
Abstract
This study aims to explore the relationship between the albumin-corrected anion gap (ACAG) and short- and long-term all-cause mortality (ACM) in patients with acute pancreatitis (AP) managed in the intensive care unit (ICU). We conducted a retrospective analysis utilizing data extracted from the Medical Information Mart for Intensive Care-IV (MIMIC-IV) database. This study sought to investigate the correlation between ACAG and ACM among patients diagnosed with AP across various disease stages. R statistical software was used to identify the optimal thresholds for ACAG. Kaplan-Meier survival curves and multivariate Cox proportional hazards regression models were employed to assess the association between ACAG and short- and long-term ACM of AP. The predictive ability, sensitivity, specificity, and area under the curve (AUC) of ACAG for short- and long-term ACM in AP were investigated using receiver operating characteristic analysis. Subgroup analyses were also conducted. A cohort comprising 605 participants was included in this study. The ideal threshold for ACAG identified by R statistical software was 21.5. Cox proportional hazards modeling revealed that there was an independent association between patients with AP with ACAG ≥ 21.5 and ACM at 3, 7, 10, 14, 28, 90, and 180 days and 1 year before and after adjustment for confounders. Survival curves demonstrated that patients with ACAG ≥ 21.5 had lower survival rates at 3, 7, 10, 14, 28, 90, and 180 days and 1 year. In addition, ACAG showed superior performance, with a larger AUC than the anion gap, albumin, and Systemic Inflammatory Response Syndrome score and Sequential Organ Failure Assessment at 3, 7, 10, 14, 28, 90, and 180 days and 1 year. Subgroup analysis revealed no significant interaction between ACAG and any subgroups Elevated levels of ACAG were found to be associated with increased short- and long-term ACM in patients with AP, and ACAG may be an independent predictor of ACM at different disease stages.
Similar content being viewed by others

1 Introduction
Acute pancreatitis (AP) is one of the most common diseases of the gastrointestinal system, impacting an estimated 2.8 million individuals globally annually, and its incidence continues to increase1. AP prognosis usually depends on disease severity. The majority of patients have mild symptoms and recover with fasting, intravenous fluids, and supportive therapy; however, the disease continues to progress in approximately 20–30% of patients, resulting in pancreatic necrosis, peripancreatic tissue necrosis, and multi-organ failure, accompanied by a mortality rate ranging from 20 to 40%2,3. Therefore, timely and accurate disease assessment is anticipated to enhance the prognosis of patients afflicted with AP.
Several methods are available to assess AP severity, such as the Sequential Organ Failure Assessment (SOFA) score, Systemic Inflammatory Response Syndrome (SIRS) score, Acute Physiology and Chronic Health Evaluation II score, and Ransom Criteria4,5. However, these methods are usually complex and require the collection of several clinical and laboratory indicators, possibly delaying the time of treatment and missing the optimal therapeutic window. Hence, there exists a pressing necessity to investigate novel, straightforward, highly sensitive, and cost-effective indicators for evaluating the progression of AP.
Acid-base disorders are common among inpatients in intensive care unit (ICU) and are strongly associated with mortality from various diseases6. Among these, the anion gap (AG), which reflects the difference between unmeasured serum anion and cation concentrations, is one of the most commonly used biomarkers for diagnosing acid-base imbalance and identifying metabolic acidosis. AG is composed primarily of albumin (ALB), lactate, sulfate, phosphate, and other ions; however, because of the net negative charge carried by ALB, an increase or decrease in its concentration can have a significant effect on AG levels7. Therefore, an increasing number of researchers have suggested that the albumin-corrected anion gap (ACAG) is better suited for evaluating acid-base disorders and determining disease prognosis8. Prior investigations have indicated a robust association between elevated ACAG levels and adverse outcomes in individuals with acute myocardial infarction9, acute kidney injury (AKI)10, and asthma11.
To our knowledge, there have been no prior studies documenting an association between ACAG and short- and long-term all-cause mortality (ACM) of AP. Thus, through the acquisition of hospitalization data of AP patients from the Medical Information Mart for Intensive Care IV (MIMIC-IV) database spanning from 2008 to 2019, our objective was to investigate the correlation between ACAG and ACM across various stages of AP. Additionally, we sought to assess the predictive capacity of ACAG in determining AP prognosis.
Materials and methods
Data source
This study was conducted retrospectively at a single center, with all data sourced from the MIMIC-IV database (version 2.2; https://mimic.mit.edu). The MIMIC-IV database, a substantial resource, is publicly accessible and overseen by the MIT Computational Physiology Laboratory. This database contains a vast amount of data relevant to the field of intensive care medicine and is an essential resource for the study of critical care outcomes, predictive modeling, clinical decision support, and other areas of research. The database includes all intensive care patients admitted to the Beth Israel Deaconess Medical Center between 2008 and 2019 and contains a detailed record of each patient’s basic information, laboratory results, treatment regimen, length of stay, physiological parameters, and other comprehensive data. The authors engaged in this study have successfully completed the Collaborative Institutional Training Initiative course, passed examinations on “Conflict of Interest” and “Data or Specimen Research Only,” and were granted permission to access the database.
Ethical considerations and data privacy
In order to safeguard patient confidentiality, all personal data underwent de-identification, with random numerical identifiers assigned in place of individual identification. Consequently, the Beth Israel Deaconess Medical Center ethics committee exempted the necessity for informed consent.
Study population
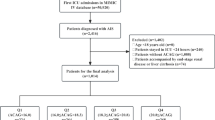
The MIMIC-IV (v2.2) database contains data on 180,733 patients admitted to the ICU during the period from 2008 to 2019. The medical records of patients with AP were extracted using codes 577.0 and K85-K85.92 from the International Classification of Diseases, Revision 9 (ICD-9) and ICD-10, respectively. Among the entries in this database, 5,894 patients diagnosed with AP were identified, with 1,271 of them requiring admission to the ICU. This study exclusively enrolled patients aged over 18 years. Additional exclusion criteria encompassed patients with recurrent admissions for AP, those with ICU stays of less than 24 h, individuals with end-stage renal disease, cirrhosis, or malignancy, and patients for whom data on AG and ALB levels were not documented within 24 h of admission. Finally, a total of 605 patients were included in the study (Fig. 1).

Flowchart for participants from the MIMIC-IV (v 2.2). “Lower ACAG” refers to values below 21.5 and “Higher ACAG” refers to values greater than or equal to 21.5. MIMIC-IV, Medical Information Marketplace Intensive Care-IV; AP, acute pancreatitis; ICU, intensive care unit; ACAG, albumin-corrected anion gap.
Data extraction and management of abnormal and missing values
ACAG was selected as the main variable in this study. ACAG was obtained by calculating AG and ALB from the first measurement taken within 24 h of admission to minimize interference with subsequent treatment. According to the relevant literature12, ACAG was calculated as follows: ACAG = AG + 2.5 X [4.4-ALB (g/dL)]. Data extraction was conducted using Structured Query Language (SQL) with the assistance of PostgreSQL (version 13.7.1) and Navicat Premium (version 15) software tools. PostgreSQL is an open-source, object-relational database management system widely used for handling complex queries and managing large datasets. In our study, PostgreSQL was utilized for data storage, retrieval, and the execution of structured query language (SQL) commands to facilitate data management and analysis. Navicat Premium is a database management tool that allows for easy connection to multiple databases. We used Navicat Premium to streamline our database management process, including creating, organizing, and managing tables within PostgreSQL, which enhanced our efficiency in data processing and organization. The primary data extracted included demographic variables, vital signs, clinical treatments, comorbidities, laboratory variables, and clinical outcomes. The list of extracted variables is summarized in Table 1. Using the STATA winsor2 command, outlier variables were processed with the winsorize method at 1% and 99% cutoffs. To solve the problem of missing values, the researchers used multiple estimation methods. Variables with more than 15% missing values were excluded, such as C-reactive protein and calcitoninogen (a precursor to calcitonin, which may serve as a biomarker in inflammatory conditions but has limited established relevance in AP, and its levels may be elevated when AP is combined with bacterial infection).
Statistical analysis
Continuous variables are reported as the median and interquartile range, and differences were analyzed using t-tests or Mann-Whitney U-tests. Categorical variables are reported as counts and proportions and compared using a chi-square test or Fisher’s exact test. In this study, we used R statistical software (R version 4.2.2, R Statistical Computing Foundation) to determine the optimal threshold for ACAG. The optimal threshold for selecting the maximum risk ratio is shown in Fig. 2. By applying a predetermined optimal threshold value, the ACAG group was divided into two subgroups: higher and lower ACAG groups. Univariate and multivariate analyses of prognostic factors were conducted utilizing Cox proportional hazards models to ascertain independent predictors of mortality among patients with AP at various intervals post-hospital admission, including 3, 7, 10, 14, 28, 90, and 180 days, as well as 1 year. The findings are presented as hazard ratios (HRs) with corresponding 95% confidence intervals (CIs). Survival curves were constructed using the Kaplan-Meier (K-M) method without adjustment, and the comparison between the two sets of curves was conducted utilizing the log-rank test. The predictive ability of AG, ALB, and SIRS and SOFA scores for mortality at 3, 7, 10, 14, 28, 90, and 180 days and 1 year after admission as well as the sensitivity and specificity of each metric were assessed using receiver operating characteristic (ROC) analysis, and the area under the curve (AUC) was calculated. Finally, we examined the robustness of ACAG in different subgroups, including age, sex, hypertension, sepsis, respiratory failure (RF), and diabetes. All statistical analyses were performed using a two-sided approach, with significance set at P < 0.05. R Statistical Software (R version 4.2.2, R Foundation for Statistical Computing), SPSS Statistics 26 (IBM, Chicago, IL, USA), and GraphPad Prism 8 (GraphPad Software, San Diego, CA, USA) were employed for data analysis.

The choice of the optimal cutoff maximized the risk ratio and the relationship between ACAG ≥ 21.5 and the distribution of ACAG.
Results
Baseline demographic and clinical characteristics
In the end, the study comprised 605 patients diagnosed with AP who received treatment in the ICU (Fig. 1). Among them, 350 were males and 255 were females. Laboratory results revealed that individuals in the elevated ACAG category exhibited markedly elevated levels of AG, AST, Crea, BUN, K, and LAC (all P < 0.001). Furthermore, patients classified in the higher ACAG group were at an increased likelihood of experiencing an unfavorable prognosis. Our study found that these patients had higher ACM rates at different stages of AP, including 3-day (0.6% vs. 10.1%, P < 0.001), 7-day (1.3% vs. 14.7%, P < 0.001), 10-day (2.1% vs. 22.5%, P < 0.001), 14-day (3.2% vs. 27.1%, P < 0.001), 28-day (5.5% vs. 38.0%, P < 0.001), 90-day (12.4% vs. 43.4%, P < 0.001), and 180-day (14.5% vs. 45.7%, P < 0.001), and 1-year mortality (16.8% vs. 49.6%, P < 0.001). In addition, patients in the higher ACAG group had longer ICU stays [3.5 (1.9, 8.1) vs. 6.2 (2.4, 14.0), P < 0.001]. The comprehensive results are outlined in Table 2.
Univariate and multivariate Cox regression models of ACAG and ACM in AP patients
Univariate and multivariate Cox regression analyses were performed to investigate the potential association between ACAG levels and ACM in patients diagnosed with AP. In the unadjusted model, elevated ACAG levels were significantly associated with increased risk of short- and long-term ACM in AP: 3- (HR = 16.75, 95% CI: 4.77–58.78, P < 0.001), 7- (HR = 12.59, 95% CI: 5.03–31.52, P < 0.001), 10- (HR = 11.95, 95% CI: 5.82–24.53, P < 0.001), 14- (HR = 9.95, 95% CI: 5.43–18.22, P < 0.001), 28- (HR = 8.57, 95% CI: 5.32–13.79, P < 0.001), 90- (HR = 4.65, 95% CI: 3.22–6.71, P < 0.001), and 180-day (HR = 4.26, 95% CI: 3.00–6.03, P < 0.001) and 1-year (HR = 4.06, 95% CI: 2.92–5.65, P < 0.001) ACM.
In Model 2, even after adjusting for confounders such as age, sex, and ethnicity, individuals categorized in the elevated ACAG group exhibited an increased risk of death at different stages of the AP: 3- (HR = 18.95, 95% CI: 5.37–66.81, P < 0.001), 7- (HR = 13.75, 95% CI: 5.45–34.64, P < 0.001), 10- (HR = 12.64, 95% CI: 6.12–26.10, P < 0.001), 14- (HR = 10.97, 95% CI: 5.95–20.24, P < 0.001), 28- (HR = 9.65, 95% CI: 5.96–15.64, P < 0.001), 90- (HR = 5.26, 95% CI: 3.62–7.64, P < 0.001), and 180-day (HR = 4.77, 95% CI: 3.35–6.80, P < 0.001) and 1-year (HR = 4.44, 95% CI: 3.17–6.21, P < 0.001) ACM.
In Model 3, which included other more likely confounders, there was still an independent positive correlation between ACAG levels and ACM during the period described above. The detailed findings are delineated in Table 3.
K-M curves analysis
In contrast to patients categorized in the lower ACAG group, those in the higher ACAG group exhibited an elevated short- and long-term ACM. K-M survival curves indicated that patients in the higher ACAG group exhibited a higher 3-day (0.6% vs. 10.1%, P < 0.001), 7-day (1.3% vs. 14.7%, P < 0.001), 10-day (2.1% vs. 22.5%, P < 0.001), 14-day (3.2% vs. 27.1%, P < 0.001), 28-day (5.5% vs. 38.0%, P < 0.001), 90-day (12.4% vs. 43.4%, P < 0.001), and 180-day (14.5% vs. 45.7%, P < 0.001), and 1-year mortality (16.8% vs. 49.6%, P < 0.001) (Fig. 3).

Kaplan-Meier survival analysis curves for 3-day (A), 7-day (B), 10-day (C), 14-day (D), 28-day (E), 90-day (F), 180-day (G), and 1-year (H) all-cause mortality in patients with acute pancreatitis admitted to the intensive care unit.
ROC curve analysis
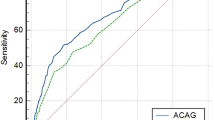
We plotted ROC curves for the five indicators, ACAG, AG, ALB, and SIRS and SOFA, that predicted ACM of AP (Fig. 4). Our study demonstrated that ACAG had higher AUC values at different times after admission compared to AG, ALB, SIRS and SOFA. For example, compared with AG [0.81 (95% CI: 0.66–0.96)], ALB [0.66 (95% CI: 0.52–0.81)], and SIRS [0.63 (95% CI: 0.50–0.76)] and SOFA [0.73 (95% CI: 0.59–0.88)], the AUC values for ACAG on day 3 of admission were significantly higher [0.84 (95% CI: 0.70–0.97)]. Compared with AG [0.70 (95% CI: 0.62–0.74)], ALB [0.61 (95% CI: 0.55–0.68)], and SIRS [0.53 (95% CI: 0.47–0.58)] and SOFA [0.65 (95% CI: 0.59–0.71)], the AUC values for ACAG on day 90 of admission were still significantly higher [0.72 (95% CI: 0.67–0.78)]. These are two examples; additional details can be found in Table 4.

Receiver operating characteristic curves for predicting 3-day, 7-day, 10-day, 14-day, 28-day, 90-day, 180-day, and 1-year all-cause mortality in patients with acute pancreatitis admitted to the intensive care unit.
Subgroup analyses for ACAG on clinical outcomes in patients with AP
Subgroup analyses were performed to evaluate whether ACAG differed significantly among the different subgroups. Figure 5 illustrates the association between ACAG and ACM in AP patients in different subgroups. After stratification according to age, sex, hypertension, diabetes, sepsis, and RF, the forest plots showed no significant interactions between ACAG and any subgroup (P > 0.05 for all interactions).

Forest plots of subgroup analyses of the relationship between 7-day, 14-day, 28-day, 90-day, 180-day, and 1-year all-cause mortality and ACAG in patients with acute pancreatitis admitted to the intensive care unit.
Discussion
In this study, we explored the correlation between ACAG and prognosis at different stages of AP. Our results demonstrated that when ACAG ≥ 21.5, short- and long-term ACM was higher in patients with AP than in those with ACAG < 21.5. Our results also indicated that ACAG was a comparable predictor of short- and long-term ACM in patients with AP, and its predictive ability was superior to that of AG, ALB, SIRS, and SOFA.
Acid-base balance is the cornerstone of life, and severe acid-base and electrolyte disorders can lead to organ damage and metabolic system failure13,14,15,16. AP is the abnormal activation of pancreatic enzymes caused by a variety of etiological factors, resulting in auto-digestion, edema, hemorrhage, and even necrosis of the pancreatic tissue14. It is characterized by rapid onset and progression, and if not treated promptly and effectively, it can lead to pancreatic necrosis, septic shock, gastrointestinal hemorrhage, and multi-organ failure17. Patients with AP hospitalized in the ICU usually have electrolyte and acid-base imbalances17. Activation of the inflammatory response and recruitment of inflammatory cells often result in tissue damage in patients, while ALB promotes the production of anti-inflammatory substances (e.g., lipotoxins, hemolysins, and protective proteins) and promotes tissue healing; therefore, this process requires a large amount of ALB, which is the main reason for the decrease in ALB in patients with AP18. In addition, other factors, such as decreased appetite and fasting due to gastrointestinal symptoms, further reduce ALB levels by limiting nutritional intake17,18. Elevated levels of inflammatory cytokines, common in AP, also play a role in decreasing ALB through increased capillary permeability and subsequent albumin redistribution into the interstitial space18. Therefore, The decrease in ALB in AP patients is a result of multiple factors.
AG is an important biomarker for assessing acid-base balance in the body and has been linked to adverse prognoses in numerous diseases19,20,21. Xu et al. reported a linear correlation between AG and 28-day ICU mortality in patients with diastolic heart failure19. Chen et al. discovered that among patients who experienced cardiac arrest, those with a higher AG were significantly less likely to survive hospitalization20. Jiang et al. similarly found that patients with sepsis-associated AKI faced a heightened risk of mortality within 28 days of ICU admission when AG ≥ 14 mmol/L21. Gong et al. also identified a nonlinear correlation between AG and 90-day ACM in patients with AKI, as 90-day ACM positively correlated with AG when AG > 13.8 mmol/L22. However, AG is primarily composed of ALB, lactate, sulfate, phosphate, and other ions, and ALB has a net negative charge, which undoubtedly contributes to errors in AG assessment7. In addition, it is common for ALB levels to drop dramatically in critically ill patients, and low ALB levels lead to false-negative AG values and affect the interpretation of results23. Kraut et al. calculated that each 1 g/dL change in ALB resulted in a 2.3–2.5-mmol/L change in AG24. As a result, an increasing number of researchers recommend the use of ACAG to assess disease severity in critically ill patients.
Compared to AG, ACAG is more accurate in detecting hidden tissue anions, identifying acidosis in critically ill patients, and partially reflecting the patients’ nutritional status8. In a study investigating the correlation between ACAG and in-hospital mortality among patients with sepsis, Hu et al. assessed the prognostic values of ALB, AG, and ACAG by plotting ROC curves12. Their investigation suggested that ACAG outperformed AG and ALB in predicting in-hospital mortality among this patient cohort. In another study, Wang et al. found that ACAG served as a significant independent predictor of 30-day mortality among patients with asthma undergoing intensive care treatment11. The AUC for ACAG was 0.703, surpassing that for AG (0.642), suggesting that ACAG is a better predictor of 30-day mortality in this population. Jian et al. also noted a significant increase in 30-day ACM in patients with acute myocardial infarction when ACAG ≥ 21.75 mmol/L25. Moreover, our results likewise demonstrated that ACM was significantly increased in AP patients with elevated ACAG levels.
More importantly, our study further illustrated the efficacy of ACAG in predicting the short- and long-term prognosis of patients with AP, which is consistent with the results observed in other diseases26,27. ACAG holds considerable promise as a clinically valuable tool as it mirrors tissue perfusion and offers more precise outcomes compared to directly measured AG values. Compared with traditional scoring criteria, ACAG is an easy-to-use and cost-effective serum biomarker for identifying the severity of AP in a short period of time and for early intervention and treatment of critically ill patients, which will improve the prognosis of patients.
Our study has several advantages. First, employed a robust sample size and utilized data from the MIMIC-IV database, representing a comprehensive, real-world investigation characterized by high-quality data. Second, the primary endpoints of this study were 3-, 7-, 10-, 14-, 28-, 90-, and 180-day, and 1-year ACM in patients with AP, which had significant predictive value at different stages of the disease. Moreover, subgroup analyses were conducted to illustrate the robustness of our findings.
However, our study also has some limitations that should be considered. First, this was a single-center retrospective study, and multicenter studies are necessary to confirm our conclusions in future. Second, the demographic data for our study were obtained from the MIMIC-IV (v2.2), which covers patients hospitalized between 2008 and 2019. However, such a broad time period does not guarantee consistency in the treatment regimens for patients with AP as medical care evolves and treatment protocols advance. Therefore, inconsistencies in treatment regimens may have affected the study results. In addition, owing to the limitations of the MIMIC-IV database itself, we were unable to obtain the specific cause of death for each patient, and therefore could not determine the relationship between ACAG and AP-specific mortality. And, this finding needs to be confirmed by future studies. Finally, this study excluded patients younger than 18 years; therefore, further research is needed to determine whether the results are applicable to this group of patients.
Conclusions
Our study revealed an association between elevated ACAG levels and increased short- and long-term ACM in patients with AP. Moreover, ACAG can be used as an independent predictor of short- and long-term ACM in patients with AP, and its prognostic effect is superior to that of the AG, ALB, SIRS, and SOFA alone.
Data availability
The raw data supporting the conclusions of this paper will be made available by the authors without reservation and can be obtained from the corresponding author.
Abbreviations
- ACAG:
-
albumin-corrected anion gap
- ALB:
-
albumin
- AKI:
-
acute kidney injury
- AP:
-
acute pancreatitis
- AUC:
-
area under the curve
- CI:
-
confidence interval
- HR:
-
hazard ratio
- ICD:
-
International Classification of Diseases
- ICU:
-
intensive care unit
- K-M:
-
Kaplan-Meier
- MIMIC-IV:
-
Medical Information Marketplace Intensive Care-IV
- ACM:
-
all-cause mortality
- RF:
-
respiratory failure
- ROC:
-
receiver operative characteristic
- SIRS:
-
Systemic Inflammatory Response Syndrome
- SOFA:
-
Sequential Organ Failure Assessment
References
Li, C. L., Jiang, M., Pan, C. Q., Li, J. & Xu, L. G. The global, regional, and national burden of acute pancreatitis in 204 countries and territories, 1990–2019. BMC Gastroenterol. 21 (1), 332 (2021).
Schepers, N. J. et al. Impact of characteristics of organ failure and infected necrosis on mortality in necrotising pancreatitis. Gut 68 (6), 1044–1051 (2019).
Bang, J. Y., Wilcox, C. M., Arnoletti, J. P. & Varadarajulu, S. Superiority of endoscopic interventions over minimally invasive surgery for infected necrotizing pancreatitis: meta-analysis of randomized trials. Dig. Endosc. 32 (3), 298–308 (2020).
Janssen, E. M. et al. F. P. Analysis of Patient preferences in Lung Cancer - estimating acceptable tradeoffs between Treatment Benefit and Side effects. Patient Prefer Adherence. 14, 927–937 (2020).
Arif, A., Jaleel, F. & Rashid, K. Accuracy of BISAP score in prediction of severe acute pancreatitis. Pak J. Med. Sci. 35 (4), 1008–1012 (2019).
Chowdhury, R., Turcotte, A. E., Rondon-Berrios, H. & Workeneh, B. T. Spurious Electrolyte and Acid-Base disorders in the patient with Cancer: a review. Am. J. Kidney Dis. 82 (2), 237–242 (2023).
Pratumvinit, B. et al. Anion gap reference intervals show instrument dependence and weak correlation with albumin levels. Clin. Chim. Acta. 500, 172–179 (2020).
Hatherill, M., Waggie, Z., Purves, L., Reynolds, L. & Argent, A. Correction of the anion gap for albumin in order to detect occult tissue anions in shock. Arch. Dis. Child. 87 (6), 526–529 (2002).
Sheng, H. et al. The correlation between albumin-corrected anion gap and prognosis in patients with acute myocardial infarction. ESC Heart Fail. 11 (2), 826–836 (2024).
Gao, P., Min, J., Zhong, L. & Shao, M. Association between albumin corrected anion gap and all-cause mortality in critically ill patients with acute kidney injury: a retrospective study based on MIMIC-IV database. Ren. Fail. 45 (2), 2282708 (2023).
Wang, S., Teng, H., Han, H. & Xu, Y. The relationship between albumin corrected anion gap levels and mortality in patients with asthma in the ICU. Sci. Rep. 13 (1), 16903 (2023).
Hu, T., Zhang, Z. & Jiang, Y. Albumin corrected anion gap for predicting in-hospital mortality among intensive care patients with sepsis: a retrospective propensity score matching analysis. Clin. Chim. Acta. 521, 272–277 (2021).
Wang, J. et al. Evaluating the efficacy and timing of blood purification modalities in early-stage hyperlipidemic acute pancreatitis treatment. Lipids Health Dis. 22 (1), 208 (2023).
Gardner, T. B. Acute Pancreatitis. Ann. Intern. Med. 174 (2), ITC17–ITC32 (2021).
Boxhoorn, L. et al. Acute pancreatitis. Lancet 396 (10252), 726–734 (2020).
Scheiner, B. et al. Acid-base disorders in liver disease. J. Hepatol. 67 (5), 1062–1073 (2017).
de-Madaria, E. et al. Aggressive or moderate fluid resuscitation in Acute Pancreatitis. N Engl. J. Med. 387 (11), 989–1000 (2022).
Lu, Y., Guo, H., Chen, X. & Zhang, Q. Association between lactate/albumin ratio and all-cause mortality in patients with acute respiratory failure: A retrospective analysis.PloS One 16(8), e0255744 (2021).
Xu, H. et al. Serum anion gap is associated with mortality in intensive care unit patients with diastolic heart failure. Sci. Rep. 13 (1), 16670 (2023).
Chen, J. et al. The association between anion gap and in-hospital mortality of post-cardiac arrest patients: a retrospective study. Sci. Rep. 12 (1), 7405 (2022).
Jiang, L. et al. Predictive value of the serum anion gap for 28-day in-hospital all-cause mortality in sepsis patients with acute kidney injury: a retrospective analysis of the MIMIC-IV database. Ann. Transl Med. 10 (24), 1373 (2022).
Gong, F., Zhou, Q., Gui, C., Huang, S. & Qin, Z. The Relationship between the serum anion gap and all-cause mortality in Acute Pancreatitis: an analysis of the MIMIC-III database. Int. J. Gen. Med. 14, 531–538 (2021).
Nicholson, J. P., Wolmarans, M. R. & Park, G. R.The role of albumin in critical illness. Br. J. Anaesth. 85 (4), 599–610 (2000).
Kraut, J. A. & Madias, N. E. Serum anion gap: its uses and limitations in clinical medicine. Clin. J. Am. Soc. Nephrol. 2 (1), 162–174 (2007).
Jian, L. et al. Association between albumin corrected anion gap and 30-day all-cause mortality of critically ill patients with acute myocardial infarction: a retrospective analysis based on the MIMIC-IV database. BMC Cardiovasc. Disord. 23 (1), 211 (2023).
Gündoğan Uzunay, B., Köker, A., Ülgen Tekerek, N., Dönmez, L. & Dursun, O. Role of albumin-corrected Anion Gap and Lactate Clearance in Predicting Mortality in Pediatric Intensive Care patients. Balkan Med. J. 40 (6), 430–434 (2023).
Wang, R. et al. Preoperative albumin corrected anion gap is associated with in-hospital and long-term mortality in patients undergoing coronary artery bypass grafting in a retrospective cohort study. J. Thorac. Dis. 14 (12), 4894–4903 (2022).
Acknowledgements
We are grateful to the MIMIV-IV participants and staff. We appreciate all the reviewers who participated in the review.
Funding
This study was supported by National Natural Science Foundation of China (NSFC) (Grant no.82400758), NHC Key Laboratory of Nuclear Technology Medical Transformation (Mianyang Central Hospital) (Grant no.2023HYX032), the Incubation Project of Mianyang Central Hospital (Grant no.2022FH010), and the Health Commission of Sichuan Province Medical Science and Technology Program (Grant no.24QNMP028).
Author information
Authors and Affiliations
Contributions
(I) Conception and design: Jianjun Wang, Pei Yang, Xintao Zeng, Xi Chen, Sirui Chen, Jianping Gong; (II) Administrative support: Huiwen Luo, Ruizi Shi, Hua Luo, Decai Wang; (III) Provision of study material or patients: All authors; (IV) Collection and assembly of data: All authors; (V) Data analysis and interpretation: Jianjun Wang, Pei Yang, Chuan Qin, Lan Deng, Hua Luo, Decai Wang; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. (Jianjun Wang, Pei Yang and Xintao Zeng contributed equally to this work and share first authorship. Jianping Gong, Hua Luo and Decai Wang contributed equally to this work and share corresponding authorship.)
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethic Statement
In order to safeguard patient confidentiality, all personal data underwent de-identification, with random numerical identifiers assigned in place of individual identification. Consequently, the Beth Israel Deaconess Medical Center ethics committee exempted the necessity for informed consent.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, J., Yang, P., Zeng, X. et al. Prognostic significance of albumin corrected anion gap in patients with acute pancreatitis: a novel perspective. Sci Rep 15, 1318 (2025). https://doi.org/10.1038/s41598-025-85773-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-85773-x
