
Abstract
Elderly adults with hip fractures are particularly vulnerable to perioperative pulmonary complications (POPCs) throughout the surgical process. While most studies have focused on predicting postoperative pulmonary complications (PPCs), there has been a lack of focus on preoperative and intraoperative phases. To address this gap, this bidirectional cohort study aims to develop and validate a predictive model for POPCs across all surgical stages in elderly patients with hip fracture. This study will involve 3481 patients, with 1914 in the retrospective dataset and 1567 in the prospective dataset, and will analyse 44 perioperative risk factors. LASSO and multiple logistic regression will be used to identify key predictors, and nomogram prediction models will be constructed via the RMS packages. The accuracy and variability of the model will be assessed using receiver operating characteristic (ROC) curve analysis and calibration plots. The primary outcome measure is the incidence of pulmonary complications from hospital admission to 30 days post-surgery, and the secondary outcomes include complications such as heart failure, myocardial infarction, renal failure, deep venous thrombosis, stroke, and death within 30 days post-surgery. This study aims to construct a comprehensive model for predicting POPCs in this patient population and verify its accuracy and ability to differentiate POPCs using both internal and external data.
Similar content being viewed by others

Introduction
The aging global population is increasing at an unprecedented rate, particularly in Asia and other developing countries. With this demographic shift, the incidence of hip fractures is projected to nearly triple between 2018 and 2050, with over 50% of the cases expected to occur in Asia1,2. In China, the world’s most populous nation, over 366 million people, or more than 26.1% of the population, are projected to be aged 65 years and older by 20503. This demographic change poses significant challenges to healthcare systems, especially in managing the increasing number of elderly patients at a high risk of hip fractures4.
Timely surgical intervention is critical for reducing mortality and improving functional outcomes in elderly patients with hip fractures5,6,7. However, despite the benefits of surgery, elderly patients undergoing hip fracture repair are at high risk of developing perioperative pulmonary complications (POPCs)8,9.These complications are particularly prevalent in elderly patients and substantially increase the risk of perioperative mortality8,10. The incidence of POPCs in elderly patients with hip fractures ranges from 13.9 to 33.3% depending on the underlying disease, preoperative pulmonary dysfunction, and diminished compensatory capacity11,12,13.
Current research on pulmonary complications in hip fracture surgery primarily focuses on postoperative complications (PPCs)14,15,with limited attention paid to the preoperative and intraoperative factors. Furthermore, existing predictive models primarily concentrate on postoperative outcomes, often neglecting intraoperative risk factors, and lacking specificity for elderly patients16,17,18,19. This results in a gap in the accurate identification of high-risk patients throughout the perioperative period, which is crucial for improving clinical decision making and patient outcomes.
To address these gaps, this study aimed to develop and validate a predictive model that incorporates preoperative, intraoperative, and postoperative risk factors to more accurately predict POPCs in elderly patients undergoing hip fracture surgery. By employing a combination of retrospective and prospective cohort designs, this study offers a comprehensive risk-assessment tool specifically tailored to the elderly population. The novelty of this approach lies in its holistic evaluation of perioperative risk factors, addressing the limitations of existing models, enhancing the accuracy of risk prediction, and ultimately, improving patient outcomes.
Methods
Study design overview
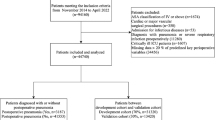
This single-center, bidirectional cohort study will include both retrospective and prospective studies. This study was approved by the Institutional Review Board of the Fengdu People’s Hospital of Chongqing (Ethical Approval ID: 2023SC0915-149) and registered with ClinicalTrials.gov (ChiCTR2300071115) on 5 March 2023 to ensure transparency and adherence to best practices. The retrospective phase spans 1 January 2017 to 31 August 2023 and the prospective phase extends from 1 September 2023 to 30 September 2024. Model development and internal validation will take place between 1 September 2023 and 30 September 2024 followed by external validation between 1 October 2024 and 31 December 2024. A total of 3667 participants from the Fengdu People’s Hospital of Chongqing, China will be recruited for the study. During the trial, participants will be evaluated for POPCs and other postoperative complications. Study assessments will be conducted at three key time points: preoperatively (day–n), intraoperatively (day 0), and postoperatively (days 1–30)20 (Fig. 1).

Flow diagram of enrolment and assessment.
Participants
Inclusion criteria
-
1.
Patients aged ≥ 65 years21.
-
2.
Radiographically confirmed hip fracture.
-
3.
Scheduling for surgical treatment of fractures.
Exclusion criteria
-
1.
Refusal to participate in the study.
-
2.
Inability to follow the study protocol due to cancellation of the procedure.
-
3.
Withdrawal was initiated by the patients or their families.
-
4.
Incomplete data or loss to follow-up for other reasons.
-
5.
Polytrauma (multiple fracture sites).
Data collection
Data will be collected in two phases, retrospective and prospective. Retrospective data will be obtained from the hospital records to provide information on patient demographics, preoperative assessments, intraoperative details, and postoperative outcomes. The data will be divided into training and validation subsets at a 7:3 ratio using the R software to facilitate model development22.
For prospective data, the collection will adhere to a standardised protocol to ensure consistency across patients. Monitoring will be performed from hospital admission until 30 days after surgery. All data will be entered into a secure, password-protected Epidata V.4.6 database with restricted access to maintain data integrity. Following data entry, information will be exported for analysis by an independent biostatistician to ensure unbiased and reliable results.
Data sources will include patient medical records, electronic health records (EHRs), and relevant clinical databases. The collection processes will ensure consistency across the retrospective and prospective phases to maintain high data quality. Six individuals, including the BT. J., JT.S., XJ.D., JH.C., L.Q., and YL.T. were included in the data-collection process. To minimize potential bias, preoperative imaging was performed and interpreted using a blinded approach, in which clinicians and radiologists were unaware of the patients’ study group allocation.
Primary objective and reporting guidelines
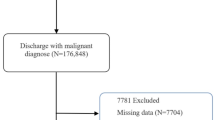
The primary objective of this study was to develop and validate predictive models for POPCs, including both the internal and external validation stages (Fig. 2). This study will strictly adhere to the reporting requirements of the Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD) framework23. To ensure consistency and rigor, Supplementary Table S1 provides detailed information on the reporting criteria and methodology.

Flow chart. LASSO least absolute shrinkage and selection operator, ROC receiver operating characteristic, DCA decision curve analysis.
Predictor variables and outcomes
Predictor variables
This study identified the key predictor variables that were clinically relevant and quantifiable. These predictors have been selected through a comprehensive review of the relevant literature, expert consensus, and their practical applicability in the clinical setting9,10,14,15,24,25,26,27,28,29,30,31. The variables will be assessed before, during, and after the surgery. The perioperative indicators are listed in Table 1.
Outcomes
Primary outcomes
This study focused on assessing POPCs from the decision to undergo surgery to 30 days after surgery or until discharge, prioritising the earlier period. It specifically considers patients released within this timeframe.
POPCs including pulmonary infection, respiratory failure, pleural effusion, atelectasis, bronchospasm, pulmonary embolism, aspiration pneumonia, acute respiratory distress syndrome (ARDS), pulmonary edema, and an unexpected need for extended mechanical ventilation8,31,32,33. Each instance of POPCs requires collaborative diagnosis based on detailed patient data, including progress notes, medical records, laboratory tests, and imaging reports. Senior radiologists will assess the perioperative images. All diagnoses will be made based on the combined opinions of the clinician and radiologist. The definitions of the POPCs are listed in Table 29,10,25,34.
Secondary outcomes
Our study will evaluate postoperative complications such as heart failure, myocardial infarction, renal failure, deep venous thrombosis, stroke, and sudden death, starting from the decision to operate and continuing until 30 days after surgery or discharge.
Sample size calculation
Retrospective cohort
To ensure robust model parameter estimation, we set the variable count to (k + 1 = 45), where (k) represents the study variable and includes 44 variables. Based on unpublished data(Supplementary Table S2), we estimated the incidence of POPCs (φ) in older patients who underwent surgery for hip fractures to be 21.43%. The sample size was calculated using Eq. (1)35.
Sample size for external validation (prospective cohort)
To ensure the accuracy of the external validation of the model, the required sample size will be calculated based on the O/E ratio (observed/expected). Debray et al. proposed the use of the delta method to compute the standard error (SE) of the O/E ratio using the following Eq. (2)36:
Recognizing that O = Nϕ, the rearranged Eq. (3) yields the minimum sample size (N) required for external validation37.
Assuming that the ϕ is 0.2143 in the population undergoing external validation and that the observed-to-expected (O/E) ratio is 1, the objective is to confirm model calibration by achieving a 95% confidence interval for O/E with a width of 0.2. The corresponding SE on the ln(O/E) scale is approximately 0.051. The sample size for external validation was determined using Eq. (4).
We estimated the loss of follow-up rate to be 10%; therefore, we increased the sample size to 1567 to allow for dropouts.
Missing data and outlier handling
Missing data
Prior to statistical analyses, we will review the initial dataset to address missing values. Variables with > 10% missing values after supplementation attempts will be excluded. If the missing value rate decreases to less than 10%, a random test will be conducted to evaluate the missingness pattern and guide subsequent actions38.
To manage different types of missingness, we will employ the following strategies39: Mean imputation will be used for completely random missing data with normal or near-symmetrical distributions; Median imputation will be applied to the right-skewed data or outliers; Multiple imputations will be performed for missing random data considering the relationships within the observed data; For data not missing at random, the‘mincemeat’package in R, which is specifically designed for such cases, will be employed.
Outlier handling
Outliers will be systematically identified and managed to maintain analysis integrity and prevent the exclusion of legitimate data points. Outliers, defined as data points significantly deviating from the overall pattern, are values beyond 1.5 × the interquartile range (IQR) from the first and third quartiles40, or with z-scores exceeding ± 3 in normally distributed data. Box plots will visually inspect outliers using the IQR method, while z-scores will identify data points more than ± 3 standard deviations from the mean41. For skewed data, outliers were defined as values outside [Q1–1.5 × IQR, Q3 + 1.5 × IQR]. The influence of outliers on model performance will be assessed using leverage analysis and Cook’s distance, excluding significant outliers with leverage greater than twice the average. Informative outliers reflecting valid variations will be retained by applying robust statistical methods, such as robust regression or log transformation, to mitigate their impact. The model’s performance will then be re-evaluated to ensure accurate variability accounting, documenting any performance metric changes in the Results section.
Statistical methods and model development
Statistical analysis
Statistical analysis will be performed via R software (version 4.0.4). Dichotomous data will be presented as percentages, and theχ²test will be used for analysis. Continuous data are shown as mean ± standard deviation or median (interquartile range, 25th–75th percentiles) based on their distribution, and t-tests or Mann-Whitney U tests will be used accordingly. A significance threshold will be established at P < 0.05, and an absolute standardised difference (ASD) over 0.118 indicated an imbalance between the development and validation groups.
Model development
-
1.
Data privacy and preliminary handling.
During the initial phase of the model development, retrospective cohort data comprising 2100 samples will be collected to train the model. The dataset will be divided into a 70% training group (n = 1470) and 30% validation group (n = 630). Critical steps to ensure data quality and privacy protection include de-identification by replacing sensitive attributes, data cleaning to correct errors, assessing outliers, and addressing missing values via established statistical methods. Descriptive statistics will be used to summarise the data distribution, and visual analysis via histograms, scatter plots, and box plots will be used to identify the patterns and anomalies. Finally, multiple imputations or mean/median imputations will be employed to address data loss and ensure the integrity of the dataset.
-
2.
Variable selection.
Least absolute shrinkage and selection operator (LASSO) and logistic regression analyses will be used to identify the key variables influencing POPCs. Significant variables will be selected based on the coefficients or p-values obtained from the regression analysis. This process is essential for eliminating redundant variables and retaining only those variables that significantly affect the prediction outcomes.
-
3.
Model construction.
A multivariate logistic regression model will be developed by using the identified variables. The Akaike information criterion (AIC) evaluates the influence of these variables by filtering out less influential factors. A nomogram prediction model will be constructed via the RMS package in the R software.
-
4.
Model validation.
The remaining 30% of the retrospective dataset, consisting of 630 samples, will be used for internal validation. The model will also be tested in a prospective cohort study to verify its effectiveness in predicting POPCs in new patient groups. The performance of the model will be rigorously evaluated via receiver operating characteristic (ROC) curve analysis, decision curve analysis (DCA), and the Hosmer–Lemeshow test. Key metrics, such as sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and area under the curve (AUC-ROC), will be used to determine the efficacy of the model. The precision and recall metrics will be used to assess the accuracy and reliability of the model in the external validation set. Prospective validation will be employed to assess the model’s performance in a real-world setting, guiding decisions regarding recalibration, replacement, or retirement of the active model based on its applicability and effectiveness.
-
5.
Model updates and maintenance.
The model will be updated periodically to incorporate new data or significant medical advancements, ensuring its accuracy and relevance by integrating the latest research and accounting for demographic changes. Updates occur annually, or when substantial new evidence emerges. Each update will undergo validation to confirm its efficacy with comprehensive documentation provided for modification and justification. Feedback from clinical practitioners could also be integrated to enhance the practical utility of the model.
Limitations
A multidisciplinary team of anaesthesiology, orthopaedic surgery, and radiology experts will use bidirectional data for model development and internal and external data validation to reduce bias and ensure study quality. Single-centre data collection may limit the generalisability of the model beyond elderly patients with hip fractures as regional characteristics and institution-specific practices could affect its applicability. The relevance of the model to different age groups and clinical conditions remains unclear. Future studies will verify the applicability of this model to multicentre data and explore the differences between the models of patients of different ages.
Ethics and dissemination
The study “Geriatric Hip Fracture Patients: Constructing and Validating a Predictive Model for Perioperative Pulmonary Complications” had been approved by the Institutional Review Board (IRB) of Fengdu People’s Hospital, Chongqing, China (Ethical Approval ID: 2023SC0915-149). The study was registered in the Chinese Clinical Trial Registry (ChiCTR.org.cn) as ChiCTR2300071115 on 5 May 2023.
This study will strictly follow the ethical guidelines, national regulations, and data protection protocols to ensure patient confidentiality and privacy. The requirement for informed consent was waived for retrospective data. In the prospective phase, written informed consent will be obtained from all participants in line with IRB approval. The study results will be published in peer-reviewed journals and presented at scientific conferences until December 2025 with the aim of enhancing the knowledge of POPCs in geriatric hip fracture patients.
Discussion
Recent studies have demonstrated that POPCs not only prolong hospital stay, but also significantly increase postoperative mortality, particularly among elderly patients with hip fractures42,43. Therefore, the timely identification of high-risk individuals is crucial to prevent adverse outcomes and improve postoperative recovery.
This study aimed to develop a comprehensive predictive risk model for POPCs in elderly patients undergoing hip fracture surgery. By incorporating risk factors from the preoperative, intraoperative, and postoperative stages, the model aimed to provide a holistic risk assessment, thereby improving the precision of POPCs prediction across the entire perioperative period.
The model will be constructed and validated using retrospective and prospective data sets. These datasets enable the identification of key risk factors across all stages of the perioperative process. A logistic regression-based approach will be employed to develop the risk model, and the results will be visually represented via a nomogram model. Internal and external data validation ensures the reliability of the model.
Despite its strengths, this model has several limitations that must be acknowledged. This included potential confounders and the single-centre nature of the study, which may have affected the generalisability of the findings. Future studies should focus on validating this model across diverse clinical settings and patient populations, to ensure its relevance and applicability. Furthermore, the incorporation of machine learning techniques and large-scale datasets could further increase the predictive accuracy and clinical utility of the model.
To the best of our knowledge, this study is one of the few to explore the effects of perioperative multistage risk factors on POPCs in elderly patients undergoing hip fracture surgery. The results of this study will have potential implications for the clinical practice of elderly patients with hip fractures.
Data availability
The data will be systematically uploaded to the ResMan Clinical Trial Public Management Platform (http://www.medresman.org.cn) within six months after study completion.
References
Ebeling, P. R. Hip fractures and aging: A Global Problem requiring coordinated global solutions. J. Bone Min. Res. 38, 1062–1063 (2023).
Chandran, M., Bhadada, S. K., Ebeling, P. R., Gilchrist, N. L. & Tiu, K. L. IQ driving QI: the Asia Pacific Consortium on osteoporosis (APCO): an innovative and collaborative initiative to improve osteoporosis care in the Asia Pacific. Osteoporos. Int. (2020).
Nations, U. World Population Prospects 2019[EB/OL],2021.
Gong, X. F. et al. Current status and distribution of hip fractures among older adults in China. Osteoporos. Int. 32, 1785–1793 (2021).
Le Manach, Y. et al. Outcomes after hip fracture surgery compared with elective total hip replacement. JAMA 314, 1159–1166 (2015).
Fullam, J., Theodosi, P. G., Charity, J. & Goodwin, V. A. A scoping review comparing two common surgical approaches to the hip for hemiarthroplasty. BMC Surg. 19, 32 (2019).
Switzer, J. A. & O’Connor, M. I. AAOS Management of Hip fractures in older adults evidence-based Clinical Practice Guideline. J. Am. Acad. Orthop. Surg. 30, e1297–e1301 (2022).
Karalapillai, D. et al. Effect of intraoperative low tidal volume vs conventional tidal volume on postoperative pulmonary complications in patients undergoing major surgery: a Randomized Clinical Trial. JAMA 324, 848–858 (2020).
Miskovic, A. & Lumb, A. B. Postoperative pulmonary complications. Br. J. Anaesth. 118, 317–334 (2017).
Fernandez-Bustamante, A. et al. Postoperative pulmonary complications, early mortality, and Hospital Stay following noncardiothoracic surgery: a Multicenter Study by the Perioperative Research Network Investigators. JAMA Surg. 152, 157–166 (2017).
Kim, S. D., Park, S. J., Lee, D. H. & Jee, D. L. Risk factors of morbidity and mortality following hip fracture surgery. Korean J. Anesthesiol. 64, 505–510 (2013).
Chang, S. C. et al. Reduction in the incidence of pneumonia in elderly patients after hip fracture surgery: an inpatient pulmonary rehabilitation program. Med. (Baltim). 97 (33), e11845 (2018).
Yakubek, G. A. et al. Chronic obstructive Pulmonary Disease is Associated with Short-Term complications following total hip arthroplasty. J. Arthroplasty. 33, 1926–1929 (2018).
Neto, A. S. et al. The LAS VEGAS risk score for prediction of postoperative pulmonary complications: an observational study. Eur. J. Anaesthesiol. 35, 691–701 (2018).
Smith, D. K. et al. D. An improved predictive model for postoperative pulmonary complications after free flap reconstructions in the head and neck. Head Neck. 43, 2178–2184 (2021).
Aragón-Benedí, C. et al. Model for predicting early and late-onset postoperative pulmonary complications in perioperative patients receiving neuromuscular blockade: a secondary analysis. Sci. Rep. 13, 5234 (2023).
Mazo, V., Sabaté, S. & Canet, J. How to optimize and use predictive models for postoperative pulmonary complications. Minerva Anestesiol. 82, 332–342 (2016).
Dankert, A. et al. Pulmonary function tests for the prediction of postoperative pulmonary complications. Dtsch. Arztebl Int. 119, 99–106 (2022).
Abd, E. et al. Predicting primary postoperative pulmonary complications in patients undergoing minimally invasive surgery for colorectal cancer. Updates Surg. 72, 977–983 (2020).
NIHR Global Health Research Unit on Global Surgery. STARSurg Collaborative. A prognostic model for use before elective surgery to estimate the risk of postoperative pulmonary complications (GSU-Pulmonary score): a development and validation study in three international cohorts. Lancet Digit. Health. 6, e507–e519 (2024).
Sen, A., Jette, N., Husain, M. & Sander, J. W. Epilepsy in older people. Lancet 395, 735–748 (2020).
Yagi, M. et al. Development and validation of machine learning-based predictive model for clinical outcome of decompression surgery for lumbar spinal canal stenosis. Spine J. 22, 1768–1777 (2022).
Collins, G. S. et al. TRIPOD + AI statement: updated guidance for reporting clinical prediction models that use regression or machine learning methods. BMJ 385, e078378 (2024).
Nijbroek, S. G., Schultz, M. J. & Hemmes, S. Prediction of postoperative pulmonary complications. Curr. Opin. Anaesthesiol. 32, 443–451 (2019).
Canet, J. et al. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology 113, 1338–1350 (2010).
Chen, Y., Wu, G., Wang, R. & Chen, J. Preoperative albumin level serves as a predictor for postoperative pulmonary complications following elective laparoscopic Gastrectomy. Curr. Pharm. Des. 24, 3250–3255 (2018).
Peng, X., Zhu, T., Chen, G., Wang, Y. & Hao, X. A multicenter prospective study on postoperative pulmonary complications prediction in geriatric patients with deep neural network model. Front. Surg. 9, 976536 (2022).
Prophylactic Penehyclidine Inhalation for Prevention of Postoperative Pulmonary. Complications in high-risk patients: a double-blind Randomized Trial: Erratum. Anesthesiology 138, 232 (2023).
Khanna, A. K. et al. R. A nomogram to predict postoperative pulmonary complications after cardiothoracic surgery. J. Thorac. Cardiovasc. Surg. 165, 2134–2146 (2023).
Wei, W. et al. Protocol for the derivation and external validation of a 30-day postoperative pulmonary complications (PPCs) risk prediction model for elderly patients undergoing thoracic surgery: a cohort study in southern China. BMJ Open. 13, e066815 (2023).
Odor, P. M., Bampoe, S., Gilhooly, D., Creagh-Brown, B. & Moonesinghe, S. R. Perioperative interventions for prevention of postoperative pulmonary complications: systematic review and meta-analysis. BMJ 368, m540 (2020).
Li, X. F. et al. Effect of ventilation mode on postoperative pulmonary complications following lung resection surgery: a randomised controlled trial. Anaesthesia 77, 1219–1227 (2022).
Gama de Abreu, M. & Sessler, D. I. Nitrous Oxide and Postoperative Pulmonary complications: conflicting evidence. Anesthesiology 138, 345–347 (2023).
Konstantinides, S. V. et al. 2019 ESC guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart J. 41, 543–603 (2020).
Riley, R. D. et al. Calculating the sample size required for developing a clinical prediction model. BMJ 368, m441 (2020).
Debray, T. P. et al. A framework for meta-analysis of prediction model studies with binary and time-to-event outcomes. Stat. Methods Med. Res. 28, 2768–2786 (2019).
Riley, R. D. et al. Minimum sample size for external validation of a clinical prediction model with a binary outcome. Stat. Med. 40, 4230–4251 (2021).
Koren, Y. et al. Respiratory effects of acute milk consumption among asthmatic and non-asthmatic children: a randomized controlled study. BMC Pediatr. 20, 433 (2020).
Enders, C. K. Missing data: an update on the state of the art. Psychol. Methods (2023).
Korhonen, O. et al. Outlier analysis for Acute blood biomarkers of moderate and severe traumatic brain Injury. J. Neurotrauma. 41, 91–105 (2024).
Hodge, V. & Austin, J. A. Survey of Outlier Detection methodologies. Artif. Intell. Rev. 22, (2004).
Yang, C. K., Teng, A., Lee, D. Y. & Rose, K. Pulmonary complications after major abdominal surgery: National Surgical Quality Improvement Program analysis. J. Surg. Res. 198, 441–449 (2015).
Epidemiology Practice of ventilation and outcome for patients at increased risk of postoperative pulmonary complications: LAS VEGAS - an observational study in 29 countries. Eur. J. Anaesthesiol. 34, 492–507 (2017).
Acknowledgements
Sthesiology Department and Professor Wenyong Shen from the Fuling District Central Hospital Gastroenterology Department for their technical assistance. We also extend our gratitude to the patients and staff for their contribution to this study.
Funding
This study will be sponsored by The Science and Technology Bureau Joint Health Bureau, Chongqing, China (2023MSXM033), and the Key Laboratory Open Fund Project of Chongqing University Cancer Hospital (cquchkfjj006). The funders and sponsors were not involved in study design, data collection, management, analysis, interpretation, writing of the report, or submission for publication.
Author information
Authors and Affiliations
Contributions
J.X.T., L.W., and S.J.B. made substantial contributions to the conceptualization and design of the study. B.T.J., J.T.S., X.J.D., J.H.C., L.Q., and Y.L.T. conducted this study.S.J.B. curated data. J.X.T. and S.J.B. conducted formal data analysis. S.J.B. and J.X.T. handled funding acquisition. J.X.T., L.W., and S.J.B. developed the study methodology. S.J.B. managed the project administration. S.J.B. wrote the original draft of the manuscript, and J.X.T. and L.W. contributed to review and editing. X.T.F. interpreted imaging data. All authors reviewed and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Patient and public involvement
The patients and the public will not be involved in the study design, conduct, reporting, or dissemination.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, L., Tian, Y., Shen, J. et al. Bidirectional cohort study protocol to construct and validate a prediction model for perioperative pulmonary complications in elderly hip fracture patients. Sci Rep 15, 6097 (2025). https://doi.org/10.1038/s41598-025-89037-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-89037-6
