
Abstract
Bladder cancer (BCa) is the second most common urological malignancy, but the techniques used today to detect and monitor BCa are frequently invasive and/or have inadequate sensitivity and specificity. Therefore, it is imperative to create a noninvasive test that is both sensitive and accurate for diagnosing BCa. This research introduces and validates the diagnostic performance of H4C6/SOX1-OT gene methylation in the diagnosis of BCa based on urine samples by designing two parts of studies: the case-control study and the prospective validation study. In the case-control study, the methylation test of H4C6/SOX1-OT achieved a sensitivity/specificity/positive predictive value (PPV)/negative predictive value (NPV) of 87.9%(95%CI, 79.4%–93.3%)/90.4%(95%CI, 80.7%–95.7%)/92.6%(95%CI, 84.8%–96.7%)/ 84.6%(95%CI, 74.3%–91.5%) (kappa value 77.6%). The sensitivities for low grade, high grade, Ta-T1, and T2-T4 were 85% (17/20), 88.6% (70/79), 85.4% (41/48) and 92.6% (25/27). Statistical analysis showed the diagnostic sensitivity of test was not affected by sex, age, tumor grade or tumor stage (P > 0.05). In the prospective validation study, the H4C6/SOX1-OT methylation test yielded an overall sensitivity/specificity/PPV/NPV of 84.8%(95%CI, 67.3%–94.3%)/90.0%(95%CI, 75.4%–96.7%)/87.5% (95%CI, 70.1%–95.9%)/84.6% (95%CI, 73.0%-95.4%) (kappa value 75.0%), indicating 38.4% of spared cystoscopy. These findings highlight the potential of the H4C6/SOX1-OT methylation in urine DNA as a promising molecular diagnostic tool for detecting BCa, especially for early-stage tumors, which may reduce the need for cystoscopy.
Similar content being viewed by others


Introduction
Bladder cancer (BCa) is the second most common urological malignancy after prostate cancer in the world, which the incidence increases with age, and it is 3 times more common in men than in women1. According to the global data in 2020, BCa has globally resulted in an estimated 573,278 new cases and approximately 212,536 deaths worldwide each year, which poses a serious threat to public health1. Among BCa patients, about 75%–80% had non-muscle-invasive cancer (NMIBC), and 70% of these tumors will recur, and 15% will progress in stage and grade2. Therefore, strict monitoring and accurate diagnoses are essential for BCa management decision-making.
Although some risk factors, such as smoking and exposure to carcinogens, have been identified, effective strategies for early detection are still not available. Visible hematuria is the most common symptom of BCa in about 80%–90% of patients, but it would be disturbed by a series of benign urinary diseases, and only 10% of hematuria patients would finally be diagnosed with BCa3,4,5. Currently, cystoscopy is the gold standard tool for BCa diagnostics containing high sensitivity but often associated with invasiveness, cost, and discomfort6,7,8. Cytology, frequently used as an adjunct to cystoscopy, is highly specific (85%–100%)9. But for diagnosis of low-grade (LG) and carcinoma-in-situ (CIS) tumors, cystoscopy lacks specificity, while cytology limits sensitivity (15%–75%)6,7,10,11,12. The US Food and Drug Administration has approved many urine-based biomarker assays to diagnose BCa, including BTA, NMP22, and the UroVysion fluorescence in situ hybridization (FISH). However, due to their low sensitivity and high false-positive rate, these markers were limited in their ability to detect BCa during the first diagnosis12,13,14,15. Considering these caveats, there is an urgent need to implement reliable, more affordable, and less invasive techniques for the diagnosis of all stages of BCa, particularly early-stage tumors, which in turn could enhance disease treatment.
Aberrant DNA methylation, a key epigenetic process that deactivates tumor suppressor or cancer-associated genes, is a prevalent molecular change in carcinogenesis and has been investigated as a potential diagnostic marker in several tumors16,17. Over the years, numerous studies have investigated aberrant urine-DNA methylation biomarkers for BCa detection, achieving favorable preliminary results18. The Bladder EpiCheck test, based on 15 DNA methylation biomarkers for surveillance of BCa recurrence using urine DNA, generated an overall sensitivity of 68.2% and specificity of 88.0%, and has been included in the European Association of Urology guidelines for clinical practice8, giving recognition to BCa diagnostics by using urine-methylation markers. However, these assays’ performance still needs to be enhanced, and routine clinical practice in Asia has not fully embraced their validation.
The gene of H4C6 (H4 Clustered Histone 6) has been reported significantly higher in bladder tumor tissue samples19. Nonetheless, there is no study about H4C6 methylation detection in urine DNA for BCa diagnosis. In this study, we tried to investigate the urine-based H4C6 methylation target combined with SOX1-OT, another marker that has been verified to distinguish patients with BCa20, and validate their diagnostic ability for patients with BCa.
Results
Study subject characteristics
The demographic characteristics of the candidates are shown in Table 1. The retrospective case-control study contained 172 cases, of which 99 (57.6%) had BCa and 73 (42.4%) formed the non-BCa group. The average age of the patients with BCa was 65.1 years (range, 40 to 85 years), which consisted of 74 (74.8%) men and 25 (25.2%) women. Of BCa cases, 20 (20.2%) were low grade cases and 79(79.8%) were high grade cases. The average age of the non-BCa group was 53.9 years (range, 23 to 86 years); and the non-BCa group consisted of 48 (65.8%) men and 25 (34.2%) women. In the validation set study, a total of 73 participants were enrolled and 33 (45.2%) had BCa and 40 (54.8%) had no BCa. The average age of the patients with BCa was 65.3 years (range, 38 to 91 years), which consisted of 25 (75.8%) men and 8 (24.2%) women. Of BCa cases, 3 (9.1%) were papillary urothelial neoplasms of low malignant potential (PUNLMP), 6 (18.2%) were low grade cases and 24 (72.7%) were high grade cases. The average age of the non-BCa group was 53.9 years (range, 24 to 84 years); and the non-BCa group consisted of 25 (62.5%) men and 15 (37.5%) women. Of total 132 BCa patients, 31 patients’ tumor stage information was missing.
Performance of H4C6/SOX1-OT methylation detection for BCa diagnosis
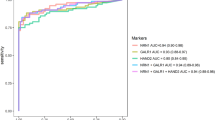
In the training set, H4C6/SOX1-OT methylation tests were proceeded in all those cases. As hematuria is a prevalent symptom of bladder malignancy, we firstly analyzed whether the relative methylation levels of H4C6 and SOX1-OT would be different between patients had hematuria and had no hematuria. Data showed that the methylation level of H4C6 and SOX1-OT between the two groups had no difference within the BCa group or the non-BCa group, indicating the methylation level of H4C6 and SOX1-OT would not be influenced by hematuria (Fig. 1A). Later, results demonstrated that the relative methylation levels of H4C6 and SOX1-OT were higher in BCa patients when compared to the methylation levels in non-BCa patients (P < 0.05) (Fig. 1B,C). Moreover, the relative methylation level of H4C6 showed higher in all stages and grades of tumors, but no difference within all stages or grades (Fig. 1B). Similar results were also seen on SOX1-OT, but tumors with T3-T4 and unknown stages were not significantly different from the control group (Fig. 1C). The ROC curve analysis revealed that the cut-off value of H4C6 and SOX1-OT were both defined as 38.0, resulting in the area under the curve (AUC) as follows: the H4C6 was 0.838 (95% CI, 0.776–0.899) and the SOX1-OT was 0.732(95% CI, 0.658–0.807) (Fig. 1D). According to the cut-off value, we defined the methylation test as positive if the Ct value of H4C6 < 38.0 and/or SOX1-OT < 38.0. Based on that rule, H4C6/SOX1-OT methylation was positive in 87/99 tumors. Compared to clinical diagnosis, H4C6/SOX1-OT methylation test based on urine-DNA yielded a sensitivity of 87.9% (87/99, 95% CI, 79.4%–93.3%), a specificity of 90.4% (66/73, 95% CI, 80.7%–95.7%), positive predictive value (PPV) of 92.6% (87/94, 95% CI, 84.8%–96.7%) and negative predictive value (NPV) of 84.6% (66/78, 95% CI, 74.3%–91.5%), respectively (kappa value 77.6%) (Table 2). The sensitivities for low grade, high grade, Ta-T1, and T2-T4 were 85.0% (17/20), 88.6% (70/79), 85.4% (41/48), and 92.6% (25/27). Statistical analysis showed the diagnostic sensitivity of test was not affected by sex, age, tumor grade or tumor stage (P > 0.05), indicating the good ability of H4C6/SOX1-OT methylation biomarkers in diagnosing BCa, including early stages (Table 3).

Results of the H4C6/SOX1-OT methylation in urine DNA using linear target enrichment followed by quantitative methylation-specific PCR in a case-control study. (A) The relative methylation levels of H4C6 and SOX1-OT in BCa and non-BCa patients with or without hematuria. The relative methylation levels of H4C6 (B) and SOX1-OT (C) in urine samples collected from training set patients. The relative methylation levels were expressed as 40-ΔCt values for each sample. A higher 40-ΔCt value indicates a higher relative methylated level of H4C6 or SOX1-OT. (D) Receiver operating characteristic (ROC) curve of H4C6/SOX1-OT for detecting all BCa from patients without BCa (including bladder benign disease and normal patients). *P < 0.05 (Kruskal-Wallis test). BCa+/-, BCa patients with hematuria/ without hematuria; Non-BCa+/-, patients without BCa had hematuria/ had no hematuria; Low, low grade; High, high grade.
Clinical validation of the H4C6/SOX1-OT methylation test for selecting BCa
To validate the performance of the H4C6/SOX1-OT methylation test in selecting BCa, the prospective study was designed and comprised samples collected from 73 patients before cystoscopy. Of the total 73 patients, 33 were diagnosed with BCa by cystoscopy/histopathology. Both the relative methylation level of H4C6 and SOX1-OT in DNA derived from urine sediment were significantly higher in patients with BCa than patients without BCa, but the results of relative methylation level within different stages or grades did not showed the same difference like in the training set maybe because of the sample size (Fig. 2A,B). Clinical performance was also analyzed according to the cut-off value of 38.0 defined in the training set. Surprisingly, in the validation set, the H4C6/SOX1-OT methylation test correctly predicted 28 of the 33 patients and yielded an overall sensitivity of 84.8% (28/33, 95% CI, 67.3%–94.3%), a specificity of 90.0% (36/40; 95% CI, 75.4%–96.7%), a PPV of 87.5% (28/32, 95% CI, 70.1%–95.9%), and a NPV of 84.6% (36/41, 95% CI, 73.0%-95.4%) with a kappa value of 75.0% (Fig. 2C; Table 4). Moreover, the methylation test probably could lead to a reduction of 38.4% in the unnecessary referral rate of cystoscopy, but further clinical data is needed for verification(Table 4). To be noted, the diagnositic sensitivity of the test still was not affected by sex, age, tumor grade, or tumor stage (P > 0.05) (Table 3). The validation part of the study further verified the ability of urine-based H4C6/SOX1-OT methylation markers in the detection of BCa, especially for early BCa.

Clinical validation of the H4C6/SOX1-OT methylation in urine DNA using linear target enrichment followed by quantitative methylation-specific PCR in a prospective study. The relative methylation levels of H4C6 (A) and SOX1-OT (B) in urine samples collected from validation set patients. The relative methylation levels were expressed as 40-ΔCt values for each sample. A higher 40-ΔCt value indicates a higher relative methylated level of H4C6 or SOX1-OT. (C) The landscape of pathological characteristics and detection results in validation cohort, including 33 cases with BCa. *P < 0.05, **P < 0.01, ****P < 0.0001 (Kruskal-Wallis test). Low, low grade; High, high grade.
Discussion
Currently, cystoscopy is still the main detection method for BCa. The lack of effective triage tools may lead to delayed diagnosis and poor prognosis. Hence, it is urgent to investigate an accurate, non-invasive and cost-effective diagnostic method with high sensitivity, PPV and NPV to ensure a low chance of missing low and early stages of tumors and to help rule out patients who could avoid unnecessary cystoscopy. Therefore, urine-based biomarker investigation attracted high attention.
In this study, we first discovered the diagnostic performance of the urine DNA-based H4C6 methylation marker on BCa by combining it with SOX1-OT. The gene relative methylated level of H4C6 based on urine sediment was significantly higher in BCa patients, but no difference was found within stages or grades, which is consistent with the previous results based on tumor tissues19. However, a published study demonstrated that the methylation level of SOX1-OT was correlated with the stages and grades of BCa when combined with the OTX1 methylation gene, whereas in our study, such a correlation relationship could not be found, which perhaps their results were shown as combined methylation levels, but not SOX1-OT or OTX1 alone20.
Several urine-based biomarkers aimed at reducing cystoscopy have been studied, and a methylation panel including several biomarkers is a common design. For example, several studies have demonstrated that ONECUT2 methylation, along with other biomarkers (2–5 markers), can successfully distinguish the BCa patients from benign illness with high sensitivity and NPV21,22,23. However, the sensitivities for low-grade tumors and Ta tumors were only 70.0% and 83.3%, respectively, when using ONECUT2 and VIM two methylation genes24. Guo et al. used a methylation panel combined with 8 markers to identify BCa, generating a sensitivity of 83% and a specificity of 60%25. Huang et al. even developed an OncoUrine assay composed of a panel of 17 gene mutations and one gene methylation biomarker to detect BCa, and the test demonstrated a sensitivity of 92.2% and an NPV of 94.1% on upper tract urinary carcinoma with hematuria26. However, multiple methylation gene detections would inevitably result in increasing patients’ expenses. In our study, the H4C6/SOX1-OT diagnostic model of BCa generated an overall sensitivity of 87.9% and a specificity of 90.4% in the modeling cohort, and similar sensitivity (84.8%) and specificity (90.0%) were also found in the validating cohort, indicating the potential diagnostic performance of this combination methylation model for BCa diagnosis.
Methods like urine cytology and FISH typically missed the early phases of BCa, which were extremely difficult to detect11,12. Therefore, it is clinically essential to detect BCa early in order to lower disease-related morbidity and mortality. Chen et al. demonstrated that the sensitivity of SOX1-OT/OTX1 for early stages of BCa was 69.2-83.3%20. Another study used PENK as methylation markers demonstrated a sensitivity of 85.7% and 76.8% for Ta-T1 and low-grade tumors, respectively27. In our study, the H4C6/SOX1-OT panel showed 85.4% and 85.0% sensitivity for early stages (Ta-T1) and low-grade BCa, respectively, indicating the capacity to identify early BCa. Furthermore, screening for biomarkers with high PPV and NPV is important to reduce needless cystoscopy, which is another pressing issue in the clinic. According to the validation set’s results in our study, the diagnosis model produced 87.5% PPV and 84.6% NPV and may be able to reduce the 38.4% rate of unnecessary referrals for cystoscopies. However, additional clinic verification is required for these data.
Nevertheless, it should be noted that there are certain limitations in this study. First, the samples tested were from a single center, and information about medical histories, such as tumor size, tumor number, smoking history, and cytology results, was not available. Second, only a small number of BCa samples were examined in the prospective validation study, which may lower the statistical power. Third, the follow-up data was unavailable in this study, and hence the performance of our diagnostic model could not be evaluated for recurrent BCa patients. Although the results in our study demonstrated that the H4C6/SOX1-OT methylation model probably could be a noninvasive diagnostic method to identify BCa early, large-scale research are still required to validate the clinical values. These shortcomings are the focus of our current and future research efforts, including conducting multicenter studies to expand the sample size and collecting follow-up data to investigate the role of H4C6/SOX1-OT gene methylation in the diagnosis of relapsed BCa patients.
Taken together, the study demonstrated the promising applications of H4C6/SOX1-OT methylation based on urine DNA in the clinical management of BCa, especially for early-stage BCa. The employment of H4C6/SOX1-OT methylation will help to reduce the frequency of cystoscopy and thus alleviate patients’ economic burden.
Methods
Study design and study population
In this research, two independent studies were designed: a retrospective case-control study for the training set and a prospective study for the validation set (Fig. 3). The case-control study contained 99 cases of BCa patients and 73 cases of non-BCa patients and the prospective clinical validation study (blinded cohort), patients (n = 73) scheduled for cystoscopy were enrolled. All cases were enrolled at Xiaolan People’s Hospital of Zhongshan, China from April 2022 to January 2023. Inclusion criteria: (a) All patients underwent standard evaluation including cystoscopy, histological evaluation to confirm the presence of BCa and the tumor’s level if presented; (b) Patients without BCa were diagnosed with urinary tract infection, urinary calculi, and benign prostatic hyperplasia; (c) All patients were older than 18 years. Exclusion criteria: (a) Important research data missing or incomplete; (b) Patients with other tumors. For the validation study, the standard evaluation results were blinded to the laboratory personnel responsible for the testing. Data analysis of the H4C6/SOX1-OT results was independently performed for comparison with the cystoscopic findings and pathology outcomes as reference standards. This study was approved by the Ethic Committee of Xiaolan People’s Hospital of Zhongshan (Reference No. ZSXL-LL2021-024). All participants in the study provided written informed consent, and the study adhered to local ethics guidelines.

Workflow indicating study design.
Urine sample collection
Fresh void urine samples (30mL for each patient) were collected before cystoscopy or surgery and stored at 4℃. Urine samples were processed within 2 h and centrifuged at 3000 g for 10 min. The resulting pelleted sediment was washed twice with phosphate-buffered saline and then stored at -80℃ until DNA extraction.
DNA extraction and conversation
Genomic DNA was extracted from the pelleted sediment using the QIAamp DNA Mini Kit (Qiagen GmbH, Hilden, Germany) following the manufacturer’s recommendations. The DNA concentrations and 260/280 ratios were measured by NanoDrop 2000 spectrophotometer (Thermo Fisher Scientific, USA), and a 260/280 ratio around 1.6–2.1 and DNA concentration no less than 30ng/µL was required for all DNA samples. The following bisulfite conversion was performed using the EZ DNA Methylation-GoldM Kit (Zymo Research, CA, USA) according to the manufacturer’s instructions, eluted in 20 µL M-Elution Buffer and stored at -80℃.
H4C6/SOX1-OT methylation detection
The quantitative methylation-specific PCR was performed using the Applied Biosystems 7500 (Thermo Fisher Scientific, USA) with the H4C6 and SOX1-OT gene methylation detection kit (Hybribro Pharmaceutical Technology Co. Ltd, Guangzhou, China) according to the manufacturer’s instructions, and the ACTB gene as reference. Ct values of H4C6, SOX1-OT and ACTB could be obtained in each sample, and the Ct value of ACTB should be between 15 and 35, otherwise would be retested. The relative level of methylated H4C6 and SOX1-OT DNA target in each samples were calculated as 40-delta Ct (ΔCt) (Ct of amplified genes-Ct of ACTB)1,27. A higher value of 40-ΔCt indicated a higher ralative methylation level of target genes.
Statistical analysis
Statistical analyses were performed using IMB SPSS Statistics 25 and illustrated with GraphPad Prism 10.1.2. The relative methylated levels of target genes in different groups were compared by one-way ANOVA test and Bonferroni’s Multiple Comparison Test. Each methylation biomarker’s performance was assessed by Receiver Operating Characteristics (ROC) curve using the Ct value. The area under the ROC curves (AUC), sensitivities, specificities and 95% confidence intervals (95%CI) were calculated to confirm the accuracy of diagnosis, sensitivity, and specificity. The Ct cutoff value of methylation was determined by the method of Youden’s index on the model ROC, which maximizes the sum of sensitivities and specificities28. Categorical data was compared by Chi-square Kappa test or Fisher exact test to evaluate the performance accuracy. P < 0.05 was considered statistically significant.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Sung, H. et al. Global Cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 71, 209–249 (2021).
Cumberbatch, M. et al. Epidemiology of bladder cancer: A systematic review and contemporary update of risk factors in 2018. Eur. Urol. 74, 784–795 (2018).
Nielsen, M., Qaseem, A. & High Value Care Task Force of the American College of Physicians &. Hematuria as a marker of occult urinary tract cancer: advice for High-Value care from the American college of physicians. Ann. Intern. Med. 164, 488–497 (2016).
Compérat, E. et al. Current best practice for bladder cancer: a narrative review of diagnostics and treatments. Lancet 400, 1712–1721 (2022).
Sarosdy, M. F. et al. Use of a multitarget fluorescence in situ hybridization assay to diagnose bladder cancer in patients with hematuria. J. Urol. 176, 44–47 (2006).
Grossman, H. B. et al. A phase III, multicenter comparison of hexaminolevulinate fluorescence cystoscopy and white light cystoscopy for the detection of superficial papillary lesions in patients with bladder cancer. J. Urol. 178, 62–67 (2007).
Fradet, Y. et al. A comparison of hexaminolevulinate fluorescence cystoscopy and white light cystoscopy for the detection of carcinoma in situ in patients with bladder cancer: a phase III, multicenter study. J. Urol. 178, 68–73 (2007). discussion 73.
Babjuk, M. et al. European association of urology guidelines on Non-muscle-invasive bladder Cancer (Ta, T1, and carcinoma in Situ). Eur. Urol. 81, 75–94 (2022).
Yafi, F. A. et al. Prospective analysis of sensitivity and specificity of urinary cytology and other urinary biomarkers for bladder cancer. Urol. Oncol. 33, 66e25–66e31 (2015).
Burger, M. et al. Photodynamic diagnosis of non-muscle-invasive bladder cancer with hexaminolevulinate cystoscopy: a meta-analysis of detection and recurrence based on Raw data. Eur. Urol. 64, 846–854 (2013).
Babjuk, M. et al. European association of urology guidelines on Non-muscle-invasive bladder Cancer (TaT1 and carcinoma in Situ) – 2019 update. Eur. Urol. 76, 639–657 (2019).
Dimashkieh, H. et al. Evaluation of urovysion and cytology for bladder cancer detection: a study of 1835 paired urine samples with clinical and histologic correlation. Cancer Cytopathol. 121, 591–597 (2013).
Lin, T. et al. Prospective evaluation of fluorescence in situ hybridization for diagnosing urothelial carcinoma. Oncol. Lett. 13, 3928–3934 (2017).
Budman, L. I., Kassouf, W. & Steinberg, J. R. Biomarkers for detection and surveillance of bladder cancer. Can. Urol. Assoc. J. 2, 212–221 (2008).
Miyake, M. et al. Influencing factors on the NMP-22 urine assay: an experimental model. BMC Urol. 12, 23 (2012).
Wang, C. et al. Loss of GATA6 expression promotes lymphatic metastasis in bladder cancer. FASEB J. 34, 5754–5766 (2020).
Papanicolau-Sengos, A. & Aldape, K. D. N. A. Methylation profiling: an emerging paradigm for Cancer diagnosis. Annu. Rev. Pathol. 17, 295–321 (2022).
Silva-Ferreira, M. et al. Diagnostic test accuracy of urinary DNA Methylation-based biomarkers for the detection of primary and recurrent bladder cancer: A systematic review and Meta-analysis. Eur. Urol. Focus S2405–4569(24)00088–00089 [pii] (2024).
Varol, N. et al. Methylation analysis of histone 4-related gene HIST1H4F and its effect on gene expression in bladder cancer. Gene 866, 147352 (2023).
Chen, X. et al. Urine DNA methylation assay enables early detection and recurrence monitoring for bladder cancer. J. Clin. Invest. 130, 6278–6289 (2020).
Dahmcke, C. M. et al. A prospective blinded evaluation of Urine-DNA testing for detection of urothelial bladder carcinoma in patients with gross hematuria. Eur. Urol. 70, 916–919 (2016).
van Kessel, K. E. et al. Validation of a DNA Methylation-Mutation urine assay to select patients with hematuria for cystoscopy. J. Urol. 197, 590–595 (2017).
Wu, Y. et al. PCDH17, POU4F2, and ONECUT2 as a urinary biomarker combination for the detection of bladder Cancer in Chinese patients with hematuria. Eur. Urol. Focus 6. HOXA9, 284–291 (2020).
Ruan, W. et al. A urine-based DNA methylation assay to facilitate early detection and risk stratification of bladder cancer. Clin. Epigenetics. 13, 91 (2021).
Guo, R. Q. et al. Detection of urothelial carcinoma, upper tract urothelial carcinoma, bladder carcinoma, and urothelial carcinoma with gross hematuria using selected urine-DNA methylation biomarkers: A prospective, single-center study. Urol. Oncol. 36, 342e15–342e23 (2018).
Xu, Y. et al. A Urine-Based liquid biopsy method for detection of upper tract urinary carcinoma. Front. Oncol. 10, 597486 (2020).
Oh, T. J. et al. Evaluation of sensitive urine DNA-Based PENK methylation test for detecting bladder Cancer in patients with hematuria. J. Mol. Diagn. 25, 646–654 (2023).
Zhang, W. et al. SDC2 and TFPI2 methylation in stool samples as an integrated biomarker for early detection of colorectal Cancer. Cancer Manag Res. 13, 3601–3617 (2021).
Funding
This project received funding from Zhongshan social welfare science and technology research project (2021B1102).
Author information
Authors and Affiliations
Contributions
The work reported in the paper has been performed by the authors. W.W.: Conceived and designed the experiments; Analyzed and interpreted the data; Editing paper. X.Y.: Conceived and designed the experiments; Analyzed and interpreted the data; Writing the original draft. W.L.: Conceived and designed the experiments; Performed the experiments; Analyzed and interpreted the data. J.C. and J.W.: Performed the experiments. J.C.: Contributed reagents, materials, and patients’ data. H.C.: Funding acquisition, supervision, and editing paper.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics statement
This study was approved by the Ethics Committee of Xiaolan Hospital of Zhongshan, the institutional review board number is ZSXL-LL2021-024. The methods were carried out in accordance with the approved guidelines. All the patients have been informed and signed informed consent before the experiments.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, WD., Yang, XR., Li, WH. et al. Analysis the diagnostic performance of H4C6/SOX1-OT gene methylation in bladder cancer based on urine sample. Sci Rep 15, 6961 (2025). https://doi.org/10.1038/s41598-025-91337-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-91337-w
