
Abstract
To analyze the relationship between hot or cold, and wet or dry interacting weather, and urolithiasis-related hospitalizations. Distributed lag nonlinear model for time series design was used to build exposure-response curves for the association of daily mean temperature and relative humidity with urolithiasis-related hospitalizations. Cut-off values were determined for temperature, humidity, and dichotomous categories to define heat-cold and wet-dry meteorological conditions. Based on a total of 38,184 urolithiasis-related hospitalizations from 2018 to 2019 in Ganzhou as a large prefecture-level city in southern China, dry-heat weather during the hot season (May to September) increased the risk of urolithiasis-related hospitalizations (relative risk [RR]: 1.17, 95% confidence interval [CI]: 1.02, 1.35), with the most pronounced effects in those aged 21–40 years and male. Wet-cold weather in the cold season (December to February) increased the risk of urolithiasis-related hospitalizations in the total population (RR: 1.58, 95% CI: 1.20, 2.07). The effect was significant in the 21–60 years old age and both genders groups. Both dry-heat weather in the hot season and wet-cold weather in the cold season could trigger urolithiasis.
Similar content being viewed by others

Introduction
Urolithiasis, also known as urinary calculi, is a common urological disease with kidney stones being the most common manifestation. The main clinical symptoms include low back pain and hydronephrosis, urinary tract infection, and hematuria, which can lead to chronic kidney disease and decreased renal function1. Climate change is expected to increase the incidence of kidney diseases, including urolithiasis, because of rising temperatures2. According to a global epidemiological study of urolithiasis3, the number of patients with urolithiasis increased from 7.78 million in 1990 to 115.55 million in 2019, a 48.57% increase in incidence. A meta-analysis of 22 provinces in China in 2022 4 found that the prevalence of urolithiasis was 8.1%, and the lifetime recurrence rate has been reported as approximately 60–80% 5. The future impact of urolithiasis on the healthcare system is predicted to be substantial because of its high prevalence and recurrence rates.
The incidence of urolithiasis has been linked to ambient temperature6,7, with higher workplace or climatic temperatures acting as risk factors for the disease. An ecological study2 found that a 1℃ increase in daily minimum temperature was associated with a 1.5% increase in emergency department admissions for urolithiasis. In China, between 2014 and 2019, annual heatwaves from May to September resulted in 138,812 hospitalizations for urolithiasis, resulting in direct and indirect costs of 1.19 billion Chinese yuan renminbi (CNY)8. In the context of global warming, the number of patients with urolithiasis and healthcare expenditures are predicted to increase9. Studies on other meteorological factors and urolithiasis have shown that relative humidity is another influential factor, with a projected reduction in the number of treatments for urolithiasis of 3.224 for every 1% increase in relative humidity in southern Taiwan10. A study of six cities in South Korea11 showed that the daily mean urolithiasis incidence in all cities positively correlated with the daily mean temperature and negatively correlated with the daily mean relative humidity.
Studies on the interaction of ambient temperature and humidity12 have shown that exposure to high temperatures and humidity increased the risk of all-cause morbidity in Shanghai, China and that the combined effects of temperature and humidity were expected to have a more pronounced impact on health in a warming climate. Humidity may be an important contributing factor and is more likely to work in conjunction with temperature changes. A current study on composite weather events showed a synergistic and additive effect between low temperature and high humidity in winter in 358 counties or districts of China and that the impact of wet-cold weather was higher than that of dry-cold weather, significantly increasing the risk of death13. Studies on high temperatures and humidity have found that dry-heat events may have a higher mortality risk than wet-heat events14. Studies on the combination of temperature and humidity indicators to evaluate kidney stones found that temperature and humidity jointly determined the risk of kidney stones15 and that the wet-heat index combined with temperature and humidity could more accurately predict the occurrence of kidney stones than ambient temperature alone16. However, most relevant studies have only treated relative humidity as a confounding factor when studying the effect of temperature on urolithiasis or have looked at the effect of temperature or humidity in isolation. Moreover, studies exploring the effect of composite meteorological conditions with combined extremes of temperature and humidity on urolithiasis are rare.
This study aimed to combine two meteorological factors, ambient temperature and relative humidity, to analyze the relationship between hot or cold, and wet or dry interacting weather, and urolithiasis-related hospitalizations in a large city in southern China during the hot and cold seasons. Exploring the effects of composite weather (ambient temperature and humidity) may contribute to determining the impact of climate change on human health and improve the effectiveness of public health prevention strategies.
Materials and methods
Study design and data collection
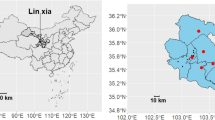
This study was based in the city of Ganzhou, China. Ganzhou City is located in southeast China (24°29′-27°09′ N; 113°54′-116°38′ E) in the south of Jiangxi Province of China. Ganzhou City has a permanent population of 8.98 million, ranking first in the province. The city covers an area of 39,379.64 square kilometers, accounting for 23.6% of the total area of Jiangxi Province, and is the largest administrative region in Jiangxi Province.
The city is situated at the southern edge of the Central Subtropics and has a humid monsoon climate in the subtropical hilly and mountainous regions with long and hot summers, whereas winters are wet and cold with frequent cold air activity. In summer, particularly in July and August, high temperatures that may be categorized as dry and hot are prevalent. In winter, wet and cold weather is more common because of the influence of cold air and increased humidity.
Hospitalization data of patients with urolithiasis in Ganzhou admitted between January 1, 2018 and December 31, 2019 of a total 38,184 cases were obtained from the diagnosis-related group (DRGs) data platform of the Jiangxi Provincial Health Commission. The average annual hospitalization rate of urolithiasis in Ganzhou during the study period was 217.41 per 100,000. Cases from 69 hospitals in Ganzhou, China were included. Of the 69 hospitals, data were collected from 16 tertiary and 53 secondary hospitals. Data included sex, age, admission date, name, and code of the main discharge diagnosis. Urolithiasis was determined according to the International Classification of Diseases, Tenth Revision (ICD-10), Disease Classification codes (N20-N23) and text screening. This study was conducted according to the guidelines of the Declaration of Helsinki. All procedures involving human subjects were approved by the ethics committee of Gannan Medical University (Approval No. 2021107). The need to obtain informed consent was waived by the ethics committee of Gannan Medical University.
Meteorological data were obtained from the National Science Data Center (http://data.cma.cn/) and four basic national meteorological monitoring stations in Ganzhou. Meteorological indicators included daily mean, maximum, and minimum temperatures (℃), and daily mean relative humidity (%), and cumulative rainfall (mm).
Meteorological and urolithiasis-related hospitalization data used in this study were consistent with a previous study17. The difference is that the previous study focused on the influence of temperature alone, while this study focused on the influence of extreme weather conditions of combined temperature and humidity on urolithiasis-related hospitalizations.
Meanwhile, air quality data of the same period were collected from the National Urban Air Quality Real-time publication platform of China (https://www.aqistudy.cn/), including the daily average pollutant data of PM2.5 (µg/m3), PM10 (µg/m3), NO2 (µg/m3), 8-h. O3 (µg/m3), SO2 (µg/m3), and CO (mg/m3). Based on the literature18,19,20, and there was also a high correlation between PM2.5 and PM10, and only five air pollutants excluding PM10 were selected as control variables.
Statistical analysis
Single meteorological effect
We employed time-series design with a distributed lag nonlinear model (DLNM) to analyze the relationship between ambient temperature, relative humidity, and urolithiasis-related hospitalizations and the cumulative lagged effect after controlling for the effects of long-term trend and weekday effects. The number of daily urolithiasis-related hospitalizations was the dependent variable, and the daily mean temperature and relative humidity were the independent variables, respectively21,22. Because of the overdispersion of the number of inpatients with urolithiasis, the model was fitted using a quasi-Poisson distribution. The relationships of the model are as follows:
where \(t\) is the observation day; \(E\left({Y}_{t}\right)\) is the expected number of inpatients on day t; \({Y}_{t}\) is the number of urolithiasis patients on day t; \(\alpha\) is the intercept; \(cb\) is the “cross-basis” function; \(tem{\text{p}}_{t}\) and \(hum{\text{i}}_{t}\) are the daily mean temperature and daily mean relative humidity on day t; lag is the maximum lag days (7 days were selected for this study13), with 3 degrees of freedom; \(ns\) is the natural cubic spline function; \(df\) is the degrees of freedom; \(time\) is the time trend; the degrees of freedom is 7/year23, and \(DOW\) is a dummy variable controlling for the day of the week effect.
Compound meteorological effect
Based on the inconsistency in the definition of heat or humid weather, we referred to previous studies13,14 to determine the thresholds for temperature and humidity. ‘Heat’ and ‘cold’ days were determined according to the cumulative effect curves of ambient temperature and urolithiasis hospitalization. The cumulative effect increased significantly when the daily mean temperature reached 20℃, therefore, the days with daily mean temperature > 20℃ were defined as heat, and the days with daily mean temperature ≤ 20℃ were defined as cold. Similarly, ‘wet’ and ‘dry’ days were determined based on the cumulative effect of relative humidity on the number of urolithiasis-related hospitalizations. We defined days with a daily mean relative humidity > 80% as ‘wet’ and days with a daily mean relative humidity ≤ 80% as ‘dry’. Therefore, the weather throughout the year was categorized as four types: wet-heat, dry-heat, wet-cold, and dry-cold weather. We chose the hot season from May to September to evaluate the effect of dry-heat weather on urolithiasis-related hospitalizations, using wet-heat weather as a reference. We chose the cold season from December to February to assess the impact of wet-cold weather on urolithiasis-related hospitalizations using dry-cold weather as a reference. The relationships of the model are presented according to the following formula:
where \(E\left({Y}_{t}\right)\) is the expected number of inpatients on day t; \(cb\) is the “cross-basis” function, and the nonlinear and lag effects of weather events are calculated by integer functions and natural cubic spline functions, respectively; and \({th}_{t}\) is the weather events on day t. In the hot season, \({\text{t}\text{h}}_{\text{t}}\) represents dry-hot condition, in the cold season, \({\text{t}\text{h}}_{\text{t}}\) represents wet-cold condition. According to qAIC, df of time in formula (3) is also determined to be 7 per year. The other parameters are the same as those in formula (1)14.
Finally, the cumulative effects over a lag of 7 days of dry-heat and wet-cold days on urolithiasis-related hospitalizations in different sex and age groups (0–20, 21–40, 41–60, and > 60 years) were compared to identify vulnerable groups. We conducted pairwise comparisons of effects between different sex and age groups24.
Microsoft Excel 2019 software was used for data collection and sorting, and statistical analyses were performed using the “dlnm” package in R4.2.3 software for distributed lag nonlinear model building, risk assessment, and visualization. Effect estimates are expressed as relative risks (RR) with 95% confidence intervals (CI). The significance level was set at α = 0.05.
Results
Based on the distribution of the monthly average temperature (Fig. 1), we divided the entire year into hot, cold, and normal temperature seasons. The hot season (May to September) and the cold season (December to February) were chosen to evaluate the effects of composite weather.

Distribution of monthly mean temperature from 2018 to 2019 in Ganzhou. Note: Red indicates the hot season; blue indicates the cold season; gray indicates the moderate-temperature season.
Descriptive data on daily admissions for urolithiasis and weather factors are shown in Table 1. A total of 101 days of wet-heat and 197 days of dry-heat in hot season, 89 days of wet-cold, and 88 days of dry-cold weather in cold season occurred between 2018 and 2019. The daily mean temperature in dry-heat weather was (\(\stackrel{-}{x}\)±standard deviation [SD]: 27.85 ± 2.19℃) and humidity was (\(\stackrel{-}{x}\)±SD: 71.66.50 ± 6.94%). Moreover, the daily mean temperature for wet-cold weather was (\(\stackrel{-}{x}\)±SD: 8.99 ± 3.80 °C) and humidity was (\(\stackrel{-}{x}\)±SD: 86.93 ± 3.97%). The mean of daily urolithiasis-related hospitalizations in wet-heat, dry-heat, wet-cold and dry-cold weather was 58, 62, 46 and 40 cases respectively, which more occurred in the male and 41–60 years groups.
According to the Spearman’s correlation analysis results of meteorological factors and urolithiasis-related hospitalizations from 2018 to 2019 (Fig. 2), daily urolithiasis-related hospitalizations positively correlated with the daily mean, maximum, and minimum temperatures, with correlation coefficients of approximately 0.4. A weak negative correlation was found between the daily mean temperature and relative humidity, with a coefficient of -0.18.

Spearman’s correlation analysis between meteorological factors and urolithiasis-related hospitalizations from 2018 to 2019 in Ganzhou.
Figure 3 shows the cumulative effects of ambient temperature and relative humidity on urolithiasis-related hospitalizations. A nonlinear relationship was found between daily mean temperature and the risk of urolithiasis-related hospitalizations, with a significant increase in the cumulative effect as the temperature reached 20 °C. The results between daily mean relative humidity and the risk of urolithiasis-related hospitalization showed that the cumulative effect increased as the relative humidity increased, with the effect curve flattening when the relative humidity was approximately 80%.

Cumulative effect of daily mean temperature and daily mean relative humidity on urolithiasis-related hospitalizations from 2018 to 2019 in Ganzhou. Notes: Left panel: Cumulative effect of daily mean temperature on urolithiasis-related hospitalizations; the solid red line represents the RR, and the gray shaded portion represents the 95% CI. Right panel: Cumulative effect of daily mean relative humidity on urolithiasis-related hospitalizations, with the solid red line representing the RR and the grey shaded portion representing the 95% CI. The dashed line represents the turning point of the corresponding curve. RR, relative risk; CI, confidence interval.
Table 2 shows the cumulative effect of composite weather on urolithiasis-related hospitalization over a lag of 7 days. The results show that the risk of hospitalization for urolithiasis increased within 7 days after the occurrence of dry-heat in hot season or wet-cold in cold season. During the hot season, the risk of urolithiasis-related hospitalization in the total population in dry-heat weather was increased (RR: 1.17, 95% CI: 1.02, 1.35). Significant results showed that for the male (RR: 1.20, 95% CI: 1.02, 1.41) and 41–60-year-old age groups (RR: 1.21, 95% CI: 1.03, 1.42). The risk of urolithiasis-related hospitalizations increased in wet-cold weather in the cold season, and in the overall population (RR: 1.58, 95% CI: 1.20, 2.07). Subgroup analysis showed significant results in the 21–60 years age and both gender groups. However none of the above effects were statistically significant between the age or sex groups. Lag effects are shown in the supplementary file (Fig. S1 and Fig. S2).
Discussions
This study found that a combination of extreme temperature and humidity was significantly associated with urolithiasis-related hospitalizations. Both dry-heat weather in the hot season and wet-cold weather in the cold season increased the risk of urolithiasis-related hospitalizations, and individuals aged 21–60 years were significantly affected by these two weather conditions. The study of the relationship between ambient temperature and humidity on the risk of urolithiasis-related hospitalizations may promote government and public awareness of the impact of complex weather in the future. Our results imply that preventive measures should be adopted to reduce the occurrence of urolithiasis in vulnerable populations under specific weather conditions.
Previous studies10,11,17 found that meteorological factors were associated with the risk of urolithiasis. However, many studies have selected individual meteorological factors such as temperature, humidity, and rainfall, and few have investigated the effects of combined meteorological factors on urolithiasis. Our study found that dry-heat weather during the hot season increases the risk of urolithiasis-related hospitalization. An animal study25 showed that hot and dry climates cause a greater physiological burden than hot and humid climates. Another study found that heat-related health problems have the potential to occur faster in hot and dry climates26. One study conducted in China14 found that high temperature and low humidity may have synergistic effects, and the combined effects may be greater than the sum of their individual effects. Hot and dry weather can accelerate urolithiasis27. According to Li et al.23, the risk of urinary disorders, including urolithiasis, in western China was higher when the ambient temperature was higher and the relative humidity was lower. Other studies on the effect of humidity on the formation of urolithiasis found that when humidity was low and the air was dry, the loss of water from the skin led to a decrease in the volume of urine. This results in concentrating the urine, promoting the precipitation of crystals and the development of stones7. An animal study28 showed that heat waves affect the water content in animals, which could stress the kidneys, and that high temperatures could lead to elevated core temperatures, dehydration, and a hypertonic state of the blood, which in turn could affect urinary function29. According to Foster et al., a dry-heat test resulted in a whole-body sweat rate (scale by body surface area) which was 75 mL/h higher than that in a wet-heat test, and dehydration occurred more rapidly26. Although the biological mechanisms of dry heat on urolithiasis are unclear, one explanation is that hot environments lead to evaporative water loss, reducing blood flow and concentrating the urine, increasing the risk of stones, and potentially affecting the kidneys30. This risk is markedly increased in dry environments with lower humidity31. These studies and the findings from our study suggest that early preventive measures should be implemented to reduce the risk of urolithiasis during dry-heat summer months.
With rising global temperatures under climate change, multiple studies have investigated the effects of heat waves and high temperatures on the human body. However, few studies have investigated the combined effects of cold and wet composite weather. One previous study only demonstrated the effect of low temperatures on urolithiasis-related hospitalization17. Our analysis found that wet-cold weather in the cold season significantly increased the risk of urolithiasis-related hospitalization. A study of wet-cold and dry-cold events and mortality burden13 found a synergistic superimposed interaction effect of low temperature and high humidity, with 6% of wet-cold deaths attributed to additive interactions. Cold and wet weather in winter increases the risk of respiratory diseases and provides suitable conditions for bacterial viruses to survive32. However, the biological mechanism of the combined effect of wet and cold conditions on this interaction remains unclear. One possible cause may be that the body’s thermoregulatory tolerance is impaired because of the cold and damp environment, making one prone to rapid hypothermia33. Further research on the risk of urolithiasis under wet and cold weather conditions is needed.
Stratified analyses of age found that working-age people (21–60 years) were more sensitive to wet–cold and dry–heat weather than other age groups. This may be because this age group, in their daily lives, may perform outdoor labor, with heavy work leading to dehydration34, which may be exacerbated by the particular weather. Previous studies have shown that exercise in cold and wet environments led to thermoregulatory instability and metabolic disturbances35. Dry summers with higher temperatures may lead to more frequent heat stress14. Workers exposed to heat stress and physical exertion are prone to recurrent water and blood volume deficits, often with urine concentration and acidification, leading to urate crystal formation36.
To our knowledge, this is the first study to focus on the combined effects of extreme ambient temperature and humidity on hospitalization for urolithiasis. However, this study had the following limitations that must be considered when interpreting the results. The main limitation of this study was its short time span, covering only two years of data. Although more than 50 cases per day were high, the shorter study period may limit our understanding of long-term trends in extreme weather and health effects. And, the sample size was further decreased by analyzing the hot and cold months separately, which may affect the robustness of the effect estimation. Second, our study considered only the population in one city in southern China, a region with a high incidence of urolithiasis. This study was based on hospital-specific records, they may not be fully representative of the characteristics of the broader population, which may affect the extrapolation of the results. Third, we used data from meteorological monitoring stations to represent individual temperature exposure and did not measure the actual exposure levels of individuals, which may have led to measurement errors. Fourth, this study was ecological in nature and inevitably introduced some errors. Therefore, our results should be interpreted with caution.
Conclusion
In conclusion, we found that dry-heat weather in the hot season and wet-cold weather in the cold season increased the risk of urolithiasis-related hospitalizations. Targeted preventive measures and strategies should be developed for specific weather conditions, and vulnerable populations should take early preventive measures to reduce the incidence of urolithiasis. Specific weather had a non-negligible impact on the occurrence of urolithiasis, providing important evidence for the impact of a complex climate on health. In the future, more research on health effects associated with exposure to multiple climate extremes is needed.
Data availability
Data from this research are available from the corresponding author upon reasonable request.
References
Alexander, R. T. et al. Kidney stones and kidney function loss: A cohort study. BMJ 345, e5287–e5287. https://doi.org/10.1136/bmj.e5287 (2012).
Borg, M., Bi, P., Nitschke, M., Williams, S. & McDonald, S. The impact of daily temperature on renal disease incidence: An ecological study. Environ. Health 16, 114. https://doi.org/10.1186/s12940-017-0331-4 (2017).
Qian, X. Y. et al. Epidemiological trends of urolithiasis at the global, regional, and national levels: A population-based study. Int. J. Clin. Pract. 6807203, (2022). https://doi.org/10.1155/2022/6807203 (2022).
Tan, S. et al. Prevalence of urolithiasis in China: A systematic review and meta-analysis. BJU Int. 133, 34–43. https://doi.org/10.1111/bju.16179 (2023).
Liu, Y. et al. Epidemiology of urolithiasis in Asia. Asian J. Urol. 5, 205–214. https://doi.org/10.1016/j.ajur.2018.08.007 (2018).
Zhang, Y. C. et al. The impact of ambient temperature on the incidence of urolithiasis: A systematic review and meta-analysis. Scand. J. Work Environ. Health 46, 117–126. https://doi.org/10.5271/sjweh.3866 (2020).
Fakheri, R. J. & Goldfarb, D. S. Ambient temperature as a contributor to kidney stone formation: Implications of global warming. Kidney Int. 79, 1178–1185. https://doi.org/10.1038/ki.2011.76 (2011).
Huang, Y. et al. Heatwave and urinary hospital admissions in China: Disease burden and associated economic loss, 2014 to 2019. Sci. Total Environ. 857, 159565. https://doi.org/10.1016/j.scitotenv.2022.159565 (2023).
Kaufman, J. et al. The impact of heat on kidney stone presentations in South Carolina under two climate change scenarios. Sci. Rep. 12, 369. https://doi.org/10.1038/s41598-021-04251-2 (2022).
Lin, C. Y., Juan, Y. S., Huang, T. Y. & Lee, H. Y. The influence of climatic factors in the seasonal fluctuation of urolithiasis and the trend of stone disease management in the southern Taiwan. Urolithiasis 51, 55. https://doi.org/10.1007/s00240-023-01416-8 (2023).
Chi, B. H. et al. Daily mean temperature and urolithiasis presentation in six cities in Korea: Time-series analysis. J. Korean Med. Sci. 32, 999–1008. https://doi.org/10.3346/jkms.2017.32.6.999 (2017).
Liang, C. et al. The influence of humid heat on morbidity of megacity Shanghai in China. Environ. Int. 183, 108424. https://doi.org/10.1016/j.envint.2024.108424 (2024).
Li, M. Y. et al. The comparison of mortality burden between exposure to dry-cold events and wet-cold events: A nationwide study in China. Sci. Total Environ. 904, 166859. https://doi.org/10.1016/j.scitotenv.2023.166859 (2023).
Fang, W. et al. The joint and interaction effect of high temperature and humidity on mortality in China. Environ. Int. 171, 107669. https://doi.org/10.1016/j.envint.2022.107669 (2023).
Ross, M. E. et al. Assessment of the combination of temperature and relative humidity on kidney stone presentations. Environ. Res. 162, 97–105. https://doi.org/10.1016/j.envres.2017.12.020 (2018).
Zhou, L. et al. Ambient heat stress and urolithiasis attacks in China: Implication for climate change. Environ. Res. 217, 114850. https://doi.org/10.1016/j.envres.2022.114850 (2023).
Li, Z. J., Li, Y. L., Wang, X. N., Liu, G. L. & Hao, Y. B. Extreme temperature exposure and urolithiasis: A time series analysis in Ganzhou, China. Front. Public. Health 10, 1075428. https://doi.org/10.3389/fpubh.2022.1075428 (2022).
Li, Y. et al. Association of short-term nitrogen dioxide exposure with hospitalization for urolithiasis in Xinxiang, China: A time series study. Environ. Sci. Pollut. Res. Int. 30, 93697–93707. https://doi.org/10.1007/s11356-023-28539-0 (2023).
Noh, T. I., Hong, J., Kang, S. H. & Jung, J. Association of meteorological factors and ambient air pollution on medical care utilization for urolithiasis: A population-based time-series study. BMC Nephrol. 22, 402. https://doi.org/10.1186/s12882-021-02614-5 (2021).
Xu, H., Liu, Y., Wang, J. & Jin, X. Short-term effects of ambient air pollution on emergency department visits for urolithiasis: A time-series study in Wuhan, China. Front. Public. Health. 11, 1091672. https://doi.org/10.3389/fpubh.2023.1091672 (2023).
Gasparrini, A., Armstrong, B. & Kenward, M. G. Distributed lag non-linear models. Stat. Med. 29, 2224–2234. https://doi.org/10.1002/sim.3940 (2010).
Li, Y. L., Hao, Y. B. & Wang, X. N. Association between ambient temperature and hospitalizations for urolithiasis in four counties of Ganzhou, China. Int. J. Environ. Health Res.. https://doi.org/10.1080/09603123.2024.2334766 (2024).
Li, Y. L. et al. Ambient temperature, humidity, and urinary system diseases: A population-based study in Western China. Environ. Sci. Pollut. R. 29, 28637–28646. https://doi.org/10.1007/s11356-021-17102-4 (2022).
Altman, D. G. & Bland, J. M. Interaction revisited: The difference between two estimates. BMJ 326, 219. https://doi.org/10.1136/bmj.326.7382.219 (2003).
Moran, D., Shapiro, Y., Meiri, U., Laor, A. & Horowitz, M. Heat acclimation: Cardiovascular response to hot/dry and hot/wet heat loads in rats. J. Basic. Clin. Physiol. Pharmacol. 7, 375–387. https://doi.org/10.1515/jbcpp.1996.7.4.375 (1996).
Foster, J., McKenna, Z. J., Atkins, W. C., Jarrard, C. P. & Crandall, C. G. Identifying the optimal heat exposure metric for predicting the physiological response to dry or humid heat stress in Young and older adults: A randomized controlled study. Environ. Health Perspect. 132, 17701. https://doi.org/10.1289/EHP13733 (2024).
Borghi, L. et al. Mean temperature and humidity variations, along with patient age, predict the number of visits for renal colic in a large urban Emergency Department: results of a 9-year survey. J. Epidemiol. Glob. Health. 2, 31–38. https://doi.org/10.1016/j.jegh.2012.01.001 (2012).
Jacobs, P. J., Oosthuizen, M. K., Mitchell, C., Blount, J. D. & Bennett, N. C. Heat and dehydration induced oxidative damage and antioxidant defenses following incubator heat stress and a simulated heat wave in wild caught four-striped field mice Rhabdomys dilectus. PLoS ONE. 15, e0242279. https://doi.org/10.1371/journal.pone.0242279 (2020).
Johnson, R. J. et al. Climate change and the kidney. Ann. Nutr. Metab. 74, 38–44. https://doi.org/10.1159/000500344 (2019).
Eisner, B. H. et al. The effects of ambient temperature, humidity and season of year on urine composition in patients with nephrolithiasis. BJU Int. 110, E1014–1017. https://doi.org/10.1111/j.1464-410X.2012.11186.x (2012).
de Lorenzo, A. & Liaño, F. Altas temperaturas y nefrología: A propósito del cambio climático. Nefrología 37, 492–500. https://doi.org/10.1016/j.nefro.2016.12.008 (2017).
Kim, J. et al. Comprehensive approach to understand the association between diurnal temperature range and mortality in East Asia. Sci. Total Environ. 539, 313–321. https://doi.org/10.1016/j.scitotenv.2015.08.134 (2016).
Thompson, R. L. & Hayward, J. S. Wet-cold exposure and hypothermia: Thermal and metabolic responses to prolonged exercise in rain. J. Appl. Physiol. 81, 1128–1137. https://doi.org/10.1152/jappl.1996.81.3.1128 (1996).
Kale, S. S., Ghole, V. S., Pawar, N. J. & Jagtap, D. V. Inter-annual variability of urolithiasis epidemic from semi-arid part of Deccan Volcanic Province, India: Climatic and hydrogeochemical perspectives. Int. J. Environ. Health Res. 24, 278–289. https://doi.org/10.1080/09603123.2013.818105 (2014).
Weller, A. S., Millard, C. E., Stroud, M. A., Greenhaff, P. L. & Macdonald, I. A. Physiological responses to a cold, wet, and windy environment during prolonged intermittent walking. Am. J. Physiol. Regul. Integr. Comp. Physiol. 272, R226–R233. https://doi.org/10.1152/ajpregu.1997.272.1.R226 (1997).
Roncal-Jimenez, C. et al. Heat stress nephropathy from exercise-induced uric acid crystalluria: A perspective on mesoamerican nephropathy. Am. J. Kidney Dis. 67, 20–30. https://doi.org/10.1053/j.ajkd.2015.08.021 (2016).
Acknowledgements
We would like to thank Ganzhou Municipal Health Commission for supporting the data required for this study. We will continue to deepen cooperation and spare no effort to contribute to building climate-resilient cities and telling the story of China’s adaptation to climate change.
Funding
This work was supported by the National Natural Science Foundation of China (Grant NO. 42165012) and Ph.D. Start-up Fund of Gannan Medical University (Grant NO. QD202013).
Author information
Authors and Affiliations
Contributions
Yanlu Li wrote the main manuscript text and was responsible for material preparation and analysis. Xubiao Duan, Shichen Wan and Xiaoning Wang provided data collection, and constructive suggestions. Yanbin Hao was responsible for conception, writing, reviewing, editing, and financial responsibility. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, Y., Duan, X., Wan, S. et al. Association analysis of dry heat or wet cold weather and the risk of urolithiasis hospitalization in a southern Chinese city. Sci Rep 15, 1651 (2025). https://doi.org/10.1038/s41598-025-86262-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-86262-x
