
Abstract
Evaluate the prognostic performance of the lactate-to-albumin ratio (LAR) for complications in children 5 years of age or younger with second and/or third degree burn injuries during hospitalization in the intensive care unit of a hospital in Lima, Peru. In this retrospective cohort study, we conducted prognostic tests by analyzing the medical records of children aged ≤ 5 years who suffered second- and/or third-degree burn injuries and were subsequently admitted to the ICU of a Lima-based hospital between 2017 and 2022. The LAR was calculated using lactate and albumin values measured within the first 48 h post-burn. The area under the curve (AUC) was utilized to evaluate the prognostic performance of the LAR in predicting complications. A cohort of 258 patients aged ≤ 5 years with second- and/or third-degree burn injuries was examined. Among them, 63 patients experienced complications (24.4%). The estimated AUC ROC for the LAR was 0.63 (95% confidence interval [CI]: 0.54–0.71). After adjusting for confounders, values of LAR above the threshold were found to be associated with a significantly increased risk of complications (adjusted relative risk: 2.23; 95% CI 1.51–3.29; p < 0.001). The LAR exhibited limited prognostic capability for complications in pediatric burn patients. Nevertheless, a significant association was observed between values of LAR above the threshold and increased risk of complications.
Similar content being viewed by others
Introduction
Burn injuries refer to injuries in live tissues induced by physical, chemical, or biological agents. The associated damage may include reversible functional alterations to irreversible tissue destruction1. According to the World Health Organization, approximately 30,000 people suffer severe burn injuries daily worldwide that require medical care, resulting in approximately 180,000 deaths every year2. South America is one of the regions with the highest incidence rate of burn injuries3. Notably, second- and third-degree burn injuries mostly require hospitalization or intensive care unit (ICU) admission. In addition, these are one of the main causes of morbidity and mortality in the pediatric population4.
Although improvements in burn management have reduced the risk of death, the mortality rate remains high5. Recently, the abbreviated burn severity index (ABSI) and Baux score6,7 have been used to predict mortality. However, these scores have some limitations. They have a potential for human error when estimating the body surface area affected by the burn8; moreover, they have a tendency to overestimate mortality risk9. In addition, these scores do not incorporate biochemical parameters that may enhance prognostic performance, such as albumin9,10, lactate11,12, and base deficit, within the first 48 h following the injury10. Although these indicators are routinely analyzed for monitoring and treating patients with burn injuries10,13, their use as prognostic factors of mortality has not been sufficiently supported by clinical studies.
Albumin is a serum protein typically used as a “negative” acute phase reactant14. Hypoalbuminemia is commonly observed in burn patients, where its severity correlates with the extent and depth of the injury9, leading to complications due to reduced oncotic pressure15. Notably, studies in Brazil9 and France16 have assessed the predictive value of albumin for mortality with mixed results, while a Tunisian study has shown high prognostic values of serum lactate for both mortality and sepsis in burn patients11.
To date, the association of the lactate-to-albumin ratio (LAR) with complications in pediatric patients with burn injuries has not been studied. However, it has been investigated in adult patients with severe burn injuries, showing good prognostic performance for mortality, with an area under the receiver operating characteristic curve (AUC) value of 0.8117. In 2019, a total of 39,221 burn cases were reported in the general population of Peru18. According to the Analysis of Health Situation (ASIS, Spanish acronym) conducted by the Instituto Nacional de Salud del Niño (INSN, Spanish acronym) of San Borja in 2019, third-degree burn injuries were associated with the highest morbidity, followed by second-degree burns19. Moreover, the ASIS revealed that the age group requiring the highest number of burn wound care sessions was the 1–4 years group, followed by the 5–9 years group19.
Given the limited evidence regarding the prognostic capability of the LAR in pediatric burn patients and its practical estimation based on values collected from these patients, the current study is highly relevant. Therefore, this study aimed to assess the prognostic performance of the LAR for complications in children aged ≤ 5 years with second- and/or third-degree burn injuries who were admitted to an ICU.
Methods
Study design and context
This was a retrospective cohort study based on prognostic tests conducted at the Instituto Nacional de Salud del Niño of San Borja, Lima, Peru. This institute is a national reference center for pediatric burn care and is the first hospital in Peru to join the WHO Global Burn Registry. It houses a dedicated Sub-Unit for Comprehensive Burn Patient Care and follows a Clinical Guideline for Acute Burn Patient Management, which includes initial stabilization protocols for patients with burn injuries.
Population and sample
The study population consisted of children aged ≤ 5 years with second- and/or third-degree burn injuries who were admitted to the ICU of INSN of San Borja during 2017–2022.
In this study, the inclusion criterion was the complete availability of data regarding the first lactate and albumin measurements within 48 h after the injury. Patients were excluded if they had received albumin prior to the initial measurement to avoid interference with baseline albumin levels. Additionally, individuals with any pre-existing comorbidities before the burn injury were excluded to isolate the effects of the burns on health outcomes. Furthermore, patients who developed any of the study’s specified complications—such as sepsis, acute respiratory distress syndrome, acute kidney injury (AKI), among others—before the collection of the initial samples were also excluded. This criterion was established to differentiate the direct consequences of the burn injuries from complications that could have influenced patient outcomes from the outset of hospitalization. However, as no patients satisfied these exclusion criteria, none of them were excluded from this study.
All patients complying with the inclusion criteria were included in this study. However, for reference purpose, a sample size was estimated using the statistical software MedCalc v. 20 (MedCalc Software Ltd, Belgium).
This study considered a confidence interval (CI) of 95%, statistical power of 80%, and expected AUC of 0.81, according to the study by Moustafa et al.20. Moreover, an allocation ratio of 2.62 was considered based on the study by Naveda-Romero et al.21. A minimum of 227 patients was estimated as necessary.
Variables and procedures
The outcome of this study was the occurrence of complications in patients aged ≤ 5 years with second- and/or third-degree burn injuries during their ICU hospitalization. The complication variables included sepsis, septic shock, respiratory distress syndrome, kidney injury, disseminated intravascular coagulation, multiorgan failure (MOF), and death. Information on complications was obtained from the hospital information system (GalenHos software, an integrated system of hospital management used in the INSN of San Borja), based on clinical records. The LAR was defined as the division of the absolute values of lactate and albumin. Albumin was quantified using a colorimetric assay on the Cobas® system, and lactate levels were determined using amperometric sensors within the GEM Premier 5000 system.
Potential cases were initially identified by searching for all cases in medical records that were compatible with the ICD-10 codes T31.1–T31.9. To obtain epidemiological data and burn characteristics of patients, the database constructed by the burn ICU was used. The database of the burn ICU included all data on patients admitted to ICU, except for the results of their laboratory tests. This information included sex (male/female), age (years), body surface area affected by the burn (%), hospital stay (days), and possible complications during ICU hospitalization (death, sepsis, septic shock, respiratory distress syndrome, acute kidney injury, disseminated intravascular coagulation, and MOF).
Laboratory test results were also collected using the GalenHos software. The values collected during the first measurement within 48 h after the burn were considered. When more than one value was obtained for that period, the first result was considered. The levels of the following parameters were collected: serum lactate (mmol/L), serum albumin (g/dL), hemoglobin (g/dL), hematocrit (%), white blood cell count (WBC/mm3), serum urea (mg/dL), serum creatinine (mg/dL), serum sodium (mEq/L), serum potassium (mEq/L), blood pH, total serum protein (g/dL), and globulins (g/dL).
Statistical analysis
The collected data were uploaded to the REDcap platform. Subsequently, a quality control assessment was conducted, comprising initial detection of coding errors and implausible data. After the completion of this process, the codified database was imported to STATA v. 17.0 (StataCorp, TX, USA).
In the univariate analysis, numerical variables were presented as either mean and standard deviation or median and 25–75 percentiles (p25–p75), contingent on the presence or absence of normality. Normality was assessed using histograms, quantile plots, kurtosis, skewness, and by comparing mean to median values. Categorical variables, on the other hand, were presented in terms of absolute and relative frequencies.
For the bivariate analysis, when comparing complication variables with other numerical variables, either the Student’s t-test or the Mann–Whitney U test was employed, based on assessments of normality and homoscedasticity. Normality was determined using the methods previously mentioned, while homoscedasticity was evaluated with the Levene test. When comparing complication variables with categorical variables, the Fisher’s exact test or Chi-squared test was utilized, depending on the number of expected values ≤ 5.
The AUC was computed to evaluate the prognostic accuracy of the LAR. Additionally, for exploratory purposes, independent AUCs were calculated for lactate and albumin. Given the inverse relationship between albumin levels and the risk of complications (i.e., lower albumin levels are associated with higher risk), the AUC for albumin was calculated by inverting its scale. To determine the optimal cutoff value for LAR, the Youden’s method was employed. Following this, we estimated the sensitivity, specificity, positive predictive value, negative predictive value, positive likelihood ratio, and negative likelihood ratio.
Finally, to assess the association between values of LAR above the threshold (optimal cutoff point) and the presence of complications, crude relative risks and adjusted relative risks (aRR) were estimated using linear models generalized with Poisson family, log link function, and robust variances. In the adjusted model, variables were input using an epidemiological approach (ie. adjusting for confounders such as age, sex, burn surface area, and hospital stay). The presence of multicollinearity was assessed via the coefficient correlation matrix. Estimations were reported with their respective 95% CI, and p-values of < 0.05 were considered to indicate statistical significance.
Ethical aspects
The study protocol was approved by the Ethics Committee of the School of Health Sciences of Universidad Peruana de Ciencias Aplicadas (#437-06-23) and the Ethics Committee of the INSN of San Borja (#028-2022). All patient data remained anonymous, ensuring confidentiality. All methods were performed in accordance with the relevant guidelines and regulations. Furthermore, this study posed no risk to the participants since it did not involve any interventions or procedures.
Results
Characteristics of the population
This study comprised 258 patients, with a median age of 2 [2–3] years. Most of them were males (n = 149, 57.8%). Overall, 63 (24.4%) complications were observed, with sepsis being the most frequent complication (59 [22.9%] patients). In total, 10 (3.9%) deaths were reported; however, not all patients who developed complications died. The median LAR was 0.8 [0.6–1.1]. The other clinical and laboratory characteristics are shown in Table 1.
Characteristics of the population by complication
The complication variables consisted of sepsis, septic shock, respiratory distress syndrome, kidney injury, disseminated intravascular coagulation, MOF, and death. The incidence of complications was significantly higher in females than in males (p = 0.014). Moreover, burn surface area (p < 0.001), hemoglobin level (p < 0.001), hematocrit level (p < 0.001), potassium level (p = 0.006), white blood cell count (p < 0.001), urea level (p < 0.001), creatinine level (p < 0.001), and number of days of hospital stay (p < 0.001) were significantly higher in patients with complications. Conversely, globulin level (p = 0.002), total protein level (p < 0.001), and albumin level (p < 0.001) were significantly lower in patients with complications. The remaining characteristics of the population by complication are shown in Table 2.
Prognostic performance of the LAR
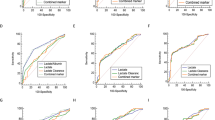
The AUC value for the LAR was 0.63 (95% CI 0.54–0.71) (Table 3). In addition, the estimated cutoff value was 1.25 (95% CI 0.93–1.58). Based on this cutoff value, sensitivity was determined to be 41.30% (95% CI 29.0%–54.50%) and specificity, 86.7% (95% CI 81.10%–91.10%). For exploratory purposes, individual AUC values were also calculated for lactate (0.56; 95% CI 0.47–0.65) and albumin (0.69; 95% CI 0.61–0.77) (Supplementary Fig. 1). Both LAR and albumin demonstrated better discriminatory performance compared to lactate alone, with statistically significant differences observed for LAR versus lactate (p = 0.002) and for albumin versus lactate (p = 0.048). Although albumin exhibited a slightly higher AUC than LAR, this difference was not statistically significant (p = 0.230).
Association between LAR and complications
In the crude model, values of LAR above the threshold were associated with an increased risk of complications (cRR: 2.78; 95% CI 1.87–4.15; p < 0.001). This association remained significant even after adjusting for confounders, such as age, sex, burn surface area, and hospital stay (aRR: 2.23; 95% CI 1.51–3.29; p < 0.001) (Table 4).
Discussion
Main results
Our study revealed that the LAR demonstrates limited prognostic performance for complications in children aged ≤ 5 years with second- and/or third-degree burn injuries. Nevertheless, considering the obtained optimal cutoff value, values of LAR above the threshold were associated with a 2.23-fold increased risk of developing complications compared to values below the threshold. It is also important to mention that we found that serum albumin alone demonstrated a slightly higher AUC compared to LAR, although this difference was not statistically significant, and both markers exhibited limited prognostic performance.
Comparison with other studies
To the best of our knowledge, no studies to date have reported on the association of the LAR with complications in pediatric patients with burn injuries; however, the LAR has been investigated in adult patients with severe burns. In addition, the prognostic performances of lactate and albumin have been evaluated individually in patients with burn injuries.
In France, a study assessed the LAR as a predictor of mortality in adult patients with severe burns. This study revealed that LAR values of > 0.13 upon admission were associated with higher mortality within the first 28 days (Adjusted Odds Ratio = 3.98 [95% CI 1.88–8.35]), and the AUC value for the LAR was 0.81 (95% CI 0.74–0.88; p < 0.05), showing good performance17.
A study conducted in Brazil involving adult patients with burn injuries reported good prognostic performance of albumin, with an AUC value of 0.879. Moreover, a study conducted in Tunisia assessed the prognostic performance of serum lactate in adult patients with burn injuries and reported the AUC values of 0.96 and 0.82 for mortality and sepsis, respectively. The study concluded that serum lactate has good prognostic performance for mortality and sepsis in adult patients with burn injuries11.
Finally, a study conducted in France assessed the association between early hypoalbuminemia (< 24 h) at different time points and mortality in patients with burn injuries. This study revealed that albumin levels measured during the first 4 h after the injury were associated with higher mortality, whereas those measured after 6 h were not useful predictors16.
Result interpretation
Albumin is a serum protein generally used as a “negative” acute phase reactant14. Hypoalbuminemia, whose severity is associated with the extension and depth of the injury, is commonly observed among patients with burn injuries9. This deficiency is caused by albumin extravasation due to increased vascular permeability, presence of wound exudates, and decreased liver synthesis22. Thus, hypoalbuminemia is associated with complications secondary to reduced oncotic pressure, such as edema and hypovolemic shock23. Further, plasma lactate is used as an indicator of hypoperfusion and cell damage. Lactate is a metabolic waste that originates from pyruvate in anaerobic glycolysis, which occurs under hypoxic conditions24. In cases of significant burns, lactate levels tend to increase due to damage and hypoperfusion in different tissues or organs. Thus, the LAR is expected to be higher in patients with more severe burn injuries, considering the greater decrease in albumin levels and increase in lactate levels.
Our study yielded an AUC value of 0.63 for the LAR (95% CI 0.54–0.71). Accordingly, we may conclude that the LAR demonstrates limited prognostic performance. Our results are inconsistent with the abovementioned findings9,11,17, which may be attributed to different reasons. In most previous studies, lactate and/or albumin measurements were obtained within 24 h after the injury11,16. This period was selected because systemic capillary leak tends to prevail from 18 to 24 h, providing the optimal period for measurements17. A study revealed that the optimal measurement period to predict mortality in patients with burn injuries is during the first 4 h after the injury; the study concluded that the closer the time of measurement is to the time of the injury, the better the performance of the marker16. However, our study considered 48 h because the INSN of San Borja is mainly a reference hospital, where patients visit from locations outside the capital city, requiring a long time to arrive to the hospital25. The other studies were conducted in countries with a wider decentralized availability of complexity centers, which was in contrast to our country, where the highest complexity centers are located in the capital city25.
In addition, our study did not assess the management of each patient after the first lactate and albumin measurements. This may affect the prognosis of patients because patients who arrived with high LAR may exhibit improved prognosis after initial management and possible albumin administration compared with those with lower LAR at the cutoff value. Given that albumin alone demonstrated slightly better performance compared to LAR, it is plausible that the capacity of LAR may be diluted when albumin levels are higher due to post-admission interventions. Furthermore, some patients may have received albumin supplementation as part of their management after admission, which could have elevated their albumin levels and impacted its prognostic performance26. Since we did not have data on albumin administration, we could not assess its impact on our results. Monitoring changes in albumin and lactate levels over time would provide additional insights into their prognostic value and the effect of clinical interventions.
The duration of hospital stay may also have indirectly influenced the prognostic performance of the LAR in our study. Prolonged hospital stays can increase exposure to nosocomial infections due to factors such as limited natural ventilation and patient interaction with various hospital procedures27. Such infections could affect prognosis independently of initial burn severity. For example, patients with lower LAR values might still develop complications or die due to secondary infections, despite presenting as noncritical at admission. This is because the prognosis of patients with burn injuries is affected not only by the pathophysiology of the burn injury but also by any other infections that the patient may contract during hospitalization.
Although the LAR showed limited prognostic performance, multivariable analysis revealed that values of LAR above the threshold were significantly associated with a 2.23-fold increased risk of developing complications compared with lower LAR at the cutoff value. This is consistent with previous studies where high LAR values (i.e., increased lactate and decreased albumin values) were associated with an increased risk of death and/or complications17. In addition, these findings are consistent with the pathophysiology of patients with burn injuries28.
Clinical relevance
As described earlier, although the LAR did not exhibit good prognostic performance in our study, it was significantly associated with the development of complications. Furthermore, while albumin alone showed a slightly higher AUC than LAR, the difference was not statistically significant, and both markers exhibited limited prognostic performance. Therefore, the LAR alone cannot be suggested as a marker for risk stratification or for guiding clinical management decisions. However, considering that both lactate and albumin levels are routinely measured in patients with burn injuries, the LAR may still provide useful information when used in conjunction with the tests suggested by clinical practice guidelines29,30 or with scores such as ABSI or Baux score6,7. Combining multiple markers and clinical assessments may improve prognostic accuracy, as relying solely on a single biomarker may not capture the complex pathophysiology of burn injuries.
Limitations
This study has certain limitations. First, lactate and albumin measurements were taken within 48 h post-injury, allowing the inclusion of all patients regardless of arrival time, a shorter interval (< 24 h) may have provided greater prognostic accuracy by capturing the peak systemic capillary leak period. This was feasible in only approximately 60% (59.69%) of patients due to logistical challenges in Peru’s referral system and transport times from remote areas. Thus, the 48 h window in our study may have impacted the accuracy of LAR as an early predictor in this setting. Furthermore, no patients were excluded from the study, as none met the exclusion criteria. While this might suggest that cases were of lower severity without complications reported in the first 48 h, it is also possible that some patients may have required albumin but did not receive it prior to admission due to limited availability in certain regions, including parts of Lima (the capital city). Second, we were unable to adjust for specific severity scores, such as PRISM, due to the unavailability of certain variables in the information system, although we adjusted for burn surface area and length of hospital stay as proxies for severity. Third, our study was conducted at a single health center, which hinders the extrapolation of results to other institutions. Fourth, the analysis did not account for the hazard ratio due to the variable times at which patients developed complications, making a single period classification impractical. Fifth, irregularities in conducting requested tests upon hospital admission for burn injuries may have biased the study findings. Notably, several cases were not included because albumin and/or lactate levels were not measured at admission, which was an inclusion criterion requiring complete data availability within the first 48 h post-injury. Sixth, the classification of burn injuries as second or third degree was not specified in the medical records. As ICU admission requires at least a second-degree burn, the exact degree of burns was not consistently recorded, posing a limitation to our analysis. Finally, there may have been a bias regarding the quality of information as the data recorded in medical records could be inaccurate. However, considering that data were obtained from a national institute specialized in the management of pediatric patients, the information is expected to be as accurate as possible.
Recommendations
Future studies should assess the LAR at different time points (from admission to initial management) to determine whether changes between measurements affect the prognostic performance of the LAR. Future studies are warranted to assess whether the inclusion of the LAR may positively affect the prognostic performance of established scores such as ABSI or Baux score.
Conclusion
The LAR exhibited limited prognostic performance for complications in pediatric patients with burn injuries; however, a statistically significant association was observed between values of LAR above the threshold and an increased risk of complications. Although albumin alone demonstrated a slightly higher prognostic performance than LAR, the difference was not statistically significant. Therefore, while neither marker can be solely recommended for risk stratification, the LAR may still contribute valuable information when assessing pediatric burn patients.
Data availability
Data available on request from the corresponding author (Carlos J. Toro-Huamanchumo, toro2993@hotmail.com) and with previous approval from the Institutional Review Board.
References
Tian, H. et al. Epidemiologic and clinical characteristics of severe burn patients: Results of a retrospective multicenter study in China, 2011–2015. Burns Trauma. 6, 14. https://doi.org/10.1186/s41038-018-0118-z (2018).
World Health Organization. Burns. Published 2018. Accessed October 16, 2023. https://www.who.int/news-room/fact-sheets/detail/burns
Collier, Z. J. et al. 57 Understanding the burden of burn injury in Latin America & the Caribbean. J. Burn Care Res Off Publ Am Burn Assoc. 43(Suppl 1), S39–S40. https://doi.org/10.1093/jbcr/irac012.060 (2022).
Basilico H, Guarranchino J, Murruni A, Tramonti N, Villaboas R. Epidemiología de las quemaduras pediátricas: seis años de experiencia en una unidad especializada de alta complejidad. 2021;24(2):14-22.
Jordan, K. C., Di Gennaro, J. L., von Saint André von Arnim, A. & Stewart, B. T. Global trends in pediatric burn injuries and care capacity from the World Health Organization Global Burn Registry. Front Pediatr. 10, 954995. https://doi.org/10.3389/fped.2022.954995 (2022).
de Melo F, L., Gragnani, A., de Oliveira, A. F. & Ferreira, L. M. Predicting mortality for critically ill burns patients, using the abbreviated burn severity index and simplified acute physiology score 3. Injury 53(2), 453–456. https://doi.org/10.1016/j.injury.2021.11.027 (2022).
Edgar, M. C. et al. The revised baux score as a predictor of burn mortality: A systematic review and meta-analysis. J. Burn Care Res. Off. Publ. Am. Burn. Assoc. 2023, 1075. https://doi.org/10.1093/jbcr/irad075 (2023).
Tejero-Trujeque, R. How effective is the abbreviated burn severity index in predicting patient mortality?. J. Wound Care. 9(10), 475–478. https://doi.org/10.12968/jowc.2000.9.10.26355 (2000).
Aguayo-Becerra, O. et al. Serum albumin level as a risk factor for mortality in burn patients. Clinics. 68(7), 940–945. https://doi.org/10.6061/clinics/2013(07)09 (2013).
Megahed, M. A., El-Helbawy, R. H., Gad, S. S., Mansour, M. M. & Elkandary, K. A. Base deficit, serum albumin level and blood haemoglobin concentration can be used as predictor factors for mortality in major burn patients. Ann Burns Fire Disasters. 33(3), 209–215 (2020).
Mokline, A. et al. Lactate: Prognostic biomarker in severely burned patients. Ann Burns Fire Disasters. 30(1), 35–38 (2017).
Herrero De Lucas, E. et al. Lactate and lactate clearance in critically burned patients: Usefulness and limitations as a resuscitation guide and as a prognostic factor. Burns J. Int. Soc. Burn Inj. 46(8), 1839–1847. https://doi.org/10.1016/j.burns.2020.06.003 (2020).
Yeong, E. K., Tung, K. Y., Chang, C. H. & Tsai, S. J. The relationships between routine admission blood tests and burn size, and length of stay in intensive care unit. J. Formos Med. Assoc. 121(12), 2512–2519. https://doi.org/10.1016/j.jfma.2022.05.012 (2022).
Urquizo Ayala, G., Arteaga Coarite, R. & Chacón, Y. P. Utilidad de los reactantes de fase aguda en el diagnóstico clínico. Rev Médica Paz. 25(2), 91–98 (2019).
Chen, Y. F. et al. Albumin supplementation may have limited effects on prolonged hypoalbuminemia in major burn patients: An outcome and prognostic factor analysis. J. Chin. Med. Assoc. 83(2), 206. https://doi.org/10.1097/JCMA.0000000000000245 (2020).
de Tymowski, C. et al. Early hypoalbuminemia is associated with 28-day mortality in severely burned patients: A retrospective cohort study. Burns J. Int. Soc. Burn. Inj. 46(3), 630–638. https://doi.org/10.1016/j.burns.2019.09.013 (2020).
Dudoignon, E. et al. Usefulness of lactate albumin ratio at admission to predict 28-day mortality in critically ill severely burned patients: A retrospective cohort study. Burns J. Int. Soc. Burn Inj. 48(8), 1836–1844. https://doi.org/10.1016/j.burns.2022.01.003 (2022).
Ministerio de Salud. Resolución Ministerial. Ministerio de Salud; 2020. Accessed September 9, 2021. https://cdn.www.gob.pe/uploads/document/file/1400166/RM%20883-2020-MINSA.PDF.PDF
Instituo Nacional de Salud del Niño. Análisis Situacional de Los Servicios de Salud INSN Año 2019 (ASIS). Instituo Nacional de Salud del Niño; 2019. Accessed September 9, 2021. http://www.insn.gob.pe/sites/default/files/publicaciones/ASIS%202019%20_TOMO%20I.pdf
Moustafa, A. A., Antonios, M. A., Abdellatif, E. M. & Hussain, A. H. Association of lactate-to-albumin ratio level to organ failure and mortality in severe sepsis in a pediatric intensive care unit in Egypt. Turk J Pediatr. 60(6), 691–701. https://doi.org/10.24953/turkjped.2018.06.010 (2018).
Romero, O. N., Meléndez, A. F. N. & Freitez, R. J. M. Factores de riesgo para mortalidad en el niño gran quemado. Pediatría. 53(3), 83–90. https://doi.org/10.14295/rp.v53i3.225 (2020).
Ramos, G., Bolgiani, P., Guastavino, P. & Prezzavento, G. Hipoalbuminemia en pacientes quemados: Un marcador de gravedad que podría definir estadios de evolución. Rev Arg Quem. 15(1), 8–19 (2000).
Lehnhardt, M. et al. A qualitative and quantitative analysis of protein loss in human burn wounds. Burns J Int Soc Burn Inj. 31(2), 159–167. https://doi.org/10.1016/j.burns.2004.08.015 (2005).
Matus-Ortega, G. et al. Las funciones metabólicas, endocrinas y reguladoras de la expresión genética del lactato. Rev. Fac Med México. 63(5), 7–17. https://doi.org/10.22201/fm.24484865e.2020.63.5.02 (2020).
Maguiña, C. & Galán-Rodas, E. Situación de la Salud en el Perú: La Agenda Pendiente. Rev. Peru Med Exp. 28(3), 564–570 (2011).
Navickis, R. J., Greenhalgh, D. G. & Wilkes, M. M. Albumin in burn shock resuscitation: A meta-analysis of controlled clinical studies. J. Burn Care Res. 37(3), e268–e278 (2016).
Llanos-Torres, K. H. Infecciones Nosocomiales En Unidades de Observación de Emergencia y su Asociación con el Hacinamiento y la Ventilación. Rev Peru Med. 37(4), 721–725 (2020).
Kaddoura, I., Abu-Sittah, G., Ibrahim, A., Karamanoukian, R. & Papazian, N. Burn injury: Review of pathophysiology and therapeutic modalities in major burns. Ann Burns Fire Disasters. 30(2), 95–102 (2017).
Eastridge B, Putz B, Ward A. Burn clinical practice guideline. Developed by Texas EMS Trauma & Acute care foundation trauma division. TETAF: TX; 2016.
Yastı, A. Ç. et al. Guideline and treatment algorithm for burn injuries. Ulus Travma Acil Cerrahi Derg. 21(2), 79–89. https://doi.org/10.5505/tjtes.2015.88261 (2015).
Funding
The authors received no specific funding for this work.
Author information
Authors and Affiliations
Contributions
All authors contributed to the design of the study. VCS, CRZ and MAPP oversaw data extraction. CJTH curated the data and performed statistical analysis. All authors contributed to the interpretation of data analysis findings. VCS, CRZ and MAPP wrote the initial draft of the manuscript, and all authors contributed to the review and editing of the manuscript until all authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
Due to the retrospective nature of the study, the Ethics Committee of the School of Health Sciences of Universidad Peruana de Ciencias Aplicadas (#437-06-23) and the Ethics Committee of the INSN of San Borja (#028-2022) waived the need of obtaining informed consent.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Cadarso-Saez, V., Ramirez-Zavala, C., Pérez-Pino, M.A. et al. Lactate to albumin ratio has limited prognostic value for complications in children under five with burn injuries. Sci Rep 15, 2551 (2025). https://doi.org/10.1038/s41598-025-86614-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-86614-7
