
Abstract
Traditional obesity-related public health messaging often includes physical activity (PA) recommendations. However, at the population level, the data are conflicting, especially when comparing different self-reported vs. measured techniques across different settings and populations. We measured the association between moderate-to-vigorous intensity PA (MVPA) and prospective weight change across five African-origin populations and the extent to which MVPA attenuated weight change over time. At baseline, 2,500 adults (median age: 37y) were recruited into the Modelling the Epidemiologic Transition Study (METS), from Ghana, South Africa, Jamaica, Seychelles, and US. 2000 participants were followed up 8 years later, with 851 participants having complete 7-day accelerometry to measure MVPA at both time points. Generalised estimating equations were used to explore the longitudinal association between weight and MVPA adjusted for several confounders. The obesity prevalence at baseline was 27.5% which increased to 38.0% at follow-up. Baseline MVPA varied from 7 (IQR: 4, 16) min/day in US women to 52 (IQR: 36, 78) min/day in South African men, and similarly at follow-up ranged from 8 min/day to 41 min/day among the same participant groups. While overall, engaging in higher MVPA levels was associated with a lower body weight, such that every additional 30 min of MVPA equalled a 600 g lower body weight (p = 0.04), the interaction between time and MVPA was not statistically significant (p = 0.18). Therefore, regardless of the amount of MVPA at any time point, body weight increased over time. Despite the association between MVPA and weight, our results suggest that objectively measured longitudinal MVPA was not associated with the change in 8-year weight in African-origin adults. Our research confirms that while PA is a critical determinant of cardiovascular health, it alone may not be enough to stem the rising obesity burden.
Similar content being viewed by others
Introduction
As of 2022, the World Health Organisation (WHO) estimates that more than 1 billion people are living with obesity worldwide1. While the burden has historically been highest in high-income countries, such as the United States (US), the epidemiologic transition, characterised by rapid urbanisation and nutrition transitions, has resulted in a rapidly worsening disease burden in low- and middle-income countries2. In fact, it is estimated that 78% of global adult deaths attributable to high body mass index (BMI) occur in low-to middle-income countries3.
Physical activity (PA), defined as any bodily movement that results in energy expenditure4,5, is an important component of energy balance6. Consequently, the WHO has issued a global PA action plan and published new daily PA guidelines5,7,8. The guidelines distinguish between the importance of different intensities of PA, including light-, moderate-, and vigorous-intensity PA. Despite these extensive public health efforts, the global prevalence of insufficient physical inactivity has remained relatively stable9 while obesity prevalence continues to rise. Nonetheless, specialist and government organisations advocate for increased PA to prevent weight gain10. To be clear, it is irrefutable that purposeful exercise or engaging in higher levels of PA is critical for improving cardiorespiratory fitness, which in turn plays an important role in reducing morbidity and mortality5,6,11,12,13,14. However, the evidence regarding the role of habitual PA in preventing obesity and promoting prospective weight loss remains conflicting15,16,17,18,19,20,21,22,23,24. Notwithstanding, supervised, purposeful exercise has been shown to have some weight loss benefits when either used alone22,23 or in combination with dietary interventions25,26.
Many studies exploring the relationship between weight gain and PA have relied on self-report measures, such as questionnaires, particularly at the population level, as opposed to using objective measures, such as actigraphy16,20,21,27,28. Compared to objectively measured PA, self-reported PA has been shown to poorly estimate total volume and/or intensity of PA owing to recall bias, and generally results in an overestimate29,30. In addition, there is no consistency in the dynamics of the obesity epidemic and long-term trends in PA at a population level17,31. On the other hand, studies have found that PA impacts metabolic functioning32, and some experts argue that a decline in population-based PA levels is instrumental in the obesity epidemic16,18,33.
Lifestyle changes resulting from urbanisation in low- to middle-income countries may significantly contribute to the increase in obesity worldwide15. Investigating the patterns of PA in populations at different stages of this transition, with varying degrees of obesity, may provide insights into the role of PA as such a risk factor34. The Modeling the Epidemiologic Transition Study (METS) is a well described cohort study of prospective weight change in adults of predominantly African descent from lower socio-economic communities within five countries, spanning the epidemiologic transition10,16. Previously, it was shown that baseline PA is not associated with 2-year prospective weight change16. In the current study, the follow-up period was extended to 8 years and included change in MVPA levels. The overall aim of the current analysis is to explore the association between objective MVPA and prospective weight change in the same 5 METS cohorts.
Methods
Study design and settings
METS was originally initiated in 2009 to investigate the relationships between body composition, PA, prospective weight change and cardiometabolic disease risk in five African-origin populations (Ghana, South Africa, Jamaica, Seychelles, and the US). In 2017, METS-Microbiome, a follow-up study of METS, was initiated35. Detailed protocols from both METS and METS-Microbiome have been published10,35. The Ghanaian study site is in rural Nkwantakese, home to approximately 5,000 residents. Khayelitsha, South Africa’s study site, and sixth largest township, is adjacent to the city of Cape Town and home to approximately 400,000 people10,36. The Seychelles study population was recruited from Victoria which is on the main island, Mahé, and home to approximately 28,000 people. The Jamaican study site is in Spanish Town, a suburb of Kingston, the country’s capital and largest city. Maywood, the study site in the US, is a low-income African American community adjoining the western border of Chicago, Illinois10. These five sites were purposefully selected to represent the “epidemiologic transition” spectrum, with Ghana and the US as opposite ends of the Human Development Index (HDI) spectrum35.
Recruitment and enrolment
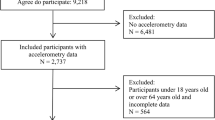
METS enrolled approximately 2,500 adults (n = 500 per study site) between the ages of 25 and 45 years between January 2010 and September 2011. Subsequently, METS-Microbiome enrolled approximately 2000 of the original METS participants (n = 400 per study site), then aged between 35 and 55 years, between January 2017 and December 2019. Potential participants were excluded from METS, and in turn METS-Microbiome, if they had any self-reported infectious diseases (including active malaria and Human Immunodeficiency Virus (HIV)), were pregnant or lactating women, or had conditions which impair everyday physical activities, e.g., severe osteo- or rheumatoid arthritis, or any lower body disability10,34,35.
The protocols for METS and METS-Microbiome were approved by the Institutional Review Board of Loyola University Chicago, IL, US; the Committee on Human Research Publication and Ethics of Kwame Nkrumah University of Science and Technology, Kumasi, Ghana; the Human Research Ethics Committee of the University of Cape Town, South Africa; the Board for Ethics and Clinical Research of the University of Lausanne, Switzerland; and the Ethics Committee of the University of the West Indies, Kingston, Jamaica. All participants provided written informed consent10,34,35. The protocol for the current analysis was also approved by the University of Cape Town’s Human Research Ethics Committee (HREC ref: 632/2022). All methods were completed in accordance with relevant guidelines and regulations.
Research procedures and data collection methods
As per standardised protocols, participants completed extensive questionnaires and attended the METS research sites to undergo clinical health measures and receive accelerometers for the objective measurement of PA. All data collection methods were the same at both time points (i.e., METS baseline and METS-Microbiome, hereafter referred to as “baseline” and “follow-up” respectively). All measurements were completed in the early morning10,37, with participants arriving at the study sites following an overnight fast.
Clinical measures and health history
Measurements involving weight and height were performed, after participants were asked to remove their shoes, while wearing only lightweight clothing. Weight (kg) was recorded to the nearest 0.1 kg, and height (cm) was recorded to the nearest 0.1 cm. Waist and hip circumferences (in centimeters) were measured to the closest 0.1 cm at both the umbilicus, and the point of maximum protrusion of the buttocks, respectively. BMI was calculated from weight and height as kg/m234. Body composition was estimated using bioelectrical impedance analysis (BIA) using a single-frequency (50 kHz) impedance analyser (model BIA 101Q; RJL Systems, Clinton Township, MI). Fat mass (kg) was estimated using an equation previously validated in the METS cohorts which incorporated measured resistance10,16. Finally, all participants completed a detailed health history questionnaire, which included socio-demographic information.
Physical activity measurement
The Actical accelerometer (Phillips Respironics, Bend, OR, US) was used to objectively measure PA, as has been previously described34,37. Briefly, the accelerometer was worn at the level of the waist just behind the right hip, continuously over an 8-day period34. This period yielded six full days (i.e., 8 days of wearing the monitor with two partial days on either end of the period). The original METS study was able to determine that this amount of wear time provides a good level of reliability with an interclass correlation coefficient of 0.83–0.92 across the five sites10. The time period for assessing PA conducted daily was between 07:00 and 23:00, and this was done to standardise the measurements as there are no global guidelines surrounding the definition of sleep-time vs. awake-time for accelerometery data which is collected for a 24-hour period37.
For data analysis, we first determined non-wear time defined as ≥ 90 min of consecutive zero activity counts by running the raw data from the accelerometers through a SAS macro programme10. This criterion was formed on visual inspection of the wear/non-wear patterns across a range of different string-length criteria in a subset of files from each country37. For a days’ entry to be valid, the measurement period should include at least 10 h of daytime wear time, i.e., wearing the accelerometer for ≥ 62% of available wear time. A participant’s PA dataset was considered for analysis if it contained at least four valid days of PA measurement34.
Raw accelerometer data are converted to “activity counts”, corresponding with the frequency and magnitude of acceleration, for subsequent analysis. This allows for the use of published cut-point thresholds to assess sedentary behaviour, light-, moderate- and vigorous-intensity PA from the accelerometer data as follows: sedentary behaviour < 100 counts per minute (cpm), light-intensity PA: 101–1534 cpm, moderate-intensity PA 1535–3959 cpm and vigorous-intensity PA ≥ 3960 cpm38,39. The same protocol which was used for the National Center for Health Statistics analysis of accelerometery data in the National Health and Nutrition Examination Survey (NHANES) was used to define minutes40 spent in PA intensities (and for the purposes of this study, included only sedentary, moderate, vigorous, or moderate- and vigorous-intensity PA (MVPA)), presented as the overall time in minutes combined in intervals of either 1- or 10-minutes37. As was used in the NHANES study protocol, the current study made allowances for up to 2 min of below threshold count activity before acknowledging that an activity bout had ended, and therefore the 10-minute interval should be regarded as a modified 10-minute bout10,37,40. Total activity counts divided by total wear time is used as an overall measure of daily PA intensity37. Average counts and time spent in 1-minute bouts of MVPA, and sedentary behaviour time are also included. For the purposes of these analyses, MVPA measured in 1-minute bouts were used.
Statistical analysis
Data analysis was conducted using R (version 4.2.2, Posit, PBC, Boston, MA). Descriptive statistics were used to summarise participant characteristics at each of the study sites, through medians and interquartile ranges (IQR) for continuous measures and proportions for categorical variables (Table 1). All tables are sequenced by country according to their HDI ranking, from lowest (Ghana) to highest (US). PA was described as the median (IQR) total number of minutes which a person moves in a day, and then the number of minutes the person moves in each intensity category (sedentary, moderate, and vigorous). Overweight and obese were considered as categorical variables according to the established BMI cut-offs of 25–29.9 kg/ m2 and ≥ 30 kg/m2, respectively. Following data cleaning, including removal of participants with no valid PA data, results were stratified according to site and sex.
Generalised estimating equations (GEEs)
GEEs were used to explore the association between longitudinal weight change and MVPA over time as a main exposure. Due to its robustness in handling the within-subject correlations, GEEs are particularly suited for analysing correlated data structures typically encountered in longitudinal studies with repeated measures designs. Due to the continuous outcome variable (weight), a linear link function was used in the GEE model. An exchangeable correlation structure was used due to time being binary (i.e., baseline and follow-up). A GEE model was used with PA measured at both time points, and the model was run with and without an interaction between MVPA and time. Age, sex, site, and obesity (time varying) were included as covariates due to their relevance in testing whether PA impacts prospective weight change over the given time-period. Sensitivity analysis included fitting the same models described above but stratified by obesity status at baseline. For ease of model interpretation, MVPA per day was reported in bouts of 30 min/day.
Results
Demographic and health-related findings
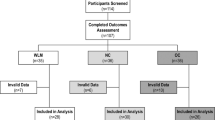
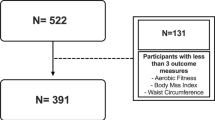
Participant characteristics are presented in Table 1. At baseline, METS recruited 2,506 participants, while METS-Microbiome completed follow-up in 1,518 participants. From this, 851 participants had complete, valid PA datasets available at both time points. The descriptive characteristics for all participants, at both time-points, are provided in Supplementary Table 1 (Baseline) and 3 (Follow-up). Of note, BMI, sex and MVPA of the final sample for the current analysis (n = 851) were all similar to those in the group without follow-up PA data (n = 1473). The median age at baseline was 37 (IQR: 31, 41) years and the median age at follow-up was 44 (IQR: 39, 49) years. Overall, the median weight increased between baseline and follow-up for both men and women and at every site except for the US site (n = 114), where weight decreased slightly for men (87 [76,109] kg vs. 85 [74,101] kg) and remained stable for women (97 kg [77, 111] kg and 97 [83, 113] kg).
The measures of adiposity were generally consistent with countries’ HDI ranking – the lower ranking countries had lower adiposity while the higher-ranking countries had higher adiposity. Among men, the highest median BMI was found in the Seychellois participants (28 kg/m2, IQR: 24, 31), followed closely by the US men (28 kg/m2, IQR: 24, 34). Obesity prevalence doubled from baseline to follow-up in the Ghanaian (3–6%), South African (2–4%), and Jamaican (4–7%) men. Although US participants remained the most obese population, the prevalence decreased from baseline to follow-up in this group (50–35%). Among the women, Ghanaian participants had the lowest median BMI (28 kg/m2; IQR: 24, 31), and the lowest obesity prevalence (35%). While women consistently had a notably higher obesity prevalence than men at each site at follow-up, more than half of the women from each country were overweight or obese. Of concern is that 74% of the US females were obese.
Physical activity parameters
Accelerometer-derived PA data are presented in Table 2; Figs. 1 and 2. South African men recorded the highest MVPA at baseline (52 min/day; IQR: 36, 78) and follow-up (41 min/day; IQR: 31, 65), reflecting substantial time spent in this intensity of PA. In contrast, US men had the lowest MVPA at baseline (22 min/day; IQR: 11, 42) and follow-up (15 min/day; IQR: 8, 33). Among the women, Ghanaians had the highest MVPA at baseline (23 min/day; IQR: 14, 36) and follow-up (16 min/day; IQR: 8, 30), whereas women in the US had the lowest MVPA at both baseline (7 min/day; IQR: 4, 16) and follow-up (8 min/day; IQR: 2, 15).

Median MVPA for men by timepoint and site (n = 362). Data are presented as median, interquartile ranges, maximum and minimum. MVPA: moderate-to-vigorous intensity PA; GH: Ghana, RSA: South Africa, JA: Jamaica, SEY: Seychelles, USA: United States.

Median MVPA for women by timepoint and site (n = 489). Data are presented as median, interquartile ranges, maximum and minimum. MVPA: moderate-to-vigorous intensity PA; GH: Ghana, RSA: South Africa, JA: Jamaica, SEY: Seychelles, USA: United States.
Associations between MVPA and prospective weight change
The GEE models evaluating the association between MVPA at both timepoints, and prospective weight change are presented in Table 3. While overall, engaging in higher levels of MVPA was associated with lower body weight (Model 1a). For every additional 30 min/day spent in MVPA at a particular time point (i.e., either baseline or follow-up), weight at that timepoint was approximately 0.63 kg (0.04–1.22 kg decrease, p = 0.04) lower on average, when accounting for covariates such as sex, age, obesity, site and time point (Model 1b). However, the interaction term between time and MVPA was not found to be statistically significant (p = 0.16), indicating that the extent to which weight changed over time was not related to the extent to which MVPA changed over time. Additionally, on average, weight increased by 2.61 kg (2.02–3.20 kg increase; p < 0.001) at follow-up, irrespective of MVPA at any time point. Findings were similar when stratified by obesity status at baseline (Supplementary Tables 6 and 7).
Associations between weight and covariate contributors to the models
Further, being male, obese, from the US, and time were all associated with weight change, adjusting for covariates (Table 3, Model 1a). On average, in participants categorised as being obese, weight was 18.17 kg (16.57–19.76 kg) more relative to those with non-obese BMIs (p < 0.001). Weight was 3.66 kg (1.78–5.55 kg) less on average in females than males (p < 0.001). On average, participants from all sites outside of the US weighed less at any time point in the study (p < 0.001) compared to the US cohort. For example, Ghanaians weighed 20.66 kg (16.96–24.36 kg) less on average than those from the US, while participants from the Seychelles weighed 12.92 kg (9.25–16.59 kg) less on average.
Associations between sedentary behaviour and weight change
The GEE models evaluating the association between sedentary behaviour at both timepoints, and weight change are presented in Supplementary Table 5. The interaction term between time and sedentary behaviour was, similarly, not statistically significant (p = 0.125), suggesting that the extent to which weight changed over time was not related to the extent to which sedentary behaviour changed over time (Model 2a). Sedentary behaviour at a particular time was not significantly associated with weight at that same time (p = 0.431) on average (Model 2b). Additionally, on average, weight increased by 2.77 kg (2.11–3.44 kg increase; p < 0.001) at follow-up, irrespective of sedentary behaviour at any time point.
Discussion
The current study sought to determine the associations between objectively measured PA and prospective weight change in five diverse African-origin populations. The main finding is that while MVPA at baseline and follow-up was associated with lower body weight, overall MVPA (both at baseline and change from baseline to follow-up) did not impact longitudinal weight changes. Instead, only time, gender, adiposity status and being from the US, were significantly associated with prospective weight change. Similar findings were found when using sedentary behaviour as the main exposure (Supplementary Table 5).
This adds to a growing body of literature exploring the relationship between PA and prospective weight change15,16,17,18,19,20,21,22,23,24,41,42. Some studies, mainly interventions and clinical trials, which similarly used objectively measured PA, have found a positive association between PA and weight change. However, these findings are generally modest, with limited translatability to real-life settings since PA was generally assessed under strict intervention conditions and for relatively short periods of time22,23,24. On the other hand, other longitudinal studies, using subjective self-report to estimate PA, have shown that PA is associated with prospective weight change, such that higher levels of self-reported PA are associated with less weight gained20,21,43. In contrast, our findings are corroborated in a number of other studies also utilising objectively measured PA15,16, including a longitudinal study by Ekeland et al.44, who similarly did not find an association between change in MVPA over time and body weight over time but did find a reverse association when using MVPA as the outcome measure. While the analyses in this current study adjusted for obesity, future studies should additionally explore the potential reverse impact of body weight (and/or obesity) on MVPA over time, across diverse populations44. This would help to clarify lingering questions in the PA-weight change debate. Nevertheless, in addition to MVPA at baseline, this study confirms in a cohort of African-origin populations, that change in MVPA over time is not significantly associated with prospective weight change, either.
The second finding is that overall, irrespective of research site, objectively measured MVPA levels were exceptionally low. In fact, because they were so low, it was necessary to use the 1-min bout data as opposed to the 10-min bout data, because so few people within each site met the 10-min bout threshold. The new WHO 2020 guidelines state that MVPA bouts of any duration now count towards total MVPA volume, irrespective of bout length8. This is different from the 2010 guidelines which indicated that MVPA needed to be accumulated in 10-min bouts6. This raises questions regarding the impact of these shorter bouts of MVPA on prospective weight change over time. However, since the outcome was weight, it is not possible to draw conclusions about the other measures of cardiorespiratory fitness or cardiovascular health. A study by Ma et al.45 supports this approach, as they confirm that low levels of MVPA are common, and that shorter bouts can contribute to overall PA levels. Although cardiorespiratory fitness is without a doubt a predictor of overall morbidity and mortality46,47, the Ma et al. study highlights that while shorter bouts may improve some health markers, longer, more structured MVPA sessions are more beneficial for cardiorespiratory fitness and reducing mortality45.
Consequently, these results do not suggest that PA is not vital for other health benefits, including cardiovascular health. Even in the current study, weight, was on average lower in those participants who did more MVPA compared to those who did less, or even no MVPA. Non-communicable diseases (NCDs), including Type II diabetes (T2D), heart disease, hypertension, stroke, and breast and colon cancer are increasing globally48, and research suggests that limited PA and physical inactivity is a contributing factor19. Regular PA which has been shown to prevent and improve management of NCDs and cardiovascular diseases such as those mentioned above5,6,11,12,13,14, also plays a role in in improving mental health, quality of life, and well-being5,6. Conversely, physical inactivity is linked with the onset of NCDs which, in turn, can result in health problems and all-cause mortality, but it is very importantly also a modifiable primary health risk factor for NCDs in all age groups6,49. Nevertheless, our findings, which contribute to the ongoing debate surrounding PA and prospective weight change, suggest that objectively measured PA is not a good indicator of longitudinal weight change at a population level. The impact of participants’ intention to lose weight and the impact of deliberate MVPA, with the goal of weight loss, remains a topic to be explored in future studies.
The importance of evidence-based public health campaigns is highlighted by our study’s findings, which clearly show the rising levels of obesity across the epidemiologic transition. In low and low-to middle-income countries, there has been a movement of inhabitants to urban centers which has provided access to a mechanized lifestyle and cheaper, often more highly processed energy sources, encouraging the rapid increase in the obesity crisis15. The greatest increases in obesity were shown in the countries at the lower HDI end, specifically among the Ghanaian, South African and Jamaican men, where the obesity prevalence doubled over time. The prevalence of obesity in the women is alarmingly high when compared to the men, with at least a third of all women from each site classifying as obese. Similar results were found in the US National Health and Nutrition Examination Survey (NHANES) 2005–2014, which found a higher prevalence of obesity among women compared to men50. Having confirmed this pattern in African-origin populations across the epidemiologic transition, global public health efforts are needed to specifically address this risk, across the life course, in women.
Several strengths of the study include the use of longitudinal objectively measured PA, and under-studied population. To minimize measurement errors, the same brand/model of calibrated equipment items were used at all research sites. However, the study also had limitations. While the local communities were representative of their respective local communities, participants may not be representative of the countries in which they live. Because of this, results must be interpreted with caution when considering them across the human development spectrum. Secondly, due to the nature of the study, measurements were completed during different seasons at the different study sites16, which may have impacted the PA results. Thirdly, sensitivity analysis showed that age was statistically different between groups with and without valid follow-up data, but age was not found to be significantly associated with prospective weight change in the GEE models and therefore we don’t expect that this would have a large impact on the results. Fourthly, the current analysis did not include total or light PA data, which may be useful as per the updated WHO PA recommendations8. Fifth the study only analysed daytime PA data between 07:00 and 23:00, assuming this to line up with participants’ wake time. Since it is possible that this period includes some sleep time, we acknowledge that the PA data may include more sedentary behaviour than intended. Lastly, the analysis did not include nutrition data, which is expected to vary widely between sites and is highly relevant when exploring prospective weight change.
Conclusion
The results of this study indicate that objectively measured MVPA is not associated with prospective weight change over time in 5 African-origin cohorts. Instead, sex, obesity status, and site (a surrogate for stage of the epidemiologic transition) were associated with prospective weight change. While there is much evidence to support the health benefits from engaging in higher levels of MVPA, including lower cardiovascular disease like hypertension, the direct weight loss effects are likely more nuanced. Thus, studies should focus on understanding the drivers of longitudinal weight gain and obesity at the population level, including the obesogenic food environment and social determinants of health.
Data availability
Data are available upon reasonable request from the corresponding author.
References
WHO. W.H.O. World Obesity Day 2022 – Accelerating action to stop obesity. (2022).
Chong, B. et al. Trends and predictions of malnutrition and obesity in 204 countries and territories: an analysis of the global burden of Disease Study 2019. EClinicalMedicine 57, 101850 (2023).
Federation, W. O. World Obesity Atlas 2024. 2024: London.
Zult, T. et al. Levels of self-reported and objective physical activity in individuals with age-related macular degeneration. BMC Public. Health. 20 (1), 1144 (2020).
WHO, W.H.O. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World (Geneva, 2018).
WHO, W.H.O. Global Recommendations on Physical Activity for Health (Geneva, 2010).
Bull, F. C. et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 54 (24), 1451–1462 (2020).
WHO, W.H.O. WHO Guidelines on Physical Activity and Sedentary Behaviour (Geneva, 2020).
Guthold, R. et al. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob Health. 6 (10), e1077–e1086 (2018).
Luke, A. et al. Protocol for the modeling the epidemiologic transition study: a longitudinal observational study of energy balance and change in body weight, diabetes and cardiovascular disease risk. BMC Public. Health. 11, 927 (2011).
Jayasinghe, S. et al. The current global state of movement and physical activity - the health and economic costs of the inactive phenotype. Prog Cardiovasc. Dis. 64, 9–16 (2021).
Lee, I. M. et al. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet 380 (9838), 219–229 (2012).
Katzmarzyk, P. T. et al. Physical inactivity and non-communicable disease burden in low-income, middle-income and high-income countries. Br. J. Sports Med. 56 (2), 101–106 (2022).
Beale, A. L. & Demaio, A. R. Non-communicable disease risk factors: a call for primary care clinicians to act and to refer. Brief intervention, not silent abdication. Br. J. Sports Med. 53 (6), 322–323 (2019).
Luke, A. et al. Energy expenditure does not predict weight change in either Nigerian or African American women. Am. J. Clin. Nutr. 89 (1), 169–176 (2009).
Dugas, L. R. et al. Accelerometer-measured physical activity is not associated with two-year weight change in african-origin adults from five diverse populations. PeerJ 5, e2902 (2017).
Luke, A. & Cooper, R. S. Physical activity does not influence obesity risk: time to clarify the public health message. Int. J. Epidemiol. 42 (6), 1831–1836 (2013).
Blair, S. N., Archer, E. & Hand, G. A. Commentary: Luke and Cooper are wrong: physical activity has a crucial role in weight management and determinants of obesity. Int. J. Epidemiol. 42 (6), 1836–1838 (2013).
Bekele, B. B. et al. Diabetes mellitus, metabolic syndrome, and physical activity among ethiopians: a systematic review. Diabetes Metab. Syndr. 15 (1), 257–265 (2021).
Byambasukh, O. et al. Physical activity and 4-year changes in body weight in 52,498 non-obese people: the lifelines cohort. Int. J. Behav. Nutr. Phys. Act. 18 (1), 75 (2021).
Hankinson, A. L. et al. Maintaining a high physical activity level over 20 years and weight gain. JAMA 304 (23), 2603–2610 (2010).
Donnelly, J. E. et al. Effects of a 16-month randomized controlled exercise trial on body weight and composition in young, overweight men and women: the Midwest Exercise Trial. Arch. Intern. Med. 163 (11), 1343–1350 (2003).
Donnelly, J. E. et al. Aerobic exercise alone results in clinically significant weight loss for men and women: midwest exercise trial 2. Obes. (Silver Spring). 21 (3), E219–E228 (2013).
Rosenkilde, M. et al. Body fat loss and compensatory mechanisms in response to different doses of aerobic exercise–a randomized controlled trial in overweight sedentary males. Am. J. Physiol. Regul. Integr. Comp. Physiol. 303 (6), R571–R579 (2012).
Curioni, C. C. & Lourenco, P. M. Long-term weight loss after diet and exercise: a systematic review. Int. J. Obes. (Lond). 29 (10), 1168–1174 (2005).
Foster-Schubert, K. E. et al. Effect of diet and exercise, alone or combined, on weight and body composition in overweight-to-obese postmenopausal women. Obes. (Silver Spring). 20 (8), 1628–1638 (2012).
Paul, P. et al. Walking for transportation and leisure among U.S. adults–National Health interview Survey 2010. J. Phys. Act. Health. 12 (0 1), S62–S69 (2015).
Song, M. et al. Physical activities of U.S. High School Students–2010 National Youth Physical Activity and Nutrition Survey. J. Phys. Act. Health. 12 (Suppl 1), S11–S17 (2015).
Sallis, J. F. Measuring physical activity: practical approaches for program evaluation in native American communities. J. Public. Health Manag Pract. 16 (5), 404–410 (2010).
Hills, A. P., Mokhtar, N. & Byrne, N. M. Assessment of physical activity and energy expenditure: an overview of objective measures. Front. Nutr. 1, 5 (2014).
Wareham, N. J. & Brage, S. Commentary: physical activity and obesity; scientific uncertainty and the art of public health messaging. Int. J. Epidemiol. 42 (6), 1843–1845 (2013).
Bergouignan, A. et al. Physical inactivity as the culprit of metabolic inflexibility: evidence from bed-rest studies. J. Appl. Physiol. (1985). 111 (4), 1201–1210 (2011).
Hill, J. O. & Peters, J. C. Commentary: physical activity and weight control. Int. J. Epidemiol. 42 (6), 1840–1842 (2013).
Luke, A. et al. A mixed ecologic-cohort comparison of physical activity & weight among young adults from five populations of African origin. BMC Public. Health. 14, 397 (2014).
Dugas, L. R. et al. Gut microbiota, short chain fatty acids, and obesity across the epidemiologic transition: the METS-Microbiome study protocol. BMC Public. Health. 18 (1), 978 (2018).
Baphumelele Baphumelele - Our Community. [cited 2022 12 September]. (2022).
Dugas, L. R. et al. Comparisons of intensity-duration patterns of physical activity in the US, Jamaica and 3 African countries. BMC Public. Health. 14, 882 (2014).
Colley, R. C. & Tremblay, M. S. Moderate and vigorous physical activity intensity cut-points for the Actical accelerometer. J. Sports Sci. 29 (8), 783–789 (2011).
Wong, S. L. et al. Actical accelerometer sedentary activity thresholds for adults. J. Phys. Act. Health. 8 (4), 587–591 (2011).
Troiano, R. P. et al. Physical activity in the United States measured by accelerometer. Med. Sci. Sports Exerc. 40 (1), 181–188 (2008).
Dhurandhar, E. J. et al. Predicting adult weight change in the real world: a systematic review and meta-analysis accounting for compensatory changes in energy intake or expenditure. Int. J. Obes. (Lond). 39 (8), 1181–1187 (2015).
Jansen, S. C. P. et al. A systematic review and meta-analysis of the effects of supervised exercise therapy on modifiable cardiovascular risk factors in intermittent claudication. J. Vasc Surg. 69 (4), 1293–1308 (2019). e2.
Moholdt, T. et al. Current physical activity guidelines for health are insufficient to mitigate long-term weight gain: more data in the fitness versus fatness debate (the HUNT study, Norway). Br. J. Sports Med. 48 (20), 1489–1496 (2014).
Ekelund, U. et al. Objectively measured sedentary time and physical activity and associations with body weight gain: does body weight determine a decline in moderate and vigorous intensity physical activity? Int. J. Obes. (Lond). 41 (12), 1769–1774 (2017).
Ma, T. et al. Revisiting the concept of bout: associations of moderate-to-vigorous physical activity sessions and non-sessions with mortality. Int. J. Behav. Nutr. Phys. Act. 21 (1), 81 (2024).
Al-Mallah, M. H., Sakr, S. & Al-Qunaibet, A. Cardiorespiratory Fitness and Cardiovascular Disease Prevention: an update. Curr. Atheroscler Rep. 20 (1), 1 (2018).
Ehrman, J. K. et al. Cardiorespiratory Fitness Change and Mortality Risk among Black and White patients: Henry Ford Exercise Testing (FIT) project. Am. J. Med. 130 (10), 1177–1183 (2017).
Ndupu, L. B. et al. Application of theoretical domains framework to explore the enablers and barriers to physical activity among university staff and students: a qualitative study. BMC Public. Health. 23, 670 (2022).
Silva, D. A. S. et al. Physical inactivity as a risk factor for all-cause mortality in Brazil (1990–2017). Popul. Health Metr. 18 (Suppl 1), 13 (2020).
Muscogiuri, G. et al. Obesity: a gender-view. J. Endocrinol. Invest. 47 (2), 299–306 (2024).
Acknowledgements
The authors would like to acknowledge all participants who were involved in the study.
Funding
METS is funded in part by the National Institutes of Health (1R01DK80763, R01DK111848 and R01HL148271).
Author information
Authors and Affiliations
Contributions
LRD, AL, TEF, EVL, JPR, KBA and PB all conceived the idea and contributed equally to the manuscript. CC, KA, PO, OD, NS, MW and BV all collected the data and contributed to the analysis. Additionally, JCD, CA, LS, AM, HG, CC, CJ and GEM all performed the analysis, tables and figures. All authors (JCD, CC, LS, HG, CA, AM, PB, BV, KBA, JPR, POB, KA, OAD, TEF, MW, EVL, DR, NS, BL, JG, GEM, CJ, AL and LRD) contributed to the interpretation of the data and writing of the manuscript.
Corresponding author
Ethics declarations
Consent for publication
All participants consented to their information being used for publication.
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
The protocols for METS and METS-Microbiome were approved by the Institutional Review Board of Loyola University Chicago, IL, US; the Committee on Human Research Publication and Ethics of Kwame Nkrumah University of Science and Technology, Kumasi, Ghana; the Human Research Ethics Committee of the University of Cape Town, South Africa; the Board for Ethics and Clinical Research of the University of Lausanne, Switzerland; and the Ethics Committee of the University of the West Indies, Kingston, Jamaica. All participants provided written informed consent10,34,35. The protocol for the current analysis was also approved by the University of Cape Town’s Human Research Ethics Committee (HREC ref: 632/2022).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Davies, J.C., Choo-Kang, C., Soepnel, L. et al. Objectively measured moderate-to-vigorous physical activity does not attenuate prospective weight gain among african-origin adults spanning the epidemiological transition. Sci Rep 15, 6765 (2025). https://doi.org/10.1038/s41598-025-85383-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-85383-7
