
Abstract
Previous studies reported that depressive symptoms were associated with a high risk of all-cause mortality. However, the effect of different long-term depressive symptom trajectory patterns on the risk of all-cause mortality has not been evaluated. Our research aimed to explore the association between different depressive symptom trajectories and the risk of all-cause mortality in Chinese adults. The data we used were from the China Health and Retirement Longitudinal Study. In total, 13,624 subjects aged over 45 years were ultimately included in the analysis. Group-based trajectory modeling was used to identify the different trajectories of depressive symptoms. The multivariable Cox regression model was used to examine the association between long-term depressive symptom trajectories and all-cause mortality. The results show that a total of five depressive symptom trajectories were identified in our study, including stable-low, stable-moderate, increasing, decreasing and stable-high. Compared with individuals in the stable-low depressive symptom trajectories group, those in the increasing and stable-high trajectory groups possessed a greater mortality rate, with a multivariable-adjusted hazard ratio (95% CIs) for mortality were 1.30 (1.06, 1.60) and 1.59 (1.26, 2.02), respectively. In addition, we have not identified the significant risk of all-cause mortality in people with decreased and stable-moderate symptom trajectories. Moreover, the risk of all-cause mortality had an increasing trend among the different trajectory groups. In the sensitivity analysis, the association was robust in most of the subgroups. In conclusion, people with increasing and persistent higher depressive symptom trajectories were associated with an increased risk of all-cause mortality.
Similar content being viewed by others


Introduction
Depression has become a common problem and major public health concern worldwide. Moreover, the prevalence of depression has increased to a higher level1. One meta-analysis showed that 34% of adolescents globally are at risk of developing clinical depression2. According to studies in China, the prevalence of clinically significant depressive symptoms was 18% in a month-long observation period3. It has been confirmed to increase the risk for cardiovascular disease, dementia, and suicidal ideation4,5,6. Moreover, the combination of these illnesses and depression can worsen existing medical issues. The Global Burden of Disease Study in 2019 reported that over 45 million all-age disability-adjusted life-years (DALYs) were contributed by depression7. Thus, the effect of depression or depressive symptoms on mortality has also been evaluated in recent decades. Lots of population-based cohort studies indicated that depressive symptoms were significantly associated with higher mortality8,9,10,11. In this study, the definition of a depressive state was only based on one-time measured depressive symptoms. However, depressive symptoms may fluctuate over the lifetime of people. As we all know depressive symptoms frequently improve with treatment, remission periods, and personal resilience. Moreover, the course of depression is inherently variable, influenced by factors such as life events, social support, and biological changes. One previous study showed that almost 20% of the total participants had great depressive symptom changes in a 4 years follow-up survey12. Nevertheless, few studies have evaluated the effect of long-term trajectories of depressive symptoms on mortality.
Therefore, our study aimed to present the different long-term trajectories of depressive symptoms, and explored their effect on all-cause mortality in Chinese middle-aged and elderly adults. We hypothesized that individuals with low to high depressive symptoms, high to low depressive symptoms, and persistent high depressive symptoms were significantly associated with all-cause mortality.
Methods
Data sources and study population
In the current study, the data we used were obtained from the China Health and Retirement Longitudinal Study (CHARLS), a nationwide, ongoing cohort of Chinese adults aged 45 years or older. The CHARLS was designed to assess changes in the social, economic and health circumstances of community residents. As a longitudinal study, the national baseline survey was conducted in June 2011 and March 2012, which included 17,708 respondents from 10,257 households. To date, CHARLS researchers have conducted four follow-up surveys in 2013, 2015, 2018 and 2020. The details of the design and sampling methods of the CHARLS have been described elsewhere13.
Data from the five survey waves, which were conducted from 2011 to 2020, were used in the current study. After excluding participants without follow-up tracking data or depressive symptom data, those under 45 years old, and those without the death information, 13,624 subjects were ultimately included in the analysis. The participant selection flow chart is shown in Fig. 1. All the participants signed informed consent forms, and all methods were performed in accordance with the relevant guidelines and regulations. This study was approved by the Ethics Review Committee of Peking University.

The participant selection flowchart.
Depressive symptoms and trajectories
Depressive symptoms were evaluated by the Center of Epidemiologic Studies Depression Scale-10 (CESD-10). The CESD-10 has been validated and widely used in the measurement of depression symptoms in China14,15. The CESD-10 consists of 10 items, including optimistic and negative states. Every item had four response levels, which were recorded as 0, 1, 2 and 3; thus, the sum scores of the CESD-10 ranged from 0 to 30, with a higher score indicating a greater level of depression. In our study, the trajectories of depressive symptoms surveyed in 2011, 2013 and 2015 were defined as the exposed variable, and whether participants died in 2018 and 2020 was defined as the outcome, details are shown in Fig. 2.

Timeline of exposure and follow-up assessment.
Assessment of mortality and covariates
We divided the participants into two groups based on their mortality status in 2018 and 2020 (alive or dead). The residential location was also divided into two groups based on the household living region of the population: urban and rural. Education levels were divided into three levels: college or above, middle or high school, and elementary school or below. Hypertension was defined as systolic blood pressure ≥ 140 mmHg, diastolic blood pressure ≥ 90 mmHg, self-reported hypertension, or taking antihypertensive medication. Diabetes was defined as Hab1c ≥ 6.5, self-reported diabetes, or receiving any medical treatment16. Smoking status and alcohol consumption were defined according to whether residents have engaged in these behaviors at any point (yes/no). BMI (kg/m2) was calculated as weight divided by height squared. In addition, the diagnosis of other diseases, including cancer, diabetes, heart disease, and stroke was based on self-reported information.
The survival time was calculated based on the time from wave 3 to wave 5 when people were alive. If participants die, the survival time is calculated from wave 3 to the time of death. If participants died and lacked a specific time of death, the death time was defined as the median of two adjacent wave intervals.
Statistical analysis
Data analysis was conducted by using the statistical analysis software package SAS 9.4 (SAS Institute Inc., Cary, North Carolina, USA). Group based trajectory modeling (GBTM) can identify latent clusters of individuals who are following similar trajectories of a particular indicator of interest17. In our study, GBTM for participants was performed by the PROC TRAJ procedure, and those without all three waves of depressive symptom survey data were handled under the missing-at-random assumption. When GBTM was used to identify the different trajectories of depressive symptoms, we started from one trajectory model to six trajectory models and fit those trajectories up to the optimal number by comparing the Bayesian information criterion. Moreover, the number of participants in every trajectory group was greater than 5% of the total number of participants in each trajectory group.
Continuous and categorical variables are presented as the mean ± standard deviation (SD) and frequency (percentage), respectively. Continuous variables were compared between participants with different depressive symptom trajectories by ANOVA or the Kruskal-Wallis test. A chi-square test was used to detect significant differences in categorical variables. The hazard ratio (HR) and 95% confidence interval (CI) for mortality were calculated by using a multivariable Cox regression model, with the trajectory of the stable-low symptoms group as the reference. Additionally, we investigated a potential dose-response relationship (P trend) based on median values of CESD-10, employing HRs and 95% CI. The significance level was set at 0.05 (two-sided).
Results
Baseline characteristics and depressive symptom trajectories
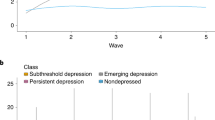
In the present research, 13,624 participants (6496 men and 7128 women) were included in the analysis, and the average age was 58.4 ± 9.0 years. A total of five depressive symptom trajectories were identified in our study (Fig. 3). Trajectory 1 (stable-low symptoms trajectory) included 4894 participants (35.9%) with an average CESD-10 score consistently < 3.5 during follow-up. Trajectory 2 (stable-moderate symptoms trajectory) included 5250 participants (38.5%) whose average CESD-10 score was consistently stable between 8.3 and 7.8 during the follow-up. Trajectory 3 (increasing symptoms trajectory) included 1193 participants (8.8%) with an average CESD-10 score that increased from 9.4 to 18.8. Trajectory 4 (decreasing symptoms trajectory) included 1539 participants (11.3%) whose average CESD-10 score decreased from 18.1 to 10.6. Trajectory 5 (stable-high symptoms trajectory) included 748 participants (5.5%) with an average CESD-10 score consistently > 19.8 during follow-up. All of the baseline characteristics were not balanced between the different groups (Table 1).

Trajectory grouping of depressive symptoms during 2011, 2013 and 2015.
Association between depressive symptom trajectories and all-cause mortality risk
The HRs (95% CIs) for the risk of all-cause mortality according to the depressive symptom trajectories are shown in Table 2. During the follow-up period from 2015 to 2020, 1194 deaths were reported, for a mortality rate of 8.7%. Subjects with increasing and stable-high depressive symptom trajectories possessed a greater mortality risk than those with stable-low depressive symptom trajectories. After adjusting for age, sex and other covariates, the multivariable-adjusted HRs (95% CIs) for mortality risks were 1.30 (1.06,1.60) and 1.59 (1.26,2.02) among participants in the increasing and stable-high trajectory groups, respectively. Moreover, the risk of mortality had an increasing trend among the different trajectory groups, and we have not identified the significant risk of all-cause mortality in people with decreased and stable-moderate symptom trajectories. In addition, the Kaplan-Meier survival curve showed individuals in the stable-high depressive symptom trajectories had the highest risk of mortality (Supplementary Fig. 1).
Stratified analyses of depressive symptom trajectories and all-cause mortality
In the sensitivity analysis, we explored the associations between different depressive symptom trajectories and the risk of mortality in the subgroup of sex, age BMI, hypertension, diabetes, smoking and alcohol status (Table 3). After adjusting a series of covariates, most of the results were consistent with those in Table 2.
Discussion
In this longitudinal study, we discovered heterogeneous depressive symptom trajectory patterns in a large cohort of 13,624 middle-aged and elderly people in China, and 5 unique depressive symptom trajectory groups were identified through the three investigations from 2011 to 2015. We found that subjects with the increasing and stable-high depressive symptoms trajectories possessed higher all-cause mortality than those with the stable-low depressive symptoms trajectory. Furthermore, we have not identified the significant risk of all-cause mortality in people with decreased and stable-moderate symptom trajectories.
Previous studies have indicated that significant positive relationship between depressive symptoms and the risk of all-cause mortality18,19,20. These researches provide important evidence about the impact of depression states at a single time point on the risk of all-cause mortality. However, the definition of a depressive state was only based on one-time measured depressive symptoms, which was always determined by the first survey. The process of depression in different populations is unique and varies with changes in influencing factors. Thereby, the study of the relationship between depressive symptoms and outcomes should utilize the process of depressive symptoms rather than a single measurement result.
Currently, few studies have reported the association between the long-time trajectories of depressive symptoms and all-cause mortality. In a previous cohort study in the United States, five depressive symptom trajectories were identified among 7810 US residents aged 50 years and older. It showed that when compared to the non-depressive trajectory group, the group with depressive symptoms trajectory had a significantly greater risk of all-cause mortality21. Nevertheless, the percentage of participants in the persistent depressive trajectory group and the improving depressive trajectory group were both less than 5%, which is seriously unbalanced and may affect the results. Another longitudinal cohort study from London used a population-based trajectory model to determine the trajectory of depression and concluded that an increase in depressive symptoms is associated with higher mortality rates22. These findings in stroke patients are consistent with our results. In our study, the individuals with high-stable trajectories (CESD-10 score > 19.8) have the highest risk of mortality, which increased by 59%. One prospective cohort study also reported there was a graded positive association between depressive symptoms and mortality23. Moreover, previous research shows that approximately 13.2% of patients with depression have a chronic course of more than two years24. Meanwhile, individuals with long-term high-level depressive symptoms are more likely to be diagnosed with depression or anxiety, indicating that individuals with this trajectory either already suffer from clinical depression or will continue to suffer in the future25. Thus, from a clinical perspective, this group is highly noteworthy. Drug intervention, resistance exercise training, improvements in quality of life, and positive psychological intervention can all improve depressive symptoms26,27,28,29. Importantly, in our study, we have not identified the risk of all-cause mortality in people with decreased symptom trajectories, when their average CESD-10 score decreased from 18 to 10.8. The all-cause mortality risk of this population could have been overestimated in previous studies. Meanwhile, our results show people with increasing depression symptom trajectories have a high risk of all-cause mortality. Those individuals did not reach the cut-off point for depression symptoms assessment with a CESD-10 score in the first survey, and this group of people is often regarded as normal. Importantly, such individuals usually overlook the risk of all-cause mortality in most single depression assessments. For this reason, our research better elucidated the association between long-term depression and all-cause mortality in Chinese adults. It indicates that through extensive long-term follow-up, a more comprehensive understanding of residents’ depression status and its evolving trends can facilitate timely interventions, potentially leading to a significant reduction in all-cause mortality associated with depression.
The potential mechanisms linking depressive symptoms trajectories and all-cause mortality could be attributed to several arguments. First, from a biological perspective, depression and depressive symptoms are usually accompanied by dysregulation of biofeedback mechanisms, such as disturbances in the activity of the HPA axis30,31, which can contribute to cardiovascular mortality, cancer and suicide behavior, all of these can increase the risk of all-cause mortality32,33,34. Second, the interaction between long-term depression and inflammation may increase the risk of all-cause mortality. Depression can prime larger cytokine responses to pathogens or stressors, leading to immune dysregulation and activation of the inflammatory response system (IRS)35. Meanwhile, proinflammatory cytokines, such as interleukin (IL)-1β, IL-2, IL-6 and interferon-gamma, can contribute directly to the development of depressive symptoms36. More importantly, these cytokines can facilitate the development of chronic diseases, such as inflammatory bowel disease, by causing tissue damage and triggering persistent inflammation37. And the formation of this comorbidity undoubtedly increases the risk of death. Third, individuals with depression may have a higher likelihood of engaging in unhealthy behaviors, including physical inactivity and unfavourable dietary intake38,39, all of which are recognized as the leading causes of all-cause mortality. Thus, the long-term high depressive symptoms could greatly increase the risk of all-cause mortality through these possible mechanisms and pathways.
The strengths of this study include the large sample size of participants in a national cohort. Additionally, our study provides a valid appraisal of the association between long depressive symptom trajectories and all-cause mortality in Chinese adults. Moreover, a lot of potential confounders were adjusted in the multivariable models. However, several limitations also exist in our study. First, the depression states of participants were defined based on the CESD, which may have led to information bias. However, the reliability of CESD has been proven, and the scale has been widely used in the assessment of depression. Second, some participants were lost to follow-up and were excluded, which may have caused selection bias. Third, self-reported hypertension and diabetes information were dependent on participants’ memory and awareness, which lacked clinical verification and may lead to inaccuracies.
In conclusion, people with increasing (from normal to high) and persistent higher depressive symptom trajectories were associated with an increased risk of mortality, while the risk of individuals with decreasing depressive symptoms is probably overestimated. Moreover, it is worth noting that multiple waves of surveys for depressive symptoms can provide some new understanding for specialists and the government regarding the association between long-term depression and mortality.
Data availability
The datasets analysed during the current study are available in the CHARLS repository, www.g2aging.org.
References
Liu, Q. et al. Changes in the global burden of depression from 1990 to 2017: findings from the Global Burden of Disease study. J. Psychiatr. Res. 126, 134–140 (2020).
Shorey, S., Ng, E. D. & Wong, C. H. J. Global prevalence of depression and elevated depressive symptoms among adolescents: a systematic review and meta-analysis. Br. J. Clin. Psychol. 61(2), 287–305 (2022).
Meng, R. et al. Association of depression with all-cause and cardiovascular disease mortality among adults in China. JAMA Netw. Open. 3(2), e1921043 (2020).
Bennett, S. & Thomas, A. J. Depression and dementia: cause, consequence or coincidence? Maturitas 79(2), 184–190 (2014).
Zhang, Y., Chen, Y. & Ma, L. Depression and cardiovascular disease in elderly: current understanding. J. Clin. Neurosci. 47, 1–5 (2018).
Rotenstein, L. S. et al. Prevalence of depression, depressive symptoms, and suicidal ideation among medical students: a systematic review and meta-analysis. Jama 316(21), 2214–2236 (2016).
He, D. et al. Association between dietary quality and prediabetes based on the diet balance index. Sci. Rep. 10(1), 3190 (2020).
Holwerda, T. J. et al. Impact of loneliness and depression on mortality: results from the Longitudinal Ageing Study Amsterdam. Br. J. Psychiatry 209(2), 127–134 (2016).
Thomson, W. Lifting the shroud on depression and premature mortality: a 49-year follow-up study. J. Affect. Disord. 130(1–2), 60–65 (2011).
Paljärvi, T. et al. Mortality in psychotic depression: 18-year follow-up study. Br. J. Psychiatry. 222(1), 37–43 (2023).
Das-Munshi, J. et al. Depression and cause-specific mortality in an ethnically diverse cohort from the UK: 8-year prospective study. Psychol. Med. 49(10), 1639–1651 (2019).
Zheng, X. et al. Distinct depressive symptom trajectories are associated with incident diabetes among Chinese middle-aged and older adults: the China Health and Retirement Longitudinal Study. J. Psychosom. Res. 164, 111082 (2023).
Zhao, Y. et al. Cohort profile: the China Health and Retirement Longitudinal Study (CHARLS). Int. J. Epidemiol. 43(1), 61–68 (2014).
Zhou, L., Ma, X. & Wang, W. Relationship between cognitive performance and depressive symptoms in Chinese older adults: the China Health and Retirement Longitudinal Study (CHARLS). J. Affect. Disord. 281, 454–458 (2021).
Jing, R. et al. Longitudinal association between sleep duration and depressive symptoms in Chinese elderly. Nat. Sci. Sleep. 12, 737–747 (2020).
Danne, T. et al. International consensus on use of continuous glucose monitoring. Diabetes Care 40(12), 1631–1640 (2017).
Nagin, D. S., Jones, B. L. & Elmer, J. Recent advances in group-based trajectory modeling for clinical research. Annu. Rev. Clin. Psychol. 20(1), 285–305 (2024).
Parker, E. D. et al. Change in weight status and development of hypertension. Pediatrics 137(3), e20151662 (2016).
Park, S. H. et al. Depressive symptoms and all-cause mortality in Korean older adults: a 3-year population-based prospective study. Geriatr. Gerontol. Int. 18(6), 950–956 (2018).
Chekroud, S. R. et al. Association between physical exercise and mental health in 1.2 million individuals in the USA between 2011 and 2015: a cross-sectional study. Lancet Psychiatry 5(9), 739–746 (2018).
Wu, T. et al. The trajectories of depressive symptoms and subsequent incident dementia, coronary heart diseases, stroke and all-cause mortality. J. Affect. Disord. 312, 9–16 (2022).
Ayis, S. A. et al. Sex differences in trajectories of depression symptoms and associations with 10-year mortality in patients with stroke: the South London Stroke Register. Eur. J. Neurol. 26(6), 872–879 (2019).
Zhang, Z. et al. Depressive symptoms and mortality among US adults. JAMA Netw. Open 6(10), e2337011 (2023).
Hasin, D. S. et al. Epidemiology of major depressive disorder: results from the national epidemiologic survey on Alcoholism and related conditions. Arch. Gen. Psychiatry 62(10), 1097–1106 (2005).
Musliner, K. L. et al. Heterogeneity in long-term trajectories of depressive symptoms: patterns, predictors and outcomes. J. Affect. Disord. 192, 199–211 (2016).
Peixoto, C. et al. Dehydroepiandrosterone for depressive symptoms: a systematic review and meta-analysis of randomized controlled trials. J. Neurosci. Res. 98(12), 2510–2528 (2020).
Gordon, B. R. et al. Association of efficacy of resistance exercise training with depressive symptoms: meta-analysis and meta-regression analysis of randomized clinical trials. JAMA Psychiatry 75(6), 566–576 (2018).
Tang, A. L. & Thomas, S. J. Relationships between depressive symptoms, other psychological symptoms, and quality of life. Psychiatry Res. 289, 113049 (2020).
Sin, N. L. & Lyubomirsky, S. Enhancing well-being and alleviating depressive symptoms with positive psychology interventions: a practice-friendly meta-analysis. J. Clin. Psychol. 65(5), 467–487 (2009).
Menke, A. The HPA axis as target for depression. Curr. Neuropharmacol. 22(5), 904–915 (2024).
Fiksdal, A. et al. Associations between symptoms of depression and anxiety and cortisol responses to and recovery from acute stress. Psychoneuroendocrinology 102, 44–52 (2019).
Cui, B. et al. Cancer and stress: NextGen strategies. Brain Behav. Immun. 93, 368–383 (2021).
Jokinen, J. & Nordström, P. HPA axis hyperactivity and cardiovascular mortality in mood disorder inpatients. J. Affect. Disord. 116(1–2), 88–92 (2009).
Berardelli, I. et al. The involvement of hypothalamus-pituitary-adrenal (HPA) axis in suicide risk. Brain Sci. 10, 9 (2020).
Dowlati, Y. et al. A meta-analysis of cytokines in major depression. Biol. Psychiatry 67(5), 446–457 (2010).
Zeng, Y. et al. The core inflammatory factors in patients with major depressive disorder: a network analysis. Front. Psychiatry 14, 1216583 (2023).
Neurath, M. F. Strategies for targeting cytokines in inflammatory bowel disease. Nat. Rev. Immunol. 24(8), 559–576 (2024).
Liang, J. et al. Association between joint physical activity and dietary quality and lower risk of depression symptoms in US adults: cross-sectional NHANES study. JMIR Public. Health Surveill. 9, e45776 (2023).
Kandola, A. et al. Physical activity and depression: towards understanding the antidepressant mechanisms of physical activity. Neurosci. Biobehav Rev. 107, 525–539 (2019).
Acknowledgements
This analysis uses data from the Harmonized CHARLS dataset and Codebook, Version D as of June 2021 developed by the Gateway to Global Aging Data.
Author information
Authors and Affiliations
Contributions
Y. F, D. H and C. G designed the research; Y. F and C. G analyzed the data; Y. F, D. H and L. C wrote the manuscript; Y. F, D. H, L. C and C. G revised the manuscript. All the authors have approved the final version of this manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Fan, Y., He, D., Chen, L. et al. Association between the depressive symptom trajectories and all-cause mortality in Chinese middle-aged and elderly adults. Sci Rep 15, 879 (2025). https://doi.org/10.1038/s41598-025-85177-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-85177-x
