
Abstract
This study evaluates the cost-effectiveness of adding durvalumab to chemotherapy, with subsequent maintenance either with olaparib (DOCT) or without olaparib (DCT), versus chemotherapy alone (CT) as a first-line treatment for advanced endometrial cancer (EC) in the United States, stratified by mismatch repair deficiency (dMMR) and proficiency (pMMR). A Markov model based on DUO-E Phase III trial data simulated disease progression and outcomes. Total costs, quality-adjusted life years (QALYs), and incremental cost-effectiveness ratios (ICER) were evaluated. Sensitivity analysis assessed model robustness. For dMMR EC, costs (QALYs) were $1,204,763.33 (5.49), $590,732.13 (4.61), and $1,495,528.15 (3.68) for DOCT, DCT, and CT, respectively, with ICER of $584,140.94/QALYs (DOCT vs. CT) and $476,946.43/QALYs (DCT vs. CT). For pMMR EC, costs (QALYs) were $421,126.70 (3.00), $400,470.92 (2.45), and $133,424.52 (1.69), with ICER of $219,601.20/QALYs (DOCT vs. CT) and $351,777.86/QALYs (DCT vs. CT). In the overall population, costs (QALYs) were $607,921.80 (3.89), $417,637.19 (2.82), and $141,594.38 (2.16), with ICER of $269,195.01/QALYs (DOCT vs. CT) and $416,098.68/QALYs (DCT vs. CT). From a U.S. payer perspective, DOCT and DCT regimens are not cost-effective compared to CT for advanced or recurrent EC, including dMMR and pMMR subgroups, at a $150,000/QALY threshold.
Similar content being viewed by others

Introduction
In the United States, endometrial cancer (EC) ranks among the most prevalent gynecological malignancies, with projections estimating 67,800 new cases and 13,250 deaths for the year 2024 1,2. Of these, 10–15% are diagnosed at an advanced stage, while an additional 15–20% of patients initially diagnosed at an early stage will experience recurrence3. Patients with advanced or recurrent EC have a poor prognosis, with a five-year survival rate of only 15–17%. Although the chemotherapy regimen of carboplatin and paclitaxel has long been the standard of care, it only yields suboptimal outcomes, highlighting the critical need for exploring innovative therapeutic strategies4.
Responding to this urgent need for better outcomes, the advent of immunotherapy and molecular targeted therapies has introduced promising new treatment options for advanced EC An increasing number of clinical trials are underway, continually exploring new opportunities to treat advanced EC5,6. durvalumab is a selective, high-affinity human IgG1 monoclonal antibody that blocks the interaction of PD-L1 with PD-1 and CD80, thereby enhancing T-cell function and antitumor immune responses7. Moreover, maintenance therapy, especially with agents like olaparib—a potent poly (ADP-ribose) polymerase (PARP) inhibitor—has garnered significant attention. It not only extends progression-free survival but also sustains therapeutic responses, a crucial benefit for patients battling recurrent or advanced stages of EC8.
The Phase III DUO-E trial (NCT04269200) recently assessed the efficacy and safety of durvalumab combined with chemotherapy, and its subsequent maintenance with olaparib (DOCT) or without olaparib (DCT), for treating advanced EC9. Relative to the standard chemotherapy control group (CT), the study revealed that the risk of disease progression or death was reduced by 45% in the DOCT group (HR 0.55; 95% CI 0.43–0.69; p < 0.0001) and by 29% in the DCT group (HR 0.71; 95% CI 0.57–0.89; p = 0.003). Both groups also showed significant improvements in progression-free survival (PFS) and overall survival (OS).
Notably, the observed improvements were primarily driven by outcomes in the deficient mismatch repair (dMMR) subgroup. In these patients, the DOCT and DCT treatments reduced the risk of disease progression or death by 59% (HR 0.41; 95% CI 0.21–0.75) and 58% (HR 0.42; 95% CI 0.22–0.80), respectively, when compared to CT9. In recognition of these compelling outcomes, the FDA approved durvalumab in combination with chemotherapy on June 14, 2024, as a new standard for treating patients with dMMR primary advanced or recurrent endometrial cancer10.
Despite the promising clinical outcomes, the high costs of durvalumab and the variable responses across patient demographics pose challenges in determining its cost-effectiveness for diverse populations. Accordingly, this study aims to rigorously evaluate the cost-effectiveness of durvalumab combined with chemotherapy and subsequent maintenance therapy (with or without olaparib), compared to standard chemotherapy alone. This analysis is conducted from the perspective of U.S. healthcare payers. The objective is to furnish crucial economic insights that will aid clinicians, healthcare financiers, and policymakers in navigating the complex terrain of EC treatment strategies.
Methods
As this study is entirely based on previous research and publicly available data, it does not include any new research involving human participants or animals by any of the authors, and therefore does not require approval from an independent ethics committee. The study was completed in July 2024. The economic analysis adhered to the methodological guidelines established by the Second Panel on Cost-Effectiveness in Health and Medicine11, and the findings are reported in accordance with the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) 2022 checklist, detailed in Table S1.
Patients and treatments
The clinical data used in this study were derived from a multicenter, open-label, randomized Phase III trial (DUO-E)9. Patients aged 18 and older, newly diagnosed with advanced or recurrent epithelial histology endometrial cancer, were screened for enrollment and randomly assigned (1:1:1) to one of three treatment groups: DOCT, DCT, or CT. Maintenance therapy commenced within 3 to 9 weeks after the initial treatment and continued until unacceptable toxicity, disease progression, or patient withdrawal of consent. The specific treatment protocols for each group were as follows. DOCT group: platinum-based chemotherapy plus durvalumab 1120 mg intravenous injection (IV) every 3 weeks for 6 cycles, followed by maintenance durvalumab 1500 mg IV every 4 weeks and olaparib 300 mg twice daily. DCT group: platinum-based chemotherapy plus durvalumab 1120 mg IV every 3 weeks for 6 cycles, followed by maintenance durvalumab 1500 mg IV every 4 weeks and a placebo. CT group: platinum-based chemotherapy (carboplatin AUC-5, paclitaxel 175 mg/m²) every 3 weeks for 6 cycles, followed by a maintenance placebo.
Following disease progression, due to the absence of detailed post-progression treatment protocols within the DUO-E trial, we assumed based on the NCCN Guidelines for Uterine Neoplasms (Version 2024.v2) and expert consultations, that patients might receive one of the following four treatment options until death: liposomal doxorubicin (50 mg/m² IV every 4 weeks), albumin-bound paclitaxel (260 mg/m² IV every 3 weeks), bevacizumab (15 mg/kg IV every 3 weeks), or topotecan (1.5 mg/m², continuous IV over 5 days every 3 weeks)12. When patients experience disease progression, we assumed an equal probability for each patient to receive these four treatment regimens, then calculated the per-cycle cost of each drug based on dosage, while also assuming that each patient would receive one session of end-of-life care prior to death.
The model assumes a median patient age of 65 years, based on the clinical trial population. According to the Centers for Disease Control and Prevention (CDC), the estimated average height and weight for a 65-year-old American woman are 162.1 cm and 75.5 kg, respectively, resulting in a body surface area of 1.80 m²13. Additionally, the estimated average creatinine clearance is 70 ml/min, as reported in the literature14.
Model construction
A Markov model was constructed using TreeAge Pro 2022 software (TreeAge Software, LLC, USA), encompassing three mutually exclusive health states: progression-free survival (PFS), disease progression (PD), and death (Fig. 1)15. PFS and death were designated as the initial and terminal states, respectively. Patients in the PFS state could transition to PD or death after initial treatment, while those in the PD state receiving subsequent therapy could deteriorate to death. All patients were initially assigned to the PFS state. The model ran for approximately 20 years, during which the mortality rate for each treatment group exceeded 95%, with a cycle length of 21 days to match the chemotherapy administration cycle. During each cycle, patients could remain in the same health state or experience disease progression; once disease progression occurred, patients could not revert to a previous state, thereby incurring specific treatment costs and health outcomes. The primary outcomes of the model included total costs, quality-adjusted life years (QALYs), and the incremental cost-effectiveness ratio (ICER). Following the World Health Organization (WHO) recommendations and previous publications, a willingness-to-pay (WTP) threshold of $150,000 per QALYs was selected for U.S. payers16. Half-cycle correction was applied in the calculation of costs and utilities, with an annual discount rate of 3%.

Model structure of a decision tree combining the Markov model with the 3 health states. DOCT Durvalumab plus Olaparib and chemotherapy, DCT Durvalumab plus chemotherapy, CT chemotherapy, OS overall survival, PD progressed disease, PFS progression-free survival.
Model parameters
Transition probabilities
The OS and PFS curves were digitized using GetData Graph Digitizer 2.0 software. Following the method developed by Guyot et al. [15], we utilized R software (version 4.4.1) to fit and extrapolate Kaplan-Meier survival curves, evaluating 15 different distributions: exponential, Weibull, gamma, log-normal, Gompertz, log-logistic, generalized gamma, FP1, FP2, restricted cubic splines (RCS), Royston-Parmar (RP) hazard, RP-odds, RP-normal, generalized additive models (GAM), and mixture-cure. The best-fitting model for long-term clinical survival outcomes was selected through a comprehensive evaluation based on visual inspection, clinical plausibility, and statistical criteria including the Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) results15. The fitted results are shown in Table S2, S3 and Fig S1, S2, S3. The cumulative number of patients in the PFS state over time was calculated by integrating the area under the PFS curve. Conversely, the area above the OS curve quantified the total number of patients in the death state, and the area between the PFS and OS curves indicated the cumulative number of patients in the post-progression state. Transition probabilities were derived from parameters of the fitted models, and mortality rates for patients in the PFS state were assessed using the U.S. female life table, stratified by age groups.
Costs estimates
Cost analysis was conducted from the perspective of U.S. payers, considering only direct medical costs. These included drug acquisition, follow-up visits, physician consultations, tumor imaging, laboratory tests, end-of-life care, and management of adverse events (AEs). Drug costs were sourced from the Centers for Medicare & Medicaid Services17 and relevant U.S. drug pricing websites18, using the average sales prices for 2024. All other costs were obtained from published literature (Table 1). To account for inflation, we adjusted the costs to 2024 levels using Tom’s Inflation Calculator19.
Utility inputs
As the DUO-E trial did not provide detailed reports from the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30) regarding the global health status and quality of life dimension, we utilized data from previously published literature. The average health utility values for PFS, PD, and death states were 0.871, 0.779, and 0, respectively20. In line with conventional research methods, our primary focus was on severe treatment-related AEs of grade 3 or higher, with an incidence rate of 5% or greater. This focus was chosen because mild AEs typically do not require treatment or incur significant costs. The impact on quality of life (QoL) associated with clinical events was assessed by multiplying the disutility values of AEs by their incidence rates (Table S5).
Sensitivity analyses
The robustness of the model was assessed through one-way sensitivity analysis and probabilistic sensitivity analysis. In the sensitivity analyses, costs were modeled using a gamma distribution, while health utilities, transition probabilities, AEs, and discount rates were modeled using a beta distribution, following the recommendations of the ISPOR-SMDM Modeling Good Research Practices Task Force21. The standard deviations for each distribution were obtained from the literature whenever possible; otherwise, they were calculated as ± 20% of the mean value. The results of the one-way sensitivity analysis will be visually presented using a tornado diagram. Additionally, for the probabilistic sensitivity analysis, we performed 1,000 Monte Carlo simulations, with the results depicted using cost-effectiveness acceptability curves and scatter plots.
Scenario analysis
Since the FDA has only approved the DCT regimen for the dMMR population, we conducted four scenario analyses within the dMMR subgroup to simulate potential real-world situations. Scenario 1: The model’s time horizon was adjusted to 10, 15, and 25 years to assess the impact of model duration on the outcomes. Scenario 2: To reflect clinical practice, where some patients discontinue treatment after disease progression, we assumed that 80%, 50%, or 0% of patients received subsequent treatments. Scenario 3: We evaluated the impact of different durvalumab prices on cost-effectiveness by reducing its initial assumed price by 50%, 25%, and 10%. In addition, since the DUO-E trial did not specify a maximum treatment duration for durvalumab, we referred to previous clinical trials on immunosuppressants for endometrial cancer, namely RUBY and GY-018, where the maximum treatment durations of dostarlimab and pembrolizumab were both set at three years22,23. Therefore, in Scenario 4, we limited durvalumab treatment to 2 years and 3 years instead of continuing until PD, to evaluate the potential impact of restricting treatment duration on cost-effectiveness.
Results
Base case analysis
In the dMMR EC cohort, DOCT incurred total costs of $1,204,763.33 with 5.49 QALYs gained, while DCT incurred $590,732.13 with 4.61 QALYs, and CT incurred $149,528.15 with 3.68 QALYs. The ICER for DOCT and DCT compared to CT were $584,140.94 and $476,946.43 per QALYs, respectively. (Table 2)
In the pMMR EC cohort, DOCT had total costs of $421,126.70 with 3.00 QALYs, DCT incurred $400,470.92 with 2.45 QALYs, and CT incurred $133,424.52 with 1.69 QALYs. The ICER for DOCT and DCT compared to CT were $219,601.20 and $351,777.86 per QALYs, respectively. (Table 2)
For the overall population, DOCT incurred $607,921.80 with 3.89 QALYs, DCT incurred $417,637.19 with 2.82 QALYs, and CT incurred $141,594.38 with 2.16 QALYs. The ICER for DOCT and DCT compared to CT were $269,195.01 and $416,098.68 per QALYs, respectively. (Table 2)
All ICER exceeded the $150,000 per QALYs willingness-to-pay threshold, indicating that neither DOCT nor DCT is cost-effective compared to CT for first-line treatment of advanced EC in the U.S., overall population, dMMR, and pMMR subgroup.
Sensitivity analysis
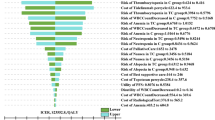
The tornado diagram, as shown in Fig. 2 and Fig S4, illustrates the significant impact of specific parameters on the ICER in this study. Notably, the cost of durvalumab, as well as the utilities of PD and PFS, had substantial effects on the ICER across all groups. Other parameters had moderate to minimal impacts on the ICER. When all parameters were varied within their respective ranges, there was no overlap between the generated ICER values and the WTP threshold, confirming the robustness of our model results.

Tornado diagrams illustrating the results of DOCT (A) and DCT (B) vs. CT for dMMR EC. DOCT Durvalumab plus Olaparib and chemotherapy, DCT Durvalumab plus chemotherapy, CT chemotherapy, EV expected value, PD progressive disease, PFS progression-free survival, dMMR mismatch repair-deficient, BSA Body surface area.
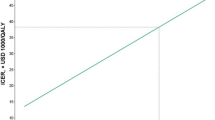
To study the spatial distribution of the data points, we conducted 1,000 Monte Carlo simulations. The results indicated that all scatter plots were located in the first quadrant of the coordinate axis (Fig. 3 and Fig S5), suggesting that increasing the use of durvalumab and olaparib improves QALYs, while also increasing the associated costs. DCT had only a 0.4% probability of being cost-effective compared to CT in dMMR EC. In contrast, the probability of DOCT being cost-effective compared to CT was 5.4% in pMMR EC and 0.6% in the overall population (Fig. 4 and Fig S6).

Scatter plot diagrams showing the incremental cost-effectiveness of DOCT (A) and DCT (B) for dMMR EC. DOCT Durvalumab plus Olaparib and chemotherapy, DCT Durvalumab plus chemotherapy, CT chemotherapy, dMMR mismatch repair-deficient, WTP Willingness to Pay.

Cost-effectiveness acceptable curve for dMMR EC. DOCT Durvalumab plus Olaparib and chemotherapy, DCT Durvalumab plus chemotherapy, CT chemotherapy, WTP Willingness to Pay, dMMR mismatch repair-deficient.
Scenario analysis
The results of all scenario analyses indicate that, regardless of whether the model duration was set at 10 years, 15 years, or 25 years, whether 80%, 50%, or 0% of patients received subsequent treatment after PD, whether the price of Durvalumab was reduced by 50% or 25%, or whether its treatment duration was extended to 2 years or 3 years, DOCT and DCT were not cost-effective compared to CT (Table S4). It was only when the price of durvalumab was reduced to 10% that DCT became cost-effective compared to CT. For DOCT to be cost-effective, the price of durvalumab would need to be reduced to 1.6%.
Discussion
EC is one of the most prevalent gynecological malignancies among women globally, with a significant rise in both incidence and mortality rates over the past few decades. This rise is particularly notable in developed countries, driven by factors such as an aging population and increasing obesity rates. The recent DUO-E trial demonstrated that combining durvalumab with chemotherapy, followed by maintenance therapy with durvalumab (with or without olaparib), significantly improved OS and PFS compared to chemotherapy alone. However, despite the notable clinical benefits of these innovative therapies, their high costs have raised considerable concerns about cost-effectiveness. In the context of limited healthcare resources and the substantial financial burden associated with cancer treatment, value-based oncology research has become increasingly critical. In recent years, the management of EC has evolved significantly, transitioning from traditional pathological classification to more precise risk stratification based on molecular and immunohistochemical markers. Studies have identified four key molecular subgroups of EC, defined by polymerase-ε (POLE) mutations, p53 protein status, and MMR protein expression, offering new insights into clinical management24,25. These molecular subgroups exhibit significant prognostic differences, with the DUO-E trial highlighting superior therapeutic outcomes in the dMMR subgroup compared to the pMMR subgroup. Building on these findings, this study conducted a cost-effectiveness analysis of the comprehensive DOCT and DCT regimens from the perspective of U.S. payers, focusing on the dMMR subgroup.
Our findings indicate that compared to chemotherapy, the incremental ICER for the DCT regimen in the dMMR, pMMR, and overall populations are $476,946.43, $351,777.86, and $416,098.68 per QALYs, respectively. For the DOCT regimen, the ICER are $584,140.94, $219,601.20 , and $269,195.01 per QALYs, respectively, all exceeding the WTP threshold of $150,000 per QALYs. Therefore, both DOCT and DCT regimens are not cost-effective in the dMMR, pMMR, and overall populations. Compared to pMMR EC patients, the treatment regimens show higher survival benefits in dMMR EC patients, with DOCT and DCT regimens increasing QALYs by 2.49 and 2.16 , respectively. This enhanced response in the dMMR subgroup may be attributed to the increased expression of the PD-1 receptor and its ligand PD-L1, characteristic of the dMMR molecular profile, which makes these patients particularly responsive to therapies targeting PD-1 and PD-L1 inhibitors. However, despite the survival benefits in the dMMR group, these come with higher costs. The total costs for the treatment regimens are $1,204,763.33 for the dMMR group, $421,126.70 for the pMMR group, and $607,921.80 for the overall population. The significantly higher costs associated with treating the dMMR group, primarily driven by the intensified therapeutic approach, are the primary contributors to the elevated ICER observed in this subgroup compared to the overall population.
Additionally, the lack of cost-effectiveness of the new treatment regimens may be attributed to the prolonged PFS and PD periods due to the extended use of durvalumab, leading to higher drug costs. In the scenario analyses, outcomes were evaluated for model durations of 10, 15, and 25 years (Table S4). Over time, the costs of DOCT and DCT escalated rapidly, directly increasing the ICER, likely due to the unrestricted use and high cost of durvalumab. To address this issue, we simulated limiting durvalumab treatment to durations of 2 and 3 years, based on evidence from the RUBY and GY-018 clinical trials22,23. However, the results indicated that DOCT and DCT still failed to achieve cost-effectiveness within the dMMR EC population. Sensitivity analyses further revealed that even when the price of durvalumab fluctuated within a range of $6.549 to $9.824 per mg, the total costs remained above the predefined WTP threshold of $150,000 per QALYs. Scenario analyses showed that, from the perspective of U.S. payers, the price of durvalumab would need to be reduced by approximately 90% for DCT and 98.4% for DOCT to achieve a cost-effectiveness probability greater than 50% compared to CT in the dMMR population. These findings underscore the critical need to reduce the price of durvalumab to improve the accessibility of DOCT and DCT. Governments and policymakers should implement strategies to make these promising therapies cost-effective, enabling broader patient access. Pharmaceutical companies can contribute by enhancing the economic feasibility of these regimens through cost reductions achieved via optimized production processes, improved supply chain efficiency, and adjusted market pricing strategies. Concurrently, governments could facilitate price reductions by introducing drug price regulations, promoting the development of generic alternatives, and offering subsidies or tax incentives.
The results of the sensitivity analysis also show that the most influential parameters in our model are the utility values of PD and PFS. The utility data for PD and PFS used in our study were derived from published research on EC patients20. To ensure the robustness of our findings, we conducted sensitivity analyses using a wide range of utility values obtained from various research sources. The results indicated that variations in utility values did not significantly affect our conclusions. Furthermore, sensitivity analysis revealed that the costs of subsequent treatment drugs also had a certain impact on the ICER. Accordingly, in the scenario analyses, we further explored situations where 80%, 50%, and 0% of patients received subsequent treatment. However, the results indicated that these variations did not substantively affect our original conclusions.
The strengths of our study are worth highlighting. Firstly, to our knowledge, this is the first cost-effectiveness analysis evaluating durvalumab as a first-line treatment for advanced EC, as well as the first to examine the cost-effectiveness of combining immunotherapy and PARP inhibition for advanced EC. Secondly, all our parameters were derived from the latest published clinical evidence and literature, thereby minimizing the potential impact of variability in healthcare costs on our results. Additionally, we analyzed different patient subgroups within the advanced EC population, including dMMR and pMMR subgroups, to gain a deeper understanding of the cost-effectiveness of each treatment regimen in specific patient groups. We also conducted scenario analyses within the dMMR population to capture a range of clinical practice scenarios, thereby enhancing the applicability and generalizability of our findings. Given the variations in healthcare systems and patient characteristics across countries, our study specifically adopts the perspective of U.S. payers. Therefore, these data can provide a basis for clinicians, policymakers, and patients in the U.S. to make the most appropriate decisions regarding healthcare-related financial issues. Our findings also offer objective references for the potential approval of DOCT and DCT regimens for broader EC subgroups under international guidelines. These findings not only provide robust scientific evidence to inform clinical practitioners, policymakers, and patients in the United States on healthcare financing decisions but also offer valuable insights to pharmaceutical companies for optimizing drug development and pricing strategies. Furthermore, our results serve as objective support for advocating the broader adoption of DOCT and DCT regimens within an expanded EC subgroup, in alignment with international guidelines.
However, our study has certain limitations that need to be acknowledged. Firstly, similar to most previous studies, our research focused solely on grade 3 or higher AEs with an incidence of ≥ 5%. This approach may lead to an underestimation of the ICER. It is important to note that the treatment costs and disutility associated with lower-grade and less frequent AEs have minimal impact on the overall results. Secondly, the DUO-E clinical trial did not provide health-related quality of life data. The utility values used in our study for disease states were derived from previously published advanced EC studies, which may not accurately reflect the quality of life of U.S. patients. However, one-way sensitivity analysis demonstrated that variations in utility values within a reasonable range did not alter the original conclusions. Thirdly, the DUO-E clinical trial did not specify standard subsequent treatments for patients with recurrent or metastatic EC after second-line treatment failure. We assumed that patients in both groups would receive follow-up treatments according to NCCN guidelines and global oncologists’ standards. Sensitivity and scenario analyses were conducted for the follow-up treatment regimens, and the results indicated that our assumed subsequent treatments did not affect the original outcomes. Despite these limitations, our findings provide valuable economic insights for decision-makers.
Conclusion
In conclusion our study evaluated the cost-effectiveness of durvalumab combined with chemotherapy, followed by maintenance therapy with durvalumab (with or without olaparib), compared to chemotherapy alone. The results indicate that, from the perspective of U.S. payers, DOCT and DCT are not cost-effective options compared to chemotherapy in the dMMR, pMMR, and overall populations. Reducing the price of durvalumab could potentially improve the cost-effectiveness of these new treatment regimens. Future real-world studies and health outcomes assessments of durvalumab are needed to provide further guidance and decision-making references for physicians, patients, and health insurance policymakers.
Data availability
The clinical data used in this study were obtained from the publicly available DUO-E Phase III trial results (NCT04269200), which can be accessed at ClinicalTrials.gov. All other cost and utility parameters were sourced from publicly available literature and databases as cited in the manuscript.
References
Cancer, F. & Fig. (2024). https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/2024-cancer-facts-figures.html
Siegel, R. L., Giaquinto, A. N. & Jemal, A. Cancer statistics, 2024. CA Cancer J. Clin. 74, 12–49 (2024).
Crosbie, E. J. et al. Endometrial cancer. Lancet 399, 1412–1428 (2022).
Rütten, H. et al. Recurrent endometrial Cancer: local and systemic treatment options. Cancers 13, 6275 (2021).
Van Gorp, T. et al. ENGOT-en11/GOG-3053/KEYNOTE-B21: a randomised, double-blind, phase III study of pembrolizumab or placebo plus adjuvant chemotherapy with or without radiotherapy in patients with newly diagnosed, high-risk endometrial cancer. Ann. Oncol. 35, 968–980 (2024).
Colombo, N. et al. Atezolizumab and chemotherapy for advanced or recurrent endometrial cancer (AtTEnd): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 25, 1135–1146 (2024).
Johnson, M. L. et al. Durvalumab with or without Tremelimumab in Combination with Chemotherapy as First-Line Therapy for Metastatic non–small-cell Lung Cancer. JCO 41, 1213–1227 (2023).
Joly, F. et al. Multicentre randomized phase II trial of olaparib as maintenance therapy in platinum-sensitive advanced endometrial carcinoma: the GINECO-UTOLA study. JCO 38, TPS6109–TPS6109 (2020).
Westin, S. N. et al. Durvalumab Plus Carboplatin/Paclitaxel followed by maintenance Durvalumab with or without Olaparib as First-Line treatment for Advanced Endometrial Cancer: the Phase III DUO-E trial. JCO 42, 283–299 (2024).
FDA approves durvalumab with chemotherapy for mismatch repair deficient primary advanced or recurrent endometrial cancer. FDA. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-durvalumab-chemotherapy-mismatch-repair-deficient-primary-advanced-or-recurrent (2024).
Sanders, G. D. et al. Recommendations for Conduct, Methodological Practices, and reporting of cost-effectiveness analyses. JAMA 316, 1093 (2016).
National Comprehensive Cancer Network. - Home. https://www.nccn.org/
National Health Statistics Reports, Number 122, December 20. (2018). (2018).
Zheng, Z., Fang, L. & Cai, H. First-line treatment with durvalumab plus chemotherapy versus chemotherapy alone for metastatic non-small-cell lung cancer in the USA: a cost-effectiveness analysis. BMJ Open. 13, e076383 (2023).
Williams, C., Lewsey, J. D., Mackay, D. F. & Briggs, A. H. Estimation of Survival probabilities for Use in cost-effectiveness analyses: a comparison of a multi-state Modeling Survival Analysis Approach with Partitioned Survival and Markov Decision-Analytic Modeling. Med. Decis. Mak. 37, 427–439 (2017).
Neumann, P. J., Cohen, J. T. & Weinstein, M. C. Updating cost-effectiveness — the curious resilience of the $50,000-per-QALY threshold. N Engl. J. Med. 371, 796–797 (2014).
Centers for Medicare & Medicaid Services. ASP drug pricing files. (2024). https://www.cms.gov/medicare/payment/part-b-drugs/asp-pricing-files
Lynparza https://everyone.org/zh/lynparza-olaparib#productprice
Tom’s Inflation Calculator. https://www.halfhill.com/inflation_js.html
Huo, G., Song, Y. & Chen, P. Cost-effectiveness of atezolizumab plus chemotherapy for advanced/recurrent endometrial cancer. J. Gynecol. Oncol. 35, e83 (2024).
Briggs, A. H. et al. Model parameter estimation and uncertainty analysis: a report of the ISPOR-SMDM modeling Good Research practices Task Force Working Group–6. Med. Decis. Mak. 32, 722–732 (2012).
Mirza, M. R. et al. Dostarlimab for Primary Advanced or recurrent endometrial Cancer. N Engl. J. Med. 388, 2145–2158 (2023).
Eskander, R. N. et al. Pembrolizumab plus Chemotherapy in Advanced Endometrial Cancer. N Engl. J. Med. 388, 2159–2170 (2023).
D’Oria, O., Giannini, A., Besharat, A. R. & Caserta, D. Management of Endometrial Cancer: Molecular Identikit and tailored therapeutic Approach. CEOG 50, 210 (2023).
Baker-Rand, H. & Kitson, S. J. Recent advances in Endometrial Cancer Prevention, early diagnosis and treatment. Cancers 16, 1028 (2024).
Zhu, Y., Liu, K. & Zhu, H. Immunotherapy plus chemotherapy in patients with advanced endometrial cancer: a cost-effectiveness analysis. J. Gynecol. Oncol. 36, e6 (2024).
Huo, G., Song, Y., Liu, W., Guo, H. & Chen, P. Cost-effectiveness of dostarlimab plus chemotherapy for primary advanced or recurrent endometrial cancer. Front. Pharmacol. 15, 1391896 (2024).
Liao, X. et al. Lenvatinib plus Pembrolizumab in the patients with advanced previously treated endometrial cancer: a cost-effectiveness analysis in the United States and in China. J. Obstet. Gynaecol. 50, 881–889 (2024).
Liu, K., Zhu, Y., Zhou, Y., Zhang, Y. & Zhu, H. Pembrolizumab plus Lenvatinib as first-line therapy for patients with mismatch repair-proficient advanced endometrial cancer: a United States-based cost-effectiveness analysis. Gynecol. Oncol. 166, 582–588 (2022).
Fee Schedules - General Information | CMS. https://www.cms.gov/medicare/payment/fee-schedules
Funding
This study was supported by grants from the National Natural Science Foundation of China [grant number 71804025].
Author information
Authors and Affiliations
Contributions
Conception and design, acquisition of data, Writing-original draft: Jiahao Zhang. Analysis and Interpretation of data: Jianying Lei, Caicong You and Wu FuCritical revision of the manuscript for intellectual content: Hongfu Cai and Bin ZhengSupervision: Maobai LiuObtaining funding: Na LiAll authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Ethics approval for this study was not required per the authors university regulations.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhang, J., Lei, J., You, C. et al. Cost-effectiveness analysis of durvalumab with chemotherapy and maintenance durvalumab with or without olaparib for advanced endometrial cancer. Sci Rep 15, 2497 (2025). https://doi.org/10.1038/s41598-025-86021-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-86021-y
