cycle-before, during, and after the tourism-perceive emotional restoration, stress alleviation, and inner growth. These effects are not restricted to individuals who intentionally participate in healing tourism but may arise from a wide range of tourism contexts. To investigate these effects, this research integrates grounded theory with quantitative validation techniques. Grounded theory is employed because the conceptual framework of healing effects remains underdeveloped; it allows theoretical categories to emerge inductively when pre-existing models do not adequately explain the phenomenon39. Complementing this, statistical analyses-including exploratory and confirmatory factor analysis-enable rigorous assessment of measurement validity and predictive relationships40. Following best practices in scale development41,42, the study combines qualitative item generation, quantitative item purification, and structural validation to enhance both reliability and generalizability.
This paper is grounded in Likert’s43 classic theory to construct the scale. Among other things, according to the scale development process, this paper constructs dimensions to measure the healing tourism experiences according to the standardized and rigorous data processing steps such as data cleaning, three.
-level coding (open coding, axial coding, and selective coding), and conceptual construction44,45.

Research Design during the Scale Development Stage.
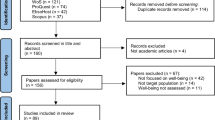
Study 1 employs offline in-depth interviews to explore the healing tourism experiences. Participants were recruited through purposive sampling to ensure that they had experienced tourism activities perceived as restorative or healing. A portion of the collected data is analyzed with grounded theory to identify conceptual structures, develop measurement items, and construct a theoretical model, while the remaining data is used for saturation testing. Study 2 utilizes multivariate statistical analyses to refine and validate scales for measuring the healing effects identified in Study 1. This phase includes item refinement, content validity assessments through online questionnaires, and integration of existing literature definitions. Study 3 built on Study 2 by conducting confirmatory factor analysis (CFA) to evaluate the structural validity and practical applicability of the scale. This phase reinforces the scientific credibility of the scale and provides substantial evidence for its effectiveness in real-world applications. Study 4 was subsequently conducted to validate the model’s predictive utility, focusing on the relationship between healing tourism experiences and tourists’ willingness to revisit. This phase tested criterion-related validity through structural equation modeling, confirming that the scale not only demonstrates strong psychometric properties but also possesses behavioral significance. To enhance clarity, Figure_1 presents a flowchart of the research design.
Study 1: item generation
To gain a deeper understanding of the factors contributing to the healing tourism experiences and ensure the comprehensiveness and depth of the material, this paper uses offline in-depth interviews for data collection. Thirty participants were recruited through purposive sampling, ensuring that they had engaged in tourism activities perceived as restorative. All participants were Chinese nationals with variation in age, gender, and occupation (e.g., private-sector employees, freelancers, and tour guides). The interview was conducted in Mandarin, allowing the interviewee to express their experiences in their native language. Each interview lasts between 30 and 60 min, and all interviews are audio-recorded with the participants’ consent. To account for differing perceptions of tourism retreats, the study balances the individual characteristics of the interviewees, such as gender and age, to eliminate potential bias.
To enhance methodological rigor and transparency, researchers were jointly trained in grounded theory coding procedures following Strauss and Corbin’s46 guidelines. Before formal coding, researchers independently analyzed two pilot transcripts to develop a shared understanding of the coding framework. Inter-coder reliability was assessed using 20% of the transcripts, yielding a Cohen’s Kappa of 0.75, which indicates substantial agreement. Coding discrepancies were resolved through iterative discussion until full consensus was achieved.
After academic discussions and expert consultations, the core interview questions are finalized as follows: (1) How did your feelings or expectations before the trip influence your experience? (2) Can you describe two or three travel moments where you felt emotionally restored? (3) How did traveling improve your social relationships? (4) How does recalling a travel experience affect your current life or work? The interview protocol is presented in Appendix A.
Following the interviews, the audio recordings are transcribed and carefully reviewed. Responses deemed too simple or irrelevant are excluded, leaving over 100,000 words of text. A random sample of 25 interviews is selected to build the theoretical model, while the remaining interviews are used for saturation testing. These interviews are coded and analyzed using grounded theory, following the stages of open coding, axial, and selective coding. Any discrepancies in coding are resolved through discussions among the researchers to ensure consistency. Following Bowen’s47 approach, theoretical saturation was reached after 25 interviews, and five additional interviews were analyzed to confirm that no new categories or conceptual properties emerged.
To strengthen the credibility of the qualitative findings and demonstrate the organic emergence of themes, representative quotations from participants were incorporated into the analysis. Participants’ narratives vividly captured the four identified dimensions of healing tourism experiences. For example, one respondent articulated anticipated healing by noting that “planning the trip made me feel hopeful during a stressful work week,” highlighting the restorative effect of positive expectations before travel. Another participant described embodied healing through sensory immersion, stating that “when I stood by the seaside, the sound of waves and the scent of salt air made me feel completely calm.” Similarly, interactive healing was reflected in the words, “talking with local residents made me realize how kindness itself can heal,” emphasizing the role of social interaction and empathy in emotional recovery. Finally, reminiscence healing was expressed through reflection on post-travel memories: “looking back at the travel photos helps me regain strength when life feels heavy.” Collectively, these quotations illustrate that the four themes-anticipated, embodied, interactive, and reminiscence healing-emerged inductively from participants’ lived experiences rather than being imposed post hoc, thereby reinforcing the authenticity and empirical credibility of the qualitative phase.
To guarantee the precision of data tracking, the study is encoded sequentially according to the order of interviews and the chronological progression of initial concepts. This process yields 143 initial concepts, which are further compared and refined into 13 subcategories. These subcategories, deemed highly relevant to tourists’ healing experiences, are ultimately consolidated into four main categories: anticipated healing (3 statements), embodied healing (5 statements), interactive healing (3 statements), and reminiscence healing (2 statements) (see Table_2).

Conceptual model.
Tourism activities can be divided into three phases: pre-tourism, in-tourism, and post-tourism51. Based on prior literatures, this study suggests that the healing impact of tourism spans across all phases52. Through repeated comparisons, this study develops a conceptual model of the healing tourism experiences consisting of four categories: anticipated healing, embodied healing, interactive healing, and reminiscence healing (see Figure_2).
In comparison to previous studies, this study introduces a new dimension-anticipated healing, which adds a novel perspective to the theoretical framework of this field. Drawing on psychological expectancy theory, this dimension suggests that positive expectations about upcoming experiences can strengthen inner resilience and reduce stress53, and prior research further indicates that individuals with optimistic expectations are more likely to undergo restorative processes, thereby alleviating present anxiety54. Importantly, the emergence of anticipated healing complements the other three dimensions-embodied, interactive, and reminiscence healing-to form a continuum across the temporal stages of tourism. Anticipated healing shapes travelers’ mindsets before departure, providing psychological readiness that facilitates embodied experiences on-site. These embodied encounters, in turn, often serve as a basis for interactive healing, where social bonds are formed and reinforced. Subsequently, both embodied and interactive experiences provide the raw material for reminiscence healing, in which reflection and memory consolidation extend the restorative benefits into post-tourism life. This interconnected framework resonates with affective forecasting research, which links expectations to emotional outcomes; with social bonding theory, which underscores the restorative role of interpersonal ties; and with autobiographical memory studies, which highlight the long-term effects of reflective recall. Together, these perspectives illustrate that the four dimensions are not discrete categories but mutually reinforcing processes that collectively explain how tourism fosters psychological well-being and recovery.
Study 2: purification of measures
Building on the qualitative results of Study 1 and insights from existing literature, an initial pool of 39 measurement items was generated. After expert review for content validity, 36 items were retained. To validate the structure of these dimensions, exploratory factor analysis is used. Participants rate the items on a scale from 1 (strongly disagree) to 7 (strongly agree) based on their perceptions of tourism’s healing effects. Data is collected via the Credamo platform, with 300 questionnaires distributed. After removing invalid responses, 280 valid ones remained, with 91 male participants, primarily aged 21–30, from various sectors.
SPSS 27.0 (https://www.ibm.com/products/spss-statistics) is used to analyze the data. First, preliminary tests confirmed data suitability for factor analysis. The KMO value was 0.858, and Bartlett’s test of sphericity was significant (χ2 = 3527.125, P < 0.001). Then exploratory factor analysis (EFA) was conducted using oblique rotation rather than orthogonal rotation, because the four conceptual dimensions-anticipated, embodied, interactive, and reminiscence healing-are theoretically interrelated rather than independent. The use of oblique rotation allows intercorrelations among factors to be estimated, thus maintaining theoretical coherence between the conceptual model and statistical design. Exploratory factor analysis is performed on the 36 items, with the following extraction criteria: eigenvalues greater than 1, elimination of items with factor loadings less than 0.4 or cross-loadings above 0.4, and requirement that each factor contain at least three items55. After repeated filtering, 13 original items are retained. Exploratory factor analysis is performed again using oblique rotation (see Table_3). Factor loadings range between 0.781 and 0.846, and the cumulative variance explained is 69.792%, exceeding the 60% threshold. This result indicates that the extracted factors account for a substantial proportion of variance, thereby supporting the structural validity of the proposed dimensions. Based on both the qualitative findings and established literature, the healing tourism experiences scale (13 items, Cronbach’s α = 0.811) are structured into four factors, ensuring conceptual clarity. They are: anticipated healing (4 items, Cronbach’s α = 0.844), embodied healing (3 items, Cronbach’s α = 0.806), interactive healing (3 items, Cronbach’s α = 0.749), and reminiscence healing (3 items, Cronbach’s α = 0.784).
To ensure the quality of the items, further item analysis is conducted. It is found that removing any item resulted in a Cronbach’s α coefficient below 0.811 for the total scale. All values under the “corrected item-total correlation” exceed 0.3, and the “item discrimination” based on the 27% grouping standard is significant at the 1% level. Therefore, all 13 items should be retained without any need for deletion, indicating that the healing tourism experiences scale have good content validity (see Table_3).
Study 3: re-purification of measures
To further validate the construct validity and applicability, this paper uses confirmatory factor analysis with maximum likelihood estimation. The baseline model is a first-order, four-factor model. Three alternative models are developed for comparison: a first-order, three-factor model, a first-order, single-factor model, and a second-order, four-factor model.
Using AMOS 26.0 (https://www.ibm.com/products/structural-equation-modeling-sem) software for structural equation modeling, the results show that the baseline model had the best fit: χ2/df = 1.043 < 3, RMSEA = 0.012 < 0.05, with NFI, TLI, and CFI all exceeding 0.90. These indices collectively confirm that the four dimensions capture the multidimensional nature of healing effects in tourist experiences. In contrast, both the three-factor and single-factor models had a poor fit (three-factor model: χ2/df = 4.177 > 3, RMSEA = 0.107 > 0.05, NFI, TLI, CFI all below 0.90; single-factor model: χ2/df = 10.207 > 3, RMSEA = 0.182 > 0.05, NFI, TLI, CFI all below 0.90).
The correlation coefficients between the dimensions of the healing tourism experiences range from 0.23 to 0.39, all significant, suggesting the presence of a higher-order common factor. In the second-order, four-factor model (see Figure_3), the fit indices are: χ2/df = 1.010 < 3, RMSEA = 0.006 < 0.05, with NFI, TLI, and CFI all above 0.90, indicating that the measurement model fit the sample data well. Factor loadings for the measurement items on their respective factors range from 0.666 to 0.812, while the relationships between the second-order and first-order factors range from 0.438 to 0.733. Although factor loadings above 0.70 are often recommended for well-established and mature measurement scales, leading methodological authorities (e.g., Hair, 2009; Hinkin, 1998) emphasize that loadings between 0.40 and 0.70 are acceptable for newly developed scales, particularly in the exploratory stage, where items are being refined for the first time and theoretical constructs are still emerging. In this study, the healing tourism experiences represent a newly conceptualized, multidimensional construct integrating anticipated, embodied, interactive, and reminiscence healing, and thus moderate loadings are expected during the early phases of scale development.
Therefore, it is confirmed that the structure of the healing tourism experiences consists of a second-order framework composed of four first-order factors: anticipated healing, embodied healing, interactive healing, and reminiscence healing. The observed intercorrelations among the four first-order factors further justify the application of oblique rotation during EFA and the adoption of a second-order model during CFA. These methodological choices ensure that the empirical structure accurately reflects the theoretical premise of healing tourism as a multiphase yet interconnected psychological process. The hierarchical structure provides theoretical insight: it implies that the four distinct dimensions are interrelated and jointly represent an overarching healing process in tourism. Specifically, anticipated healing captures the role of pre-tourism expectations; embodied healing reflects immersive and affective experiences during travel; interactive healing emphasizes relational and social bonding; and reminiscence healing highlights reflective meaning-making after travel. Together, they form a coherent higher-order construct, suggesting that healing in tourism is best understood as an integrated, multi-phase psychological process rather than isolated effects.

Second-order Confirmatory Factor Analysis of the Healing Tourism Experiences Note: *** indicates p < 0.001.
Regarding construct validity, each item’s factor loadings in the scale (see Figure_3) exceed the threshold of 0.6, satisfying the load requirement. Following the method proposed by Fornell60, the construct validity of the healing tourism experiences is tested using composite reliability (CR), correlation coefficients, and average variance extracted (AVE) to examine both convergent and discriminant validity.
The results for convergent validity show that the CR values of the four factors of healing tourism experiences are 0.846, 0.808, 0.750, and 0.785, all of which are above the 0.7 standard recommended by Hair61. The AVE values for the factors are 0.555, 0.559, 0.501, and 0.534, all above the 0.5 threshold recommended by Fornell60 indicating good convergent validity for the scale.
When calculating the correlation coefficients between the factors, the values range from 0.097 to 0.209, all lower than the square root of the AVE, indicating moderate to low correlations between the factors. Moreover, the AVE are higher than the maximum shared squared variance (MSV) and average shared squared variance (ASV)62(see Table_4). This suggests that while the elements that make up the healing tourism experiences are interrelated to some extent, they also maintain good discriminant validity, forming a coherent and unified construct.
Study 4: model validation
Questionnaire design and data statistics
To enhance the comprehensiveness and credibility of the scale, this study incorporates a fourth empirical phase focusing on model validation and predictive testing. While Studies 2 and 3 have established the dimensional structure and psychometric soundness of the healing tourism experiences scale, it is essential to examine whether this scale holds predictive validity-that is, whether healing experiences can meaningfully influence tourist behavioral outcomes. Thus, Study 4 aims to test the effect of healing experiences on willingness to revisit, a key behavioral intention in tourism research. This approach is consistent with recommendations from scale development literature, which advocate for external validation through criterion-related outcomes41,42.
The formal questionnaire consisted of three sections: (1) the 13-item healing tourism experiences scale, (2) a three-item scale measuring revisit willingness, and (3) demographic information. All items adopted a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree). Data were collected through the Credamo platform. A total of 255 questionnaires were returned, of which 244 were valid, yielding a response rate of 95.7%. Respondents included 79 males, with 40.2% aged 21–30, 41.8% aged 31–40, and the remainder distributed across other age groups, representing a range of industries.
Empirical results and analyses
Reliability analysis demonstrated that the scales exhibited high internal consistency, with Cronbach’s α coefficients of 0.860 for the overall healing scale, and values of 0.801, 0.783, 0.816, and 0.769 for the four healing dimensions, respectively. The revisit willingness scale also showed strong reliability (α = 0.800). Exploratory factor analysis of the 16 items extracted five factors-anticipated healing, embodied healing, interactive healing, reminiscence healing, and revisit willingness-that explained 70.282% of the total variance. Confirmatory factor analysis confirmed a good model fit (χ²/df = 1.788, RMSEA = 0.057, SRMR = 0.061, CFI = 0.948, TLI = 0.936), meeting recommended thresholds63,64. Convergent validity was supported, as AVE values ranged from 0.416 to 0.711, while discriminant validity was established since the square root of each AVE exceeded the corresponding inter-factor correlations.
To assess potential common method variance, Harman’s single-factor test was conducted. The results showed that no single factor accounted for the majority of the variance, indicating that common method bias was not a serious concern in this study.
Finally, apply structural equation modeling (SEM) to evaluate the hypothesized relationship between healing effects and willingness to revisit65. The model demonstrated excellent fit indices (χ2/df = 1.788, RMSEA = 0.057, SRMR = 0.061, CFI = 0.948, and TLI = 0.936). Results indicated that the healing tourism experiences had a significant positive influence on revisit willingness (γ = 0.762, t = 6.01; P < 0.001). The results of the analyses are illustrated in Figure_4 This finding validates the predictive utility of the scale and confirms that healing effects are not only conceptually and psychometrically sound but also behaviorally meaningful, as they enhance tourists’ intention to revisit destinations.

Regression analysis results of the healing tourism experiences.on willingness to revisit Note: *** indicates p < 0.001.
Conclusions and discussions
Research conclusions
This study concludes that tourism experiences yield significant healing effects, which can be categorized into four key dimensions: anticipated healing, embodied healing, interactive healing, and reminiscence healing66,67,68. These four dimensions not only offer a multidimensional framework for understanding the complexity of healing tourism experiences but also provide a theoretical foundation for evaluating and optimizing such effects. The empirical analysis reveals that reminiscence healing has the most substantial impact on revisit intention, closely followed by anticipated healing. Although interactive healing and embodied healing have a relatively smaller effect, their contribution should not be overlooked. Moreover, Study 4 explicitly validated the predictive power of the scale, demonstrating that healing tourism experiences significantly enhance tourists’ willingness to revisit destinations. This finding not only confirms the construct’s criterion-related validity but also strengthens its practical implications for tourism management.
Anticipated healing emphasizes the psychological benefits derived from anticipating tourism activities, which foster positive expectations and enhance mental well-being. Embodied healing, on the other hand, refers to the sensory and physical engagement during travel, such as appreciating local landscapes and immersing in cultural experiences, both of which alleviate stress and contribute to emotional satisfaction. Interactive healing focuses on the social interactions between tourists and locals, as well as with fellow travelers, which strengthen interpersonal relationships and promote psychological comfort. Finally, reminiscence healing pertains to the reflective process after travel, where treasured memories continue to evoke positive emotions and sustain long-term well-being.
The paper also presents a verification of the positive influence of healing tourism experiences on tourists’ revisit intention, as demonstrated through the establishment of structural equation modeling. The results indicate that healing tourism experiences enhance revisit intention by increasing tourists’ satisfaction, well-being, and happiness. Specifically, the emotions of anticipation and excitement before the trip, the satisfaction and healing experiences during the journey, and the positive memories following the trip collectively form a chain of positive emotions that promote the intention to revisit69,70,71. Additionally, tourists’ motivation to share their experiences and their sense of identity and attachment to the destination are also crucial factors influencing revisit intention72,73,74.
Theoretical contributions
First, it explicitly links each identified healing dimension to established psychological theories, thereby situating the framework within broader scholarly debates. Specifically, anticipated healing resonates with expectancy-value theory75, as pre-tourism expectations shape emotional regulation and motivation; embodied healing aligns with research on affective forecasting76, highlighting the role of sensory immersion and emotional engagement; interactive healing draws on social identity theory49, underscoring how group belonging and relational bonding foster restoration; and reminiscence healing is grounded in the autobiographical memory literature50, which explains how reflective recall enhances meaning-making and long-term well-being.
Second, by consolidating these dimensions into a higher-order construct, this study offers an integrated framework that captures healing as a multiphase psychological process spanning pre-tourism, in-tourism, and post-tourism stages. This perspective moves beyond fragmented prior research that emphasized isolated effects, thereby advancing theory toward a holistic understanding of tourism’s restorative potential.
Third, the study contributes methodologically by combining grounded theory with SEM in a sequential mixed-method design. This integration enables both the inductive generation of context-specific constructs and the deductive testing of measurement validity. However, it is important to acknowledge the challenges of such integration, including potential conceptual overlap during coding and the risk of model overfitting in SEM with newly developed items. Recognizing these limitations enhances the credibility of the methodological claim.
Collectively, these contributions demonstrate that healing in tourism should be conceptualized as an integrated, theory-informed, and empirically validated construct, offering new avenues for future research on the restorative power of travel.
Managerial implications
This study provides a series of managerial implications that can guide destination managers, wellness resorts, and tourism marketers in designing and promoting healing-oriented experiences. These implications are not only practically relevant but are also grounded in well-established theoretical perspectives, thereby bridging academic insights with managerial applications.
First, the dimension of anticipated healing underscores the importance of expectation management in enhancing visitors’ psychological well-being prior to travel. Destination marketers should develop promotional materials and online content that evoke positive expectations and emotional readiness, consistent with research on expectation-setting and priming effects77,78. Carefully crafted messages that emphasize opportunities for emotional restoration can foster anticipatory pleasure and stimulate stronger travel intentions.
Second, embodied healing highlights the role of multi-sensory engagement in shaping restorative tourism experiences. Destination planners can incorporate nature-based attractions, cultural immersion, and wellness practices, aligning with affective forecasting research, which shows that sensory-rich experiences amplify emotional outcomes79. Strategic investments in infrastructure and programs that stimulate multiple senses can substantially enhance visitors’ perceived authenticity and emotional recovery.
Third, interactive healing emphasizes the centrality of social connection and group bonding. Organizing parent-child programs, group tours, or community-based initiatives can foster a sense of belonging and interpersonal closeness. This approach is supported by social bonding theory80 and group tourism research81, both of which highlight the restorative role of shared experiences.
Finally, reminiscence healing offers opportunities to extend the healing process beyond the trip. Destinations can implement digital storytelling campaigns, memory-sharing platforms, or personalized souvenirs to encourage visitors to preserve and share their memories. This strategy is consistent with research on autobiographical memory and meaning-making, which suggests that reflective recall reinforces positive emotions and contributes to long-term well-being50,82.
Collectively, these implications demonstrate that destination management strategies should not be treated as isolated marketing or operational actions. Instead, they represent evidence-based applications of psychological and tourism theories, enabling practitioners to enhance visitor satisfaction, strengthen revisit intentions, and contribute to the broader goal of positioning tourism as a sustainable pathway for psychological well-being.
Limitations and future suggestions
While the healing benefits of tourism have been demonstrated at both theoretical and practical levels, several limitations should be acknowledged, which also provide directions for future research.
First, the present study, like much of the existing literature, primarily examined the experiences of Chinese tourists. This cultural focus restricts the generalizability of the findings83. Future research should adopt a broader, cross-cultural perspective to capture both the universal and culture-specific aspects of healing tourism. For instance, while Chinese tourists may emphasize interpersonal harmony and collective well-being, Western tourists may attach greater importance to personal growth and self-actualization. Comparative research of this kind would enrich our understanding of cultural variations in healing tourism experiences and their influence on consumption behavior.
Second, this study did not encompass the full range of tourism activity types. Future work could extend the framework to diverse forms of tourism, such as adventure tourism, wellness tourism, or dark tourism, and investigate how different activities elicit distinct healing dimensions84,85. Moreover, examining contrasting destination contexts-such as urban versus rural settings-would clarify how environmental attributes shape the manifestation and intensity of healing experiences.
Third, the current study did not comprehensively examine the antecedents and consequences of healing tourism experiences. Future research could identify the factors that facilitate or hinder healing (e.g., destination attributes, social interactions, or individual traits) and investigate outcomes that extend beyond revisit intention, such as destination image, value perceptions, and loyalty formation. Moreover, future studies could theoretically enrich the predictive framework by examining potential mediating mechanisms that link healing experiences to behavioral outcomes. Psychological states such as emotional well-being, satisfaction, and destination attachment may act as mediators through which healing experiences influence revisit intention. For example, reminiscence healing might indirectly enhance revisit intention by evoking positive emotional memories or strengthening affective attachment to the destination. Incorporating these mediating pathways would align future models with established behavioral and emotional theories, offering a more nuanced understanding of how healing tourism experiences translate into actual tourist behavior. Such investigations would extend the explanatory power of the proposed framework and deepen theoretical insights into the psychological mechanisms underlying healing tourism.
Lastly, several methodological limitations should be noted. Although the overall design is robust, using the same dataset for both EFA and CFA in Studies 2 and 3 raises the risk of statistical overfitting, as models derived from a single sample may not generalize well to other populations. This decision was constrained by time, resources, and the scope of the project, making it impractical to collect a new dataset or split the existing one without reducing statistical power. Consequently, the generalizability and external validity of the findings may be somewhat limited. Future research should employ independent validation samples or split-sample techniques to strengthen methodological rigor and test the stability of the scale across contexts.
Data availability
Data used in this study will be made available by the corresponding author upon reasonable request.
References
Chen, H., Jiao, Y., Li, X. & Zhang, K. Family tourism: interpersonal interaction, existential authenticity and quality of tourist experience. J. VACAT MARK. 28, 82 (2022).
Christou, P. & Simillidou, A. Tourist experience: the catalyst role of tourism in comforting melancholy, or not. J. HOSP. TOUR MANAG. 42, 210 (2020).
He, M., Liu, B. & Li, Y. Tourist inspiration: how the wellness tourism experience inspires tourist engagement. J. HOSP. TOUR RES. 47, 1115 (2023).
Sun, S. et al. Health tourism evolution: a review based on bibliometric analysis and the China National knowledge infrastructure database. SUSTAINABILITY-BASEL 14, 10435 (2022).
Liu, B., Kralj, A., Moyle, B., He, M. & Li, Y. Perceived destination restorative qualities in wellness tourism: the role of ontological security and psychological resilience. J. TRAVEL RES. 64, 658059581 (2024).
Wong, I. A., Lin, Z. & Kou, I. E. Restoring hope and optimism through staycation programs: an application of psychological capital theory. J. SUSTAIN. TOUR. 31, 91 (2023).
Buckley, R. C. Therapeutic mental health effects perceived by outdoor tourists: A large-scale, multi-decade, qualitative analysis. ANN. TOURISM RES. 77, 164 (2019).
Kim, S. E., Um, S. H. & Lee, T. J. Healing effects from the on-site experiences of tourists. INT. J. TOUR RES. 22, 192 (2020).
Kim, H. & So, K. K. F. Two decades of customer experience research in hospitality and tourism: A bibliometric analysis and thematic content analysis. INT. J. HOSP. MANAG. 100, 103082 (2022).
Cohen, E. A phenomenology of tourist experiences. SOCIOLOGY 13, 179 (1979).
Lin, C. & Kuo, B. Z. The behavioral consequences of tourist experience. TOUR MANAG PERSPECT. 18, 84 (2016).
Oh, H., Fiore, A. M. & Jeoung, M. Measuring experience economy concepts: tourism applications. J. TRAVEL RES. 46, 119 (2007).
Otto, J. E. & Ritchie, J. B. The service experience in tourism. TOURISM MANAGE. 17, 165 (1996).
Teoh, M. W., Wang, Y. & Kwek, A. Conceptualising co-created transformative tourism experiences: A systematic narrative review. J. HOSP. TOUR MANAG. 47, 176 (2021).
Buzova, D., Cervera Taulet, A. & Sanz Blas, S. Exploring multisensory place experiences through cruise blog analysis. PSYCHOL. MARKET. 37, 131 (2020).
Chirakranont, R. & Sakdiyakorn, M. Conceptualizing meaningful tourism experiences: case study of a small craft beer brewery in Thailand. J. DESTIN MARK. MANAGE. 23, 100691 (2022).
Agapito, D., Valle, P. & Mendes, J. The sensory dimension of tourist experiences: capturing meaningful sensory-informed themes in Southwest Portugal. TOURISM MANAGE. 42, 224 (2014).
Bagheri, F., Guerreiro, M., Pinto, P. & Ghaderi, Z. From tourist experience to satisfaction and loyalty: Exploring the role of a sense of well-being. J TRAVEL RES 63 (2024). (1989).
Packer, J. & Ballantyne, R. Conceptualizing the visitor experience: A review of literature and development of a multifaceted model. VISIT STUD. 19, 128 (2016).
Tung, V. W. S. & Ritchie, J. B. Exploring the essence of memorable tourism experiences. ANN. TOURISM RES. 38, 1367 (2011).
Chen, H. & Rahman, I. Cultural tourism: an analysis of engagement, cultural contact, memorable tourism experience and destination loyalty. TOUR MANAG PERSPECT. 26, 153 (2018).
Fan, D. X., Tsaur, S., Lin, J., Chang, T. & Tsa, Y. T. Tourist intercultural competence: A multidimensional measurement and its impact on tourist active participation and memorable cultural experiences. J. TRAVEL RES. 61, 414 (2022).
Triantafillidou, A. & Petala, Z. The role of sea-based adventure experiences in tourists’ satisfaction and behavioral intentions. J. TRAVEL TOUR MARK. 33, 67 (2016).
Lu, Y. et al. Flow in soundscape: The conceptualization of soundscape flow experience and its relationship with soundscape perception and behaviour intention in tourism destinations. CURR ISSUES TOUR 25 (2022). (2090).
Craig, C., Hiskey, S. & Spector, A. Compassion focused therapy: A systematic review of its effectiveness and acceptability in clinical populations. EXPERT REV. NEUROTHER. 20, 385 (2020).
Kazdin, A. E. Interventions in everyday life to improve mental health and reduce symptoms of psychiatric disorders. AM. PSYCHOL. 79, 185 (2024).
Bucea-Manea-Țoniș, R. & Păun, D. G. Yoga, a mindfulness therapy to prevent PTSD as to encompass athletes’ performance. FRONT. PSYCHOL. 15, 1334278 (2024).
Rogers, L., Phillips, K. & Cooper, N. Energy healing therapies: A systematic review and critical appraisal. HEALTH PSYCHOL. REV. 2, 162 (2021).
Buckley, R. Nature tourism and mental health: parks, happiness, and causation. J. SUSTAIN. TOUR. 28, 1409 (2020).
Kaplan, R. & Kaplan, S. The Experience of Nature: A Psychological Perspective (Cambridge University Press, 1989).
Kwok, I. et al. Poetry as a healing modality in medicine: Current state and common structures for implementation and research. J PAIN SYMPTOM MANAG 64 e91 (2022).
Stuckey, H. L. & Nobel, J. The connection between art, healing, and public health: A review of current literature. AM. J. PUBLIC. HEALTH. 100, 254 (2010).
Yang, J. Y., Paek, S., Kim, T. & Lee, T. H. Health tourism: needs for healing experience and intentions for transformation in wellness resorts in Korea. INT. J. CONTEMP. HOSP. M. 27, 1881 (2015).
Terzidou, M., Scarles, C. & Saunders, M. N. The complexities of religious tourism motivations: sacred places, vows and visions. ANN. TOURISM RES. 70, 54 (2018).
Bhalla, R., Chowdhary, N. & Ranjan, A. Spiritual tourism for psychotherapeutic healing post COVID-19. J. TRAVEL TOUR MARK. 38, 769 (2021).
Knobloch, U., Robertson, K. & Aitken, R. Experience, emotion, and eudaimonia: A consideration of tourist experiences and well-being. J. TRAVEL RES. 56, 651 (2017).
Churchill, G. A. Jr A paradigm for developing better measures of marketing constructs. J. Mark. RES. 16, 64 (1979).
Hinkin, T. R. A brief tutorial on the development of measures for use in survey questionnaires. ORGAN. RES. METHODS. 1, 104 (1998).
Makri, C. & Neely, A. Grounded theory: A guide for exploratory studies in management research. INT. J. QUAL. METH. 20, 2119180822 (2021).
Mertler, C. A., Vannatta, R. A. & LaVenia, K. N. Advanced and Multivariate Statistical Methods: Practical Application and Interpretation (Routledge, 2021).
DeVellis, R. F. & Thorpe, C. T. Scale Development: Theory and Applications (Sage, 2021).
Manthiou, A., Ulrich, I. & Kuppelwieser, V. The travel influencer construct: an empirical exploration and validation. TOURISM MANAGE. 101, 104858 (2024).
Likert, R. A technique for the measurement of attitudes. Archives Psychol. 140, 155 (1932).
Li, X., Cui, W. & Chee, W. M. Investigating tourism experiences and attention allocation of outbound tourists through the lens of the two-factor theory: a grounded theory analysis of Chinese tourists’ travelogues in Malaysia. HELIYON 9 (2023).
Meng, K., Wang, M., Yuan, H. & Zhang, B. The countryside in the eyes of the beholder: developing and testing a tourists’ rurality perception scale. CURR. ISSUES TOUR. 27, 2815 (2024).
Strauss, A. & Corbin, J. Basics of qualitative research techniques. (1998).
Bowen, G. A. Naturalistic inquiry and the saturation concept: a research note. QUAL. RES. 8, 137 (2008).
Csikszentmihalyi, M. Flow: The psychology of optimal experience (Harper & Row New York, 1990).
Tajfel, H. & Turner, J. C. In Political Psychology pp. 276 (Psychology, 2004).
Pillemer, D. Directive functions of autobiographical memory: the guiding power of the specific episode. MEMORY 11, 193 (2003).
Zou, Y. & Yu, Q. Sense of safety toward tourism destinations: A social constructivist perspective. J. DESTIN MARK. MANAGE. 24, 100708 (2022).
Zhong, L., Deng, B., Morrison, A. M., Coca-Stefaniak, J. A. & Yang, L. Medical, health and wellness tourism research—A review of the literature (1970–2020) and research agenda. Int. J. Environ. Res. Public Health. 18, 10875 (2021).
Zheng, Y., Hou, Y. & Dong, Z. From good expectancy to good feelings: how optimism is related to subjective well-being in Chinese adults through the pathway of coping. BEHAV. SCI-BASEL. 14, 165 (2024).
Lench, H. C. et al. Optimistic expectations have benefits for effort and emotion with little cost. EMOTION 21 1213 (2021).
Saeed, B., Tasmin, R., Mahmood, A. & Hafeez, A. Development of a multi-item operational excellence scale: exploratory and confirmatory factor analysis. TQM J. 34, 576 (2022).
Karl, M., Kock, F., Ritchie, B. W. & Gauss, J. Affective forecasting and travel decision-making: an investigation in times of a pandemic. ANN. TOURISM RES. 87, 103139 (2021).
Zhuang, X. & Wang, Y. Social support and travel: enhancing relationships, communication, and Understanding for travel companions. INT. J. TOUR RES. 26, e2712 (2024).
Puusepp, V. Becoming closer to one another: shared emotions and social relationships. PHILOS. PSYCHOL. 37, 2533 (2024).
Karagöz, D. & Ramkissoon, H. Loneliness, travel nostalgia, subjective well-being and prevention regulatory focus: A moderated mediation model analysis. CURR. ISSUES TOUR. 27, 217 (2024).
Fornell, C. Structural equation models with unobservable variables and measurement error: Algebra and statistics. (1981).
Hair, J. Multivariate data analysis. Exploratory factor analysis (2009).
Byrne, B. M. Basic concepts, applications, and programming. Struct. Equation Model. AMOS. 396, 227 (2010).
Hu, L. T. & Bentler, P. M. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct. Equation Modeling: Multidisciplinary J. 6, 1 (1999).
Stylos, N., Vassiliadis, C. A., Bellou, V. & Andronikidis, A. Destination images, holistic images and personal normative beliefs: predictors of intention to revisit a destination. TOURISM MANAGE. 53, 40 (2016).
Hu, L. & Bentler, P. M. Fit indices in covariance structure modeling: sensitivity to underparameterized model misspecification. PSYCHOL. METHODS. 3, 424 (1998).
Huang, X. presented at the International Conference on Human-Computer Interaction, 2024 (unpublished).
Lin, G., Li, M., Li, B. & Meng, Y. A healing journey with animals. J. HOSP. TOUR MANAG. 60, 252 (2024).
Wood, E. H., Kinnunen, M., Moss, J. & Li, Y. Shared festival tourism experiences: the power and purpose of remembering together. J. TRAVEL RES. 63, 409 (2024).
Kim, Y., Ribeiro, M. A. & Li, G. Tourism memory, mood repair and behavioral intention. ANN. TOURISM RES. 93, 103369 (2022).
Rahman, I., Martin, D. S. & Liu, S. Outbound medical tourists: the interplay of perceived quality, length of stay, group-size, post-visit destination image and revisit intention. PLOS ONE. 17, e0267755 (2022).
Zhao, Z., Shi, D., Huang, Z. & Liu, X. How does tourism memory affect revisit decisions? The mediating role of episodic future thinking. TOUR MANAG PERSPECT. 49, 101199 (2023).
Lin, C. & Wang, W. Impacts of climate change knowledge on coastal tourists’ destination decision-making and revisit intentions. J. HOSP. TOUR MANAG. 56, 322 (2023).
Stylidis, D. Exploring resident–tourist interaction and its impact on tourists’ destination image. J. TRAVEL RES. 61, 186 (2022).
Yuxin, F., Jianpeng, Q., Xiaoyu, L., Yunxia, T. & Weilong, M. Exploring the influence of historical storytelling on cultural heritage tourists’ revisit intention: A case study of the Mogao Grottoes in Dunhuang. PLOS ONE 19 e0307869 (2024).
Vroom, V. H. Work and motivation. (1964).
Wilson, T. D. & Gilbert, D. T. Affective forecasting: knowing what to want. CURR. DIR. PSYCHOL. SCI. 14, 131 (2005).
Wilson, T. D., Lindsey, S. & Schooler, T. Y. A model of dual attitudes. PSYCHOL. REV. 107, 101 (2000).
Yi, Y. & La, S. What influences the relationship between customer satisfaction and repurchase intention? Investigating the effects of adjusted expectations and customer loyalty. PSYCHOL. MARKET. 21, 351 (2004).
Gilbert, D. T. & Wilson, T. D. Prospection: Experiencing the future. SCIENCE 317 1351 (2007).
Okleshen Peters, C. L., Shelton, J. & Sharma, P. An investigation of factors that influence the consumption of dietary supplements. Health Mark. Q. 21, 113 (2003).
Blichfeldt, B. S. & Halkier, H. Mussels, tourism and community development: a case study of place branding through food festivals in rural North Jutland, Denmark. EUR. PLAN. STUD. 22, 1587 (2014).
Wildschut, T., Sedikides, C., Arndt, J. & Routledge, C. Nostalgia: content, triggers, functions. J. PERS. SOC. PSYCHOL. 91, 975 (2006).
Jelinčić, D. A. & Matečić, I. Broken but well: healing dimensions of cultural tourism experiences. SUSTAINABILITY-BASEL 13, 966 (2021).
Beames, S., Mackenzie, S. H. & Raymond, E. How can we adventure sustainably? A systematized review of sustainability guidance for adventure tourism operators. J. HOSP. TOUR MANAG. 50, 223 (2022).
Sun, J. & Lv, X. Feeling dark, seeing dark: Mind–body in dark tourism. ANN. TOURISM RES. 86, 103087 (2021).
Funding
This research was supported by [Sichuan Province Natural Science Foundation] under Grant [2024NSFSC0270]; [the Ministry of Education’s Humanities and Social Sciences Research Youth Fund Project] under Grant [24YJC890053]; [the Natural Science Foundation of Sichuan (Youth Project)] under Grant [23NSFSC1062]; [the Philosophy and Social Science Foundation of Sichuan Province (General Project)] under Grant [SCJJ24ND081, SCJJ24ND169]; [Chengdu University of Technology “Double First-Class” initiative Construction Philosophy and Social Sciences Key Construction Project] under Grant [ZDJS202320].
Author information
Authors and Affiliations
Contributions
Jize Xie: Writing – original draft, Visualization, Formal analysis, SoftwareHan Li: Writing – review & editing, Supervision, MethodologyZiyu Chen: Writing – original draft, Formal analysis, Data curationHong Wang: Writing – review & editing, Conceptualization, InvestigationHaiyan Hua: Writing – review & editing, Conceptualization, Project administration.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Methods and human experiments statement
The ethics committee of the Business School Chengdu University of Technology has approved the experiment on " Developing a Multidimensional Scale of Healing Tourism Experiences Based on a Mixed Methods Approach” conducted by Jize Xie et al. The research group promised that the experiment would be conducted with full information given, and informed consent from all subjects received. The experiment would not cause any psychological or physical harm to the subjects. Subjects have the right to withdraw from the experiment at any stage. For data collected in the experiment, they can be used in the study after anonymization. The subject has the right to ask the research group to delete the experiment result about himself at any stage.
Furthermore, we confirm that this study has been conducted in accordance with the relevant guidelines and regulations and that all methods have been approved by the appropriate authorities.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Xie, J., Li, H., Chen, Z. et al. Developing a multidimensional scale of healing tourism experiences based on a mixed methods approach. Sci Rep 16, 4193 (2026). https://doi.org/10.1038/s41598-025-34286-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-34286-8
