
Abstract
To explore whether intravesical chemotherapy (IVC) between primary and second transurethral resection of bladder tumor (TURBT) affects the prognosis of non-muscle invasive bladder cancer (NMIBC) patients receiving Bacillus Calmette-Guérin (BCG) treatment. NMIBC patients who underwent a second TURBT and subsequent BCG treatment between 2012 and 2023 at the Affiliated Hospital of Xuzhou Medical University were retrospectively analyzed. These patients were divided into Group A, which received IVC between TURBT, and Group B, which did not. Recurrence-free survival (RFS) was compared among the different risk subgroups. A total of 292 NMIBC patients were included in this study. In the entire cohort, IVC treatment between the primary and second TURBT was associated with longer RFS (P = 0.009). When stratified by risk groups, in intermediate-risk patients, the difference in RFS between the groups was not statistically significant (P = 0.434). By contrast, for high-risk patients, the treated group exhibited a better prognosis compared to the non-treated group (85.6% vs. 77.6%, P = 0.007). In both univariate and multivariate COX regression analyses, after adjusting for clinical factors such as tumor stage and tumor grade, the IVC between the primary and second TURBT remained an independent prognostic factor for NMIBC patients (HR 0.571, 95% CI [0.380, 0.859], p = 0.007). IVC treatment administered between the primary and second TURBT has been demonstrated to enhance RFS of high-risk NMIBC patients undergoing BCG treatment, whereas it is not applicable to intermediate-risk patients.
Similar content being viewed by others
Introduction
Bladder cancer is the tenth most malignant tumor globally and can be classified into muscle-invasive and non-muscle-invasive bladder cancer (NMIBC) based on TNM staging1,2. NMIBC includes the pTa, pT1, and pTis stages, with tumors confined to the mucosa or submucosa accounting for approximately 75% of all bladder cancer. Compared with muscle-invasive bladder cancer, NMIBC has a better prognosis, and the treatment regimen is different. Transurethral resection of a bladder tumor (TURBT) is the standard treatment for NMIBC, frequently performed in conjunction with postoperative intravesical chemotherapy (IVC) or intravesical Bacillus Calmette-Guérin (BCG) immunotherapy3. The benefits of maximal TURBT for NMIBC are well documented, and surgical removal of all visible tumors is the cornerstone of NMIBC treatment3,4,5. However, it has been reported that approximately 17–67% of patients with stage Ta and 20–71% of patients with stage T1 still have residual tumors after the initial TURBT, which are mostly located at the initial resection site6. These residual tumors worsen patient prognosis, further emphasizing the importance of TURBT7.
Current guidelines for the treatment of NMIBC recommend a second TURBT at 2–6 weeks after the initial TURBT in patients with stage T1 and high-grade Ta cancer3,8,9. The objectives of re-TURBT are to guarantee complete removal of the initial tumor, reduce the patient’s tumor burden, and enhance the quality of the pathological specimen10. Numerous studies have shown that a second TURBT improves the prognosis of NMIBC patients7,11,12,13. Patients who meet the criteria for a second TURBT usually also fulfil the criteria for BCG medication3. Therefore, theoretically, patients with NMIBC who undergo a second TURBT should also receive postoperative BCG immunotherapy.
IVC directly kills intraoperatively disseminated tumor cells and residual tumor cells in trauma, and an immediate single instillation within 24 h after TURBT has been shown to reduce the rate of disease recurrence in patients with NMIBC14,15,16. However, there is no consensus as to whether continuing IVC therapy between the first and second TURBT improves the prognosis of patients with NMIBC treated with BCG. Therefore, this study aimed to investigate whether IVC applied between the first and second TURBT improves the prognosis of patients with NMIBC treated with BCG.
Materials and methods
Study population
Patients with NMIBC who underwent a second TURBT and subsequent BCG treatment between January 2012 and December 2023 at the Affiliated Hospital of Xuzhou Medical University were retrospectively analyzed. All methods in this study were carried out in strict accordance with the relevant guidelines and regulations3. The inclusion criteria were as follows: (1) pathological diagnosis of uroepithelial carcinoma of the bladder after TURBT, with pathological stage pTa, pTis, or pT1; (2) a second TURBT at our hospital 2–6 weeks after the first TURBT; (3) IVC treatment within 24 h after the first and second TURBT; and (4) intravesical BCG immunotherapy after the second TURBT. The exclusion criteria were as follows: (1) patients with incomplete or missing information, (2) patients whose first or second TURBT was not performed at our hospital, (3) patients with low-risk and very high-risk tumors, and (4) patients with other potential comorbidities. The patients were divided into groups A and B according to whether they received IVC treatment between the first and second TURBT, with group A being the group that received IVC treatment and group B being the group that did not receive IVC treatment. The endpoint was recurrence-free survival (RFS), defined as the time interval between the second TURBT and disease recurrence.
Treatment schedule
During the second TURBT, all visible tumors and scars were removed. An immediate single instillation was performed within 24 h for both the initial and second TURBT. The main chemotherapeutic agents used for intravesical chemotherapy after TURBT in our hospital are pirarubicin and epirubicin (pirarubicin or epirubicin, 40 mg dissolved in 40 mL of sterile injectable water, was injected into the empty bladder through a sterile catheter and retained for 0.5 2 h). Between the initial and second TURBT, the treatment group received weekly IVC treatment after an immediate single instillation, and the non-treatment group received no additional IVC treatment after an immediate single instillation. The BCG regimen was started at least 2 weeks after the second TURBT, once a week for the first eight sessions and once a month for the next ten sessions. After the second resection, follow-ups were performed every three months for two years; every six months for the following three years; and annually thereafter. Follow-up included urine cytology, radiological imaging, and cystoscopy.
Clinical and pathological information
The collected clinicopathological data included age, gender, body mass index (BMI), smoking history, hematuria history, tumor stage, tumor grade, tumor number, maximum tumor diameter, surgical intervals, residual tumor, and IVC treatment regimen between the first and second TURBT. Pathological tumor staging was performed according to the International Union against Cancer TNM staging system (8th edition, 2017), whereas tumor grading was performed according to the 2004 World Health Organization bladder cancer grading system. The highest pathological stages and grades after the initial and second TURBT were included in this study. All pathological specimens, especially those obtained before 2017, were reassessed by a specialized bladder cancer pathologist.
Statistical analysis
Categorical variables of the demographic and clinicopathological characteristics of the two groups are expressed as numbers and percentages and compared using the χ2 test. For continuous variables expressed as means and standard deviations, the t-test was used for comparisons. Kaplan–Meier survival curves for patients were plotted and compared using log-rank tests. Univariate and multivariate Cox regression analyses were conducted to ascertain independent risk factors associated with patient prognosis. The results were expressed as 95% confidence intervals (CI) and hazard ratios (HR). All statistical analyses were performed using SPSS (version 26.0; IBM Corporation, Armonk, NY, USA) and R 4.2.3 (https://www.R-project.org). All p-values were two-sided, and p < 0.05 was considered statistically significant.
Results
Demographic and clinicopathological characteristics
Altogether, 292 patients were included with a median follow-up of 91 months (Fig. 1), all the patients were treated with adequate BCG therapy. In all, 164 patients who received IVC treatment between the initial and second TURBT were included in Group (A) A total of 128 patients who did not receive IVC treatment between the initial and second TURBT were included in Group (B) There were no statistically significant differences in the variables between the groups (Table 1). According to the EAU NMIBC prognostic factor risk groups, 64 patients (39%) were at intermediate risk, and 100 patients (61%) were at high risk in group A. In group B, 52 patients (40.6%) were at intermediate risk and 76 patients (59.4%) were at high risk.

Patient flow chart.
Kaplan–Meier survival analysis
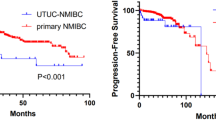
At the end of the study, 96 (32.8%) experienced tumor recurrence: 49 (29.9%) patients in group A and 47 (36.7%) patients in group B. Among all patients, there was a statistically significant difference in RFS after the second TURBT between Group A and Group B (p = 0.009) (Fig. 2). The 5-year RFS rates were 87.2 and 81.8% in Groups A, and B, respectively. In intermediate-risk NMIBC patients, the difference in postoperative RFS between the two groups was not significant (p = 0.434) (Fig. 3). The 5-year RFS rates in Groups A and B were 89.6 and 88.0%, respectively. In high-risk NMIBC patients, the 5-year postoperative RFS was higher in the treatment group than in the non-treatment group (85.6 vs. 77.6%, p = 0.007) (Fig. 4).

Recurrence-free survival (RFS) curve for both groups in all NMIBC patients.

Recurrence-free survival curve (RFS) for both groups in intermediate-risk NMIBC patients.

Recurrence-free survival (RFS) curve for both groups in high-risk NMIBC patients.
Univariate and multivariate Cox regression analyses for RFS
In the univariate analysis, pathology T stage (p = 0.002), pathology grade (p = 0.041), IVC between the primary and second TURBT (p = 0.010), and residual tumor (p = 0.017) were significantly associated with patients’ postoperative RFS. After adjusting for the above confounders, multivariate analysis showed that pathology T stage (HR 2.445, 95% CI [1.117,5.353], p = 0.025) and receiving IVC between the primary and second TURBT (HR 0.571, 95% CI [0.380,0.859], p = 0.007) remained as independent risk factors for postoperative RFS in NMIBC patients (Table 2).
Discussion
In this study, we analyzed the prognostic impact of IVC transplantation between primary and second TURBT in patients with NMIBC treated with BCG. Furthermore, we conducted an in-depth analysis of its prognostic value in the different risk subgroups. Our findings indicate that IVC treatment between the primary and second TURBT is an effective intervention for improving the prognosis of high-risk patients with NMIBC treated with BCG. However, for patients with intermediate-risk NMIBC, IVC treatment before the second TURBT did not reduce the tumor recurrence rate, and unnecessary instillation treatments could be avoided in these patients.
TURBT is regarded as a low-risk procedure, and complete resection of all visible tumors is the cornerstone of NMIBC treatment and has been endorsed by various clinical treatment guidelines3,8,9,10. The benefits of maximal TURBT for NMIBC are well documented17. The rate of residual tumors in the first TURBT ranges from 4 to 78%, depending on the tumor stage, tumor number, and operator technique18,19. A second TURBT is effective in improving the prognosis of NMIBC and is usually performed 2–6 weeks after the initial TURBT10. A systematic review by Cumberbatch et al. included one randomized controlled trial and 30 non-randomized controlled trials, which provided an in-depth analysis of the efficacy of a second TURBT for NMIBC6. The study data showed that the disease recurrence rate for patients with stage Ta tumors was 16% for those who underwent a second TURBT and 58% for those who did not. For patients with stage T1 tumors, the recurrence rate was 45% for those who underwent a second TURBT and 49% for those who did not. These results further confirm the effectiveness of a second TURBT in reducing disease recurrence, especially in patients with stage Ta tumors. IVC can directly kill tumor cells, and immediate single instillation after TURBT can significantly reduce the recurrence rate of NMIBC14,15,16,20. Except for patients with contraindications to immediate single instillation after surgery, all patients with NMIBC should be treated with immediate intravesical chemotherapy within 24 h after TURBT3. However, there is no consensus on the need for further IVC treatment after primary TURBT and secondary TURBT. To the best of our knowledge, this is the first medical center to conduct this study.
The efficacy of BCG immunotherapy in patients with NMIBC is remarkable, particularly in intermediate- and high-risk patients21,22,23. A recent systematic review of real-world evidence from studies on patients with high-risk NMIBC revealed significant variations in survival, with five-year RFS ranging from 17 to 89% and progression-free survival (PFS) ranging from 58–89%24. Further findings suggest that patients who receive intravesical BCG therapy have longer survival times25,26. Specifically, for patients with intermediate-risk NMIBC, the five-year survival results were particularly promising, with RFS and PFS rates of 86 and 100%, respectively. For high-risk patients, these figures were 72 and 91%, respectively27. Similar to the above findings, in our study, the five-year RFS rates of patients with intermediate- and high-risk NMIBC were 88.8 and 82.2%, respectively. Of particular note, we found that for high-risk patients, IVC treatment between the primary and second TURBT significantly improved five-year RFS, from 77.6 to 85.6% (p = 0.007).
The results of this study can be analyzed at two levels. First, we speculate that the presence of post-TURBT trauma may enhance the killing effect of the IVC on residual tumors. However, over time, epithelial tissue formation and scarring can weaken the tumor-killing effect of the drug. The efficacy of an immediate single instillation after TURBT for NMIBC is widely accepted and used in all patients with NMIBC3. A systematic review conducted by Tabayoyong et al., which comprehensively analyzed 16 randomized controlled trials, found no significant benefit in terms of recurrence, progression, or survival with maintenance intravesical chemotherapy compared with induction chemotherapy alone, further emphasizing the importance of early IVC treatment28. In addition, owing to the different tumor burdens of intermediate- and high-risk patients, the intensity of drug therapy they require postoperatively also differs. These findings suggest that tumor recurrence in patients with NMIBC tends to occur at the site of primary TURBT6, which may be because of incomplete surgical resection, resulting in tumor cells remaining in the bladder and regrowth. It is also possible that surgical trauma creates conditions for tumor implantation, thereby increasing the risk of recurrence. In high-risk patients with NMIBC, multiple resections of the tumor in a single operation are often required to achieve complete tumor removal, owing to deeper tumor growth or larger and more numerous tumors. This may have led to the spread of tumor cells within the bladder. Furthermore, larger trauma increases the risk of tumor cell replantation within the bladder, making it difficult to completely eradicate all tumor cells with a single IVC treatment. Therefore, increasing the number of IVC treatments before wound healing may help eliminate residual cancer cells more effectively. By contrast, intermediate-risk patients have a lower tumor burden, and surgery usually results in more complete and less invasive removal of the tumor. An immediate single postoperative instillation and subsequent BCG therapy are effective. Additional IVC therapy may not provide significant benefits but may result in undesirable side effects. Currently, some of the discussions on this aspect are partly based on the observed trends in clinical practice and the limited clues from relevant previous studies. In the future, large-scale targeted clinical trials will still be needed to conduct a comprehensive verification.
This study is the first to investigate the potential benefits of IVC applied in primary and secondary TURBT for patients with NMIBC. During the patient selection phase, we excluded patients with NMIBC who did not receive BCG therapy after the second TURBT. This was because we believe that, in addition to incomplete resection or pathology specimens that do not show muscle layers, patients with NMIBC who undergo a second TURBT should theoretically also receive postoperative BCG. Furthermore, considering the impact of factors such as tumor stage, grade, and size on prognosis, we conducted a subgroup analysis of NMIBC patients according to the EAU NMIBC prognostic factor risk groups to make the experimental results more reasonable. Two treatment options were provided to patients with NMIBC who were expected to undergo a second TURBT and subsequent BCG treatment, thereby facilitating the management of the patients’ disease for surgeons. However, this study has some limitations. First, it should be noted that this was a retrospective study, and that the non-randomized design may allow for some potential bias on the part of surgeons in the way they treat their patients. Second, as this was a single-center study, the sample size was relatively small, which may have some bias in our final results. In the future, it would be beneficial for prospective studies with larger samples to validate our findings. Finally, because the second TURBT was performed within a certain timeframe, the number of IVC treatments varied. Furthermore, chemotherapeutic agents used for IVC have not been standardized. These factors may have affected the experimental results. Future research initiatives will focus on IVC treatment for NMIBC. We will execute a multicenter, large-sample prospective study, collaborating with leading professional medical centers to pool resources and enlarge the sample size, thereby enhancing the robustness of the results. Simultaneously, we will establish a standardized diagnostic and treatment protocol. This involves precisely defining the parameters of IVC chemotherapy drugs and detailing the TURBT operational procedures. We aim to mitigate the impact of variability, standardize treatment application, enhance patient prognoses, and furnish a solid foundation for this field of study.
Conclusions
IVC treatment between the primary and second TURBT reduces the rate of tumor recurrence in high-risk NMIBC patients treated with BCG. However, it is not applicable for intermediate-risk NMIBC, and unnecessary IVC treatment can be avoided in these patients.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Change history
23 April 2025
A Correction to this paper has been published: https://doi.org/10.1038/s41598-025-98177-8
References
Jubber, I. et al. Epidemiology of bladder Cancer in 2023: A systematic review of risk factors. Eur. Urol. 84(2), 176–190 (2023).
Bray, F. et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA-Cancer J. Clin. 68(6), 394–424 (2018).
Babjuk, M. et al. European Association of Urology Guidelines on non-muscle-invasive bladder Cancer (Ta, T1, and carcinoma in situ). Eur. Urol. 81(1), 75–94 (2022).
Teoh, J. Y. et al. An international collaborative consensus statement on en bloc resection of bladder tumorincorporating two systematic reviews, a two-round delphi survey, and a consensus meeting. Eur. Urol. 78(4), 546–569 (2020).
Richterstetter, M. et al. The value of extended transurethral resection of bladder tumor(TURBT) in the treatment of bladder cancer. BJU Int. 110(2 Pt 2), E76–E79 (2012).
Cumberbatch, M. et al. Repeat transurethral resection in non-muscle-invasive bladder cancer: A systematic review . Eur. Urol. 73(6), 925–933 (2018).
Hashine, K. et al. Results of second transurethral resection for high-grade T1 bladder cancer. Urol. Ann. 8(1), 10–15 (2016).
Flaig, T. W. et al. NCCN guidelines(R) insights: Bladder cancer, version 2.2022. J. Natl. Compr. Cancer Netw. 20(8), 866–878 (2022).
Chang, S. S. et al. Diagnosis and treatment of non-muscle invasive bladder cancer: AUA/SUO Guideline. J. Urol. 196(4), 1021–1029 (2016).
Jin, Y. H. et al. Treatment and surveillance for non-muscle-invasive bladder cancer: A clinical practice guideline (2021 edition). Mil. Med. Res. 9(1), 44 (2022).
Eroglu, A., Ekin, R. G., Koc, G. & Divrik, R. T. The prognostic value of routine second transurethral resection in patients with newly diagnosed stage pT1 non-muscle-invasive bladder cancer: Results from randomized 10-year extension trial. Int. J. Clin. Oncol. 25(4), 698–704 (2020).
Gordon, P. C., Thomas, F., Noon, A. P., Rosario, D. J. & Catto, J. Long-term outcomes from re-resection for high-risk non-muscle-invasive bladder cancer: A potential to rationalize use . Eur. Urol. Focus 5(4), 650–657 (2019).
Lee, K., Jeong, S. H., Yoo, S. H. & Ku, J. H. Evaluating the efficacy of secondary transurethral resection of the bladder for high-grade Ta tumors. Investig. Clin. Urol. 63(1), 14–20 (2022).
Bosschieter, J. et al. Value of an immediate intravesical instillation of Mitomycin C in patients with non-muscle-invasive bladder cancer: A prospective multicentre randomised study in 2243 patients. Eur. Urol. 73(2), 226–232 (2018).
Messing, E. M. et al. Effect of Intravesical Instillation of Gemcitabine vs saline immediately following resection of suspected low-Grade non-muscle-invasive bladder cancer on tumor recurrence: SWOG S0337 randomized clinical trial. JAMA-J. Am. Med. Assoc. 319(18), 1880–1888 (2018).
Sylvester, R. J. et al. Systematic review and individual patient data meta-analysis of randomized trials comparing a single immediate instillation of chemotherapy after transurethral resection with transurethral resection alone in patients with stage pTa-pT1 urothelial carcinoma of the bladder: Which patients benefit from the instillation?. Eur. Urol. 69(2), 231–244 (2016).
Bree, K. K. et al. Repeat transurethral resection of muscle-invasive bladder cancer prior to radical cystectomy is prognostic but not therapeutic. J. Urol. 209(1), 140–149 (2023).
Brauers, A., Buettner, R. & Jakse, G. Second resection and prognosis of primary high risk superficial bladder cancer: Is cystectomy often too early?. J. Urol. 165(3), 808–810 (2001).
Brausi, M. et al. Variability in the recurrence rate at first follow-up cystoscopy after TUR in stage Ta T1 transitional cell carcinoma of the bladder: A combined analysis of seven EORTC studies. Eur. Urol. 41(5), 523–531 (2002).
Sylvester, R. J., Oosterlinck, W. & van der Meijden, A. P. A single immediate postoperative instillation of chemotherapy decreases the risk of recurrence in patients with stage Ta T1 bladder cancer: A meta-analysis of published results of randomized clinical trials. J. Urol. 171(6 Pt 1), 2186–2190 (2004).
Han, J., Gu, X., Li, Y. & Wu, Q. Mechanisms of BCG in the treatment of bladder cancer-current understanding and the prospect. Biomed. Pharmacother. 129, 110393 (2020).
Marttila, T. et al. Intravesical Bacillus calmette-guerin versus combination of epirubicin and interferon-alpha2a in reducing recurrence of non-muscle-invasive bladder carcinoma: FinnBladder-6 study. Eur. Urol. 70 (2), 341–347 (2016).
Shang, P. F. et al. Intravesical bacillus calmette-guerin versus epirubicin for Ta and T1 bladder cancer. Cochrane Datab. Syst. Rev. 11(5), CD6885 (2011).
Musat, M. G. et al. Treatment outcomes of high-risk non-muscle invasive bladder cancer (HR-NMIBC) in real-world evidence (RWE) studies: Systematic literature review (SLR). ClinicoEcon. Outcome Res. 14, 35–48 (2022).
Matulay, J. T. et al. Contemporary outcomes of patients with nonmuscle-invasive bladder cancer treated with bacillus calmette-guerin: Implications for clinical trial design. J. Urol. 205(6), 1612–1621 (2021).
Kamat, A. M. et al. Definitions, end points, and clinical trial designs for non-muscle-invasive bladder cancer: Recommendations from the international bladder cancer group. J. Clin. Oncol. 34(16), 1935–1944 (2016).
Grabe-Heyne, K. et al. Intermediate and high-risk non-muscle-invasive bladder cancer: An overview of epidemiology, burden, and unmet needs. Front. Oncol. 13, 1170124 (2023).
Tabayoyong, W. B. et al. Systematic review on the utilization of maintenance intravesical chemotherapy in the management of non-muscle-invasive bladder cancer. Eur. Urol. Focus 4(4), 512–521 (2018).
Acknowledgements
Everybody who made a contribution to the research has been listed as an author.
Funding
No.
Author information
Authors and Affiliations
Contributions
Z, Wand H conceived the study, participated in its design, performed the statistical analysis, and drafted the manuscript. Zewei W, Y and L helped to collect the data and performed the statistical analysis. All authors contributed to the article and approved the submitted version.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Ethics approval and consent to participate: This retrospective study was approved by the Ethics Committee of the Affiliated Hospital of Xuzhou Medical University (XYFY2022-KL340). All patients provided written informed consent.
Consent for publication
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this Article was revised: The original version of the Article contained an error in the Author Information. “Zhen Li, Zewei Wang, Yang Liu, Lei Yang and Ling Gu contributed equally to this work.” now reads: “Zhen Li, Zewei Wang and Yang Liu contributed equally to this work.”
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, Z., Wang, Z., Liu, Y. et al. IVC treatment between primary and second TURBT may improve the prognosis of high-risk NMIBC patients receiving BCG treatment. Sci Rep 15, 4874 (2025). https://doi.org/10.1038/s41598-025-89008-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-89008-x
