
Abstract
This study aimed to evaluate the effectiveness of a new combined treatment approach using arthrocentesis, hyaluronic acid (HA) injection, mandibular manipulation (MM), and the Twin-Block appliance (TBA) for managing acute anterior disc displacement without reduction (ADDwoR). A retrospective cross-sectional study was designed. Thirty-seven patients (38 joints) diagnosed with acute ADDwoR were treated with arthrocentesis plus HA combined with MM and TBA in turn from January 2022 to December 2023. The maximum mouth opening (MMO), visual analogue scale (VAS) pain score, condyle/disc position were measured and comparatively analyzed at baseline and one week, three and six months post-treatment. Analysis of variance, Dunnett’s T3 analysis, and paired samples t-tests were conducted for statistical analyses setting the threshold for statistical significance at P < 0.05. This treatment achieved a success rate of 94.59% (35/37). After one week of treatment, the MMO exhibited a statistically significant improvement, while the VAS pain scores showed a statistically significant decrease (P < 0.001). Magnetic resonance imaging revealed that at six months post-treatment, there was a significant forward shift in the condylar position compared with pre-treatment (P < 0.001),alongside a significant backward movement of the disc on the affected side (P < 0.001).The combination of arthrocentesis plus HA, MM, and TBA can effectively relieve clinical symptoms and restore the disc-condylar relationship in patients with acute ADDwoR.
Similar content being viewed by others
Anterior disc displacement of temporomandibular joint (TMJ) is one of the most common TMJ disorders which can be classified into two categories: with and without reduction (ADDwR/ADDwoR)1,2,3,4,5. Patients with ADDwR typically present with symptoms such as clicking that occur during mouth opening2,3,6.
The signs and symptoms of ADDwR can aggravate into ADDwoR, characterized by limited mouth opening immediately after the disappearance of joint clicking, minimal or no condylar translation, restricted lateral movement away from the affected side, and deviation of the mandible toward the affected side during mouth opening4,6. This condition can be classified into two stages based on the duration of mouth opening restriction: ADDwoR acute stage (≤ 2 months) and chronic stage (> 2 months)5. Following an acute episode, pain may gradually be relieved, possibly becoming nonexistent, and mouth opening can also be improved7. However, articular cartilage and subarticular bone abrasion may develop gradually over time5,7. Due to potential long-term harmful effects, some scholars suggest that the repositioning of a displaced TMJ disc should be considered8.
Mandibular manipulation (MM) is an effective treatment for acute ADDwoR, first reported by Farrar et al.9 in 1978. Numerous studies have confirmed its effectiveness, and additional procedures, including pre-treatment intracapsular anesthetic injection, arthrocentesis and the use of a stabilization splint or an anterior repositioning splint (ARS), have been employed to increase the success rate of treatment on the basis of MM5,10,11,12.
Arthrocentesis is an effective treatment for ADDwoR as it removes inflammatory mediators, breaks adhesions, alleviates pain, and improves joint mobility13. Since its introduction by Nitzan et al.14 in 1991, arthrocentesis has become a widely accepted treatment option. Following arthrocentesis, hyaluronic acid (HA) is usually administered into the TMJ. By facilitating smooth gliding of the articular surfaces, HA decreases pain and enhances patient cooperation during MM.
The Twin-Block appliance (TBA) is made up of upper and lower plates, along with posterior bite blocks that have inclined planes. These components slide against each other, guiding the mandible forward as the mouth closes with the TBA in position15. Rohida et al.16 found that the TBA effectively relieves joint pain, reduces joint dysfunction, and minimizes joint clicking in patients with ADDwR. It can serve as an ARS by actively positioning the mandible downward and forward, thus recapturing the anteriorly displaced disc16. Chavan et al.17 found that the disc position moved backward after 6 months of TBA treatment. TBA is generally better tolerated by patients because of its compact size, absence of a visible acrylic part at the front, and minimal interference with speech18,19.
By combining arthrocentesis with HA, MM, and TBA in turn, our department has achieved significant therapeutic effects in the treatment of acute ADDwoR. This study focuses on assessing the effectiveness of the above-mentioned treatment in improving clinical symptoms and repositioning the disc and condyle in patients diagnosed with acute ADDwoR.
Materials and methods
Study design
To achieve the research objective, the investigators conducted a cross-sectional retrospective study. The study protocol was approved by the Institutional Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University (approval number: K202108-25) and followed the principles outlined in the Announcement of Helsinki. Informed consent was provided by all subjects and their legal guardian(s).
Patients selection
The Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD) list important diagnostic points for TMJ ADD as follows: TMJ clicking or noise during mouth movements, varying degrees of mouth opening limitation, jaw deflection while opening, pain localized in the TMJ area both at rest and during activity20.
The following inclusion criteria were used: (1) diagnosis of ADDwoR confirmed by magnetic resonance imaging (MRI); (2) with a duration of mouth opening restriction ≤ 2 months; (3) patient and/ or the patient’s legal representative are aware of and consent to the treatment. Subject exclusion criteria were as following: (1) prior maxillofacial trauma or inflammation history; (2) prior TMJ treatment history; (3) presence of any systemic joint disease; (4) missing follow-up and incomplete clinical data.
A total of 37 patients were collected from the TMJ Specialist Clinic at the First Affiliated Hospital of Xinjiang Medical University from January 2022 to December 2023. All patients agreed to participate in the investigation. The 37 subjects had an average age of 26.14 ± 9.63 years, ranging from 12 to 51 years, with 29 females and 8 males. There were nineteen cases on the left side, seventeen cases on the right side, and one case on bilateral sides. The study flowchart based on the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement21 is shown in Fig. 1.

The flow diagram describing the subjects’ enrollment as well as the working plan. Abbreviations: ADDwoR anterior disc displacement without reduction, ANOVA analysis of variance, MMO maximum mouth opening, MRI magnetic resonance imaging, VAS visual analogue scale.
Treatment procedures
First, we performed arthrocentesis along with HA injection, in accordance with the findings of Li et al.22. After administering local anesthesia of 2% lidocaine hydrochloride injection (ZhaoHui Pharmaceutical, Shanghai, China) and preparing the affected TMJ sterilely, we injected 2 mL of physiological saline into the upper joint cavity. This was done under pressure using a single-needle technique, with the saline being pumped in and out several times. Once the procedure is completed, proceed to inject 1mL (10 mg) of HA (Seikagaku, Tokyo, Japan) into the joint space.
Second, MM is performed to manage the condition of jaw “locking”23. With their thumb on the mandibular molar of the affected side, the clinician gently pulled the mandible downward on the contralateral side. The clinician placed their other hand on the same side of temporal region to stabilize the patient’s head during the MM procedure. Two criteria indicate successful MM: the affected TMJ produces an audible click, and the maximum mouth opening (MMO) is more than 40 mm immediately5,23.
Third, we followed Clark’s guidelines24 to prepare the TBA. The mandible was positioned in an edge-to-edge relationship, and the vertical dimension was augmented by 4–5 mm. The vestibular arch and the screw for lateral expansion in the midline of the maxillary component were omitted from the TBA design. The angle between the upper and lower components of the appliance was precisely calibrated to 70°. The TBA was required to wear the device continuously for one week (24 h per day). The patient followed a liquid or semi-liquid diet and gargled to ensure oral hygiene this week. After the first week, the patients were instructed to wear their TBA only while sleeping at night for the next six months.
Clinical efficacy evaluation
MMO refers to the distance between the upper and lower central incisors. This measurement excludes any overbite and is taken when patients are seated and open their mouths as wide as they can25. The intensity of TMJ pain during MMO was assessed using the visual analogue scale (VAS) score. The VAS is a tool that enables participants to express their pain intensity by choosing a point on a line marked from 0 to 10 25. MMO and VAS pain score were recorded separately at four time points: before treatment, and one week, three months, and six months after treatment.
MRI examination
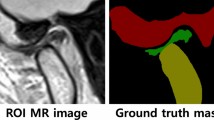
As described in our previous work26, MRI was performed using a 1.5 T scanner (MAGNETOM Aera; Siemens Healthineers, Erlangen, Germany) with TMJ surface coils. T2-weighted images were obtained in the oblique sagittal plane for both closed and open mouth positions, with a repetition tine of 2 500 ms and an echo time of 60 ms. The slice thickness was set to 2 mm, and the inter-slice spacing was set to 0.2 mm.
MRI is performed before the treatment and six months after treatment to observe the position of the joint disc on the affected side. The disc position is categorized into three distinct conditions for clarity: (1) normal disc-condyle relationship; (2) ADDwR; (3) ADDwoR.
Disc and condyle position measurement
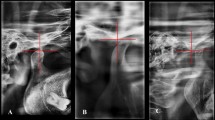
The methodology for accurately measuring the positions of the condyle and disc in joint is thoroughly outlined in Drace & Enzmann27. As shown in Fig. 2, a line (line 1) was defined as a tangent drawn from the lowest part of the articular eminence (point T) to the highest part of the porus acusticus externus (point P). The X-axis, parallel to line 1, was drawn through the highest part of the articular fossa (point G). While the Y-axis was drawn perpendicular to the X-axis from point G, which was designated as the origin of coordinates. The X–Y coordinates of condyle position (points C) and disc position (points D) were recorded respectively.

The procedures for measuring the anatomical positions of the disc and condyle in the joint. Point T: the articular eminence; Point P: the porus acusticus externus; Point G: the articular fossa; Point C: the condyle position; Points D: the disc position.
Statistical analysis
All statistical analyses were performed using SAS software version 9.4 (North Carolina State University, Raleigh, NC, USA). The Shapiro–Wilk test was used to verify the normality of all data. The MMO and VAS values of patients at four different time points were compared utilizing analysis of variance (ANOVA), followed by a least significant difference post hoc analysis performed for normal data with homoscedasticity1. Due to the normal distribution of data with heteroscedasticity, a Dunnett T3 analysis was employed for post-hoc multiple comparisons. A paired t-test was conducted to compare the position of the affected condyle/disc before and after six months of treatment. The differences were statistically significant when P < 0.05.
Results
Clinical effect evaluation
Among the 37 cases, 35 patients (94.59%) demonstrated successful reduction of the joints with audible clicks and immediate improvement in MMO to a normal level (Fig. 3). Two patients did not achieve successful MM: a 21-year-old woman with bilateral ADDwoR and a 37-year-old man with left-sided ADDwoR. The man may be attributed to his anxiety which caused muscle tension and ultimately led to the failure of MM; while the other patient’s failure may be due to the complexity of her bilateral mandibular manipulation.

The maximum mouth opening before/after mandibular manipulation (MM) and Twin-Block appliance (TBA) usage. (a) The patient with ADDwoR had limited mouth opening before treatment. (b) The patient’s mouth opening recovers to normal after arthrocentesis plus HA combined with MM. (c) Immediate TBA insertion after successful disc restoration.
As shown in Table 1; Figs. 4 and 5, the MMO of the remaining 35 patients exhibited significant improvement after treatment, and the VAS pain score also significantly reduced (all P < 0.001). However, no significant differences were found in MMO and VAS pain score at 1 week, 3 months, and 6 months post-treatment (all P > 0.05).

Comparison of maximum mouth opening (MMO) before treatment and at 1 week, 3 months and 6 months after treatment. *p < 0.05, **p < 0.01, ***p < 0.001. ns, no significant difference.

Comparison of visual analogue pain scale (VAS) pain score before treatment and at 1 week, 3 months and 6 months after treatment. *p < 0.05, **p < 0.01, ***p < 0.001. ns, no significant difference.
MRI examination and change in condyle/disc position
Among the 35 patients who underwent successful treatment, 24 cases achieved a normal disc-condylar relationship (Fig. 6), while 11 cases reverted to ADDwR (Fig. 7). According to Table 2, after 6 months of treatment, the condylar position moved significantly forward from its initial position (P < 0.001), while the disc on the affected side shifted significantly backward (P < 0.001).

T2-weighted MRI images reveal that patients with acute anterior disc displacement without reduction have restored a normal disc-condylar relationship after treatment. (a) Before treatment, the MRI showed anterior displacement of the disc and joint effusion in the closed-mouth position. (b) Before treatment, the sagittal MRI showed that the disc was still anteriorly displaced in the opened-mouth position. (c, d) After 6 months of treatment, the sagittal closed (c) / opened (d) position shows the disc was repositioned. TMJ disc positions are indicated by the yellow arrows.

T2-weighted MRI images of patients with acute anterior disc displacement without reduction, who were treated and subsequently restored to anterior disc displacement with reduction. (a) Before treatment, the MRI showed anterior displacement of the disc and joint effusion in the closed-mouth position. (b) Before treatment, the sagittal MRI showed that the disc was still anteriorly displaced in the opened-mouth position. (c) After 6 months of treatment, the sagittal closed position shows the disc anterior displacement slightly. ( d) After 6 months of treatment, the sagittal opened position shows the disc was repositioned. TMJ disc positions are indicated by the yellow arrows.
Discussion
The bilaminar zone of the TMJ is composed of elastic fibres5,28,29. It stretches and generates backward tensile force when the mouth opens wide, which is essential for repositioning the TMJ disc28. However, the elastic fibers may deteriorate and lose their elasticity due to prolonged pressure and progression of the disc displacement5. In addition, joint adhesions are often found in cases of disc displacement, and their severity tends to escalate with prolonged ADDwoR30,31. Chronic ADDwoR patients may also exhibit significant deformities or perforations in their joint discs, articular cartilage, along with issues in the subarticular bone, even dentofacial malformation, bite derangement and various functional impairments that affect their quality of life1,7,9,32. Some scholars believe that within 2 months of the onset of acute ADDwoR, the discs maintain their biconcave shape and exhibit normal condylar bone structure with minimal internal adhesions33,34. Therefore, this study selected patients whose history of restricted mouth opening lasting less than 2 months as subjects.
The treatment concept involves initially restoring ADDwoR to the state of ADDwR through MM, followed by the application of TBA. A crucial requirement for the success of MM is the audible clicking, along with a significant improvement in MMO5,35. The clicking sound usually means that the TMJ has released its locked position and successfully recaptured the disc5,10,11,12,35. It has been reported that arthrocentesis with or without HA injection is effective in alleviating pain and increasing mouth opening36. Otherwise, the improvement in mouth opening is due to the disc being pressed further forward.
Although ARS is effective in treating disc displacement, there is uncertainty about how it works. The first proposal suggests that ARS can help the condyle move forward and downwards to meet the anteriorly displaced disc. This realignment may restore a normal disc-condyle relationship and improve or eliminate clinical symptoms37. The second theory posits that the ARS facilitates the repositioning of displaced discs back into their normal alignment in therapeutic mandibular positions38. Our study examines the role of TBA in treating disc displacement. We found that TBA facilitates the relocation of the displaced disc by guiding the forward movement of the condyles and causing upward movement of the disc at its posterior aspect, similar to the research conducted by Lei et al.5 in ARS.
Throughout the treatment period of one week, three months, and six months, the MMO consistently remained at normal levels, with no significant differences detected. The main reason for the restricted MMO in patients with ADDwoR is the obstacles resulted from TMJ disc displacement. Once MM was administered, MMO levels quickly returned to normal and were effectively maintained by our combined treatment strategy. In addition, the treatment significantly improved the VAS pain score, since MM effectively alleviated the pain resulting from the displaced joint disc that obstructed condylar movement5,35; and arthrocentesis plus HA injection lessened the pain caused by intra-articular inflammation6.
There are currently no standardized instructions regarding the different wearing times for TBA or ARS. According to the study by Lei et al.5, participants were required to wear ARS for 24 h a day during the first three months, whereas TBA was only worn for 24 h a day during the first week of this treatment. Additionally, the MRI examination six months after treatment revealed that the disc moved backward and the condyle moved forward5. In a previous study, Martini et al.11 recommended that patients with acute ADDwoR wear splints continuously for two weeks, followed by usage only at night. Conti et al.39 also suggested wearing splints at night and using additional splints during the day only when experiencing pain, as they found that nighttime use provides significant symptom relief. TBA should be worn 24 h per day during the first week to prevent the disc from displacing again. After this initial period, wearing TBA at night will help prevent permanent changes to the joint structure and occlusion, such as a posterior open bite and myostatic contracture of the inferior head of lateral pterygoid muscle40.
Conclusion
In conclusion, the combination of arthrocentesis with HA, MM and TBA can effectively alleviate clinical symptoms and restore the disc-condylar relationship in patients suffering from acute ADDwoR. This study is limited by its single-center retrospective design and a short follow-up period. Future research should aim for multi-center prospective studies with large sample size and longer follow-up durations.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Li, C. X. et al. Morphologic analysis of Condyle among different disc status in the temporomandibular joints by three-dimensional reconstructive imaging: A preliminary study. BMC Oral Health. 22 (1), 395 (2022).
del Pérez, A. & Doblaré, M. An accurate simulation model of anteriorly displaced TMJ discs with and without reduction. Med. Eng. Phys. 29 (2), 216–226 (2007).
Deregibus, A. et al. Diagnostic concordance between MRI and electrovibratography of the temporomandibular joint of subjects with disc displacement disorders. Dentomaxillofac Radiol. 42 (4), 20120155 (2013).
Bas, B. et al. Use of artificial neural network in differentiation of subgroups of temporomandibular internal derangements: A preliminary study. J. Oral Maxillofac. Surg. 70 (1), 51–59 (2012).
Lei, J. et al. Clinical protocol for managing acute disc displacement without reduction: A magnetic resonance imaging evaluation. Int. J. Oral Maxillofac. Surg. 49 (3), 361–368 (2020).
Dhiman, N. K. et al. Efficacy of arthrocentesis with intra-articular injection of hyaluronic acid and corticosteroid in the treatment of internal derangement of temporomandibular joint. Natl. J. Maxillofac. Surg. 14 (1), 93–100 (2023).
Hu, Y. K. et al. Changes in disc status in the reducing and nonreducing anterior disc displacement of temporomandibular joint: A longitudinal retrospective study. Sci. Rep. 6, 34253 (2016).
Ma, Z. et al. Can anterior repositioning splint effectively treat temporomandibular joint disc displacement? Sci. Rep. 9 (1), 534 (2019).
Farrar, W. B. Characteristics of the condylar path in internal derangements of the TMJ. J. Prosthet. Dent. 39 (3), 319–323 (1978).
Murakami, K. I. et al. Recapturing the persistent anteriorly displaced disk by mandibular manipulation after pumping and hydraulic pressure to the upper joint cavity of the temporomandibular joint. Cranio 5 (1), 17–24 (1987).
Martini, G. et al. MRI study of a physiotherapeutic protocol in anterior disk displacement without reduction. Cranio 14 (3), 216–224 (1996).
Kurita, H. et al. Efficacy of a mandibular manipulation technique in reducing the permanently displaced temporomandibular joint disc. J. Oral Maxillofac. Surg. 57 (7), 784–788 (1999).
Heo, H. A. & Yoon, H. J. Clinical outcomes of patients with bilateral anterior disc displacement without reduction and erosive change of the temporomandibular joint after performance of unilateral arthrocentesis and stabilisation splint therapy. J. Oral Rehabil. 47 (3), 307–312 (2020).
Nitzan, D. W. et al. Temporomandibular joint arthrocentesis: A simplified treatment for severe, limited mouth opening. J. Oral Maxillofac. Surg. 49 (11), 1163–1170 (1991).
Dong, L. et al. Evaluating stress and displacement in the craniomandibular complex using Twin Block appliances at varied angles: A finite element study. J. Mech. Behav. Biomed. Mater. 156, 106603 (2024).
Rohida, N. S. & Bhad, W. A clinical, MRI, and EMG analysis comparing the efficacy of twin blocks and flat occlusal splints in the management of disc displacements with reduction. World J. Orthod. 11 (3), 236–244 (2010).
Chavan, S. J. et al. Comparison of temporomandibular joint changes in Twin Block and Bionator appliance therapy: A magnetic resonance imaging study. Prog Orthod. 15 (1), 57 (2014).
Khoja, A. et al. Cephalometric evaluation of the effects of the Twin Block appliance in subjects with class II, division 1 malocclusion amongst different cervical vertebral maturation stages. Dent. Press. J. Orthod. 21 (3), 73–84 (2016).
Ehsani, S. et al. Short-term treatment effects produced by the twin-block appliance: A systematic review and meta-analysis. Eur. J. Orthod. 37 (2), 170–176 (2015).
Li, C. X. et al. Effects of osseous structure based on three-dimensional reconstructive imaging evaluation in the assessment of temporomandibular joint disc position. Clin. Oral Investig. 27 (4), 1449–1463 (2023).
von Elm, E. et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 370 (9596), 1453–1457 (2007).
Li, Z. et al. Disc-condyle relationship alterations following stabilization splint therapy or arthrocentesis plus hyaluronic acid injection in patients with anterior disc displacement: A retrospective cohort study. Oral Radiol. 39 (1), 198–206 (2023).
Fu, K. et al. Manipulation aided by joint cavity extension followed by occlusal splint for treatment of acute anterior disk displacement without reduction. Chin. J. Stomatol. 37 (1), 36–38 (2002).
Clark, W. J. The twin block technique. A functional orthopedic appliance system. Am. J. Orthod. Dentofac. Orthop. 93 (1), 1–18 (1988).
Li, C. X. et al. Modified minimally invasive surgery in reconstructing the temporomandibular joint disk by transplantation of the temporalis myofascial flap. BMC Musculoskelet. Disord. 24 (1), 7 (2023).
Li, C. X. et al. Effects of condyle on disc status of the reducing and nonreducing anterior disc displacement of the temporomandibular joint based on 3D reconstructive imaging: A pilot study. Quintessence Int. 54 (2), 156–166 (2023).
Drace, J. E. & Enzmann, D. R. Defining the normal temporomandibular joint: Closed-, partially open-, and open-mouth MR imaging of asymptomatic subjects. Radiology 177 (1), 67–71 (1990).
Clément, C. et al. Quantitative analysis of the elastic fibres in the human temporomandibular articular disc and its attachments. Int. J. Oral Maxillofac. Surg. 35 (12), 1120–1126 (2006).
Benigno, M. I. et al. The structure of the bilaminar zone in the human temporomandibular joint: A light and scanning electron microscopy study in young and elderly subjects. J. Oral Rehabil. 28 (2), 113–119 (2001).
Millon-Cruz, A. et al. Relationship between intra-articular adhesions and disc position in temporomandibular joints: Magnetic resonance and arthroscopic findings and clinical results. J. Craniomaxillofac. Surg. 43 (4), 497–502 (2015).
Lee, K. M. et al. An additional lysis procedure during arthrocentesis of the temporomandibular joint. Maxillofac. Plast. Reconstr. Surg. 43 (1), 38 (2021).
Ooi, K. et al. Incidence of anterior disc displacement without reduction of the temporomandibular joint in patients with dentofacial deformity. Int. J. Oral Maxillofac. Surg. 47 (4), 505–510 (2018).
Liu, J. et al. Joint cavity injection combined with manual reduction and stabilization splint treatment of anterior disc displacement. Int. J. Clin. Exp. Med. 8 (4), 5943–5948 (2015).
Cai, B. Physical therapy for temporomandibular joint anterior disc displacement without reduction. Chin. J. Stomatol. 52 (3), 166–170 (2017).
Mongini, F. A modified extraoral technique of mandibular manipulation in disk displacement without reduction. Cranio 13 (1), 22–25 (1995).
Yuce, E. & Komerik, N. Comparison of the efficiacy of intra-articular injection of liquid platelet-rich fibrin and hyaluronic acid after in conjunction with arthrocentesis for the treatment of internal temporomandibular joint derangements. J. Craniofac. Surg. 31 (7), 1870–1874.
Lundh, H. et al. Anterior repositioning splint in the treatment of temporomandibular joints with reciprocal clicking: comparison with a flat occlusal splint and an untreated control group. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 60(2), 131–136 (1985).
Kurita, H. et al. Change of position of the temporomandibular joint disk with insertion of a disk-repositioning appliance. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 85 (2), 142–145 (1998).
Conti, P. C. et al. Partial time use of anterior repositioning splints in the management of TMJ pain and dysfunction: A one-year controlled study. J. Appl. Oral Sci. 13 (4), 345–350 (2005).
Guo, Y. N. et al. An overview of anterior repositioning splint therapy for disc displacement-related temporomandibular disorders. Curr. Med. Sci. 41 (3), 626–634 (2021).
Acknowledgements
Authors appreciate all financial support that granted, and are also grateful to the research volunteers and collaborators.
Funding
All phases of this study was supported by National Natural Science Foundation of China (grant number: 82160189); Scientific Research Innovation Project - Hubei Province Key Laboratory of Oral and Maxillofacial Development and Regeneration (grant number: 2022kqhm008); Natural Science Foundation of Xinjiang Uygur Autonomous Region (grant number: 2023D01D14).
Author information
Authors and Affiliations
Contributions
Conceptualization: Zhi-qiang Song, Chen-xi Li, Zhong-cheng Gong.Writing—original draft: Chen-xi Li and Zhi-qiang Song.Writing—revision, review & editing: Chen-xi Li.Data curation: Zhi-qiang Song.Formal analysis: Zhi-qiang Song and Chen-xi Li.Funding acquisition: Zhong-cheng Gong and Chen-xi Li.Investigation: Zhi-qiang Song and Chen-xi Li.Methodology: Zhi-qiang Song, Chen-xi Li, Zhong-cheng Gong.Supervision: Zhong-cheng Gong.Validation: Zhi-qiang Song and Zhong-cheng Gong.Project administration: Zhong-cheng Gong.All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study protocol was reviewed and approved by the Ethics Committee at the First Affiliated Hospital of Xinjiang Medical University, Urumqi, PR China, with the onset of baselined data collection (approval no. K202108-25). Procedures operated in this study were completed in keeping with the standards set out in the Announcement of Helsinki and laboratory regulations of research in China.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Song, Zq., Li, C. & Gong, Z. A novel combination of treatments for acute anterior disc displacement without reduction of temporomandibular joint. Sci Rep 15, 4176 (2025). https://doi.org/10.1038/s41598-025-88622-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-88622-z
