
Abstract
Double-lumen tube (DLT) intubation is frequently performed for thoracic surgery, and a fiberoptic bronchoscopy (FOB) can improve the success rate of correct placement. Disposcope endoscope-guided DLT intubation was recently introduced and has a high first-attempt success rate. We tested whether compared with FOB-guided DLT intubation, disposcope endoscope-guided DLT intubation results in a non-inferior first-attempt success rate. A total of 181 patients who underwent thoracic surgery and required DLT intubation were randomly assigned to two groups: FOB guidance (FOB group) and disposcope endoscope guidance (DE group). The primary outcome was the first-attempt success rate. The secondary outcomes included the number of attempts, first intubation time, intraoperative dislodgement, and changes in the mean arterial pressure (MAP) and heart rate (HR) after intubation. The difference in the first DLT attempt success rate between the groups did not exceed the non-inferiority margin of 8% (DE group: 91.3% vs. FOB group: 89.9%; difference: 1.4%, 95% exact CI: −7.1–9.9%). The difference in the number of multiple DLT attempts also did not differ between the DE group and the FOB group (two attempts: 6.5% vs. 6.7%, P = 0.953; three attempts: 2.2% vs. 3.4%, P = 0.120). The first DLT intubation time [66 (55–86) vs. 77 (64–98) s, P = 0.010] was significantly shorter in the DE group. No significant differences were observed in the intraoperative dislodgement or changes in the MAP or HR after intubation (P > 0.05). Compared with FOB guidance, disposcope endoscope guidance provided a non-inferior first-attempt success rate and a shorter first intubation time for DLT intubation.
Similar content being viewed by others


Introduction
Double-lumen tube (DLT) are recommended as the first choice for tracheal intubation, as it is used for lung isolation during thoracic surgery1,2. However, DLT intubation can be challenging because of the large size of the tube and the angulation mismatch between the airway and endobronchial tube3,4. Multiple attempts may increase complications such as airway trauma, sore throat, hoarseness, and hypoxemia5,6. Therefore, rapid and accurate DLT intubation is particularly important7. FOB is considered the gold standard for the placement of DLT, but it takes a relatively long time8,9. Moreover, there are other disadvantages to FOB use for anesthesiologists, including unfamiliarity with the equipment, uncertain timely availability of the device, and high expenses with maintenance costs10. In addition, video double-lumen tube (VDLT) is increasingly being used for lung isolation because of the development of visualization technology, which has improved the first-attempt success rate5,11; however, VDLT increases the incidence of postoperative sore throat and hoarseness5.
The disposcope endoscope (Jiangsu Taiyuan Medical Equipment Technology Co., Ltd., Taiyuan, China) is a soft and flexible airway device that is composed of three main parts: a video monitor, a wireless transmitter, and a videostylet (Fig. 1). When the wireless transmitter is connected to the videostylet endoscope tube, the video monitor can show real-time direct visualization. In contrast to FOB, the videostylet offers the advantage of detachability from the video monitor, providing enhanced flexibility and convenience. In previous studies, compared with blind insertion, the use of a disposcope endoscope increased the success rate of DLT placement and shortened the total operation time12. However, no study has assessed the success rate of the first DLT intubation attempt with a disposcope endoscope and FOB.

Composition of the disposcope endoscope.
Considering the limited use of FOB in real-world practice, the use of disposcope endoscope guidance can be a feasible alternative for DLT intubation. We hypothesized that DLT intubation with disposcope endoscope guidance would provide a non-inferior first-attempt success rate to FOB guidance in patients undergoing thoracic surgery.
Methods
Study design and population
This single-center, non-inferiority, prospective randomized controlled study was conducted under the Declaration of Helsinki. The protocol was approved by the Ethics Committee of Deyang People’s Hospital (Ref. No. 2023-04-033-K01) on April 14, 2023, and was registered in the Chinese Clinical Trial Registry (number: ChiCTR2300071071, date of registration: May 4, 2023). All patients were enrolled between August 2023 and January 2024, and each patient provided written informed consent before entering the trial.
Patients aged 18 years or older, with American Society of Anesthesiologists (ASA) physical status I–III, who are scheduled for elective thoracic surgery requiring DLT intubation, were screened for eligibility. The exclusion criteria were as follows: emergency surgery, recent respiratory tract infection, history of thoracic, body mass index (BMI) > 35 kg m–2, presence or anticipation of airway management difficulties (such as interincisor gap < 3.0 cm, thyromental distance < 6.0 cm, abnormal range of motion of head and neck, or modified Mallampati score ≥ 3), severe liver impairment (Child-Pugh class C), congestive heart failure (New York Heart Association classification III or IV) and current maintenance dialysis.
Randomization and blinding
According to a computer-generated random number table using PASS 15.0 (NCSS LLC., Kaysville, U.T., USA), participants were randomly assigned at a 1:1 ratio to the DE group or the FOB group. The patients were unaware of the group allocation, as this assignment was concealed in an opaque and sequentially numbered envelope. An investigator not involved in the trial opened the envelope to the attending anesthetists. Anesthetists performing DLT intubation need to use disposcope endoscope or the FOB, making it impossible to blind them to group allocation. The surgeons, postoperative outcome assessors, and statisticians were also blinded to the group assignments.
Intervention and anesthesia
Demographic characteristics were obtained through the electronic medical records system. Standardized monitoring included temperature, 3-lead electrocardiography, SpO2, blood pressure, end-tidal carbon dioxide (ETCO2), the neuromuscular transmission monitoring, and the bispectral index (BIS). After preoxygenation for > 3 min, anesthesia was induced via intravenous midazolam (0.04 mg/kg), sufentanil (0.3–0.5 µg/kg), and propofol (1–1.5 mg/kg). After confirming loss of consciousness, rocuronium (0.6–1 mg/kg) was administered to facilitate DLT intubation and mask ventilation. The difficulty of mask ventilation and the use of an oropharyngeal airway were recorded. When the TOF ratio was less than 10%, DLT intubation was attempted by resident anesthetists with a collective history of more than 30 successful DLT intubations.
Images of the assembly of the disposcope endoscope and DLT are shown in Fig. 2. In the DE group, we used videolaryngoscopy to view the vocal cords. Based on the images from the video monitor, a suitable size DLT was inserted into the bronchus and adjusted to the correct location. In the FOB group, we also used videolaryngoscopy to view the vocal cords, and then the DLT was inserted into the correct location under the guidance of FOB. The correct location was defined as when the bronchial cuff had entered the dependent bronchus and was in the same plane as the carina (Fig. 3). After removing the stylet, videostylet, or FOB, the correct placement was confirmed again by auscultation in both groups. MAP and HR were recorded before DLT intubation and 1 min postintubation. After the lateral decubitus position was used, the correct placement was confirmed again by a disposcope endoscope or FOB. Intraoperative dislodgement was judged by the attending anesthetists and confirmed and adjusted to the correct location via a disposcope endoscope or FOB according to the group assignment. After surgery, the patient was confirmed to be fully conscious (BIS was at least 90) and had recovered from neuromuscular blockade, the DLT was removed, and the patient was transferred to the post-anesthesia care unit (PACU).

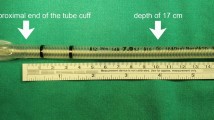
The pre-shaped double-lumen tube.

The correct placement of DE-guided DLT intubation.
Outcomes
The primary outcome was the first-attempt success rate. DLT intubation was allowed for the same anesthetist, with a 150-s time limit for the first attempt. If the DLT is not placed in the correct location, it is considered a failed attempt. Moreover, if SpO2 was reduced to < 92% during the DLT intubation attempt, rescue mask ventilation was performed until SpO2 reached 100%, and the first attempt was also considered to have failed.
The secondary outcomes included the attempt times, first DLT intubation time, intraoperative dislodgement, change in MAP after intubation, and change in HR after intubation. The first DLT intubation time was defined as the duration from the video laryngoscope passing the patient’s lips to the appropriate cuff position, and no further manipulation was needed. Intraoperative dislodgement was assessed by the anesthetist in charge, taking into account the results of the FOB or disposcope endoscope examination.
Other outcomes included sore throat and hoarseness. Thirty minutes after extubation, sore throat, or hoarseness were reported by an independent investigator or patient in a yes or no question. This uniform assessment was repeated 24 h later.
Sample size and statistical analysis
Sample size calculation was performed via PASS 15.0 (NCSS, LLC, Kaysville, Utah, USA). Based on a previous study12, the first attempt success rate of FOB-guided DLT intubation in patients undergoing thoracic surgery is 92%, and we expect a 95% first attempt success rate in the DE group. With a difference of 8% between the 2 groups and a binary outcome (success/failure), 86 patients were needed per group (α = 0.05, power = 0.90). We considered a drop-out rate of 10%, and the total number of patients was set at 99 per group.
Statistical analysis was carried out via SPSS v26.0 (IBM Corp., Armonk, N.Y., USA). Continuous data were tested for normality via the Shapiro-Wilk test and are expressed as the means ± standard deviations and medians (interquartile ranges, IQR). Continuous normally distributed variables, including age, height, weight, and BMI, were compared via Student’s t test, whereas the Mann‒Whitney and Wilcoxon tests were used for nonnormally distributed variables, such as the intubation time. Two or more proportions, including the first attempt success rate, attempt times, smoking history, degree of difficulty mask ventilation, side of surgery, and type of surgery, are expressed as numbers (proportions) and were compared via the chi-square test or Fisher’s exact test, as appropriate. We evaluated non-inferiority by comparing the difference in first DLT success rates between the DE and FOB groups in terms of proportions and 95% CIs. We then assessed whether the CI limits exceeded the predefined 8% non-inferiority margin. The decision to reject the null hypothesis was based on visual verification of whether the CI’s lower limit surpassed this margin. P < 0.05 was considered statistically significant.
Results
Among the 266 eligible patients, 42 patients were excluded according to the exclusion criteria, and 26 patients declined to participate in the study. A total of 198 patients were subsequently randomized into the two groups. After randomization, 10 patients in the FOB group were lost to follow-up because their operation was changed, or the operation was canceled, whereas 7 patients in the DE group were lost to follow-up for the same reasons (Fig. 4). The clinical characteristics of the patients did not differ between the two groups (Table 1).

CONSORT flow diagram showing patient screening, randomization, and analysis.
No significant difference was detected in the first DLT attempt success rate between the two groups (DE group: 91.3% vs. FOB group: 89.9%; difference: 1.4%, 95% exact CI: −7.1–9.9%; Table 2; Fig. 5). Because the lower limit of the 95% CI was lower than the prespecified non-inferiority margin (δ = 8), non-inferiority was established between the two groups (Fig. 5). The number of patients who needed 2 attempts was not significantly different between the two groups (6.5% vs. 6.7%, P = 0.953). The DE group included two patients (2.2%), and the FOB group included three patients (3.4%), where DLT intubation was achieved after the third attempt (P = 0.120). Compared with the FOB group, the DE group had a significantly shorter time to first DLT intubation [66 (55–86) vs. 59.0 (64–98) s, P = 0.01]. Compared with those in the FOB group, no significant differences were observed in terms of intraoperative dislodgement or changes in the MAP or HR after intubation (P > 0.05) (Table 2).

Non-inferiority graph of the first DLT attempt success rate between the FOB group and the DE group. The error bars indicate the 95% CIs of proportional differences. The dotted line represents the margin of non-inferiority. The nontinted area indicates the zone of inferiority.
No significant differences were detected in postoperative hoarseness or sore throat between the DE and FOB groups within 30 min and 24 h postoperatively (P > 0.05) (Table 3).
Discussion
In our study, which compared the use of a disposcope endoscope and FOB to assist DLT intubation, we found that the use of disposcope endoscope guidance provided a high first-attempt success rate of DLT intubation, which was equivalent to that of FOB guidance. However, disposcope endoscope guidance was associated with a shorter first DLT intubation time. There was no significant difference in the number of multiple DLT attempts, intraoperative dislodgement, or changes in the MAP and HR after intubation.
Given the challenging nature of DLT intubation and its role in managing thoracic surgery, reliable tools for accurately assisting DLT intubation are crucial13,14,15. FOB and auscultation are the traditional positions of DLT intubation, and FOB has been accepted as the gold standard for DLT intubation16. However, owing to the large number of procedures and the need for cleaning, in many clinical situations, FOB is not available in time. In contrast, the disposcope endoscope has recently been used in patients undergoing thoracic surgery and has advantages, including being easy to use and not requiring an assistant12. Although a previous study indicated that disposcope endoscope guidance can offer clinical usefulness for DLT intubation, there is still a lack of clear evidence compared with FOB-guided DLT intubation12. To our knowledge, this is the first prospective randomized trial that examines this clinical question by comparing DLT intubation via FOB with the use of a disposcope endoscope.
Our study revealed a first-attempt success rate of 91.3% for disposcope endoscope-guided DLT intubation, which is equal to the 89.9% success rate for assisting DLT intubation with FOB. The disposcope endoscope is the same as FOB, allowing for real-time visualization of every step in the placement of the DLT and enabling seamless adjustments during the insertion process17,18. Consequently, these properties of disposcope endoscope guidance likely led to a non-inferior success rate compared with that of FOB guidance in this study. The shorter first DLT intubation time of disposcope endoscope guidance for DLT intubation shown in this study may be explained in two ways. First, the lens of the FOB may come out through the tip of the DLT, making it susceptible to contamination by airway secretions, whereas the lens of the disposcope endoscope used in this study does not overtop its tip, thus avoiding direct contact with secretions and reducing the time required for lens cleaning. Second, the operation of disposcope endoscope guidance does not require an assistant, reducing the time required for coordination. Therefore, we believe that disposcope endoscope guidance should be considered an alternative tool for DLT intubation considering several limitations of FOB in clinical practice, the high success rate, and several advantages of disposcope endoscope guidance.
With the advancement of visualization technology, many visualization devices are increasingly used for lung isolation7,13,19,20, with video DLT being the most popular5,21. In previous studies, the VDLT has been shown to play a beneficial role22; however, it has also been linked to increased incidences of sore throat and hoarseness. Moreover, there is a substantial cost difference between VDLT and common DLT, and VDLT cannot completely avoid the use of a FOB, which may increase FOB-associated costs10. Owing to its high cost (about $200 in another hospital in our country), VDLT has not been integrated into clinical practice in our country. In our study, the high first-attempt success rate suggests that confirmation of DLT placement via the VDLT is not necessary when a disposable endoscope is used, which can reduce both the overall cost, as the VDLT is an expensive procedure, and the postoperative sore throat and hoarseness associated with VDLT placement.
The relatively low first-attempt success rate of disposcope endoscope and fiber-copic DLT intubation in this study compared with previous data12,13 may be due to three reasons. First, there was a clear definition of failed DLT intubation attempts in our studies (allowing us to continue for 150 s unless SpO2 decreased to < 92%). Second, simply withdrawing the DLT from the mouth for any reason was considered a failed attempt. Third, we chose to place the DLT on the nonoperative side, contrary to previous studies that preferred the left side for DLT placement23. Placement of the DLT on the right may be recorded as a first attempt failure due to prolonged positioning time. Therefore, the first attempt success rate of DLT intubation was relatively low in our study.
We assessed other outcomes (including intraoperative dislodgement, changes in mean arterial pressure, and heart rate after intubation) and the frequency of complications such as postoperative sore throat and hoarseness. The results revealed no significant difference between the groups because the interventions after intubation were consistent in both groups, and no additional extracavitary procedures were performed.
Our study had several limitations. First, the results may have been biased because the anesthetists performing DLT intubation could not be blinded to the group allocation. Second, we did not differentiate between glottis visualization time and auscultation time, as these interventions were consistent between the two groups. Third, we did not investigate the success rates of anesthetists with varying levels of experience, nor did we examine patients with challenging airways. Fourth, the study was conducted at a single center, and larger clinical trials including more patients from multiple centers are needed to confirm the findings reported here.
Conclusion
In conclusion, the results of our non-inferiority trial demonstrated that real-time disposcope endoscope guidance provides a similar success rate to FOB guidance for DLT intubation. Moreover, the use of disposcope endoscope-guided DLT intubation was superior in reducing the time to the first DLT intubation attempt. These findings suggest that disposcope endoscope guidance may be considered an alternative method for DLT intubation.
Data availability
The datasets generated are available from the corresponding author upon reasonable request.
Abbreviations
- DLT:
-
Double-lumen tube
- FOB:
-
Fiberoptic bronchoscope
- DE:
-
Disposcope endoscope
- MAP:
-
Mean arterial pressure
- HR:
-
Heart rate
- VDLT:
-
Video double-lumen tube
- BMI:
-
Body mass index
- ASA:
-
American Society of Anesthesiologists
- ETCO2 :
-
End-tidal carbon dioxide
- TOF:
-
Train-of-four
- BIS:
-
Bispectral index
- PACU:
-
post-anesthesia care unit
References
Risse, J. et al. Videolaryngoscopy versus direct laryngoscopy for double-lumen endotracheal tube intubation in thoracic surgery - a randomised controlled clinical trial. BMC Anesthesiol. 20, 150 (2020).
Xiang, Y-Y., Chen, Q., Tang, X-X. & Cao, L. Comparison of the effect of double-lumen endotracheal tubes and bronchial blockers on lung collapse in video-assisted thoracoscopic surgery: a systematic review and meta-analysis. BMC Anesthesiol. 22, 330 (2022).
Ishibashi, H. et al. Extubation by supraglottic airway after lobectomy prevents cough-associated air leaks and prolonged coughing or sore throat. Eur. J. Cardio-Thoracic Surgery: Official J. Eur. Association Cardio-Thoracic Surg. 63, ezad158 (2023).
Cameron, R. B., Peacock, W. J., Chang, X. G., Shin, J. S. & Hoftman, N. Double lumen endobronchial tube intubation: lessons learned from anatomy. BMC Anesthesiol. 24, 150 (2024).
Shui, W. et al. The effects of video double-lumen tubes on intubation complications in patients undergoing thoracic surgery: a randomised controlled study. Eur. J. Anaesthesiol. 41, 305–313 (2024).
Park, J-W. et al. Comparison of conventional and fibreoptic-guided advance of left-sided double-lumen tube during endobronchial intubation: a randomised controlled trial. Eur. J. Anaesthesiol. 37, 466–473 (2020).
Hsu, H-T. et al. Cheng K-I. Trachway® flexible stylet facilitates the correct placement of double-lumen endobronchial tube: a prospective, randomized study. BMC Anesthesiol.22, 260 (2022).
Matek, J., Kolek, F., Klementova, O., Michalek, P. & Vymazal, T. Optical devices in Tracheal Intubation-State of the art in 2020. Diagnostics (Basel Switzerland). 11, 575 (2021).
Palaniappan, D., Friedlander, D. & Desai, A. Is it time to reconsider the routine blind insertion of double lumen endobronchial tubes? J. Clin. Anesth. 79, 110766 (2022).
Onifade, A. et al. Comparing the rate of fiberoptic bronchoscopy use with a video double lumen tube versus a conventional double lumen tube-a randomized controlled trial. J. Thorac. Disease. 12, 6533–6541 (2020).
Wang, W. et al. Hypoxemia in thoracoscopic lung resection surgery using a video double-lumen tube versus a conventional double-lumen tube: a propensity score-matched analysis. Front. Surg. 10, 1090233 (2023).
Chen, P. T. et al. A randomised trial comparing real-time double-lumen endobronchial tube placement with the Disposcope® with conventional blind placement. Anaesthesia72, 1097–1106 (2017).
Long, S., Li, Y., Guo, J. & Hu, R. Effect of the VivaSight double-lumen tube on the incidence of hypoxaemia during one-lung ventilation in patients undergoing thoracoscopic surgery: a study protocol for a prospective randomised controlled trial. BMJ open. 13, e068071 (2023).
Cohen, E. Current practice issues in thoracic anesthesia. Anesth. Analg. 133, 1520–1531 (2021).
Huybrechts, I., Tuna, T. & Szegedi, L. L. Lung separation in adult thoracic anesthesia. Saudi J. Anaesth. 15, 272–279 (2021).
Kang, S., Chae, Y. J., Kim, D. H., Kim, T. G. & Yoo, J. Y. Comparison of fiberoptic bronchoscopic intubation using silicone and polyvinyl chloride double-lumen tubes. Korean J. Anesthesiol.. 76, 300–306 (2023).
Yu, J., Hu, R., Wu, L., Sun, P. & Zhang, Z. A comparison between the Disposcope endoscope and fibreoptic bronchoscope for nasotracheal intubation: a randomized controlled trial. BMC Anesthesiol. 19, 163 (2019).
Yang, N., Hou, Y-B. & Yu, J-M. Awake nasotracheal intubation in a patient with ankylosing spondylitis by Disposcope endoscope: a case report. Asian J. Surg. 46, 2191–2192 (2023).
Wasem, S. et al. Comparison of the Airtraq and the Macintosh laryngoscope for double-lumen tube intubation: a randomised clinical trial. Eur. J. Anaesthesiol. 30, 180–186 (2013).
Zhang, Y. et al. Comparing the effectiveness and safety of MedAn with the Nishikawa Blade and UE Videolaryngoscopes for Left-Sided double-lumen endobronchial tube intubation: a Randomized Controlled Trial. Med. Sci. Monitor: Int. Med. J. Experimental Clin. Res. 29, e940916 (2023).
Marchant, B. E., Morris, B. N. & Royster, R. L. The video double-lumen tube: does it have a future? J. Thorac. Disease. 15, 2385–2388 (2023).
Lopez-Lopez, D., Neira-Somoza, P., Mato-Bua, R. & Pato-Lopez, O. Video double-lumen tubes: how much room for improvement can they provide? J. Thorac. Disease. 15, 960–963 (2023).
Zhou, H., Fei, Y., Zhang, Y., Quan, X. & Yi, J. Individualized rotation of left double lumen endobronchial tube to improve placement success rate: a randomized controlled trial. Respir. Res. 25, 184 (2024).
Funding
This work was supported by the Research Project on the Fine Management of Airways During Anesthesia (Grant No. RCLX2315010).
Author information
Authors and Affiliations
Contributions
Name: Wencai Jiang. Contribution: This author helped design and conduct the study, and prepare and approve the final manuscript.Name: Xinyu Zhou. Contribution: This author helped prepare and approve the final manuscript.Name: Xu Zeng. Contribution: This author helped collect and analyze the data.Name: Huawei Pang. Contribution: This author helped conduct the study.Name: Huifang Zheng. Contribution: This author helped revise the final manuscript.Name: Siyu Peng. Contribution: This author helped collect the data.Name: Yue Zhang. Contribution: This author helped collect the data.Name: Xianjie Zhang. Contribution: This author helped design and conduct the study, and prepare and approve the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Deyang People’s Hospital on April 14, 2023 (No. 2023-04-033-K01). Each patient provided written informed consent before entering the trial. This study adhered to the CONSORT guidelines, and all methods were performed under the relevant guidelines and regulations (for example, the Declaration of Helsinki).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Jiang, W., Zhou, X., Zeng, X. et al. Disposcope endoscope guidance versus fiberoptic bronchoscopy guidance for double-lumen tube intubation in patients undergoing thoracic surgery: a randomized controlled non-inferiority trial. Sci Rep 15, 5476 (2025). https://doi.org/10.1038/s41598-025-89945-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-89945-7
