
Abstract
This study aimed to examine the impact of both the initial state of emergency (SOE) imposed from April to May 2020 in response to the COVID-19 pandemic and the COVID-19 outbreak itself on the utilization of mental health services among children and adolescents in Japan during the recent pandemic. We conducted an interrupted time series analysis of the number of mental health visits and average incurred medical expenses, stratified by sex and age group, using monthly medical claims data on 3,029,048 patients for the period from January 2016 to December 2020. It was demonstrated that the SOE resulted in a reduced number of visits for mental health services. After the second outbreak of COVID-19 in Japan, which occurred after the SOE, the number of initial visits and the average incurred medical expenses for mental health services increased notably among girls and adolescent females. The findings of this study suggest that: (1) the provision of mental health services for potential patients with mental disorders was insufficient during the pandemic, and (2) the mental health of girls and adolescent females deteriorated during the pandemic. Early screening and treatment of potentially vulnerable patients with mental disorders should be enhanced during a pandemic.
Similar content being viewed by others

Introduction
In March 2020, the World Health Organization declared COVID-19 to be a pandemic. Many countries implemented lockdowns and/or a state of emergency (SOE) to arrest the spread of infection. In Japan, the first such SOE was implemented from April to May 2020, during the country’s initial outbreak of COVID-191. Although the pandemic-related SOEs in Japan did not involve compulsory deterrence, they did influence people’s lives by, for example, recommending that people refrain from going out when not necessary as well as reducing the business hours of restaurants and other establishments1. Notably, visits to medical institutions were regarded as urgent and were recommended when necessary during the SOEs.
The effectiveness of lockdowns and SOEs in preventing further spread of COVID-19 has been confirmed in many countries. However, several studies have also reported adverse effects of these restrictive measures on individuals’ mental health2,3,4,5,6,7,8,9,10. Furthermore, it has been shown that utilization of medical services, including mental health services, tended to decrease during the pandemic11,12,13,14.
Mental disorders can be associated with suicide, as evidenced by various studies15,16. In Japan, suicide is a major cause of death among children and adolescents, and the incidence of suicide remains high among these age groups, contrary to a decreasing trend in adult suicide rates17. A meta-analysis of 54 studies reported an increased suicide rate among young people, including women, during the COVID-19 pandemic18. In Japan, increased suicide rates among young women were reported after the country’s second outbreak of COVID-19, especially in October 20201.
In societies with high suicide rates, the importance of mental health care is particularly heightened. The provision of such care, however, may be significantly affected during pandemics and SOEs. Detailed examination of the trends in mental health service utilization during such extraordinary times is important from a public health perspective. Nonetheless, to the best of our knowledge, only a few such studies have been conducted in Japan.
This study aimed to analyze the impact of the COVID-19 pandemic on the utilization of mental health service among children and adolescents and did so by using a large longitudinal health insurance database covering more than 3 million people in Japan over the 4 years including 2017 to 2020. We used interrupted time series analysis to examine the impact of the pandemic on the number of visits and average incurred medical expenses for mental health and health care services by month, stratified by sex and age group. The results of this study elucidate the trends and shifts in the utilization of mental health services during the pandemic and contribute to the development of a more resilient mental health care system in preparation for future crises.
Methods
COVID-19 pandemic in Japan
Supplementary Figure S1 (available online) presents the weekly number of COVID-19 cases plotted against the dates of the COVID-19 SOE and outbreaks in Japan during 2020. The SOE was initiated in early April 2020, which coincided with the peak of the initial outbreak, and remained in effect until the end of May 2020. On the basis of these data, we designated February 2020, when the weekly occurrence of confirmed cases became continuous, as the start of the COVID-19 pandemic in Japan.
Participants
We used the JMDC Claim Database19, which comprises medical claims data from approximately 300 health insurance societies in Japan. The JMDC Claim Database includes longitudinal observational data on company employees and their dependents and provides information on these individuals’ sex, age, and treatment received at medical institutions.
This study included 3,029,048 individuals, aged 64 years or younger as of February 2020, who were continuously enrolled in the database from January 2016 to December 2020. Those less than 20 years of age were categorized as “children and adolescents,” and those 20 to 64 years were categorized as “adult.” Participants were then stratified by age and sex. The number of participants (age, mean ± SD) in each of these groupings by age category and sex included: 405,716 (11.4 ± 4.5 years) boys and adolescent males, 387,663 (11.5 ± 4.5 years) girls and adolescent females, 1,328,582 (44.0 ± 11.1 years) adult males, and 907,088 (44.6 ± 10.6 years) adult females.
The study protocol was approved by the Ethics Committee of the Research Institute of Healthcare Data Science (Approval No. RI2022010). All research was conducted in accordance with relevant guidelines and regulations. The requirement to obtain informed consent was waived by the Ethics Committee of the Research Institute of Healthcare Data Science because the study used anonymized data.
Outcomes
The number of visits (NOV) and average incurred medical expenses (AIE) by month were used as outcomes pertaining to both initial visits and follow-up visits for mental health services. The use of health care services was also assessed to examine differences in the impact of the pandemic on mental health care vs. general health care services. We defined individuals who used health care services at least once per month from January 2017 to December 2020 as visitors to health care services and defined the total number of monthly visitors as the NOV. Additionally, visitors to mental health services were defined as those who used health care services in a certain month and had at least 1 code indicating receipt of psychiatric treatment (Japanese medical score classification code I002 or I002-2) in that same month. Among these mental health visitors, those who had not visited a mental health service in the past 12 months were defined as initial visit patients, and those who had visited a mental health service in the past 12 months were defined as follow-up visit patients. The AIE for each type of health care service was calculated by dividing the total monthly incurred medical expenses specific to that service by the NOV. Finally, to facilitate comparisons, each NOV and AIE value was normalized to the value as of January 2020.
Statistical analysis
Descriptive statistics
The mean and SD of the NOV and the AIE by sex and age for health care and mental health services were summarized for the 11 months before and after the COVID-19 outbreak (i.e., before the period from February to December 2019 and after the period from February to December 2020).
Impact analysis
For the NOV and AIE specific to each type of health service, we estimated the counterfactual time series assuming that COVID-19 had not occurred and conducted an interrupted time series analysis. We designated February 2020 as the onset of the COVID-19 pandemic in Japan and fitted a time series model using monthly data from January 2017 to January 2020. To create a counterfactual time series, we estimated predicted values for the period from February to December 2020. The Bayesian structural time series (BSTS) model was used to create the counterfactual time series20. Structural time series models consider the seasonality and trend of the time series of interest and allow for flexible and robust modeling, without requiring stationarity. By calculating the sample autocorrelation and partial autocorrelation of each time series for health care services, seasonality was identified in the 1/T asymptotic methods, where T represents the number of time points in the time series21. Therefore, for this study, seasonality terms were incorporated into the BSTS model. Additionally, after removing the seasonality component, the Mann-Kendall test showed that there was a significant trend (P < .001); therefore, we also included the trend effect in the BSTS model. The posterior distribution of the parameters of the BSTS model can be computed using Markov Chain Monte Carlo methods to obtain the posterior distribution of the counterfactual time series and its Bayesian credible interval (BCI). Using this approach, we estimated the mean values and the 95% BCIs of the impacts of the pandemic by calculating the difference between the observed values and the counterfactual values as well as their corresponding BCIs. A BCI differs from a confidence interval in that the BCI represents a probability of the true value being included within the BCI interval. Therefore, on the basis of a prior study20, we defined instances in which the 95% BCI did not contain zero as being representative of a “strong” impact. Furthermore, to facilitate comparison of the impact of the pandemic across groups, we expressed the impact as a percentage that was calculated by dividing the difference between the observed and estimated values by the observed values.
All statistical analyses were conducted using R Statistical Software version 4.1.1 (R Core Team 2021), and CausalImpact package was used to build the BSTS model20.
Results
Descriptive statistics
Number of visits
The NOV for health care services and the NOV for initial and follow-up visits for mental health services from January 2017 through December 2020 are presented in Supplementary Figure S2 through S4. All values were normalized on the basis of the NOV in January 2020. Also, Table 1 presents the unnormalized monthly and mean (SD) NOV for health care services and for initial and follow-up visits for mental health services, by sex and age group, both before (February to December 2019) and after (February to December 2020) the start of the COVID-19 pandemic in Japan. In all groups, the mean NOV for health care services decreased after the onset of the pandemic as compared to before the pandemic. By contrast, after the start of the COVID-19 pandemic, the mean NOV for initial visits for mental health services increased among girls and adolescent females but decreased among all other groups; the mean NOV for follow-up visits for mental health services increased in all groups, reflecting an increasing trend that is depicted in Supplementary Figure S4.
Average incurred medical expenses
The AIE for health care services and for initial and follow-up visits for mental health services from January 2017 through December 2020 are presented in Supplementary Figure S5 through S7. All values were normalized on the basis of the AIE in January 2020. Additionally, Table 2 displays the unnormalized monthly and mean (SD) AIE (in Japanese yen) for health care services and for initial and follow-up visits for mental health services, by sex and age group, before and after the start of the COVID-19 pandemic in Japan. In all groups, the mean AIE for health care services and for initial visits for mental health services increased after the pandemic began; however, the mean AIE for follow-up visits for mental health services increased only among girls and adolescent females.
Impact analysis
Number of visits
Figure 1 presents the results of the analysis of the impact of the COVID-19 pandemic on the NOV by all study participants who visited health care services. Specifically, Fig. 1-a shows the observed and estimated values derived from the BSTS model. All values were normalized on the basis of the observed values as of January 2020 (N = 1,130,411). The estimated values correspond to counterfactual values for the period after the onset of the pandemic. Figure 1-b illustrates the impact of the COVID-19 pandemic on the NOV for health care services along with how well the model fits the observed data for the period before the pandemic began. Implementation of the pandemic-related SOE (April to May 2020) had a strong negative impact on the NOV for health care services, with a particularly notable decrease in the NOV in May 2020 (− 20.7%; 95% BCI, − 30.6% to − 10.7%). Supplementary Figure S8 shows the impact of the COVID-19 pandemic on the NOV for health care service by age/sex group; the negative impact on the NOV in May 2020 was larger among boys and adolescent males (− 30.0%) and girls and adolescent females (− 32.8%) as compared to among adult males (− 14.2%) and adult females (− 20.3%).

Analysis of the impact of the COVID-19 pandemic on the number of visits for health care services. (a) Observed and estimated values of the NOV for health care services, derived from the BSTS model. Pale pink indicates the period after the onset of the pandemic. The estimated values after the onset of the pandemic represent the counterfactual time series. (b) Impact of the COVID-19 pandemic on the NOV after the onset of the pandemic, along with the fitting discrepancy for the period before the pandemic began. BSTS, Bayesian structural time series; NOV, number of visits.
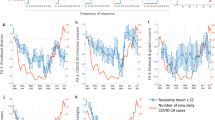
During the period of the SOE, the NOV for initial visits for mental health services was strongly and adversely impacted among all age/sex groups (Fig. 2). After the second outbreak of COVID-19 in Japan, however, in October 2020, a strong increase in the NOV for initial mental health visits was seen among girls and adolescent females (58.6%; 95% BCI, 21.6–96.7%).

The impact of the COVID-19 pandemic on the number of initial visits for mental health services, by sex and age group. Pale pink indicates the period after the onset of the pandemic. The broken line indicates the baseline.
Among all age/sex groups, the NOV for follow-up visits for mental health services was strongly and negatively impacted during the SOE (Fig. 3), although the magnitude of this impact was small compared to the effect of the SOE on initial mental health visits. Similar to the effects on the NOV for health care services in May 2020, the negative impact on the NOV for follow-up visits for mental health services in May 2020 was larger among boys and adolescent males (− 22.2%) and girls and adolescent females (− 22.3%) as compared to adult males (− 6.3%) and adult females (− 12.3%). Additionally, after the second outbreak of COVID-19 in Japan, the NOV for follow-up visits for mental health services in December 2020 increased among girls and adolescent females, although not strongly (8.7%; 95% BCI, − 1.5–18.8%).

The impact of the COVID-19 pandemic on the number of follow-up visits for mental health services, by sex and age group. Pale pink indicates the period after the onset of the pandemic. The broken line indicates the baseline.
Average incurred medical expenses
The impact of the COVID-19 pandemic on AIE for health care services is depicted in Supplementary Figure S9. During the SOE, a strong positive impact was seen among boys and adolescent males (8.5%; 95% BCI, 3.5–13.5%) and adult females (8.2%; 95% BCI, 3.1–13.1%).
Throughout the entire period of the study, there was no evidence of a strong impact of the pandemic and SOE on AIE for initial visits for mental health services, except among girls and adolescent females; in this group, the AIE for initial mental health services was most positively impacted in September 2020 (29.9%; 95% BCI, 2.5–58.4%), after the second outbreak of COVID-19 (Fig. 4). The impact of the pandemic on AIE for follow-up visits for mental health services was not strong among any of the age/sex groups during the study period (Fig. 5).

The impact of the COVID-19 pandemic on average incurred expenses for initial visits for mental health services, by sex and age group. Pale pink indicates the period after the onset of the pandemic. The broken line indicates the baseline.
82

The impact of the COVID-19 pandemic on average incurred expenses for follow-up visits for mental health services, by sex and age group. Pale pink indicates the period after the onset of the pandemic. The broken line indicates the baseline.
Discussion
This study aimed to examine the impact of the COVID-19 pandemic and SOE on the utilization of mental health services among children and adolescents in Japan. We performed an interrupted time series analysis using Japanese medical claims data stratified by sex and age group. The results of this analysis yielded several important findings. We found that the NOV for health care services and mental health services decreased during the SOE, with similar findings across age/sex groups. Moreover, after the second wave of COVID-19 cases, there was an increase in the NOV and AIE for initial visits for mental health services among girls and adolescent females.
The NOV for health care services and mental health services declined significantly during the SOE (April to May 2022), with a particularly large negative impact among young people. A systematic review based on 81 studies across 20 countries identified a significant decrease in health care service visits that was due to the COVID-19 pandemic (− 42.3%; IQR, − 52.8% to − 31.5%), although there was a large degree of heterogeneity across the studies13. By contrast, in our study, the decrease in the NOV for health care services during the SOE (− 20.7%) was relatively small, even in the month with the largest decrease (May 2020). These findings may be explained by the facts that the SOEs implemented in Japan were noncompulsory and modest, and the government recommended proceeding with visits to medical institutions if necessary.
In each age/sex group, the decrease in the NOV for initial visits for mental health services during the SOE was larger than that for health care services, whereas the decrease in the NOV for the follow-up visits for mental health service was smaller than that for health care services. This finding suggests that although patients previously diagnosed with mental disorders were less likely to refrain from visiting medical services, potential patients with mental disorders were more likely to refrain from accessing medical services during the SOE, suggesting that the provision of mental health care that could have reduced foregone care among potential patients may have been insufficient during this period.
In Japan, where mental health care is primarily provided by psychiatric specialists rather than primary care physicians, having a usual source of primary care has been identified as a contributor to maintaining opportunities for medical consultation during the COVID-19 pandemic, although these reports indicated that the rate of uptake for screening for mental disorders was very low during this period22. Meanwhile, studies from countries other than Japan have found that patients’ satisfaction with telehealth services for mental health treatment during the pandemic was comparable to levels of satisfaction with face-to-face and telephonic treatment23,24. Furthermore, studies have suggested that replacing face-to-face care with telehealth services has mitigated the reduction in consultation opportunities during the pandemic25 and that implementing telehealth for mental health services may have reduced overall medical costs, including costs associated with non–mental health diseases26. Therefore, enhancing telehealth capacity for mental health services in primary care in Japan could contribute to early detection and treatment of mental disorders, potentially leading to improved health care access and cost containment, not only during pandemics. This approach has strong potential to improve access for groups such as young people and those living in remote areas who may not have received adequate care through traditional face-to-face consultations. In the future, it will be important to develop a system of telehealth mental health services that is suitable for Japan’s health care system, to verify the effectiveness and safety of this new approach to mental health services, and to introduce it gradually. Simultaneously, it is necessary to promote the environment required to expand the scope of telemedicine, including education and technical support for health care providers and improving patients’ digital literacy.
After the second outbreak of COVID-19 in Japan, the impact of the pandemic on AIE for health care services and follow-up visits for mental health services was limited; whereas, both the NOV and AIE for initial visits for mental health services increased among girls and adolescent females. This finding suggests that the COVID-19 pandemic contributed to a deterioration in the mental health of girls and adolescent females, consistent with prior reports3,4,6,7,8,9,10. Several factors may have contributed to this deterioration. First, the economic impact of the pandemic was particularly pronounced in industries with high proportions of women workers, with more severe employment losses among women1. Ueda et al. also reported a surge in suicides among young women in October 2020, finding that young women workers were more likely to experience job and income loss than any other demographic group, suggesting economic factors may have contributed to mental health deterioration28. Second, Ueda et al. noted education-related factors, including loss of educational opportunities and anxiety about graduation and future prospects28. During the pandemic, school-age children and adolescents experienced mandatory home confinement lasting approximately 3 months until the SOE was lifted in late May. According to a survey administered in June and July 2020, approximately 72% of the participants exhibited symptoms of psychological distress, indicating that the extended period of school closures potentially had adverse effects on students’ mental health28. For university students in particular, the shift to online classes beginning in April 2020 and continuing through both spring and fall semesters resulted in an isolated learning environment without in-person campus activities, potentially leading to accumulated stress. Their online survey also reported that 29.41% of university students were classified as being in a depressive state28. These findings from multiple studies in Japan suggest that the pandemic had substantial effects on mental health among adolescents and young adults, as evidenced by the increased utilization of mental health services in this demographic group. In addition to being a young woman, other risk factors for worsening mental health during the pandemic included COVID-19 infection status, a high level of fear associated with COVID-19, and low socioeconomic status2,3,5,6,9. Pierce et al. identified 2 patterns in the chronology of deteriorating mental health during the pandemic: one in which mental health declines in immediate response to the pandemic and the another in which mental health deteriorates gradually27. During the first COVID-19 outbreak in Japan, the government granted cash benefits to each individual citizen, and the daily number of cases of COVID-19 was not yet particularly high1. Thus, a significant negative impact on mental health may not have existed at that time. Later during the pandemic, however, several factors may have contributed to cumulative stress: the increased risk of infection during the second outbreak, the prolonged nature of the pandemic itself, and the termination of government cash benefits amid a worsening economy. For school-age children and adolescents, while schools had shifted to remote learning during the first COVID-19 outbreak, the subsequent transition back to in-person schooling may have presented additional challenges, such as difficulties in rebuilding relationships with teachers and peers, and anxiety about returning to school29. For university students, the continued isolated learning environment through online classes may have further contributed to accumulated stress28. Furthermore, the number of COVID-19 cases temporarily decreased after the second outbreak, possibly facilitating access to health care for patients who had been refraining from obtaining medical services. As a result of the combined effects of these factors, the increased NOV and AIE among girls and adolescent females may have finally become apparent after the second wave of COVID-19. The suicide rate in Japan decreased during the initial outbreak of COVID-19, relative to before the pandemic, but increased in the second outbreak, with the increased rate of suicide being most pronounced among young women1,28. Notably, in our study, while the AIE did not show significant changes during the initial outbreak, suggesting that severe mental health deterioration had not yet progressed at this point, it increased substantially in the later phase of the pandemic. This temporal pattern of AIE may be attributed to two factors: the potential progression of symptoms due to delayed appropriate medical visits during the early pandemic, and the gradual deterioration of mental health due to the prolonged nature of the pandemic. Our study suggests that the mental health of girls and adolescent females deteriorated after the second outbreak, which would be consistent with the findings of prior studies on elevated suicide rates1,28. Therefore, early detection and treatment of patients with potential mental disorders is needed to prevent increased suicides during a pandemic. Among vulnerable groups, particularly girls and adolescent females, more proactive screening and enhanced support systems could be beneficial. Additionally, it is important to establish systems for providing continuous care that is accessible even under pandemic conditions, for example by utilizing telemedicine and collaborating with local communities through training community volunteers to identify high-risk patients, provide psychological first aid, and coordinate between caregivers and mental health professionals29. In this context, Japan has been developing the Disaster Psychiatric Assistance Team (DPAT) system to provide comprehensive mental health support during emergencies, including pandemics30. Our findings suggest critical areas where DPAT’s functions could be enhanced: maintaining access to mental health services during the initial phase of a pandemic, developing targeted support strategies for vulnerable populations (particularly young women), and ensuring continuity of care for patients with mental disorders. These insights could contribute to building a more resilient mental healthcare system for future crises. Through such measures, it may be possible to minimize the adverse effects of a pandemic on mental health and to contribute to suicide prevention. Further research is needed to evaluate the effectiveness of these strategies in various pandemic-related contexts.
To the best of our knowledge, this is the first study in Japan to analyze the impact of the COVID-19 pandemic on the utilization of mental health services among children and adolescents, using a large cohort of over 3,000,000 individuals. Moreover, the study estimated counterfactual time series using a BSTS model and robustly analyzed the longitudinal impact of the COVID-19 pandemic. This study has several limitations. First, the data used in the study only included individuals enrolled in health insurance societies and thus is not representative of the entire population in Japan. Second, the database used in this study only contained data up to December 2020; therefore, the study could not assess the long-term impact of the pandemic on the outcomes of interest. Third, previous studies have suggested that demographic and socioeconomic factors are associated with mental health outcomes during the pandemic1,2,4,27,28,31,32. However, our analysis could only stratify by sex and age due to data limitations and sample size constraints. Further studies incorporating more detailed demographic and socioeconomic variables are necessary for a comprehensive assessment of the differential impacts of the pandemic across population subgroups. Fourth, the major deregulation and expansion of telemedicine in Japan in April 2020 might have affected mental health care utilization patterns. However, this influence was likely minimal, as the proportion of medical institutions providing telemedicine for initial visits temporarily increased from 0.72 to 1.18% immediately after its implementation but subsequently decreased to 0.64% by October 2020, returning to pre-pandemic levels33. Moreover, in-person continuity of care for mental health services was maintained for initial visits requiring the prescription of psychotropic medications as Japanese regulations prohibited the prescription of psychotropic medications through telemedicine for initial visit patients. Finally, although the Japanese government actively encouraged medical service utilization during the SOE, changes in psychiatric care delivery systems and mental health specialist availability during the pandemic might have had some slight influence on our findings.
Conclusion
The findings of this study suggest that the provision of mental health care services for potential patients was insufficient during the COVID-19 pandemic in Japan. Furthermore, the findings suggest that mental health among the population was deteriorating during this time, especially among girls and adolescent females. During a pandemic, it is necessary to improve the mental health care system for providing early detection and treatment of potentially vulnerable new patients with mental disorders. The findings can inform the enhancement of emergency mental health support systems for future pandemic preparedness.
Data availability
JMDC provides fee-based access to its databases, which contain information from medical institutions that is maintained for the purpose of enabling use of the data for surveys, research, and commercial endeavors. Information about these databases can be obtained at the JMDÇ website (https://www.jmdc.co.jp/en/bigdata). Access to the data is granted upon completion of an agreement for the use of specific datasets.
References
Tanaka, T. & Okamoto, S. Increase in suicide following an initial decline during the COVID-19 pandemic in Japan. Nat. Hum. Behav. 5, 229–238 (2021).
Brooks, S. K. et al. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 395, 912–920 (2020).
Fernández, R. S., Crivelli, L., Guimet, N. M., Allegri, R. F. & Pedreira, M. E. Psychological distress associated with COVID-19 quarantine: Latent profile analysis, outcome prediction and mediation analysis. J. Affect. Disord. 277, 75–84 (2020).
González-Sanguino, C. et al. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain. Behav. Immun. 87, 172–176 (2020).
Liu, C. H., Zhang, E., Wong, G. T. F., Hyun, S. & Hahm, H. “Chris”. Factors associated with depression, anxiety, and PTSD symptomatology during the COVID-19 pandemic: Clinical implications for U.S. young adult mental health. Psychiatry Res. 290, 113172 (2020).
Luo, M., Guo, L., Yu, M., Jiang, W. & Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public—a systematic review and meta-analysis. Psychiatry Res. 291, 113190 (2020).
Pieh, C., Budimir, S. & Probst, T. The effect of age, gender, income, work, and physical activity on mental health during coronavirus disease (COVID-19) lockdown in Austria. J. Psychosom. Res. 136, 110186 (2020).
Ribeiro, F., Schröder, V. E., Krüger, R. & Leist, A. K. The evolution and social determinants of mental health during the first wave of the COVID-19 outbreak in Luxembourg. Psychiatry Res. 303, 114090 (2021).
Santomauro, D. F. et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 398, 1700–1712 (2021).
Thomas, D., Lawton, R., Brown, T. & Kranton, R. Prevalence, severity and distribution of depression and anxiety symptoms using observational data collected before and nine months into the COVID-19 pandemic. Lancet Reg. Health - Americas. 100009 https://doi.org/10.1016/j.lana.2021.100009 (2021).
Aoki, T. & Matsushima, M. The Ecology of Medical Care during the COVID-19 pandemic in Japan: A Nationwide Survey. J. GEN. INTERN. MED. 37, 1211–1217 (2022).
Carr, M. J. et al. Effects of the COVID-19 pandemic on primary care-recorded mental illness and self-harm episodes in the UK: A population-based cohort study. Lancet Public. Health. 6, e124–e135 (2021).
Moynihan, R. et al. Impact of COVID-19 pandemic on utilisation of healthcare services: A systematic review. BMJ Open. 11, e045343 (2021).
Ryu, S. et al. Decline in Hospital visits by patients with Schizophrenia Early in the COVID-19 outbreak in Korea. Clin. Psychopharmacol. Neurosci. 20, 185–189 (2022).
Farooq, S., Tunmore, J., Wajid Ali, M. & Ayub, M. Suicide, self-harm and suicidal ideation during COVID-19: A systematic review. Psychiatry Res. 306, 114228 (2021).
Gunnell, D. et al. Suicide risk and prevention during the COVID-19 pandemic. Lancet Psychiatry. 7, 468–471 (2020).
Isumi, A., Doi, S., Yamaoka, Y., Takahashi, K. & Fujiwara, T. Do suicide rates in children and adolescents change during school closure in Japan? The acute effect of the first wave of COVID-19 pandemic on child and adolescent mental health. Child Abuse Negl. 110, 104680 (2020).
Dubé, J. P., Smith, M. M., Sherry, S. B., Hewitt, P. L. & Stewart, S. H. Suicide behaviors during the COVID-19 pandemic: A meta-analysis of 54 studies. Psychiatry Res. 301, 113998 (2021).
Nagai, K. et al. Data resource profile: JMDC claims databases sourced from Medical Institutions. J. Gen. Fam Med. 21, 211–218 (2020).
Brodersen, K. H., Gallusser, F., Koehler, J., Remy, N. & Scott, S. L. Inferring causal impact using bayesian structural time-series models. Ann. Appl. Stat. 9, (2015).
Ke, Z. & Zhang, Z. (eds) (Johnny). Testing autocorrelation and partial autocorrelation: Asymptotic methods versus resampling techniques. Br. J. Math. Stat. Psychol. 71, 96–116 (2018).
Aoki, T., Fujinuma, Y. & Matsushima, M. Usual source of primary care and preventive care measures in the COVID-19 pandemic: A nationwide cross-sectional study in Japan. BMJ Open 12, e057418 (2022).
Benudis, A., Re’em, Y., Kanellopoulos, D., Moreno, A. & Zonana, J. Patient and provider experiences of telemental health during the COVID-19 pandemic in a New York City academic medical center. Psychiatry Res. 311, 114496 (2022).
Zimmerman, M., Benjamin, I., Tirpak, J. W. & D’Avanzato, C. Patient satisfaction with partial hospital telehealth treatment during the COVID-19 pandemic: Comparison to in-person treatment. Psychiatry Res. 301, 113966 (2021).
Hansen, J. P., Sas, T. Q. B., Fløjstrup, M., Brabrand, M. & Hvolby, A. The effect of the March 2020 COVID-19 lockdown on national psychiatric contacts in Denmark: An interrupted time series analysis. Brain Behav. brb3.2264 https://doi.org/10.1002/brb3.2264 (2021).
Zhang, Y. et al. Disparities and medical expenditure implications in pediatric tele-mental health services during the COVID-19 pandemic in Mississippi. J. Behav. Health Serv. Res. https://doi.org/10.1007/s11414-024-09906-2 (2024).
Pierce, M. et al. Mental health responses to the COVID-19 pandemic: A latent class trajectory analysis using longitudinal UK data. Lancet Psychiatry. S2215036621001516 https://doi.org/10.1016/S2215-0366(21)00151-6 (2021).
Ueda, M., Nordström, R. & Matsubayashi, T. Suicide and mental health during the COVID-19 pandemic in Japan. J. Public. Health fdab. 113. https://doi.org/10.1093/pubmed/fdab113 (2021).
Singh, S. et al. Impact of COVID-19 and lockdown on mental health of children and adolescents: A narrative review with recommendations. Psychiatry Res. 293, 113429 (2020).
Ministry of Health. Labour and Welfare, Japan. Guidelines for Disaster Psychiatric Assistance Team (DPAT) Activities. https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000164413.html. [in Japanese].
Stickley, A. & Ueda, M. Loneliness in Japan during the COVID-19 pandemic: Prevalence, correlates and association with mental health. Psychiatry Res. 307, 114318 (2022).
Penner, F. et al. Racial and demographic disparities in emergency department utilization for mental health concerns before and during the COVID-19 pandemic. Psychiatry Res. 310, 114442 (2022).
Ministry of Health. Labour and Welfare, Japan. Guidelines for Telemedicine Services During the COVID-19 Pandemic. https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/kenkou_iryou/iryou/rinsyo/index_00014.html. [in Japanese].
Acknowledgements
We would like to thank Professor Furui for his support in this project.
Author information
Authors and Affiliations
Contributions
Fumihiro Endo: conception, design of the work, data analysis, interpretation of data, manuscript review; Yuji Hiramatsu: conception, design of the work, data analysis, interpretation of data, manuscript writing, manuscript review; Hiroo Ide: manuscript review.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Endo, F., Hiramatsu, Y. & Ide, H. Impact of the COVID-19 pandemic on utilization of mental health services among children and adolescents using an interrupted time series analysis. Sci Rep 15, 2411 (2025). https://doi.org/10.1038/s41598-025-87072-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-87072-x
