
Abstract
This study aimed to assess the prognostic impact of plasma albumin (PA) and C-reactive protein (CRP), measured up to 30 days before a bloodstream infection (BSI), on 30-day mortality risk using nomogram models. Two cohorts comprising 5,221 inpatients from Singapore (SG) and 15,710 from Denmark (DK) with first-time BSIs were included from 2006 to 2016. Using multivariable logistic regression models, we analyzed the association between CRP and PA measured at different time-points (segmented into 5-day intervals, up to 30 days before the day of BSI (D0), and on D0) and 30-day mortality. Moreover, nomogram models assessed the relative attributions of PA and CRP to 30-day mortality risk. Both cohorts had similar 30-day mortality rates (SG: 17.4%, DK: 20.2%). Correlation coefficients between PA on D0 and PA in all 5-day intervals were high (range: 0.55/0.75) whereas it was only high between CRP on D0, and CRP measured 1–5 days before D0. In nomogram models, PA contributed most to the prognostic predictability (from 20 to 55%) whereas CRP contributed little (from 0.5 to 9%) regardless of time interval from D0. Albumin, measured up to 30 days before a BSI episode, was a strong prognosticator of 30-day mortality. Nomogram models enable rapid evaluation of a patient’s prognosis.
Similar content being viewed by others

Introduction
Despite significant advances in medical science over the past century, bloodstream infections (BSIs) prevail as a major cause of morbidity and mortality worldwide with an estimated 30-day mortality rate of 20%1. Hence, it is imperative for early prognosis of mortality risk to enable closer monitoring of high-risk individuals. C-reactive protein (CRP), procalcitonin, interleukin-6 and plasma albumin (PA), typically measured on the day of BSI diagnosis, are widely reported to be useful predictors of clinical outcomes of BSI in previous studies2,3,4. However, the prognostic value of CRP and PA levels in the days leading up to a BSI episode remains largely unexplored. Given that CRP and PA are already established predictors for BSI, a key clinical question emerges: Can incorporating earlier measurement before BSI encounter improve mortality prediction beyond what is achievable with day-of-diagnosis values alone? Furthermore, understanding the relative contributions of different biomarkers measured at various time points could guide clinicians in prioritising which laboratory values to monitor most closely in high-risk patients. Hence, this study aimed to assess and compare the prognostic value of CRP and PA levels up to 30 days before a BSI episode for 30-day mortality risk using data from Asian and European inpatient cohorts, and to develop nomograms for 30-day mortality risk for the convenient application by clinicians. Nomograms are intuitive. With a quick look at a nomogram model, factors of high impact (based on the points delegated) to 30-day mortality in patients with BSI are easily distinguishable to clinicians. It is hypothesised that CRP and PA levels measured at multiple time points up to 30 days before a BSI episode can predict 30-day mortality risk in patients with bloodstream infections. Furthermore, we postulated that CRP and PA would demonstrate similar prognostic patterns across both Singaporean and Danish cohorts and that the relationship between CRP and PA and mortality can be effectively modelled using predictive nomograms for clinical application.
Methods
Study setting
As in a previous study by Sim et al. (2024), the same cohorts of Singaporean and Danish BSI patients were examined5. Both cohorts were analyzed simultaneously as this approach allows direct comparison of prognostic patterns across the two populations with different healthcare systems, rather than using one as a training set and the other for validation.
Singapore
With a total population of 5.6 million in 2022 living in a compact area of 733 km2, Singapore (SG) is a tropical city-state situated near the equator in Southeast Asia that experiences consistently high temperatures all-year round6. It is a multi-ethnic country that has three major ethnic groups: 74.1% Chinese, 13.6% Malays and 9.0% Indians according to 2022 census7. In this study, we included patients with BSI who were admitted into Tan Tock Seng Hospital (TTSH), which is a 1600-bed multi-disciplinary tertiary-care hospital. Serving an estimated resident population of 1.4 million (approximately 25% of SG’s population) from the central region of SG, healthcare services provided at TTSH are heavily subsidized by the government. All Singaporean residents have a unique personal identifier that is linked to their electronic health records and administrative databases that exist in TTSH.
Denmark
Denmark (DK) is a country in Northern Europe with a population of 5.8 million in 2022 living in an area of 42,493 km2 and has a temperate climate marked by relatively cool summers and moderately cold winters8. Majority (85.6%) of the resident Denmark population is ethnically Danish9. The health-care system is tax-financed and hence free of charge for residents. Approximately 35% of DK’s population reside in Region Zealand and the Region of Southern DK (i.e., 2.0 million residents). As in SG, all Danish residents have a unique personal identifier used for linkage between all health records, national administrative registries, and laboratory information systems10.
Patient cohort, inclusion, and exclusion criteria
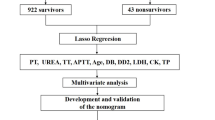
Patients aged 15 years [DK]/21 years [SG] and older hospitalized with at least one BSI episode between 1 January 2006 [SG]/2007 [DK] and 31 December 2016 were included. The difference in cut-off age is due to the difference in the eligibility for inclusion criteria. If a patient had multiple admissions, only the index (first) admission was included with the earliest date of the positive blood culture defined as the date of BSI episode (D0) and a non-contaminant microorganism was included. We excluded patients whose blood culture grew a contaminant, defined as coagulase-negative staphylococci, Bacillus spp, Propionibacterium spp, Corynebacterium spp, viridans group streptococci, Aerococcus spp, or Micrococcus spp, unless they were isolated in ≥ 2 blood cultures within 5 days11. A poly-microbial BSI was defined as ≥ 2 different pathogens isolated within 2 days during an admission episode12. Thereafter, patients with invalid death dates (i.e., death dates recorded as occurring before hospital admission dates, indicating data entry errors), no CRP or PA measured on D0 were excluded, leaving 5,221 Singaporean patients and 15,710 Danish patients for this analysis (Fig. 1). The Singaporean cohort had fewer CRP/PA measurements (i.e., no CRP/PA measurements on D0) compared to the Danish cohort, resulting in more patients being excluded from the Singaporean cohort.

Flow diagram for Singapore and Denmark. *Unknown microorganism: the genus and/or species of the microorganism could not be identified.
Data collection
Data included demographic variables (age and gender), presence of comorbidity, place of acquisition, microbiological and biochemistry data, and mortality data. Comorbidities were identified from discharge diagnosis codes and the Charlson comorbidity index (CCI) score derived using coding algorithm developed by Quan et al. (2005)13. Microbiological data consisted of the earliest positive blood culture date and microorganism. Place of acquisition of BSI were defined as followed: (i) Nosocomial BSI: a positive blood culture that occurred more than two days after admission; (ii) Healthcare- associated (HA) BSI: a positive blood culture that occurred within two days of admission and the patient had history of either hospital admission or an outpatient contact/appointment to a department of hematology, oncology, or nephrology within the last 30 days (iii) Community-acquired BSI: a positive blood culture that occurred within two days of admission, with no history of hospital admissions or contacts to the said departments within the last 30 days14,15. Biochemistry data comprised all specimens with CRP (in per mg/L) or PA (in per g/L) levels measured up to 30 days before D0. Primary outcome of interest was 30-day all-cause mortality, defined as death occurring within 30 days from the specimen collection date of the positive blood culture (D0).
Data for the Singaporean cohort were extracted from TTSH’s electronic medical records. For DK, data on positive blood cultures were retrieved from the laboratory information system (MADS) of the four departments of clinical microbiology in the Region of Southern DK16. Data on hospital admissions were obtained from the Danish National Patient Registry (DNPR), and CRP and PA were retrieved from laboratory information systems of the departments of clinical biochemistry (BCC and LABKA) in the Region of Southern DK17,18.
Due to the retrospective nature of the study, a waiver of informed consent was obtained from the National Healthcare Group Domain Specific Review Board, Singapore (Reference number: 2017/00246). In Denmark, as the studies were registry-based and without patient contact, approval from an ethics committee or consent from participants is not required. However, because microbiology data are legally considered to be medical chart data, permission for using these was required (Danish Patient Safety Authority, rec. no. 3-3013-945/1 & 3-3013-945/2). A Data Processor Agreement was completed between the two countries (rec. no. 18/57806). This study was approved by the National Healthcare Group Domain Specific Review Board, Singapore, and the Danish Patient Safety Authority and was conducted in accordance with the Declaration of Helsinki.
Statistical analysis
We categorized the measurements of CRP and PA into 7 groups according to 5-day interval period—specifically: D0 (day of BSI diagnosis), 1–5 days before D0 (D-1/D-5), 6–10 days before D0 (D-6/D-10), 11–15 days before D0 (D-11/D-15), 16–20 days before D0 (D-16/D-20), 21–25 days before D0 (D-21/D-25) and 26–30 days before D0 (D-26/D-30)—to examine their attributable 30-day mortality risk. This temporal categorization allowed us to assess how levels of CRP and PA at different time points before BSI diagnosis contribute to mortality prediction. Individual patients could enter multiple subgroups if they had CRP or PA measurements performed within different time windows (i.e. 2 or more measurements within their admission).
For patients with at least 1 more measurement of CRP or PA within 30 days in addition to D0 measurement, we calculated Pearson’s correlation coefficient by comparing their earliest measurement (from D-1/D-30) to D0 measurement. Multivariable logistic regression models were then constructed to assess for the independent associations of the PA/CRP level groups during the seven groups of time period (earliest specimen on D0, D-1/-5, D-6/-10, D-11/D-15, D-16/D-20, D-21/D-25, D-26/-30) and CRP/PA level on D0, on 30-day mortality risk. Odds ratios (OR) and 95% confidence intervals (CI) were estimated, adjusting for age, CCI, place of acquisition and microorganism group.
Four main models of multivariable logistic regression were constructed: (i) a baseline model that included the covariates—specifically age, CCI, place of acquisition of BSI and the four main microorganism groups (Mono-microbial Gram-negative, Mono-microbial Gram-positive, Fungi, Poly-microbial); (ii) the baseline model and the earliest PA measurement; (iii) the baseline model and CRP on D0; and (iv) the baseline model, the earliest PA measurement, and CRP on D0. For each main regression model, further seven models (i.e. the seven different time-window groups) were derived using the earliest PA or CRP levels. Areas Under the Receiving Operating Curves (AUROC) for each model were derived for comparison. We evaluated differences in AUROCs between all models by C-statistics19,20. A p-value of < 0.05 was considered statistically significant.
We developed nomograms that harness the fundamentals of logistic regression and enhance the technique to assess the impact of each independent variable and its relative attribution to 30-day mortality risk. A nomogram allocates maximum points (up to 10 points) to the variable with the highest impact on the outcome (30-day mortality) and standardizes the other variables’ points according to it21. This allows a direct comparison of each variable’s impact on the outcome. Interpretation of a nomogram is simple: Variables in a model have different score scales in the nomogram. Obtain the scores for all variable values, add the scores, and obtain the probability of an event (outcome) using the total score to probability graph21. The higher the total score, the greater the probability of the outcome. Please refer to Supplementary Figure S1 for a detailed guide. Lastly, we applied Decision Curve Analyses to demonstrate the clinical utility and net benefit of albumin and CRP-based models in guiding early treatment decisions for patients with bloodstream infection. All statistical analyses were performed using Stata 16.1 (StataCorp, College Station, TX).
Results
Baseline characteristics
Patients with BSI from SG and DK had similar distributions of age, gender and CCI (Table 1). There was a slight preponderance of males, with similar median age of the patients of 72 years (IQR SG: 60/81 vs. DK 62/81). Compared to the Danish cohort, the Singaporean cohort had a greater proportion of community-acquired BSIs (SG: 71.9% vs. DK: 50.6%), but lower proportion of HA BSIs (SG: 9.2% vs. DK: 29.4%). Escherichia coli and Staphylococcus aureus were the most common causative pathogens of BSI, ranking amongst the top four pathogens in both countries (Table 1). Whilst Klebsiella and poly-microbial infections ranked second and third-most common BSI in SG, respectively. Streptococcus pneumoniae, Enterococcus and Coagulase-negative staphylococci pathogens were more common in DK.
Interval between earliest CRP and PA level, BSI incidence, and 30-day mortality risk
Majority of SG and DK cohort had their earliest CRP or PA level measurement made on D0 (For CRP, SG: 77.4% vs DK: 45.9%; For PA, SG: 64.1% vs DK: 44.3%), followed by D-1/D-5 (For CRP, SG: 5.2% vs DK: 10.2%; For PA, SG: 9.7% vs DK: 9.6%) (Supplementary Tables S1 and S2). The number of patients having earliest measurement were found steadily increasing in the periods nearer to D0.
Moreover, similar proportions of patients diagnosed with BSI died within 30 days (SG: 17.4% vs. DK: 20.2%) (Supplementary Tables S1 and S2). The 30-day mortality risk was lowest for patients with their earliest PA level measured on D0 (SG: 13.6% vs. DK: 14.7%).
Correlation between earliest PA values and PA value on D0 or CRP value on D0
For 1,876 Singaporean (35.9%) and 8,751 Danish patients (55.7%) who had additional measurement of PA before D0 measurement, Pearson’s correlation coefficient of PA level measured in all time intervals indicated high positive correlations with PA level measured on D0 (SG: 0.55/0.75, all p < 0.001 vs. DK: 0.45/0.62, all p < 0.001) (Supplementary Tables S3A and S4A).
We also compared the patients’ earliest PA level with their CRP level on D0 (Supplementary Tables S3B and S4B). There was no unanimous finding observed among different time intervals, some periods showed negative or no correction.
Correlation between earliest CRP values and CRP value on D0 or PA value on D0
There were 1,178 Singaporean (22.6%) and 8,506 Danish patients (54.1%) who had additional measurement of CRP before D0 measurement, and we compared their earliest CRP level with their CRP level on D0 (Supplementary Tables S3A and S4A). For both SG and DK, all time intervals displayed low positive correlations with CRP on D0, apart from the D-1/D-5 interval, which exhibited moderate to high positive correlations with CRP on D0 (SG: 0.70 vs. DK: 0.54).
The Pearson’s coefficient of the earliest CRP measured in all time intervals vs. PA on D0 generally exhibited low negative correlations (Supplementary Tables S3B and S4B; range: − 0.38/− 0.10 for SG range: − 0.34/− 0.14 for DK).
Multivariable logistic regression models
Lower PA levels were overall associated with an increase in 30-day mortality risk for both cohorts (Supplementary Tables S5 and S6). Amongst the seven models that displayed earliest PA measured and CRP measured on D0, the strongest association between PA levels and 30-day mortality risk was observed for PA level measured on D0. For each g/L increase in PA on D0, the 30-day mortality risk decreased by more than 10% (SG: 14% vs. DK: 12%). For patients with PA on D-26/D-30, 30-day mortality risk decreased by at least 4% for every g/L increase in PA (SG: 10% vs. DK: 4%).
For the seven models that had the earliest CRP measured and PA measured on D0, the association between CRP levels and 30-day mortality risk was not significant, apart from the model with CRP on D0, in which an increase in the CRP level was associated with higher 30-day mortality (Supplementary Tables S5 and S6). In the same models, it was observed that lower PA levels were associated with increased odds of 30-day mortality.
Areas Under the Receiving Operating characteristic Curves (AUROCs)
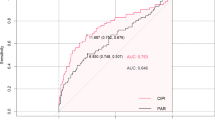
For both cohorts, AUROCs increased marginally in the models when adjusted for CRP (baseline model and CRP on D0) but increased substantially when adjusted for PA (baseline model and earliest PA measurement) and both PA and CRP (baseline model, earliest PA measurement and CRP on D0) respectively (Supplementary Tables S7 and S8). Although there was no increasing trend of AUROCs with the increasing proximity of PA measurement to D0, AUROCs were the highest for the D0 model.
Nomograms and maximum points for patients with CRP measured on D0 & ≥ 1 PA measured up to 30 days before D0
The numbers in Tables 2 and 3 represent probability scores for 30-day mortality outcomes, calculated for different covariates within each subgroup of PA and CRP measurements during their respective time periods. These scores predict 30-day mortality in BSI patients from the Singaporean and Danish cohorts, indicating which factors contribute most (i.e. highest scores that are bolded) significantly to mortality risk at different time intervals. Overall, earliest PA level measured was a significant contributing variable to 30-day mortality risk, mostly ranking first or amongst the top three places as the highest contributor in all models (range: 19.0/44.6% for SG; range: 27.0/54.6% for DK) (Tables 2A and 3A, Supplementary Figures S2 and S3). Age was the second most important contributing factor (range: 11.2/33.6% for SG; range: 20.4–30.7% for DK). Most score points were notably allotted for PA in the nomogram models for PA measured on D0 and D-26/-30 (Tables 2A and 3A, Figs. 2A, 2B, 3A and 3B). Apart from the earliest PA level and age, other covariates (CCI, place of acquisition, micro-organism group and CRP on D0) did not contribute substantially to 30-day mortality risk.

(top left to bottom right): (A) Nomogram for Singaporean patients with earliest PA measured on D0 and CRP measured on D0. (B) Nomogram for Singaporean patients with earliest PA measured 26–30 days before D0 and CRP measured on D0. (C) Nomogram for Singaporean patients with earliest CRP measured on D0 and PA measured on D0. (D) Nomogram for Singaporean patients with earliest CRP measured 26–30 days before D0 and PA measured on D0.

(top left to bottom right): (A) Nomogram for Danish patients with earliest PA measured on D0 and CRP measured on D0. (B) Nomogram for Danish patients with earliest PA measured 26–30 days before D0 and CRP measured on D0. (C) Nomogram for Danish patients with earliest CRP measured on D0 and PA measured on D0. (D) Nomogram for Danish patients with earliest CRP measured 26–30 days before D0 and PA measured on D0.
Nomograms and maximum points for patients with PA measured on D0 & ≥ 1 CRP measured up to 30 days before D0
PA measured on D0 was a statistically significant contributor to 30-day mortality risk, ranking first or second place in all models for Singaporean and Danish cohorts (range: 20.6/53.1% for SG, range: 44.8/55.9% for DK) (Tables 2B and 3B, Supplementary Figures S4 and S5). In contrast, earliest CRP measured up to 30 days before D0 contributed meagrely to the total scores of the nomogram models (range: 1.8/8.0% for SG, range: 0.5/8.8% for DK) (Tables 2B and 3B, Figs. 2C, 2D, 3C and 3D). Like the nomogram models with earliest PA level and CRP on D0, the other covariates had little contribution to 30-day mortality risk.
Decision Curve Analysis graphs for patients with CRP measured on D0 & ≥ 1 PA measured up to 30 days before D0
For Singaporean and Danish cohorts, there was positive net benefit at the lower threshold probabilities (0–20%), implying that the albumin-based prediction models offer a small net benefit when clinicians are willing to treat patients at low predicted risk threshold (≤ 20%) (Figs. 4A & 5A). Beyond 30%, the DCA curves converge near zero. Additionally, Kaplan–Meier (KM) survival curves were constructed to compare mortality outcomes across different patient groups, stratified by earliest measurement of PA/CRP through the different time-periods (Supplementary Figures S6-S9). For this analysis, PA and CRP values were divided into four equal quartiles, where the first quartile represented the lowest 25% of values, the second and third represented the middle 50%, and the fourth quartile represented the highest 25% of values. The KM curves for the PA models showed that across all time intervals, lower albumin quartiles (e.g. the first quartile) had higher mortality outcomes compared to higher quartiles, but the magnitude of this protective effect likely decreases with increasing time intervals (with clear distinction between each quartile in all time intervals Supplementary Figure S6 and S7).

Decision Curve Analysis (Singapore). (A) Decision curve analysis for models with earliest PA value, measured days before the day of bloodstream infection in Singapore. (B) Decision Curve Analysis for models with earliest CRP value, measured days before the day of bloodstream infection in Singapore.

Decision Curve Analysis (Denmark). (A) Decision curve analysis for models with earliest PA value, measured days before the day of bloodstream infection in Denmark. (B) Decision Curve Analysis for models with earliest CRP value, measured days before the day of bloodstream infection in Denmark.
Decision Curve Analysis graphs for patients with PA measured on D0 & ≥ 1 CRP measured up to 30 days before D0
The CRP models for both Singaporean and Danish cohorts had a positive net benefit up to 30% at low thresholds (Figs. 4B & 5B). The net benefit was maintained up to 30% threshold and after, the DCA curves approach zero, similar to the albumin models. The KM curves for the CRP models demonstrated that CRP measured closer to the infection diagnosis is better than predicting mortality with clear distinction between the different quartiles of CRP measurements; the fourth quartile (i.e. higher CRP values) had higher % mortality (Supplementary Figures S8A and S9A), compared to CRP measured up to 30 days prior to the BSI episode in both Singapore and Denmark cohorts where the quartiles (i.e. coloured lines) are closer together (Supplementary Figures S8F and S9F).
Discussion
In this study, the cohorts from tropical Singapore and Denmark with a temperate climate were similarly sized despite the differences in the climate, geography and ethnicities. The 30-day mortality in SG’s cohort were comparable to DK (SG: 17.4% vs DK: 20.2%) and also similar to mortality rates of 15% to 20% reported by other developed countries1,22,23. Moreover, Escherichia coli and Staphylococcus aureus were amongst the top four most common causative pathogens of BSI for both cohorts. It was observed that the prevalence of Streptococcus pneumoniae, Enterococcus and Coagulase-negative pathogens were markedly higher in the Danish cohort than the Singaporean cohort (SG: 1.9%, 1.2%, 0.2% vs. DK: 6.4%, 6.7%, 7.5%, respectively), which is consistent with the findings by Sim et al. (2024)5. This may be related to the difference in the prevalence of malignancy in Denmark compared to Singapore5.
The findings of our study concluded that measurement of PA level was a key prognostic biomarker of 30-day mortality risk, whether it was taken on the day of the BSI episode or taken in the 30 days prior. Furthermore, in all seven nomogram models of CRP measured in different time periods, PA measured on D0 was the highest contributing variable. PA on D-26/D-30 had a higher contribution to the prognostic predictability for 30-day mortality than CRP measured on D0. Albumin is the primary constitutive protein in the human body and performs several crucial functions such as the maintenance of appropriate osmotic pressure, binding, transportation of various substances in blood, as well as the neutralisation of free radicals24. Hypoalbuminemia is a well-established indicator of inflammation during a systemic infection and is associated with poor clinical outcomes; Previous studies found that low PA level measured at the time of BSI is a good predictor of 30-day mortality risk25,26,27. During an ongoing BSI, cytokines such as TNF-α and interleukin-1 may decrease albumin levels by controlling albumin gene expression that leads to catabolism24. Moreover, the intravascular redistribution of albumin during an ongoing infection may lead to increased capillary leakage which will significantly increase the risk of mortality. Serum albumin levels may serve as an indicator of inflammation, capillary leakage, and oxidative stress damage in severe sepsis, all of which likely to contribute to the prognostic role of albumin concentration in patients with BSI24. Similar to the findings in our study, in a meta-analysis of 90 cohort studies that evaluated hypoalbuminemia as a prognostic biomarker in acutely ill patients, each 10 g/l decrease in serum albumin concentration was associated with a 137% increase in the odds of death, an 89% increase in morbidity, and a 71% increase in length of hospital stay28.
Separately, CRP, when measured as early as 30 days before the BSI episode, is thus neither a precise indicator of whether there is improvement or deterioration of a patient’s clinical state. CRP is an acute-phase protein with a half-life of less than 24 h, and a well-established biomarker for inflammation during an infection29. In the event of a BSI, monocytic mediators such as interleukin-1 and interleukin-6 stimulate the acute-phase increase of CRP production. This facilitated the immune response by the binding of CRP to phosphocholine on the pathogen molecule and the activation and amplification of the innate immune response30. CRP concentrations increase markedly but only for a transient period, rendering one-time concentrations to be weak prognosticators31,32,33. In contrast, PA levels continue to decrease modestly and only start to increase in the event of recovery; Persistently low levels of PA can indicate poor clinical state of a patient with BSI34. Our findings showed that CRP on D0 was an insignificant and inconsistent contributor, unlike PA levels at various times prior to the incidence of BSI that were consistently high contributors to 30-day mortality risk. This suggested that CRP at D0 is not a reliable predictor of 30-day mortality risk. Additionally, earliest measurement of CRP (up to 30-days prior to BSI) contributed weakly to 30-day mortality risk, in comparison to other variables, suggesting that there is little to no prognostic value in measuring CRP early. Moreover, the AUROCs for the model adjusting for CRP increased marginally for both Singaporean and Danish cohort, demonstrating that CRP had little contribution to the prediction of 30-day mortality risk for BSI patients.
Inverse correlation between CRP on D0 and earliest PA levels was observed, and it was more evident in the D0 model. This corroborates with previous literature that reported close correlation between increases in CRP and decreases in serum albumin levels27,35,36. There were high correlation coefficients (range: 0.55/0.75 for SG; range: 0.45/0.62 for DK, all p-values < 0.001) between PA on D0 and PA in all 5-day intervals, suggesting that low PA levels can be observed in BSI patients as early as 30 days prior to the BSI episode. On the contrary, earliest CRP level measured 1–30 days before D0 had weak correlation to CRP measured on D0 (Supplementary Tables S3A and S4A), which supports previous findings32,33.
Strengths and limitations
While published studies have assessed the prognostic value of albumin and CRP levels for 30-day mortality in bloodstream infections, they have predominantly reported single measurements taken either one day before or on the day of infection. This limitation did not effectively capture the dynamic nature of these biomarkers and their potential early warning capabilities. Our study uniquely contributes to the literature by measuring albumin and CRP levels at multiple time points through a 30-day window before the onset of a bloodstream infection, a comprehensive approach not usually undertaken in previous studies. This methodology allowed us to track the temporal changes of albumin and CRP levels leading up to the infection event. Moreover, our findings demonstrated a strong association between albumin levels and 30-day mortality, with the association remaining significant even for measurement taken as early as 30 days before the bloodstream infection. This suggests that the prognostic value of albumin extends well before the immediate pre-infection period, potentially offering an early warning signal for adverse outcomes (30-day mortality). In contrast, it was observed that the prognostic value of CRP for 30-day mortality was not significant when measured prior to the day of bloodstream infection, unlike albumin.
Our study developed nomograms, which few studies have done. A regression model predicts the probability of the outcome by using a set of independent variables, but the individual outputs of the variables do not provide direct comparison with other variables. Although AUROC assess the model’s discriminatory power, it is still difficult to assess the relative impact of an individual variable. Thus, using a nomogram, which is a graphical representation of a predictive model derived from regression analyses, generates a probability of a clinical event, such as mortality, for a particular individual. Multiple variables can be included into a nomogram model, whereby the weight of each variable is computed in a points-scoring system which provide an overall scale of attributable mortality21. Nomograms are relatively simple yet intuitive. With a quick look at a nomogram model, factors of high impact (based on the points delegated) to 30-day mortality in patients with BSI are easily distinguishable to clinicians. This should serve as an indication of the patient’s poor prognosis, hence for clinicians to conduct more evaluation to stay vigilant about impending infections, for example, a suspected BSI at earliest opportunity. If there could be an early detection of BSI pathogens, it could help healthcare personnel promptly facilitate appropriate treatment for the infection.
Moreover, our study conducted in an Asian and a European population further adds to the knowledge. The healthcare systems in Singapore and Denmark use unique personal identifiers to link electronic medical records between registries, laboratory systems and health institutions, allowing for accruement of the respective 10-year cohorts and the longitudinal follow-up. Both SG and DK cohorts cover 25% and 35% of their countries’ total population, hence enabling the establishment of population-based studies which can determine the burden of BSI in the population over time with precision. This study yields informative data from two geographically distinct populations with the ability to analyse multiple risk factors that can attribute to 30-day mortality in patients with BSI. Any misclassification bias was diminished as a microbiological finding of BSI in a patient is clear and accurate. Additionally, we used the same definitions for BSI and laboratory classification of microorganism into different groups for both cohorts. Since the study included an overall large sample representing populations in two continents (Asia and Europe) across multiple years, the findings in this study may be generalized to populations in other countries.
For the DCA graphs for Singapore and Denmark, the albumin and CRP models provide a clear net benefit at low threshold probabilities (up to 20% for PA and up to 30% for CRP). CRP’s predictive value is more time-sensitive, in contrast to albumin’s stability across the time-points, hence demonstrating that albumin has consistent clinical value for early decision-making for patients with BSI, critical for clinicians aiming to intervene early and prevent complications that could lead to mortality.
However, there were limitations. First, the number of BSI patients included within each seven groups of the 5-day intervals of earliest measurements of CRP/PA were not equal and the inclusion criteria (e.g., at least two CRP or PA specimens) probably selected a frailer cohort among all the BSI patients. Nonetheless, most of our subgroups were larger than those reported in many other studies on BSI patients and as the findings were consistent, the mechanisms are likely to be similar regardless of subgroup. A selection of frailer patients may also be more clinically useful than the opposite. Baseline characteristics as well as the 30-day mortality were very similar to the bigger cohorts in the two countries5. Second, the nomograms were developed using data from hospitalised patients with available biomarker measurements spanning 0 to 30 days before the diagnosis of BSI. Hence they may not be generalizable to non-hospitalised patients and hospitalised patients without biomarker measurements prior to BSI. Third, as in most other retrospective studies there was a lack of clinical data, such as clinical symptoms. The impact of such factors on possible pathophysiological mechanisms are difficult to assess, but they are probably minor.
Conclusion
In conclusion, plasma albumin was a strong prognosticator of 30-day mortality risk for patients with BSI, even when measured up to 30 days prior to the BSI episode. CRP, although commonly measured for BSI evaluation, was not as strong a predictor of 30-day mortality risk as the measurement of plasma albumin levels. Hypoalbuminemia could be an indication to an infection when measured for patients on admission to hospital, or for patients that are at risk of post-operative infection. The strong association between plasma albumin levels and 30-day mortality makes trending of albumin levels a functional tool, when incorporated with nomogram models, to assess the improvement or deterioration of a patient’s outcome. Moreover, nomogram models can be easily applied in clinical care to prognosticate mortality risk.
Data availability
The datasets analysed are not publicly available but are available from the corresponding author on reasonable request.
References
Goto, M. & Al-Hasan, M. N. Overall burden of bloodstream infection and nosocomial bloodstream infection in North America and Europe. Clin. Microbiol. Infect. 156, 501–509. https://doi.org/10.1111/1469-0691.12195 (2013).
Leibovici-Weissman, Y., Tau, N. & Yahav, D. Bloodstream infections in the elderly: what is the real goal?. Aging Clin. Exp. Res. 33, 1101–1112. https://doi.org/10.1007/s40520-019-01337-w (2021).
Greenberg, B. M., Atmar, R. L., Stager, C. E. & Greenberg, S. B. Bacteraemia in the elderly: Predictors of outcome in an urban teaching hospital. J. Infect. 50, 288–295. https://doi.org/10.1016/j.jinf.2004.06.014 (2005).
Lee, E. H., Lee, K. H., Song, Y. G. & Han, S. H. Discrepancy of C-reactive protein, procalcitonin and interleukin-6 at hospitalization: Infection in patients with normal C-reactive protein, procalcitonin and high interleukin-6 values. J. Clin. Med. 11, 7324. https://doi.org/10.3390/jcm11247324 (2022).
Sim, P. J. et al. Comparative epidemiology of bacteraemia in two ageing populations: Singapore and Denmark. Epidemiol. Infect. 152, e74. https://doi.org/10.1017/S0950268824000645 (2024).
Singapore Department of Statistics. (2022) Population Trends 2022. https://www.singstat.gov.sg/-/media/files/publications/population/population2022.ashx. Accessed 4 March 2024.
Singapore Department of Statistics. (2022) SingStat Table Builder. https://tablebuilder.singstat.gov.sg/table/TS/M015651. Accessed 4 March 2024.
Statistics Denmark. (2022) Population Statistics 2022 https://www.statistikbanken.dk/statbank5a/default.asp?w=1440. Statistics Denmark accessed 4 March 2024.
Statistics Denmark 2022. Population Figures. https://www.dst.dk/en/Statistik/emner/borgere/befolkning/befolkningstal. Accessed 4 March 2024.
Schmidt, M. et al. The Danish health care system and epidemiological research: from health care contacts to database records. Clin. Epidemiol. 11, 563–591. https://doi.org/10.2147/CLEP.S179083 (2019).
Horan, T. C., Andrus, M. & Dudeck, M. A. CDC/NHSN surveillance definition of health care–associated infection and criteria for specific types of infections in the acute care setting. Am. J. Infect. Control 36, 309–332. https://doi.org/10.1016/j.ajic.2008.03.002 (2008).
Roberts, F. J. Definition of polymicrobial bacteremia. Rev. Infect. Dis. 11, 1029–1030. https://doi.org/10.1093/clinids/11.6.1029 (1989).
Quan, H. et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 43, 1130–1139. https://doi.org/10.1097/01.mlr.0000182534.19832.83 (2005).
Trick, W. E. et al. Computer algorithms to detect bloodstream infections. Emerg. Infect. Dis. 10, 1612–1620. https://doi.org/10.3201/eid1009.030978 (2004).
Friedman, N. D. et al. Health care-associated bloodstream infections in adults: A reason to change the accepted definition of community-acquired infections. Ann. Intern. Med. 137, 791–797. https://doi.org/10.7326/0003-4819-137-10-200211190-00007 (2002).
Møller, J. K. A microcomputer-assisted bacteriology reporting and information system. Acta Pathol. Microbiol. Scand. Ser. B: Microbiol. 92, 119–126. https://doi.org/10.1111/j.1699-0463.1984.tb02805.x (1984).
Christiansen, J. U., Maruard, C. D. & Nielsen, H. C. LABKA. A real-time computer system for the clinical laboratory. Scand. J. Clin. Lab. Investig. Suppl. 194, 57–61 (1989).
Schmidt, M. et al. The Danish National Patient Registry: A review of content, data quality, and research potential. Clin. Epidemiol. 7, 449–490. https://doi.org/10.2147/CLEP.S91125 (2015).
Newson, R. B. Comparing the predictive powers of survival models using Harrell’s C or Somers’ D. Stata J. 10, 339–358. https://doi.org/10.1177/1536867X1001000303 (2010).
Hanley, J. A. & McNeil, B. J. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology 148, 839–843. https://doi.org/10.1148/radiology.148.3.6878708 (1983).
Zlotnik, A. & Abraira, V. A general-purpose nomogram generator for predictive logistic regression models. Stata J. 15, 537–546. https://doi.org/10.1177/1536867X1501500212 (2015).
Hattori, H. et al. Epidemiology and risk factors for mortality in bloodstream infections: A single-center retrospective study in Japan. Am. J. Infect. Control 46, 75–79. https://doi.org/10.1016/j.ajic.2018.06.019 (2018).
Abernethy, J. K. et al. Thirty day all-cause mortality in patients with Escherichia coli bacteraemia in England. Clin. Microbiol. Infect. 21, 251-e1. https://doi.org/10.1016/j.cmi.2015.01.001 (2015).
Yin, M. et al. Predictive value of serum albumin level for the prognosis of severe sepsis without exegenous human albumin administration: A prospective cohort study. J. Intensive Care Med. 33, 687–694. https://doi.org/10.1177/0885066616685300 (2018).
Garvik, O. S. et al. C-reactive protein and albumin kinetics before community-acquired bloodstream infections–a Danish population-based cohort study. Epidemiol. Infect. 148, e38. https://doi.org/10.1017/S0950268820000291 (2020).
Schmidt de Oliveira-Netto, A. C. et al. Procalcitonin, C-Reactive Protein, Albumin, and Blood Cultures as Early Markers of Sepsis Diagnosis or Predictors of Outcome: A Prospective Analysis. Clinical Pathology 12, 2632010X19847673; https://doi.org/10.1177/2632010X19847673 (2019).
Wiedermann, C. J. Hypoalbuminemia as surrogate and culprit of infections. Int. J. Mol. Sci. 22, 4496. https://doi.org/10.3390/ijms22094496 (2021).
Vincent, J. L. et al. Albumin administration in the acutely ill: What is new and where next?. Crit. Care 18, 1–10. https://doi.org/10.1186/cc13991 (2014).
Husain, T. M. & Kim, D. H. C-Reactive Protein and Erythrocyte Sedimentation Rate in Orthopaedics. Univ. Pa. Orthopaed. J. 15, 13–16 (2002).
Sproston, N. R. & Ashworth, J. J. Role of C-reactive protein at sites of inflammation and infection. Front. Immunol. 9, 754. https://doi.org/10.3389/fimmu.2018.00754 (2018).
Gradel, K. O. et al. Does C-reactive protein independently predict mortality in adult community-acquired bacteremia patients with known sepsis severity?. APMIS 121, 835–842. https://doi.org/10.1111/apm.12040 (2013).
Silvestre, J. et al. Is C-reactive protein a good prognostic marker in septic patients?. Intensive Care Med. 35, 909–913. https://doi.org/10.1007/s00134-009-1402-y (2009).
Kato, A., Takita, T., Furuhashi, M., Maruyama, Y. & Hishida, A. Comparison of serum albumin, C-reactive protein and carotid atherosclerosis as predictors of 10-year mortality in hemodialysis patients. Hemodial. Int. 14, 226–232. https://doi.org/10.1111/j.1542-4758.2009.00432.x (2010).
Soeters, P. B., Wolfe, R. R. & Shenkin, A. Hypoalbuminemia: Pathogenesis and clinical significance. J. Parenter. Enter. Nutr. 43, 181–193. https://doi.org/10.1002/jpen.1451 (2019).
Gradel, K. O. et al. Hypoalbuminaemia as a marker of trans-capillary leakage in community-acquired bacteraemia patients. Epidemiol. Infect. 146, 648–655. https://doi.org/10.1017/S0950268818000274 (2018).
Gradel, K. O. et al. Longitudinal trajectory patterns of plasma albumin and C-reactive protein levels around diagnosis, relapse, bacteraemia, and death of acute myeloid leukaemia patients. BMC Cancer 20, 1–13. https://doi.org/10.1186/s12885-020-06754-z (2020).
Funding
The authors declare that there is no funding involved.
Author information
Authors and Affiliations
Contributions
Conceptualization: A.C., K.O.G.; Methodology: A.C., K.O.G.; Formal analysis and investigation: K.O.G., Z.J.P.; Supervision: A.H.A., J.E.C., M.C., S.L.N., T.G.J., J.K.M., R.B.D., P.P., K.O.G., A.C.; Reading and approval of the final manuscript: all authors (Z.J.P., A.A.H., P.J.W.S., J.E.C., M.C., S.L.N., T.G.J., J.K.M., R.B.D., P.P., K.O.G., A.C.). Z.J.P. wrote the manuscript.
Authors’ information
Contributing members of SG-DK Bacteraemia study group include Zhi Jing Phua, Aung Hein Aung, Patrick Jian Wei Sim, John Eugenio Coia, Ming Chen, Stig Lønberg Nielsen, Thøger Gorm Jensen, Jens Kjølseth Møller, Ram Benny Dessau, Pedro Póvoa, Kim Oren Gradel, Angela Chow, Olav Sivertsen Garvik, and Caroline Thingholm Thorarinsson.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Phua, Z.J., Aung, A.H., Sim, P.J.W. et al. Nomogram-based analysis of plasma albumin and C-reactive protein 30 days before bloodstream infection for 30-day mortality in Singapore and Denmark. Sci Rep 16, 4483 (2026). https://doi.org/10.1038/s41598-025-34710-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-34710-z
