
Abstract
Medicinal plants hold immense potential for drug discovery, with indigenous knowledge being crucial for their identification and utilization. This study investigated medicinal plant use in rural communities of Lar, Gerash, and Lamerd counties, southern Iran. A total of 200 respondents from three ethnic groups in 27 local communities were interviewed over a two-year period (2020–2022) and the data was analyzed using the ethnobotanyR package in R software. Quantitative ethnobotanical indices including (FC), (FL), (RFC), (ICF), (UR), (UV), (CI), (CVs), (CV), (FUV), and (PPV) were calculated. The conservation status of the plants was assessed based on the IUCN Red List. A total of 171 plant species from 53 families were documented, with Lamiaceae and Fabaceae being the most common. Leaves were the most utilized plant part in the preparation of medicines. Decoction was the most prevalent method of preparation, and oral administration was the most common route of consumption. Gastrointestinal diseases have the highest ICF value. Notably, the study documented new medicinal applications for 70 plant species, expanding the region’s ethnobotanical knowledge. The study highlights the need for documenting and disseminating traditional knowledge, as it provides fundamental data for further research and conservation efforts.
Similar content being viewed by others
Introduction
Plants form the foundation of traditional medicine, offering a safe, biocompatible, and cost-effective approach to treating various diseases1,2. Ethnobotanical studies, which document the traditional knowledge of medicinal plant use, are essential for new drug discovery and for understanding the relationship between biodiversity and cultural practices3,4. Preserving this traditional knowledge is essential for future medical progress and safeguarding cultural heritage5.
Scientific literature consistently highlights the significant reliance on traditional medicine in African and Asian countries, with 80% of their populations utilizing it for health care needs6. Iran, a developing country with a wealth of valuable plant resources, has a long-standing tradition of incorporating medicinal plants into its health care system7. Iran boasts remarkable biodiversity, with approximately 8,000 plant species, of which 2,300 possess medicinal properties. Notably, 75% (1,728) of these medicinal plants are native to Iran8. Historically, Iranian herbalists (attars) and physicians emphasized the importance of herbal therapy in treatments. The renowned physician, Hakim Bu Ali Sina (980–1037 AD), a prominent figure in traditional medicine, extensively utilized medicinal plants. His influential medical text, “The Canon of Medicine,” documented 800 herbal medicines and their properties, including single-plant and multi-plant remedies. The use of medicinal plants in Iran predates the Islamic period, with roots tracing back to the Babylonian-Assyrian civilization7. This ancient heritage reflects the accumulated knowledge of generations who sought beneficial herbs to enhance health9. Plants continue to be relevant in contemporary health care systems, complementing modern medical practices10. In addition to the high plant diversity based on the diverse climate and topography, the cultural and ethnic diversity of Iran with seven main languages (Persian, Azeri, Balochi, Kurdish, Arabic, Turkmen, Lori) and many smaller tribes, has created a huge wealth of indigenous ethnobotanical and ethnopharmacological knowledge7. Even with the widespread availability of modern medicines, a substantial portion of Iran’s rural population continues to rely on herbal and indigenous remedies9.
In recent decades, ethnobotanical and pharmacological studies have been increasing in order to preserve indigenous knowledge and discover new drugs, including7,8,9,11,12,13,14in Iran and1,2,3,4,15,16,17,18,19,20,21,22,23,24,25,26around the world.
Two primary medical systems are prevalent in Iran. Firstly, there is the Islamic traditional medicine system, an ancient and rational school with well-documented sources and a clear historical background. Traditional medicine operates on precise principles of health and disease. Secondly, there is the folk medicine system, where various ethnic groups in Iran, such as Turks, Lurs, Kurds, Arabs, Balochis, and Turkmen, provide health care services based on their community’s culture, religion, knowledge, attitudes, and beliefs. Iranian folklore medicine is not a documented medical system, and its definitions of health and disease may vary among different ethnic groups in Iran. Therefore, one of the main challenges in this field is documenting the valuable knowledge of Persian folklore in the field of medicine6,13.
Rural communities possess a wealth of knowledge about medicinal plants. Traditional remedies derived from these plants are often simpler to prepare than pharmaceuticals produced through complex chemical processes. Rural populations favor medicinal plants due to their accessibility, digestibility, general lack of side effects, and cost-effectiveness compared to expensive pharmaceutical drugs. These preferences stem from intergenerational knowledge transfer, trust in herbal remedies’ efficacy, and a deep understanding of the local health care system. Consequently, rural communities continue to rely on traditional medicine1,21,27,28. However, modernization, migration, education, and socioeconomic shifts can impact the preservation of traditional knowledge28. Despite the growing global demand for medicinal plants, traditional knowledge, particularly in developing countries, is rapidly eroding29. Furthermore, local climate change patterns, such as reduced rainfall and increased summer temperatures, threaten vital traditional plant species30.
Ethnobotanical studies are crucial to understanding traditional ecological knowledge as a link between ecosystem services and human well-being31. Research has identified various useful plants, including those used for medicine, food, and crafts. However, plant use varies among individuals, reflecting diverse cultural identities32. Knowledge of medicinal plants can foster environmental awareness and address future human health challenges. Further research is needed to validate the efficacy of these plants33. This study presents the first comprehensive ethnobotanical investigation of medicinal plants used by rural communities in Lar, Gerash, and Lamerd counties, southern Iran.
Materials and methods
Study area
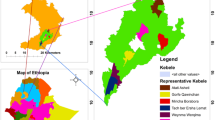
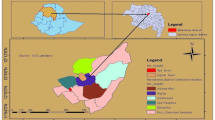
The study area is located between 53°22’4.41” to 53°49’12.98” East longitude and 27°30’58.63” to 27°35’36.12” North latitude, which covers an area of 880 square kilometers in Larestan, Gerash and Lamerd counties in Fars province (Fig. 1). The maximum height of the study area is 1553 m and the minimum height is 458 m and the average height of the range is 630 m above sea level.

Map of Iran showing the study area in Fars province (Larestan, Gerash, and Lamerd counties). Map was generated using QGIS 3.38.2 (https://www.qgis.org).
The average annual rainfall in this region is 206.24 mm, mainly from late November to early April. The average annual temperature is 24.6 ° C. The warmest month of the year is July with an average temperature of 35.18 ° C and the coldest month of the year is January with an average temperature of 13.27 ° C34.
In natural conditions prevailing in dry regions, it is not possible to witness the expansion of all types of plant species. Mostly in these areas, natural vegetation is scattered and includes annual plants, perennial grasses, other herbaceous plants, shrubs, and small trees. Annual rainfall fluctuations in dry regions are severe. In dry areas, considering that the main limitation for the growth and sustainability of plants is moisture, and in the climatic conditions of these areas, typically, drought-tolerant plants are capable of growth and survival, requiring less water. Therefore, even the slightest change in climatic conditions or the growing medium that improves available moisture will increase the percentage of plant canopy coverage and the number of plant species35. Most native plant species are ephemerals and appear after the rainy season in winter and spring36. Dominant perennial species in the flora include Calotropis procera, Capparis spinosa, Seidlitzia rosmarinus, Ephedra pachyclada, Prosopis stephaniana, Phoenix dactylifera, Astragalus fasciculifolius, Ziziphus nummularia, Prunus scoparia, and others37.
The Bikhayi, Achomi, Korosh, and a limited number of Tork ethnic groups reside in this region. The first group in the studied area reside in the villages of Lamerd County includes Na’ama, Dehno, Dehban, Chahvarz, Chah-Chahvarz, and parts of Laristan County, such as Lavarestan, Joozaghdan, Pohrost Oliya, Pohrost Sofla, Kirishki, Najafabad, Husseinabad, Kamalabad, Aliabad, Mohammad Ghasemi, Deh-Kohneh, Beyram, and Baladeh. They speak the Bikhayi dialect, and due to slight differences between villages, this dialect is further categorized into smaller sub-dialects such as Beyrami Baladehi, Chahvarzi, and others. The Lari or Achomi people primarily reside in Fedagh and Dideban areas of the region and speak the Achomi language and Fedaghi dialect. The third group, known as the Korosh, originate from the southeast, specifically from Baluchistan. They are mainly livestock farmers and have also engaged in agriculture in the past few decades. They reside in the villages of Bashirabad, Lab-eshkan, Husseinabad, Heydarabad, Mohammadzaina, Okoshi, Kong-o Risheh, and Kalat Kordshir in Gherash and Laristan counties. They speak the Koroshi dialect. Although the people in this region share close bonds among themselves, these three ethnic groups have their own unique dialect, traditional customs, arts, and culture38.
The residents of these areas are predominantly Muslims who uphold traditional Islamic values. The majority of adults possess limited literacy, with most having elementary-level education or less. Agriculture and livestock farming constitute the primary occupations in this region. Date palm cultivation holds significant cultural and economic importance, a common practice in many desert regions. However, there is a noticeable shift towards commercial, administrative, and service-oriented jobs. The population in this region often migrates to larger cities seeking better employment prospects, higher education opportunities, or to escape the challenges of drought and harsh weather conditions39.
Data collection
This study was conducted in 27 villages across Laristan, Gerash, and Lamerd counties to document ethnic information related to medicinal plant use. The villages included Okoshi, Abkaneh, Baladeh, Bashirabad, Beyram, Pohrost Oliya, Pohrost Sofla, Joozaghdan, Chah Chahvarz, Chahvarz, Husseinabad-e-Gerash, Husseinabad-e-Laristan, Heydarabad, Aliabad, Kamalabad, Dehban, Dehno, Didehban, Fedagh, Kirishki, Kalat Kordshir, Lavarestan, Labeshkan, Mohammad Ghasemi, Mohammadzina, Najafabad, and Na’ama in the outskirts of these counties. Data collection took place between 2020 and 2022. As a first step, we prepared a questionnaire to identify and determine the uses of commonly used medicinal plants in the region’s traditional and indigenous medicine. The questionnaire covered various aspects, including the local and Persian names of the plant, habitat, used parts, harvesting time, medicinal uses, contraindications, preparation methods, consumption methods, side effects, changes in natural resources, and the plant’s extinction status. Furthermore, we recorded supplementary information, such as traditional instructions for combining plants with other products or details about plant toxicity, whenever available. We also documented the use of non-plant substances as medicine40. To gather this information, we conducted face-to-face interviews with native individuals, primarily experienced elders, in each region. Leveraging our familiarity with local dialects and with the assistance of knowledgeable local individuals, we conducted all interviews in the local language. Interviews were conducted individually with each respondent, and occasionally in group discussions. We recorded the responses in both audio and written formats. This research involved an ethnobotanical study including interviews with human participants. According to the guidelines of Shiraz University, this type of research, which focuses on traditional plant use for common ailments, does not require formal ethics committee review, as it involves non-sensitive topics and poses minimal risk to participants. However, informed consent was obtained from all participants before their involvement in the study. The study adhered to the ethical principles outlined in the Declaration of Helsinki and was conducted with respect for the cultural traditions and knowledge of the participating communities.
We established specific criteria for selecting interviewees from the ethnic groups residing in the study area. These criteria included: (1) The interviewee should have sufficient knowledge of the traditional uses of plants in the region. (2) The interviewee should express a willingness and interest in sharing their knowledge and experience. (3) The interviewee should be a permanent resident of the region30. We employed a non-probability sampling method known as “snowball sampling.”41This method involved identifying an initial interviewee and then requesting referrals to other knowledgeable individuals within the same community. This process continued until we had identified and interviewed all potential interviewees40. Snowball sampling is suitable for quantitative ethnobotanical exploratory studies40,42. Based on this sampling approach, we selected key informants based on their knowledge and standing within their communities43. The interviewees consisted of villagers, farmers, shepherds, and herbalists, with the majority being housewives who had extensive experience with native plants1.
To gather data for this study, field visits were conducted to compile a floristic list, collect plant specimens, verify questionnaire information, and take photographs. We prioritized field trips accompanied by local people. Throughout the research period, 90 field trips were conducted, with 48 days fully dedicated to collecting information on the medicinal values of plants alongside the local communities.
All collected plant specimens were pressed, dried, and mounted on herbarium sheets. The identification of plant specimens was based on morphological characteristics of fruits, flowers, leaves, stems, etc., using reliable sources such as “Identification of Medicinal and Aromatic Plants of Iran” and “Dictionary of Iranian Plant Names”, the Flora of Lamerd37,44,45. If necessary, the online database of the International Plant Names Index46 was used to confirm the identification. After identification, all plant specimens were deposited in the herbarium of the Fars Agricultural and Natural Resources Research and Education Center.
We determined the plant families and classification of all species, as well as their habitat priority, using the World Flora Online47and the Plants of the World Online database48. (Accessed in 2022).
We assessed the conservation status of each plant based on the IUCN Red List of Threatened Species49 (Accessed in 2022).
Classification of diseases
We organized and classified all reported uses of medicinal plants and the diseases they treat based on the International Classification of Primary Care50. This classification resulted in 16 disease groups: (1) General and unspecified, (2) Blood, blood-forming organs, and immune mechanisms, (3) Digestive, (4) Eye, (5) Ear, (6) Circulatory, (7) Musculoskeletal, (8) Neurological, (9) Psychological, (10) Respiratory, (11) Skin, (12) Endocrine, metabolic and nutritional, (13) Urinary system, (14) Pregnancy, childbearing, family planning, (15) Female genital system (including breast), (16) Male genital system. Cancer was categorized as a general disease within the first group.
Data analysis
Documenting and analyzing indigenous knowledge about plant resources is crucial for understanding traditional lifestyles and evaluating medicinal plants’ value. Various ethnobotanical indices were used to quantify plant use for food, health care, veterinary medicine, and economic benefits51,52. The Use Value (UV) measures the importance of a plant to a specific group53, while the Frequency Citation (FC) counts how often a species is mentioned54. The Fidelity Level (FL) indicates the percentage of informants using a plant for a specific purpose, with higher values suggesting greater consensus on its use for treating a particular disease52,55. The Relative Frequency of Citation (RFC), reflects the local importance of each species56. The Informant Consensus Factor (ICF) measures agreement among informants on plant use for particular ailments, with higher values indicating stronger consensus57,58. The Cultural Importance Index (CI) and Cultural Value Index (CVs) assess not only the prevalence of use but also the diversity of applications for each species56,59. Choice Value (CV) determines preferred species for each use category60, and Family Use Value (FUV) identifies key medicinal plant families. Plant Part Value (PPV) highlights the most commonly used plant parts61. The Jaccard Index (JI) compares documented data with previously published data collected from a neighboring area19. It identifies species composition, overlap, and similarities in plant uses51. Data were organized in MS-Excel and analyzed using the ethnobotanyR package in R. This package calculates the mentioned indices to assess the cultural importance of plant species based on informant consensus62.
Results
The age range of the informants was between 40 and 90 years, with an average age of 66 years. The gender distribution was 18.5% male and 81.5% female. On average, each person mentioned 22 plant species (minimum 5 and maximum 92). Men reported fewer plant species (average of 20 species per person) compared to women (24 species). However, in the age range of 61–81 years, the average number of species mentioned by men and women was equal at 25 species (Fig. 2).

Characteristics of informants: the average number of species reported by men (gray) and women (yellow).
Among the documented plant species, 4 were reported by only one informant, 25 by 2–5 individuals, 22 by 6–10 individuals, and 102 by 11–98 individuals. Additionally, 15 species were mentioned by more than 100 individuals, indicating a high level of consensus regarding these species and their uses.
The health of communities, particularly tribal groups, is influenced by various factors, including their way of life, socioeconomic conditions, age, beliefs, and socio-religious customs. This raises the question of whether there is a relationship between the knowledge of medicinal plants reported by informants and social factors such as gender, age, and geographical characteristics63. Women often play a primary role in health care and medicinal plant collection within these communities. They also tend to possess a deeper understanding of traditions across all age groups compared to men. Furthermore, individuals residing in remote areas, further from urban centers, tend to rely more on medicinal plants for their daily health care needs compared to those living closer to urban areas.
The majority of interviewees were from the Bikhei ethnic group (134 individuals), with 37 Koreish and 29 Achomi speakers also participating. Some participants were Tork migrants who had settled in the area after marriage and were considered part of their respective ethnic groups due to their permanent residency (Table 1). Most informants were illiterate, with a few having secondary-level education or higher.
Men listed 136 plants (from 45 families), and women listed 168 plants (from 51 families). There were 133 medicinal plants common to both lists. Men solely listed 3 medicinal plants, while women solely listed 35.
In total, 171 plant species were identified, belonging to 53 families, including 12 unidentified species. Of these, 5 belong to monocots, 46 to dicots, one family to gymnosperms, and one family to pteridophytes (Fig. 3 All recorded plant species are listed alphabetically by family, along with their scientific name, Persian name, local name, habit, habitat, species nature, accessibility, and IUCN Red List status (Supplementary Table 1). Plant species identified only to the genus level are coded as A, B, and C. For example, some species of the genus Allium are coded in this way. Additionally, due to reported different properties for subspecies of Teucrium polium L. and the inability to accurately identify these subspecies, they were also coded as A, B, and C.

Types of plant species.
The majority of plant species (60%) were sourced from wild habitats, while 22% were imported from abroad or other provinces within Iran. Additionally, 18% of the species were cultivated within the region. This highlights the community’s preference for wild plants and their availability in the area.
Lamiaceae, Fabaceae, Asteraceae, and Apiaceae were the most commonly used plant families in the study area (Fig. 4). The therapeutic importance of these families may be related to the widespread distribution of their species in the region38. The common use of these medicinal families has also been reported in previous studies in Iran7,8,9,10,13,64,65.

Families having high number of species.
Due to the limitations imposed by the COVID-19 pandemic, drought conditions, and the inability of some local people to accompany the researcher in the field, it was not possible to collect all of the plant samples, including the plants listed in Table 2.
This study found that 156 plant species (91% of the total) had reported medicinal uses. Of these, 126 species were reportedly used to treat multiple diseases, while 30 species were used for a single disease. For instance, Astragalus fasciculifolius Boiss. was used for gastrointestinal, ocular, musculoskeletal, respiratory, dermatological, metabolic, nutritional, and urinary system disorders, while Ocimum basilicum L. was solely used for relieving joint pain.
The most common medical conditions treated with local herbal remedies include gastrointestinal disorders, dermatological problems, muscular and joint pain, as well as issues related to pregnancy, fertility, family planning, and respiratory ailments.
This study also revealed that some plants are prepared in various ways for different medicinal purposes. For example, the decoction of Alhagi mannifera Jaub. & Spach is used for body wash and to treat conditions such as psoriasis, eczema, and rheumatism. The plant distillate is used to alleviate kidney pain, while its extract is employed for treating gastrointestinal issues. Interviewees frequently stated that certain plants, such as Teucrium polium L. (B), Artemisia sieberi Besser, and Suaeda fruticosa Forssk. ex J.F.Gmel, are considered “good for any health problem” and are used for a wide range of ailments (Supplementary Table 2).
Out of the total collected plant species, 59 plants are used for the treatment of general and unspecified diseases, 11 species for blood, blood-forming organs, and immune mechanisms, 106 species for gastrointestinal diseases, 19 plants for eye disorders, 14 plants for ear problems, 29 species for Circulatory, 76 plants for musculoskeletal issues, 22 plants for neurological conditions, 22 species for psychological, 66 plants for respiratory problems, 85 species for skin-related issues, 50 plant species for endocrine, metabolic, and nutritional disorders, 24 plants for urinary system diseases, 62 plants for pregnancy, childbearing, and family planning, 47 species for female genital system (including breast), and 5 plant species for male genital system.
The medicinal plants that are commonly used by almost all participants (highest FC) are as follows: Shirazi thyme (Zataria multiflora Boiss.), Kirishk-Azad (Teucrium polium L. (B)), and Salvia mirzayaniiRech.f. & Esfand. (Supplementary Table 3). These plants are primarily chosen due to their proven beneficial effects, easy accessibility, and, to a lesser extent, their association with the most common health problems and the abundance of related plants66.
The fidelity levels (FL) for human diseases in the study area varied from 0.55 to 100%. There are 52 cases with a fidelity level of 100%, which can be observed in Supplementary Table 4. For example, Aizoanthemopsis hispanica (L.) Klak is used for psychological disorders, Senna italica Mill. is used for gastrointestinal disorders, Hyparrhenia hirta (L.) Stapf is used for reproductive issues, Echinops sp. is used for respiratory problems, Ocimum basilicum L. is used for musculoskeletal problems, Poa trivialis L. is used for dermatological issues, and Zea mays L. is used for renal and urinary tract conditions. All of these plants have an FL of 100.
Almost all parts of plants, including leaves, roots, bark, fruits, seeds, and flowers, possess medicinal properties. The analysis of medicinal plant parts in the study area showed that the registered wild plant parts used by the local people include aerial parts (AP), fruits (F), flowers (FL), leaves (L), roots (R), resin (RE), seeds (S), stems (ST), bulbs (B), nuts (N), barks (Ba), whole plant (Wh), capsules (Cp), rhizomes (Rh), and frond (Fd) (Fig. 5). According to the Plant Part Value Index (PPV), the most commonly used plant parts for the treatment of human diseases are as follows: leaves (PPV = 0.247), seeds (PPV = 0.169), aerial parts (PPV = 0.153), fruits (PPV = 0.113), resin (PPV = 0.105), flowers (PPV = 0.088), roots (PPV = 0.048), stems (PPV = 0.035), and bulbs (PPV = 0.013).

Plant parts used for ethnomedicine.
The plant parts commonly used for the treatment of animal diseases include aerial parts (PPV = 0.242), fruits (PPV = 0.152), roots (PPV = 0.152), leaves (PPV = 0.121), seeds (PPV = 0.121), resin (PPV = 0.091), bark (PPV = 0.061), stems (PPV = 0.030), and the whole plant (PPV = 0.030). (Fig. 6).

Percentage of plant parts used for the treatment of livestock.
The most common methods of preparation include decoction (27%), infusion (17%), raw usage (12%), powder (10%), poultice (8%), crushing and heating (6%), mixing with milk, honey, sugar, local butter oil, egg yolk, date syrup, yogurt, salt, etc. (6%), burning (4%), cooking (3%), plant water (2%), distillate (2%), and topical application (1%). Boiling, oil, maceration, syrup, chewing, and steaming are among the other methods of utilizing plants (Fig. 7).

Percentage of different preparation methods of plant parts.
The preparation methods of animal medicines include decoction (31%), infusion (15%), pounding (15%), raw (13%), mixture (8%), oil (5%), poultice (5%), distillate (5%), roasted (3%), and syrup (3%) (Fig. 8).

Percentage of different preparation methods in veterinary.
We assessed all medicinal plants for their presence in the IUCN Red List. Out of the 171 plants studied, the Devil’s pomegranate (Tecomella undulata (Sm.) Seem.), an important native plant, is classified as Endangered (EN). The native plant Pistacia atlantica Desf. is listed as Near Threatened (NT). The introduced plant Eucalyptus camaldulensis Dehnh., used in green spaces and forestry, is also listed as Near Threatened (NT). Additionally, three imported plants, Boswellia sacra Fluck. (NT), Indian Bdellium (Commiphora wightii (Arn.) Bhandari) (CR), and Coffee (Coffea arabica L.) (EN), are included in the IUCN Red List.
We calculated the family use value (FUV) based on the total use value of plants in each family across all use categories, including medicinal, edible, forage, cosmetic, and handicrafts. Rhamnaceae had the highest FUV, followed by Cucurbitaceae, Palmaceae, Lamiaceae, Pedaliaceae, Anacardiaceae, Rutaceae, Capparidaceae, Asteraceae, Nitrariaceae, and Apiaceae. The other families had FUV values below 0.3 (Table 3).
Local communities have reported side effects associated with some medicinal plants, which emphasizes the importance of traditional knowledge in ensuring safe usage and preventing harm67. Therefore, medicinal plants should be used cautiously and subjected to toxicological research and safety measures. This research should aim to enhance the understanding of these plants and improve the preparation of plant-based remedies for communities. The toxicity of medicinal plants can vary based on several factors, including dosage, the potency of secondary metabolites, harvesting season, duration of exposure, climate and soil conditions, preparation methods, and the specific plant part used61.
Twelve species are used exclusively by the Achomi people, nine species by the Bikheii people, and five species by the Korosh people. 101 species (59%) are common to all three groups (Fig. 9).

Venn diagram showing the total number and overlapping species among the three tribes.
The study area is depicted in Fig. 10.

A view of the study area and medicinal plants.
To validate and compare the reported traditional botanical uses in our study regarding important plant species in the region, a comparison was made with 25 ethnobotanical studies published at local, national, and global levels. Due to significant cultural and geographical differences among indigenous communities, indigenous botanical knowledge varies greatly from one region to another. Documenting and comparing traditional knowledge for the discovery of new medicinal resources requires extensive research and considerable knowledge and wisdom. In this study, the percentage of similar plant uses ranged from 2 to 35%, while the percentage of dissimilar plant uses ranged from 1 to 16% (Supplementary Table 5).
New medicinal applications
To identify new medicinal applications of plants, a comparison was made with the “Identification of Medicinal and Aromatic Plants of Iran”45. Out of the plants studied, 87 species (51%) had similar uses to those reported in the book, while 55 species (32%) had different applications. The recorded ethnobotanical information of these 55 species was then compared with published works from Iran and neighboring countries in databases such as ScienceDirect, PubMed, ResearchGate, and Google Scholar. This comparison involved 70 articles, including 52 case studies and reviews within Iran7,8,9,11,14,64,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113and 18 studies from other countries19,21,22,25,30,36,38,39,57,58,114,115,116,117,118,119,120,121, primarily neighboring countries. New therapeutic applications of 70 species that were not previously mentioned in ethnobotanical texts have been documented (Supplementary Table 6).
Discussion
This study represents the first comprehensive documentation of traditional medicinal plant use in Garash, Laristan, and Lamerd counties. A comparison of our findings with local and global ethnobotanical studies revealed an important aspect of this research: the validation of traditional knowledge. Many of the documented medicinal plant uses were consistent with those reported in previous studies, supporting the efficacy and cultural significance of these practices. Furthermore, this study led to the documentation of new medicinal applications for 70 plant species. This discovery highlights the potential of ethnobotanical research to uncover novel uses for plants, even those previously studied, and emphasizes the importance of preserving traditional knowledge systems that may hold untapped therapeutic potential.
Women were found to have more extensive knowledge of medicinal plants than men. This is likely due to their roles as caregivers and food preparers. A similar trend has been observed in studies on medicinal plant use in Jeddah, Saudi Arabia. This highlights the importance of considering gender roles in ethnopharmacological research116.
The study identified 53 plant families, with Fabaceae and Lamiaceae being the most common. Rhamnaceae had the highest Family Use Value, indicating its importance in traditional medicine.
Zataria multiflora Boiss. was the most valued plant for treating gastrointestinal diseases, based on various ethnobotanical indices.
Gastrointestinal disorders were the most common health issue addressed with medicinal plants (ICF = 0.95). These issues are prevalent in the region. People often seek immediate relief, which encourages the widespread use of local plants for these conditions39,122.
People preferred highland medicinal plants over lowland varieties, believing them to be more potent. For example, Teucrium species from mountainous areas were used for various ailments, while desert-dwelling Teucrium species were mainly for women’s health. This preference aligns with a study in Chitral, Pakistan117.
Different plant parts contain specific compounds with medicinal properties. Leaves are commonly used due to their ease of collection and their role in synthesizing secondary metabolites. This preference for leaves is supported by both traditional and scientific evidence52,63,114,123,124.
As shown in Supplementary Table 1, a significant portion of the medicinal plants used in this region are herbaceous. Compared to plants requiring specific parts like roots or bark, herbaceous plants are generally more suitable for sustainable cultivation and drug development125.
The primary methods for preparing herbal medicines were decoctions and infusions. Softer plant parts were typically infused, while harder parts were decocted to extract maximum bioactive compounds122. For example, the leaves of Ziziphus nummularia were infused, while the roots and gum were decocted. Oral administration was the most common method of delivering herbal remedies, surpassing topical application.
Dosage recommendations for similar diseases varied among informants in the studied region. This lack of standardization stems from the personalized nature of traditional medicine, where dosages are often determined based on factors like age, physical appearance, and individual responses to treatment. While this personalized approach may have benefits, it also introduces variability in treatment outcomes and raises concerns about potential side effects, especially when the precise active compounds and their concentrations in the plants are unknown126.
Despite the lack of standardized measurements, traditional healers possess a wealth of empirical knowledge passed down through generations, which includes information about safe dosages and potential side effects. This knowledge is often complemented by close observation of patients and adjustments in dosages based on individual responses. Additionally, the use of specific plant parts and traditional preparation methods (decoctions, infusions) contributes to ensuring safety.
However, the variability in plant composition due to factors like growing conditions and harvesting time can influence the concentration of active compounds, potentially affecting treatment outcomes. Moreover, individual sensitivities to these compounds can vary, making it difficult to predict responses to a given dosage. The absence of formal documentation of dosages and recorded side effects further adds to the challenges in ensuring safety and efficacy63.
Informants employed a variety of imprecise measurement methods, ranging from fingernail size to handfuls (“penj”), tablespoons, teaspoons, glasses, and small cups (estimated at 60 ml). Generally, children receive smaller doses than adults. For example, infants might be given a “chenko” (2–5 ml), while adults typically consume a glass (around 250 ml), or a small cup for potent medicines. Treatment durations also varied. Some remedies were prescribed once, twice, or three times daily until the patient improved, while others were given for a specific period (e.g., three days, one week). For instance, to alleviate jaundice, an infant is washed once with a decoction of Tecomella undulata (Sm.) Seem. leaves and flowers; this treatment is repeated only if the jaundice persists after 20 days due to its bitterness.
This lack of precision in dosage and treatment duration, coupled with the variability in plant composition and individual sensitivities, can lead to inconsistent results and potential side effects, hindering the wider acceptance of traditional medicine38,43. Many researchers have reported similar findings regarding the lack of standardized measurements in traditional practices21,38,40,43,58,63,126. Future research should prioritize standardizing dosages, identifying active compounds, and systematically documenting traditional knowledge to improve the safety and efficacy of these valuable medicinal resources.
Indigenous knowledge regarding medicinal plants is a dynamic “social product” embedded within specific cultural systems. This knowledge can vary significantly among different ethnic groups due to factors like location, altitude, urbanization level, gender, ethnicity, and age127.
In the studied region, a comparison of ethnobotanical knowledge revealed that while 101 plant species were used in common across the three main ethnic groups (Achomi, Bikheii, and Korosh), some species were unique to specific groups. The Achomi people utilized 12 unique species, the Bikheii people 9, and the Korosh people 5. This sharing of knowledge likely stems from intertribal exchange and communication in neighboring regions43.
Interestingly, even when different ethnic groups utilize the same plant species, variations are observed in the plant parts used, methods of preparation, and targeted ailments38. This diversity in medicinal plant use is not solely reflected in the variety of species used, but also in how those species are utilized. For example, the Korosh and Bikheii people consume the fresh leaves of Carthamus oxyacantha M. B. as a vegetable. In contrast, the Achomi people burn or dry the plant, grind it, mix it with cow’s butter or yogurt, and apply it topically to treat burns. Another example is Pulicaria aucheri Jaub. & Spach. The Bikheii people use a decoction of its aerial parts to wash old wounds and prevent infection. The Achomi people, however, boil this plant with Haplophyllum laristanicum C.C.Towns. to create a remedy for muscle pain.
Despite a significant overlap in the medicinal plant species utilized, this study reveals distinct variations in how these plants are prepared, applied, and for which ailments they are used across the three ethnic groups. This highlights the dynamic nature of traditional knowledge and its adaptation to specific cultural practices and environmental contexts.
Two plant species identified in this study, Tecomella undulata and Pistacia atlantica, are currently listed as threatened on the IUCN Red List. This designation underscores the urgent need for conservation efforts to address the threats these species face, including overharvesting, habitat loss, and climate change. Protecting these plants is crucial not only for maintaining ecological balance but also for preserving their economic value within local communities.
It is important to note that the relatively low number of endangered or vulnerable plant species identified in this study does not diminish the urgency for conservation action63. Several factors can contribute to this seeming discrepancy. Many plant species may not have been formally assessed for their conservation status. This is particularly true for those with restricted distributions or limited research. For example, the population of Ferula assa-foetidaBoiss., though not yet evaluated by the IUCN (listed as “NA” in Supplementary Table 1), is reportedly experiencing a severe decline due to unregulated harvesting. This highlights the need for a comprehensive assessment of its conservation status. Even for assessed species, data deficiency can hinder accurate categorization. This lack of information can mask the true extent of threats to certain species. Official conservation status listings may not immediately reflect the current population trends. A species may be experiencing significant decline even before it is officially classified as threatened52.
It is crucial to acknowledge the potential influence of climate change and drought on the availability and distribution of medicinal plants in the region. Changes in precipitation patterns and increased aridity may lead to shifts in plant communities, potentially affecting the abundance and accessibility of certain species. Future studies should investigate the long-term impacts of climate change on the region’s medicinal flora and incorporate this understanding into conservation strategies128,129.
Therefore, ongoing monitoring and research are essential to identify and protect vulnerable species, such as Otostegia persica (Burm.) Boiss., a valuable medicinal plant with potential conservation concerns. Future conservation efforts should prioritize developing sustainable harvesting practices, promoting cultivation techniques, and restoring degraded habitats to ensure the long-term survival of these vital plant resources.
this study revealed the highest similarity in medicinal plant use between our study region and other areas in Iran (Fasa and Kerman provinces)8,105and Saudi Arabia116. This similarity likely stems from shared cultural practices, linguistic connections, and similar ecological conditions that favor the growth of common medicinal species. Conversely, geographical barriers and reduced social exchange between our study region and more distant areas were associated with lower similarity in plant use51. This finding highlights the influence of both geographical proximity and cultural exchange on the transmission and evolution of traditional medicinal knowledge.
This study clearly demonstrates the direct reliance of local communities on native plants for fulfilling various basic needs, including medicine, food, fodder, and fuel. The examined area predominantly comprised herbaceous plants and shrubs, with a remarkable 91% of documented species utilized for medicinal purposes. Beyond medicinal applications, the most common uses included food (52%) and fodder (44%), followed by ethnoveterinary practices (18%), handicrafts (12%), cosmetics (10%), religious purposes (3%), and other miscellaneous applications (9%). This diverse utilization underscores the crucial role of native plants in supporting the livelihoods and cultural practices of the local population.
Multipurpose plants play a crucial role in the diversity of plant utilization within a region, serving as valuable indicators of biocultural diversity. In this study, plants with three distinct uses were most common, particularly those serving as sources of food, medicine, and fodder. Notably, some species exhibited even greater versatility. For instance, Prunus scoparia Spach is not only a source of food and medicine for both humans and livestock but also finds applications in cosmetics and handicraft production. Similarly, the date palm (Phoenix dactyliferaL.) provides food, medicine, and fodder, while also being utilized in handicrafts. Studies focusing on multipurpose plants contribute significantly to documenting traditional ecological knowledge at regional and ethnic levels, identifying potential applications for these versatile species, and promoting the conservation of biocultural diversity67.
This study had limitations regarding challenges in data collection, the potential for respondent bias, and difficulties in accurately identifying plant species. Due to the COVID-19 pandemic and drought conditions, some local people could not accompany the researcher in the field, and it was not possible to collect all the plant samples. In terms of respondent bias, some respondents may have provided information based on their beliefs or perceptions rather than actual experiences, potentially influencing the results. The study also faced challenges in accurately identifying plant species due to the lack of available taxonomic expertise and the presence of subspecies, potentially affecting the precision of the results. It is important to consider these limitations when interpreting the findings of this study.
Conclusion
This study provides valuable insights into the rich tradition of medicinal plant use in the southern Fars province, highlighting the deep connection between local communities and their natural environment. The documentation of 171 plant species, along with their diverse applications and associated traditional knowledge, contributes significantly to the growing body of ethnobotanical literature. However, several key areas require further investigation to fully understand and conserve this valuable biocultural heritage:
Species identification: Proper identification of the plant species that were not collected due to limitations is crucial to explore their potential medicinal properties and contribute to a comprehensive inventory of the region’s medicinal flora.
Subspecies of Teucrium polium L.: Given the documented variations in medicinal applications within Teucrium polium L., further research should investigate its subspecies and their distinct chemical profiles to understand the basis for these varied uses.
Phytochemical analysis: Traditional medicinal plants lacking a thorough assessment of their chemical constituents require phytochemical studies to validate their therapeutic potential and identify bioactive compounds. This is particularly important for species like Haplophyllum laristanicum C.C.Towns., a valuable native plant with promising medicinal applications.
By addressing these knowledge gaps, researchers can gain a more comprehensive understanding of the medicinal plant diversity in the region, contributing to the development of sustainable conservation strategies and potentially uncovering new sources of therapeutic agents. This study underscores the importance of integrating traditional ecological knowledge with scientific research to ensure the long-term preservation of both biological and cultural diversity.
Data availability
Data is provided within the manuscript.
Abbreviations
- FC:
-
Frequency Citation
- FL:
-
Fidelity Level
- ICF:
-
Informant Consensus Factor
- UR:
-
Use Reports
- UV:
-
Use Value
- CV:
-
Choice Value
- PP:
-
Plant Part
- FUV:
-
Family Use Value
- JI:
-
Jaccard Index
- A:
-
Achomi
- B:
-
Bikheii
- K:
-
Koroshi
- T:
-
Torki
- DD:
-
Data Deficient
- LC:
-
Least Concern
- NT:
-
Near threatened
- VU :
-
Vulnerable
- EN:
-
Endangered
- CR:
-
Critically Endangered
- NA:
-
Not Assessed
- D:
-
Difficult
- M:
-
Moderate
- E:
-
Easy
References
Shuaib, M. et al. Ethnobotanical and ecological assessment of plant resources at District Dir, Tehsil Timergara, Khyber Pakhtunkhwa, Pakistan. Acta Ecol. Sin. 39, 109–115 (2019).
Awan, A. A., Akhtar, T., Ahmed, M. J. & Murtaza, G. Quantitative ethnobotany of medicinal plants uses in the Jhelum Valley, Azad Kashmir, Pakistan. Acta Ecol. Sin. 41, 88–96 (2021).
Idm’Hand, E., Msanda, F. & Cherifi, K. Ethnobotanical study and biodiversity of medicinal plants used in the Tarfaya Province, Morocco. Acta Ecol. Sin. 40, 134–144 (2020).
Bahadur, S. et al. Traditional usage of medicinal plants among the local communities of Peshawar valley, Pakistan. Acta Ecol. Sin. 40, 1–29 (2020).
Mahwasane, S. T., Middleton, L. & Boaduo, N. An ethnobotanical survey of indigenous knowledge on medicinal plants used by the traditional healers of the Lwamondo area, Limpopo province, South Africa. South. Afr. J. Bot. 88, 69–75 (2013).
Tembo, N., Lampiao, F., Mwakikunga, A. & Chikowe, I. Ethnobotanical survey of medicinal plants used for cervical cancer management in Zomba District, Malawi. Sci. Afr. 13, e00941 (2021).
Hosseini, S. H., Sadeghi, Z., Hosseini, S. V. & Bussmann, R. W. Ethnopharmacological study of medicinal plants in Sarvabad, Kurdistan province, Iran. J. Ethnopharmacol. 288, 114985 (2022).
Hosseini, S. H., Bibak, H., Ghara, A. R., Sahebkar, A. & Shakeri, A. Ethnobotany of the medicinal plants used by the ethnic communities of Kerman province, Southeast Iran. J. Ethnobiol. Ethnomed. 17 (2021).
Sadeghi, Z., Kuhestani, K., Abdollahi, V. & Mahmood, A. Ethnopharmacological studies of indigenous medicinal plants of Saravan region, Baluchistan, Iran. J. Ethnopharmacol. 153, 111–118 (2014).
Sadat-Hosseini, M., Farajpour, M., Boroomand, N. & Solaimani-Sardou, F. Ethnopharmacological studies of indigenous medicinal plants in the south of Kerman, Iran. J. Ethnopharmacol. 199, 194–204 (2017).
Ghorbani, A. Studies on pharmaceutical ethnobotany in the region of Turkmen Sahra, north of Iran (Part 1): General results. J. Ethnopharmacol. 102, 58–68 (2005).
Ebrahim Hosseini, S., Tavakoli, F. & Karami, M. Medicinal plants in the treatment of diabetes Mellitus. J. Clin. Exc 2 (2014).
Mehrnia, M., Akaberi, M., Amiri, M. S., Nadaf, M. & Emami, S. A. Ethnopharmacological studies of medicinal plants in central Zagros, Lorestan Province, Iran. J. Ethnopharmacol. 280, 114080 (2021).
Delfan, B., Bahmani, M., Rafieian-Kopaei, M., Delfan, M. & Saki, K. A review study on ethnobotanical study of medicinal plants used in relief of toothache in Lorestan Province, Iran. Asian Pac. J. Trop. Dis. 4, S879–S884 (2014).
Wangchuk, P., Yeshi, K. & Jamphel, K. Pharmacological, ethnopharmacological, and botanical evaluation of subtropical medicinal plants of Lower Kheng region in Bhutan. Integr. Med. Res. 6, 372–387 (2017).
Khan, M. N. & Badshah, L. Floristic diversity and utility of flora of district Charsadda, Khyber Pakhtunkhwa. Acta Ecol. Sin. 39, 306–320 (2019).
Khan, W. M., Shah, S. Z., Khan, M. S. & Akhtar, N. Evaluation of indigenous knowledge of medicinal plants from Tall Dardyal Hills, Khyber Pakhtunkhwa, Pakistan. J. Herb. Med. 20, 100314 (2020).
Aziz, M. A., Khan, A. H. & Pieroni, A. Ethnoveterinary plants of Pakistan: a review. Journal of ethnobiology and ethnomedicine vol. 16 25 Preprint at (2020). https://doi.org/10.1186/s13002-020-00369-1
Shuaib, M. et al. Traditional knowledge about medicinal plant in the remote areas of Wari Tehsil, Dir Upper, Pakistan. Brazilian J. Biology. 83, 1–28 (2023).
Majid, A. et al. Exploring threatened traditional knowledge; ethnomedicinal studies of rare endemic flora from lesser himalayan region of Pakistan. Revista Brasileira De Farmacognosia. 29, 785–792 (2019).
Hassan, N. et al. Identification and quantitative analyses of medicinal plants in Shahgram valley, district swat, Pakistan. Acta Ecol. Sin. 40, 44–51 (2020).
Ashfaq, S. et al. Medicinal plant biodiversity used among the rural communities of arid regions of northern Punjab, Pakistan. Indian J. Traditional Knowl. 18, 226–241 (2019).
Tali, B. A., Khuroo, A. A., Ganie, A. H. & Nawchoo, I. A. Diversity, distribution and traditional uses of medicinal plants in Jammu and Kashmir (J&K) state of Indian Himalayas. J. Herb. Med. 17–18, 100280 (2019).
Guo, C. A. et al. An ethnobotany survey of wild plants used by the tibetan people of the Yadong River Valley, Tibet, China. J. Ethnobiol. Ethnomed. 18, 1–25 (2022).
Figueiredo Junior, E. C. et al. Ethnobotanical knowledge of herbalists about medicinal plants from the semiarid region in northeastern Brazil. Bol. Latinoam. Caribe Plantas Med. Aromat. 21, 803–815 (2022).
Belichenko, O., Kolosova, V., Kalle, R. & Sõukand, R. Green pharmacy at the tips of your toes: medicinal plants used by Setos and russians of Pechorsky District, Pskov Oblast (NW Russia). J. Ethnobiol. Ethnomed. 18, 1–38 (2022).
Ahoyo, C. C. et al. Traditional medicinal knowledge of woody species across climatic zones in Benin (West Africa). J. Ethnopharmacol. 265 (2021).
Khajuria, A. K., Manhas, R. K., Kumar, H. & Bisht, N. S. Ethnobotanical study of traditionally used medicinal plants of Pauri district of Uttarakhand, India. J. Ethnopharmacol. 276, 114204 (2021).
Lee, C. et al. Ethnobotanical study on medicinal plants used by local Van Kieu ethnic people of Bac Huong Hoa nature reserve, Vietnam. J. Ethnopharmacol. 231, 283–294 (2019).
Al Hatmi, S. & Lupton, D. A. Documenting the most widely utilized plants and the potential threats facing ethnobotanical practices in the Western Hajar Mountains, sultanate of Oman. J. Arid Environ. 189, 104484 (2021).
Caballero-Serrano, V. et al. Traditional ecological knowledge and medicinal plant diversity in Ecuadorian Amazon home gardens. Glob Ecol. Conserv. 17, e00524 (2019).
Kimpouni, V., Mamboueni, J. C., Tsoungould, F. G. M. & Mikoko, E. N. Ethnobotanical and phytotherapeutic study from Kouni community of the sub-prefecture of Kayes (Bouenza – Congo). Heliyon 5, e02007 (2019).
Cordoba-Tovar, L. et al. Cultural belief and medicinal plants in treating COVID 19 patients of western Colombia. Acta Ecol. Sin. https://doi.org/10.1016/j.chnaes.2021.10.011 (2021).
Fars Meteorological Organization. www.farsmet.ir/ReportAmar.aspx. (2020).
Sehati, M. T. Impact of slope and rock layers of conglomerate and sandstone lithology on vegetation cover in arid lands (Case study: Lamerd Fars Province). Arid Biome Sci. Res. J. 1, 39–48 (2012).
Alalwan, T. A., Alkhuzai, J. A., Jameel, Z. & Mandeel, Q. A. Quantitative ethnobotanical study of some Medicinal plants used by herbalists in Bahrain. J. Herb. Med. 17–18, 100278 (2019).
Moradi, G., Abbasi, E. & Zare Chahooki, M. A. Flora, life forms, and geographical distrbution of plants in Lamerd ranges, Fars, Iran. Watershed management researchers (pajouhesh-va-sazandegi) 86, 70–80 (2010).
Panmei, R., Gajurel, P. R. & Singh, B. Ethnobotany of medicinal plants used by the Zeliangrong ethnic group of Manipur, northeast India. J. Ethnopharmacol. 235, 164–182 (2019).
Yebouk, C. et al. Ethnobotanical study of medicinal plants in the Adrar Province, Mauritania. J. Ethnopharmacol. 246, 112217 (2020).
Miara, M. D. et al. Medicinal plants and their traditional uses in the highland region of Bordj Bou Arreridj (Northeast Algeria). J. Herb. Med. 16, 100262 (2019).
Cochran, W. G. Sampling Techniques (Wiley Blackwell, 1977).
Espinosa, M. M., Bieski, I. G. & Martins, D. T. Sampling in ethnobotanical studies of medicinal plants. Methods and Techniques in Ethnobiology and Ethnoecology 197–212 (2014).
Tamang, S., Singh, A., Bussmann, R. W., Shukla, V. & Nautiyal, M. C. Ethno-medicinal plants of tribal people: a case study in Pakyong subdivision of East Sikkim, India. Acta Ecol. Sin. https://doi.org/10.1016/j.chnaes.2021.08.013 (2022).
Mozaffarian, V. Dictionary of Iranian Plant Names: Latin-English-Persian (Farhang moaser, 2009).
Mozaffarian, V. Identification of Medicinal and Aromatic Plants of Iran (Farhang moaser, 2016).
International Plant Names Index. www.ipni.org. (2022).
World Flora Online. www.worldfloraonline.org. (2022).
Plants of the World Online. www.plantsoftheworldonline.org. (2022).
The, I. U. C. N. & Red List. www.iucnredlist.org (2022).
International Classification Committee of WONCA. International Classification of Primary Care (Oxford University, 2005).
Hussain, S. et al. Quantitative ethnopharmacological profiling of medicinal shrubs used by indigenous communities of Rawalakot, District Poonch, Azad Jammu and Kashmir, Pakistan. Revista Brasileira De Farmacognosia. 29, 665–676 (2019).
Sukumaran, S., Sujin, R. M., Geetha, V. S. & Jeeva, S. Ethnobotanical study of medicinal plants used by the Kani tribes of Pechiparai Hills, Western Ghats, India. Acta Ecol. Sin. 41, 365–376 (2021).
Phillips, O., Gentry, A. H., Reynel, C., Wilkin, P. & Galvez-Durand, B. C. Etnobotánica cuantitativa y la conservación de la Amazonia. Conserv. Biol. 8, 225–248 (1994).
Whitney, C. EthnobotanyR: Calculate quantitative ethnobotany indices. (2022). https://CRAN.R-project.org/package=ethnobotanyR
El-Ghazouani, F., El-Ouahmani, N., Teixidor-Toneu, I., Yacoubi, B. & Zekhnini, A. A survey of medicinal plants used in traditional medicine by women and herbalists from the city of Agadir, southwest of Morocco. Eur. J. Integr. Med. 42, 101284 (2021).
Tardío, J. & Pardo-De-Santayana, M. Cultural importance indices: a comparative analysis based on the useful wild plants of southern Cantabria (northern Spain). Econ. Bot. 62, 24–39 (2008).
Sargin, S. A. & Büyükcengiz, M. Plants Used in Ethnomedicinal Practices in Gulnar District of Mersin, Turkey. J. Herb. Medi. 15 (2019).
Polat, R. Ethnobotanical study on medicinal plants in Bingöl (City center) (Turkey). J. Herb. Med. 16 (2019).
Reyes-García, V., Huanca, T., Vadez, V., Leonard, W. & Wilkie, D. Cultural, practical, and economic value of wild plants: a quantitative study in the Bolivian Amazon. Econ. Bot. 60, 62–74 (2006).
Kremen, C., Raymond, I. & Lance, K. An interdisciplinary tool for monitoring conservation impacts in Madagascar. Conserv. Biol. 12, 549–563 (1998).
Chaachouay, N., Benkhnigue, O., Douira, A. & Zidane, L. Poisonous medicinal plants used in the popular pharmacopoeia of the Rif, northern Morocco. Toxicon 189, 24–32 (2021).
Aparicio, H., Hedberg, I., Bandeira, S. & Ghorbani, A. Ethnobotanical study of medicinal and edible plants used in Nhamacoa area, Manica province–Mozambique. South. Afr. J. Bot. 139, 318–328 (2021).
Nguyen, X. M. A., Bun, S. S., Ollivier, E. & Dang, T. P. T. Ethnobotanical study of medicinal plants used by K’Ho-Cil people for treatment of diarrhea in Lam Dong Province, Vietnam. J. Herb. Med. 19, 100320 (2020).
Mosaddegh, M., Naghibi, F., Moazzeni, H., Pirani, A. & Esmaeili, S. Ethnobotanical survey of herbal remedies traditionally used in Kohghiluyeh Va Boyer Ahmad province of Iran. J. Ethnopharmacol. 141, 80–95 (2012).
Saki, K. et al. The most common native medicinal plants used for psychiatric and neurological disorders in Urmia city, northwest of Iran. Asian Pac. J. Trop. Dis. 4, S895–S901 (2014).
Savić, J., Mačukanović-Jocić, M. & Jarić, S. Medical ethnobotany on the Javor Mountain (Bosnia and Herzegovina). Eur. J. Integr. Med. 27, 52–64 (2019).
Xiong, Y., Sui, X., Ahmed, S., Wang, Z. & Long, C. Ethnobotany and diversity of medicinal plants used by the Buyi in eastern Yunnan, China. Plant. Divers. 42, 401–414 (2020).
Hosseini, S. H. & Bibak, H. Ramezani Ghra, A. Ethnobotanical study of medicinal plants of south Kerman. Eco-phytochemical J. Med. Plants. 1, 30–63 (2020).
Bazgir, A. & Pour Hashemi, M. Ethnobotany of plants of the Bastam region of Selseleh county, Lorestan province. Sci. J. Iran. Indigenous Knowl 7, 85–158 (2021).
Dolatkhahi, M., Ghorbani Nohooji, M., Mehrafarin, A., Amini Nejad, G. & Dolatkhahi, A. Ethnobotanical Study of Medicinal Plants in Kazeroon, Iran: identification, distribution and traditional usage. J. Herb. Drugs 2, (2012).
Zolfaghari Baghersad, R., Piri, K., Abdoli, A., Mehrabian, A. R. & Abdoli, S. Importance of Using Ethnobiological Knowledge for the Conservation of Medicinal Plants Biodiversity in the Lar Region (Iran). Journal of Medicinal Plants and By-products (2012).
Razmjoue, D., Zarei, Z. & Armand R.
Malekpourzadeh, L., Ghahremaninejad, F. & Mirtajadini, S. M. Collection and Identification of Some Selected Medicinal Plants with Antimicrobial Properties from Takhte-Sartashtak Region, Kerman, Iran. Journal of Medicinal Plants and By-products (2012).
Mehrnia, M. & Hosseini, Z. Ethnobotanical study of medicinal plants native to Al-shatar region (Lorestan). J. Traditional Med. Islam Iran. 11, 81–112 (2020).
Mir shekar, M., Ebrahimi, M. & Ajourloo, M. Ethnobotanical study and traditional uses of some medicinal plants of Khash County. J. Traditional Med. Islam Iran. 9, 361–370 (2018).
Rahim foruzeh, M., Heshmati, G. & Barani, H. Collection and ethnobotanical study of selected plants from Kohgiluyeh and Boyer Ahmad province. J. Traditional Med. Islam Iran. 5, 131–139 (2014).
Delfan, B., Bahmani, M., Hassanzadazar, H. & Saki, K. Ethnobotany study of effective medicinal plants on gastric problems in Lorestan Province, West of Iran. J. Chem. Pharm. Res. 7, 483–492 (2015).
Khodayari, H., Amani, S. & Amiri, H. Ethnobotany of medicinal plants of northeastern Khuzestan Province. J. Eco-phytochemistry Med. Plants. 8, 12–26 (2014).
Delfan, E., Khodayari, H. & Azizi, K. Ethnobotany of Native Medicinal Plants in Zagheh and Biranshahr districts, Lorestan Province, Iran. Ech-Phytochem. J. Med. Plants 4 (2019).
Parsaei, P., Bahmani, M., Naghdi, N. & Asadi-Samani, M. Identification of medicinal plants effective on common cold: an ethnobotanical study of Shiraz, South Iran. Pharm. Lett. 8, 90–97 (2016).
Jivad, N., Bahmani, M. & Asadi-Samani, M. A review of the most important medicinal plants effective on wound healing on ethnobotany evidence of Iran. Pharm. Lett. 8, 353–357 (2016).
Sharififar, F., Moharam Khani, M. R., Moattar, F., Babakhanloo, P. & Khodami, M. Ethnobotanical Study of Medicinal Plants of Joopar Mountains of Kerman Province, Iran. J. Kerman Univ. Med. Sci. 21, 37–51 (2014).
Ahmadipour, S., Mohsenzadeh, A., Eftekhari, Z. & Ahmadipour, S. An overview of the most important medicinal plants affecting on child’s jaundice in Ethnobotanical resource of Iran. Pharm. Lett. 8, 135–139 (2016).
Mozaffari Nejad, A. S. & Laey, G. Ethnobotany and Folk Pharmaceutical properties of major trees or shrubs in Northeast of Iran. Asian J. Chem. 21, 5632–5638 (2009).
Moradi, M. T., Asadi-Samani, M. & Bahmani, M. Hypotensive medicinal plants according to ethnobotanical evidence of Iran: a systematic review. Int. J. PharmTech Rerearch. 9, 416–426 (2016).
Parsaei. Pouya, Bahmani, M., Asadi-Samani, M. & Rafieian-Kopaei, M. The most important medicinal plants effective on constipation by the ethnobotanical documents in Iran: a review. Pharm. Lett. 8, 188–194 (2016).
Rouhi-Boroujeni, H., Majid, A. S. & Moradi, M. T. A review of the medicinal plants effective on headache based on the ethnobotanical documents of Iran. Pharm. Lett. 8, 37–42 (2016).
Delfan, B. et al. Effective herbs on the wound and skin disorders: a ethnobotanical study in Lorestan province, west of Iran. Asian Pac. J. Trop. Dis. 4, S938–S942 (2014).
Bahmani, M., Zargaran, A., Rafieian-Kopaei, M. & Saki, K. Ethnobotanical study of medicinal plants used in the management of diabetes mellitus in the Urmia, Northwest Iran. Asian Pac. J. Trop. Med. 7, S348–S354 (2014).
Mosaddegh, M., Esmaeili, S., Hassanpour, A., Malekmohammadi, M. & Naghibi, F. Ethnobotanical Study in the Highland of Alvand and Tuyserkan, Iran. Res. J. Pharmacognosy (RJP) 3 (2016). http://rjpharmacognosy.ir
Ma’ameri, M., Abbasi khalaki, M. & Dadjoo, F. Ethnobotany of plants of Darvish Chai Sarein watershed with a medicinal and nutritional approach. Sci. J. Rangel. 14, 698–714 (2020).
Moghanloo, L., Ghahremaninejad, F. & Vafadar, M. Ethnobotanical study of medicinal plants in the central district of the Zanjan County, Zanjan Province, Iran. J. Herb. Med. 9, 121–131 (2019).
Saadatpour, M., Barani, H., Abedi Sarvestani, A. & Forouzeh, M. R. Ethnobotanical study of Sojasrood medicinal plants (Zanjan Province). J. Herb. Drugs. 8, 185–193 (2017).
Mardani nejad S. & Vazir poor, M.
Abbasi, S., Afsharzadeh, S., Mohajeri, A. & reza Introduction of plant species with medicinal properties in Natanz region (Kashan). J. Herb. Drugs. 3, 147–156 (2012).
Eskandari, M., Assadi, M., Shirzadian, S. & Mehregan, I. Ethnobotanical study and distribution of the Solanum section Solanum species (Solanaceae) in Iran. J. Med. Plants. 18, 85–98 (2019).
Dolat khahi, M. Nabi poor, I. Ethnobotanical study of medicinal plants of the northeastern Persian Gulf watershed. J. Herb. Drugs. 2, 129–143 (2014).
Ethnobotanical study of some medicinal plants. Of Abhar County, Zanjan Province. J. Herb. Drugs. 19, 30–54 (2020).
Moradi, M. T., Asadi-Samani, M., Bahmani, M. & Shahrani, M. Medicinal plants used for liver disorders based on the ethnobotanical documents of Iran: a review. Int. J. Pharmtech Res. 9, 407–415 (2016).
Mohamadi, N., Sharififar, F., Koohpayeh, A. & Daneshpajouh, M. Traditional and ethnobotanical uses of medicinal plants by ancient populations in Khabr and Rouchon of Iran. J. Appl. Pharm. Sci. 5, 101–107 (2015).
Zahra Sadeghi, I. & Kuhestani, K. Ethnobotany of Date Palm (Phoenix Dactylifera) in Baluch Tribe of Saravan Region. Journal of Agricultural Technology vol. 10 www.naturland.de (2014).
Naghibi, F., Esmaeili, S., Malekmohammadi, M., Hassanpour, A. & Mosaddegh, M. Ethnobotanical survey of medicinal plants used traditionally in two villages of Hamedan, Iran. Res. J. Pharmacognosy (RJP). 1, 7–14 (2014).
Kiyasi, Y. & Forouzeh, M. R. Ethnobotanical Study of Medicinal Plants in Abadeh County (Case Study: Almalicheh Range). J. Tradit. Med. Islam Iran. (2019).
Haerinasab, M. & Abbasi, S. Ethnobotanical study of medicinal plants and introduction to some poisonous plant species of Ardestan (Isfahan province). J. Med. Plants. 18, 122–143 (2019).
Ramezanian, M. & Minaie far, A. Ethnobotanical Study of Medicinal plants of Fasa County. J. Tradit. Med. Islam Iran. 7 (2016).
Dastyar, N. & Altememy, D. Ethnobotanical Study for Hypertension Treatment: an ethnobotanical study of Abadeh, South Iran. J. Biochemicals Phytomedicine. 1, 13–16 (2022).
Dastyar, N. & Lysiuk, R. Identification of the most important Medicinal plants used for Wound Healing: an ethnobotanical study of Sistan and Baluchestan Province, Southeastern Iran. J. Biochemicals Phytomedicine. 2, 16–19 (2023).
Dastyar, N. & Ahmadi, M. An Ethnobotanical Study of Medicinal Plants administered for the Treatment of Hyperlipidemia in Bushehr, South Iran. J. Biochemicals Phytomedicine. 1, 26–30 (2022).
Ghasemi Pirbalouti, A. Ethnobotany and antimicrobial activity of medicinal plants of Bakhtiari Zagross mountains, Iran. J. Med. Plants Res. 6 (2012).
Negahdari, S. Ethnobotanical Study of Medicinal Plants Used for Management of Diabetes Mellitus in the East of Khuzestan, Southwest Iran. J. Biochemicals Phytomedicine. 2, 7–10 (2023).
Bahmani, M. Overview of Medicinal plants used for Cardiovascular System disorders and diseases in Ethnobotany of different areas in Iran. J. HerbMed Pharmacol. J. Homepage: J. HerbMed Pharmacol. 5 (2016). http://www.herbmedpharmacol.com
Nadaf, M. et al. Ethnobotanical Diversity of Trees and Shrubs of Iran: A Comprehensive Review. International Journal of Plant Biology vol. 14 120–146 Preprint at (2023). https://doi.org/10.3390/ijpb14010011
Hosseini, M., Rahim Forouzeh, M. & Barani, H. Identification and investigation of ethnobotany of some medicinal plants in Razavi Khorasan Province. J. Med. Plants. 18, 212–231 (2019).
Mechaala, S., Bouatrous, Y. & Adouane, S. Traditional knowledge and diversity of wild medicinal plants in El Kantara’s area (Algerian Sahara gate): an ethnobotany survey. Acta Ecol. Sin. 42, 33–45 (2022).
Mogale, M. M. P., Raimondo, D. C. & VanWyk, B. E. The ethnobotany of Central Sekhukhuneland, South Africa. South. Afr. J. Bot. 122, 90–119 (2019).
Alqethami, A., Aldhebiani, A. Y. & Teixidor-Toneu, I. Medicinal plants used in Jeddah, Saudi Arabia: a gender perspective. J. Ethnopharmacol. 257, 112899 (2020).
Birjees, M. et al. Traditional knowledge of wild medicinal plants used by the inhabitants of Garam Chashma Valley, district Chitral, Pakistan. Acta Ecol. Sin. 42, 19–33 (2022).
Ullah, A. et al. Ethnomedicinal flora of Frontier Region Tank, Fata, Pakistan. Acta Ecol. Sin. 39, 321–327 (2019).
Lin, Y. et al. Ethnobotanical survey of medicinal plants in Gaomi, China. J. Ethnopharmacol. 265, 113228 (2021).
Al-Fatimi, M. Ethnobotanical survey of medicinal plants in central Abyan governorate, Yemen. J. Ethnopharmacol. 241, 111973 (2019).
Prabhu, S., Vijayakumar, S., Morvin Yabesh, J. E., Prakashbabu, R. & Murugan, R. An ethnobotanical study of medicinal plants used in pachamalai hills of Tamil Nadu, India. J. Herb. Med. 25, 100400 (2021).
Petrakou, K., Iatrou, G. & Lamari, F. N. Ethnopharmacological survey of medicinal plants traded in herbal markets in the peloponnisos, Greece. J. Herb. Med. 19, 100305 (2020).
Abdusalam, A. et al. Documenting the heritage along the Silk Road: an ethnobotanical study of medicinal teas used in Southern Xinjiang, China. J. Ethnopharmacol. 260, 113012 (2020).
Bhattarai, S., Chaudhary, R. P. & Taylor, R. S. L. Ethnomedicinal plants used by the people of Manang district, central Nepal. J. Ethnobiol. Ethnomed. 2, 1–8 (2006).
Kyaw, Y. M. M., Bi, Y., Oo, T. N. & Yang, X. Traditional medicinal plants used by the Mon people in Myanmar. J. Ethnopharmacol. 265, 113253 (2021).
Gumisiriza, H., Birungi, G., Olet, E. A. & Sesaazi, C. D. Medicinal plant species used by local communities around Queen Elizabeth National Park, Maramagambo Central Forest Reserve and Ihimbo Central Forest Reserve, South western Uganda. J. Ethnopharmacol. 239, 111926 (2019).
Joshi, N., Ghorbani, A., Siwakoti, M. & Kehlenbeck, K. Utilization pattern and indigenous knowledge of wild medicinal plants among three ethnic groups in Makawanpur district, Central Nepal. J. Ethnopharmacol. 262, 113219 (2020).
Roy, S. K. & Roy, D. K. Use of Medicinal Plant and its vulnerability due to Climate Change in Northern Part of Bangladesh. Am. J. Plant. Sci. 07, 1782–1793 (2016).
Hounsou, K. E., Sonibare, M. A. & Elufioye, T. O. Climate change and the future of medicinal plants research. Bioactive Compounds in Health and Disease vol. 7 152–169 Preprint at (2024). https://doi.org/10.31989/BCHD.V7I3.1310
Acknowledgements
The authors would like to thank our interviewees for their time and effort dedicated to our interviews and field trips.
Funding
This study was supported by Department of Natural Resources and Environmental Engineering, School of Agriculture, Shiraz University, Shiraz, Iran.
Author information
Authors and Affiliations
Contributions
S.Gh. Conceptualization; Methodology; Software; Validation; Formal analysis; Investigation; Resources; Data Curation; Visualization; Roles/ Writing – original draft and R. S. Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Software; Supervision; Validation; Visualization; Roles/ Writing – original draft and Gh. Gh. Formal analysis; Methodology; Resources; Software; Roles: review & editing and Th. L. Conceptualization; Formal analysis; Methodology; Roles/ Writing – review & editing and E. Gh. Software; Formal analysis; Data Curation; Visualization. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Human subjects
Informed consent was obtained from all individual participants involved in the study. The research did not require ethical approval according to the regulations of Shiraz University and Iranian research ethics guidelines.
Plant material
The plant material used in this study was collected from a wild population growing on public land, adhering to local or national guidelines. No specific license or permission was required for this collection. The plant specimens were identified by Mr. Ahmad Hatami and deposited in the herbarium of the Fars Agricultural and Natural Resources Research and Education Center.
Generative AI and AI-assisted technologies in the writing process
During the preparation of this work the authors used ChatGPT in order to improve readability and language. After using this tool, the authors reviewed and edited the content as needed and takes full responsibility for the content of the publication.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ghafouri, S., Safaeian, R., Ghanbarian, G. et al. Medicinal plants used by local communities in southern Fars Province, Iran. Sci Rep 15, 5742 (2025). https://doi.org/10.1038/s41598-025-88341-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-88341-5
Keywords
This article is cited by
-
Ethnomedicinal plants and traditional healing practices of indigenous communities in Dan Sub-district, Kap Choeng District, Surin Province, Thailand
Journal of Ethnobiology and Ethnomedicine (2026)
-
An overview on ethnomedicinal uses, phytochemistry, pharmacological activities, and conservation status of Maerua oblongifolia (Forssk.) A. Rich.
Genetic Resources and Crop Evolution (2025)
