
Abstract
Chronic total occlusion (CTO) was frequently observed during coronary angiography. Successful revascularization of chronic total occlusion showed controversial result on long-term survival in previous studies. There is scarce report about long-term outcome of successful recanalization of CTO in patients with end stage renal disease (ESRD) receiving renal replacement therapy. This is a retrospective study conducted in two tertiary medical centers (Taipei and Taichung Veterans General hospitals) in Taiwan. From January 2005 to December 2016, a total of 47,784 patients received coronary angiography in these centers. Among them, 216 patients with ESRD who were found to have CTO lesions during coronary angiography received revascularization. Revascularization was succeeded in 163 patients (75%). Patients were followed up for three years. Successful revascularization was associated with lesser major adverse cardiovascular event (MACE) at 3 year (hazard ratio (HR) 0.518, 95% confidence interval (CI) 0.332–0.810, p = 0.004), better survival at 3 years (HR 0.502, 95% CI 0.314–0.800, p = 0.004) and improved cardiovascular death (HR 0.449, 95% CI 0.223–0.902, p = 0.025). In multivariate analysis, successful revascularization remained independent predictor of three-years MACE (HR 0.588, 95% CI 0.369–0.939, p = 0.026) irrespective of age, gender, serum hemoglobin level, co-morbidities such as peripheral arterial disease and diabetes mellitus and medications such as beta blocker and statin. In patients on renal replacement therapy, successful recanalization of chronic total occlusion reduced MACE at 3 years compared to those failed.
Similar content being viewed by others

Introduction
Patients with chronic kidney disease (CKD) account for as high as 15–20% of general population1. There were 3587 per million people in Taiwan who were in end stage renal disease (ESRD) and required renal replacement therapy (RRT) either by hemodialysis or peritoneal dialysis by the year of 20182. According to the United States renal data system, Taiwan had the highest prevalence of patients with ESRD on RRT in the world as RRT was imbursed by national insurance system. CKD is a well-known risk factor for coronary artery disease, myocardial infarction, heart failure, stroke, and peripheral arterial disease3. Co-morbidities such as coronary artery disease and heart failure increased mortality in patients with ESRD4. Besides, cardiovascular related mortality was the most common cause of death in patients with renal disease. However, adjusted all-cause mortality of ESRD receiving hemodialysis decreased from 192.9 per thousand patient-year in 2009 to 164.6 per thousand patient-year in 2018. The decline is even more prominent in patients on peritoneal dialysis5. It may be related to the improvement in RRT and partly from better treatment of cardiovascular morbidity. Optimal medical therapy with antiplatelet, statin, beta blocker and angiotensin converting enzyme inhibitors decreased mortality in patients with coronary artery disease after revascularization with either coronary artery bypass graft or percutaneous coronary intervention (PCI)6. Successful revascularization of chronic total occlusion (CTO) showed survival benefit in patients with CKD compared to failed PCI although there is increased risk of contrast induced nephropathy7. However, the impact of CTO PCI in patients with ESRD receiving RRT was not well known. Therefore, we investigated long-term outcome of patients with ESRD according to revascularization status of CTO lesion.
Materials and methods
Study population
It is a retrospective study that enrolled the patients receiving coronary catheterization at Taipei and Taichung Veterans General hospitals, two tertiary referral medical centers, in Taiwan. Patients received coronary angiography under the indications of acute coronary syndrome, unstable angina, or before cardiac surgery. We included the patients with both end stage renal disease who receiving regular renal replacement therapy with either hemodialysis or peritoneal dialysis and CTO lesions who received PCI for CTO in this study. CTO lesion is defined as the presence of thrombolysis in myocardial infarction (TIMI) flow 0 within an occluded coronary arterial segment of estimated duration of more than three months. ESRD is estimated glomerular filtration rate (eGFR) less than 15 ml/min/1.73m2 present for more than 3 months duration8 and patient is receiving RRT, either hemodialysis or peritoneal dialysis, due to electrolyte, acid-base abnormalities, unable to control volume status, poor nutritional status refractory to dietary intervention, cognitive impairment or pruritus9. The patients on hemodialysis received RRT thrice every week at dialysis clinic and those on peritoneal dialysis received RRT every day. CTO PCI was performed due to (1) angina refractory to optimal medical therapy or (2) exercise induced myocardial ischemia. Successful revascularization is defined as restoration of antegrade coronary flow (TIMI 3) in the previously occluded segment with < 50% of residual stenosis. Patients who didn’t receive revascularization for CTO lesion or referred for coronary artery bypass graft surgery (CABG) were excluded. Patient’s clinical characteristics, laboratory results, echocardiography, coronary angiography, PCI report, in-hospital treatments, and outpatient department record were extracted from web based electronic medical system of the hospitals.
Coronary angiography and PCI procedure
Coronary angiography is performed via radial or femoral artery. It was carefully evaluated by experienced interventionist to identify the characteristics of CTO lesion and collateral channels. According to interventionist’s preference and patient’s vascular condition, intervention was attempted by uni or bidirectional approaches (bi-radial or radial and femoral or bi-femoral). Activated clotting time > 300 s was maintained throughout the intervention using unfractionated heparin. Depending on CTO character, interventionist may attempt primary antegrade (wire escalation, parallel wire, intravascular ultrasound guided parallel wire technique) or retrograde technique (kissing wire or reverse controlled antegrade and retrograde tracking technique). Procedure may stop if operation time was more than 3 h without any progress, or radiation dose exceeds 5 Gy.
Dual antiplatelet therapy was prescribed one day or on the day before PCI procedure or immediately after intervention. Prescribed medications were aspirin 100 mg/day after 300 mg loading dose and clopidogrel (75 mg/day after 300 or 600 mg loading dose) if not on long-term medication. Dual antiplatelet therapy is maintained for at least 6 months unless there were side effects such as bleeding. After that, single antiplatelet therapy either aspirin or clopidogrel was maintained life-long. Other medications for coronary artery disease such as statin, beta blockers, calcium channel blockers, or nitrate were prescribed accordingly.
Clinical outcomes
Primary endpoints were major adverse cardiovascular event (MACE) (composite of all-cause mortality, cardiovascular mortality and non-fatal myocardial infarct), all-cause mortality, cardiovascular (CV) mortality, non-fatal myocardial infarct (MI) at 3 years. CV mortality was any death with definite cardiovascular cause or any death that was not apparently related to non-CV cause. Non-fatal MI is defined as the presence of typical symptoms of myocardial ischemia, new persistent ST elevation or transient ST segment elevation, depression or T wave inversion with increase or decrease of high sensitivity troponin T or I10. Periprocedural MI was excluded from this definition of MI. For clinical outcomes, admission and outpatient clinic records were extracted from two hospitals’ web-based electronic medical systems. If patients were loss of follow up in these two hospitals, research coordinators contacted them in telephone interviews. This study was approved by institutional review boards at Taipei and Taichung Veterans General Hospitals. (Protocol code No. 2019-12-013CC). This conduction of this study were in accordance with the Declaration of Helsinki.
Statistical analysis
Data were presented as percentages and mean ± standard deviation accordingly. Categorical variables were compared between two groups with Chi-square test and continuous variables with Student’s t-test respectively. Event-free survival was calculated with log-rank test by Kaplan-Meier method. Cox proportional hazard methods were used to estimate clinical outcomes such as MACE, all-cause mortality, CV mortality and non-fatal MI. Variables with p value of < 0.05 in univariate analysis were included in multivariate analysis. A p value of < 0.05 was considered as statistically significance. SPSS version 24 software (IBM, New York, USA) was used for statistical analysis.
Results
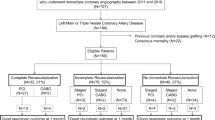
From January 2005 to December 2016, a total of 47,784 patients received coronary angiography at two centers. Among them, 266 patients with ESRD receiving RRT were found to have CTO lesion. 10 patients who underwent CABG and 40 patients on medical therapy were excluded from our study. Flowchart of patients’ enrollment was shown in (Fig. 1). Mean age of entire population was 71 ± 13 years old. 174 (81%) patients were male. Co-morbidities were common in study population whereas 88%, 61% and 39% of patients had hypertension, diabetes mellitus and heart failure respectively. Most common location of CTO was right coronary artery (52%).

Flow diagram of patients with chronic total occlusion diagnosed during coronary angiography.
Table 1 illustrated the comparison of baseline characteristics of ESRD patients whose revascularization of CTO was succeeded and failed. There was no significant difference in age, gender, co-morbidities such as hypertension, diabetes mellitus, hyperlipidemia, heart failure, atrial fibrillation, serum hemoglobin level and left ventricular ejection fraction between two groups. There was higher prevalence of peripheral arterial disease in patients with failed CTO PCI (14 vs. 28%, P value = 0.020).
Severity of coronary artery disease is not statistically different between two groups as well as CTO location. Primary antegrade approach was attempted more in failed revascularization group although not statistically significance (50 vs. 69%, P value = 0.200). (Table 2) The incidences of clinical events were listed in (Table 3). At three years follow up, MACE and all-cause mortality was significantly higher in patients who failed revascularization compared to those with successful revascularization (36 vs. 55%, P = 0.003 and 31 vs. 51%, P = 0.008, respectively). Failure to revascularization was also associated with significantly higher cardiovascular mortality than successful revascularization group (12 vs. 25%, P value = 0.030) although there was no difference in non-fatal myocardial infarct between two groups (6 vs. 9%, P value = 0.533). Kaplan-Meier survival curve revealed successful revascularization had lesser MACE at three-years compared to those who failed (Log-rank test P value = 0.003). (Fig. 2) Successful revascularization reduced MACE at three years follow up (hazard ratio (HR) 0.518; 95% confidence interval (CI) 0.332–0.810, p = 0.004). In multivariate analysis, successful revascularization was associated with all-cause survival benefit (HR 0.588, 95% CI 0.369–0.939, p = 0.026) after controlling possible confounding variables (age, gender, serum hemoglobin at time of coronary angiography, co-morbidities such as peripheral arterial disease and diabetes mellitus, long-term medications (beta blocker and statin) (Table 4).

Kaplan-Meier survival curve for 3-years MACE according to revascularization status.
Table 5 shows summary of periprocedural complications. Incidence of ventricular tachycardia, in-hospital pulmonary edema, shock during intervention necessitating intra-aortic balloon pump and extracorporeal membrane oxygenation, coronary artery perforation leading to cardiac tamponade, emergent referral for coronary artery bypass surgery were higher in failed to revascularization group although not statistically significant. Cardiogenic shock and in hospital mortality happened more frequently in failure group (3 vs. 12%, P = 0.027 and 2 vs. 13%, P = 0.002, respectively).
In subgroup analysis, patients younger than 75 years old, male gender, co-morbidities such as hypertension, diabetes mellitus, patients without abnormal lipid profile, heart failure, and peripheral arterial disease showed survival benefit in successful revascularization group although interaction P value were not significant. (Fig. 3)

Subgroup analysis of patients with end stage renal disease who received CTO PCI.
Discussion
This study, to our knowledge, was the first study to compare successful CTO PCI and failed CTO PCI in patients with ESRD. The result of this study showed that successful revascularization of coronary CTO lesion was associated with three-years MACE in patients with end stage renal disease. The results remained the same after controlling age, gender, co-morbidities (peripheral arterial disease), long term medications (beta blockers and statin).
Various observational studies showed successful revascularization of CTO lesion improved long-term survival (HR 0.72; 95% CI 0.62–0.83, P value < 0.001) especially when complete revascularization was achieved (HR 0.70; 95% CI 0.56–0.87; P = 0.002).11,12 However, randomized controlled trial (DECISION CTO trial) failed to demonstrate improvement in major adverse cardiovascular events in successful revascularization group compared to optimal medical management (HR 1.03; 95% CI 0.77–1.37, P = 0.86). One of the important limitations in this trial was that there was high crossover rate (20%) from no CTO PCI to CTO PCI group. Besides, there was high percentage (25%) of patients with relatively low risk of future cardiovascular events13. It may be difficult to reflect in patients with various co-morbidities and complex vascular conditions. Long-term outcome of CTO revascularization in patients with diabetes mellitus is reported to be associated with better survival compared to those without diabetes mellitus14. So, the benefit of revascularization may be more prominent in patients with more cardiovascular risk factors.
Taiwan had the highest prevalence rate of ESRD compared to other countries. The prevalence increased from 1322 to 2288 per million populations in the year of 2007 to the year of 2011 based on National Dialysis Registry of Taiwan Society of Nephrology. Diabetes mellitus, chronic glomerulonephritis and hypertension accounted three most common underlying causes for end stage renal disease in 200715. Survival rates after initiation of dialysis at 60 months was 53.6% and cardiovascular death remains the most common cause of death in patients with end stage renal disease in Taiwan15,16. The most common cause of death in normal renal function was cancer (38.1%) while more patients die from cardiovascular disease when renal function declines (43.7% in patients with eGFR 15–29.9 ml/min).17 CKD shares traditional risk factors such as diabetes mellitus, hypertension and dyslipidemia with coronary artery disease18. Explanations of high prevalence and better survival of ESRD in recent years are because of improve in dialysis care and treatment of co-morbidities such as diabetes mellitus, hypertension and coronary artery disease from both recent advancement in medications and devices19,20,21.
CKD increased major adverse cardiac and cerebrovascular events in patients with CTO lesion22. Successful revascularization of CTO lesion improved all-cause mortality in different stages of renal function23,24. Nevertheless, revascularization increased risk of contrast induced acute kidney injury and future requirements for RRT despite overall net survival benefit25. There was scarce report about long-term outcome of revascularization of CTO lesion in patients on dialysis. This study fills the gap that successful revascularization of CTO in patients on dialysis improved long-term outcome.
There was higher prevalence of co-morbidities such as hypertension, type 2 diabetes mellitus, peripheral arterial disease, left ventricular dysfunction in patients with CKD compared to those with normal renal function26. These co-morbidities lead to revascularization procedure more complex and higher periprocedural morbidities. Moreover, prominent arterial calcification which is due to abnormal phosphate metabolism in patients with ESRD results in higher Japanese CTO score27,28. It increases technical difficulties and requires advanced devices such as microcatheter and rotablation for revascularization. So, procedural success rate of CTO PCI also decreased with declining renal function25. It may be one of the reasons behind the relatively low procedural success rate (75%) in our study.
Stain users with low-density lipoprotein < 100 mg/dl had significant reduction in risk of major adverse cardiac and cerebrovascular events in patients with CKD compared to those with low-density lipoprotein > 100 mg/dl.29 In patients on dialysis with peripheral arterial disease and dyslipidemia, statin therapy reduced all-cause death, adverse limb outcome and amputation (HR: 0.85; 95% CI 0.73–0.99, P = 0.04)30. Baigent C et al. reported that there is trend towards reduction of major atherosclerotic events in patients on dialysis receiving simvastatin plus ezetimibe compared to placebo at 5 years follow up although not statistically significance. In our study, statin users were also associated with better all-cause survival compared to those without.
There were several limitations in this study. Firstly, this is a retrospective observational study. Secondly, treatment option via either revascularization or medical therapy was decided by interventionist, cardiovascular surgeon and patient’s preference. There may be selection bias. Thirdly, although Taipei and Taichung Veterans General hospital are tertiary referral medical centers, the experience in CTO revascularization was varied among interventionists so there may be different in success rate and periprocedural complications. However, there are well-experienced CTO interventionists in both centers mentoring every CTO procedure. It is a real world study so that the result may be able to reflect to our daily practice. Fourthly, all patients enrolled in our study were Taiwanese. Therefore, our results may not be similar across different races as cardiovascular risk factors are not the same. Fifth, the duration of renal replacement therapy either hemodialysis or peritoneal dialysis at the time of revascularization is not known.
Conclusion
Our results showed that revascularization of CTO in patients with end stage renal disease may improve long-term MACE compared to those who failed. Our study extended survival benefit of CTO PCI from patients with chronic kidney disease to those with ESRD.
Data availability
The data underlying this article will be shared on reasonable request to the corresponding author.
Abbreviations
- CTO:
-
Chronic total occlusion
- ESRD:
-
End stage renal disease
- HR:
-
Hazard ratio
- CI:
-
Confidence interval
- CKD:
-
Chronic kidney disease
- RRT:
-
Renal replacement therapy
- PCI:
-
Percutaneous coronary intervention
- TIMI:
-
Thrombolysis in myocardial infarction
- eGFR:
-
Estimated glomerular filtration rate
- CABG:
-
Coronary artery bypass graft
- CV:
-
Cardiovascular
- MI:
-
Myocardial infarct
References
Matsushita, K. et al. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet 375, 2073–2081. https://doi.org/10.1016/s0140-6736(10)60674-5 (2010).
The United States Renal Data System. 2020 annual report, ESRD Chap. 1.
Matsushita, K. et al. Estimated glomerular filtration rate and albuminuria for prediction of cardiovascular outcomes: a collaborative meta-analysis of individual participant data. Lancet Diabetes Endocrinol. 3, 514–525. https://doi.org/10.1016/s2213-8587(15)00040-6 (2015).
Herzog, C. A. Congestive heart failure and chronic kidney disease: the cardiorenal/nephrocardiology connection. J. Am. Coll. Cardiol. 73, 2701–2704. https://doi.org/10.1016/j.jacc.2019.03.474 (2019).
The United States Renal Data System. Annual Report, ESRD Chap. 5. (2020).
Kawashima, H. et al. Impact of optimal medical therapy on 10-year mortality after coronary revascularization. J. Am. Coll. Cardiol. 78, 27–38. https://doi.org/10.1016/j.jacc.2021.04.087 (2021).
Liu, Y. et al. Percutaneous coronary intervention for chronic total occlusion improved prognosis in patients with renal insufficiency at high risk of contrast-induced nephropathy. Sci. Rep. 6, 21426. https://doi.org/10.1038/srep21426 (2016).
K/DOQI clinical. Practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am. J. Kidney Dis. 39, S1–266 (2002).
Chap. 1: Definition and classification of CKD. Kidney Int. Suppl (2011) 3, 19–62 https://doi.org/10.1038/kisup.2012.64 (2013).
Collet, J. P. et al. 2020 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 42, 1289–1367. https://doi.org/10.1093/eurheartj/ehaa575 (2021).
George, S. et al. Long-term follow-up of elective chronic total coronary occlusion angioplasty: analysis from the U.K. Central cardiac audit database. J. Am. Coll. Cardiol. 64, 235–243. https://doi.org/10.1016/j.jacc.2014.04.040 (2014).
Goel, P. K., Khanna, R., Pandey, C. M. & Ashfaq, F. Long-term outcomes post chronic total occlusion intervention-implications of completeness of revascularization. J. Interv Cardiol. 31, 293–301. https://doi.org/10.1111/joic.12480 (2018).
Lee, S. W. et al. Randomized trial evaluating percutaneous coronary intervention for the treatment of chronic total occlusion. Circulation 139, 1674–1683. https://doi.org/10.1161/circulationaha.118.031313 (2019).
Tsai, C. T., Huang, W. C., Teng, H. I., Tsai, Y. L. & Lu, T. M. Long term clinical impact of successful recanalization of chronic total occlusion in patients with and without type 2 diabetes mellitus. Cardiovasc. Diabetol. 19, 119. https://doi.org/10.1186/s12933-020-01093-6 (2020).
Yang, W. C. & Hwang, S. J. Incidence, prevalence and mortality trends of dialysis end-stage renal disease in Taiwan from 1990 to 2001: the impact of National health insurance. Nephrol. Dial Transpl. 23, 3977–3982. https://doi.org/10.1093/ndt/gfn406 (2008).
Yang, C. W. et al. Global case studies for chronic kidney disease/end-stage kidney disease care. Kidney Int. Suppl (2011) 10, e24-e48 https://doi.org/10.1016/j.kisu.2019.11.010 (2020).
Thompson, S. et al. Cause of death in patients with reduced kidney function. J. Am. Soc. Nephrol. 26, 2504–2511. https://doi.org/10.1681/asn.2014070714 (2015).
Wilson, P. W. et al. Prediction of coronary heart disease using risk factor categories. Circulation 97, 1837–1847. https://doi.org/10.1161/01.cir.97.18.1837 (1998).
9. Pharmacologic approaches to glycemic treatment: standards of medical care in diabetes-2021. Diabetes Care 44, S111–s124. https://doi.org/10.2337/dc21-S009 (2021).
Balmforth, C. et al. Outcomes and effect of treatment according to etiology in HFrEF: an analysis of PARADIGM-HF. JACC Heart Fail. 7, 457–465. https://doi.org/10.1016/j.jchf.2019.02.015 (2019).
O’Neill, W. W. et al. Improved outcomes in patients with severely depressed LVEF undergoing percutaneous coronary intervention with contemporary practices. Am. Heart J. 248, 139–149. https://doi.org/10.1016/j.ahj.2022.02.006 (2022).
Zhang, Q. B. et al. Influence of chronic kidney disease on the outcome of patients with chronic total occlusion. Am. J. Transl Res. 8, 196–208 (2016).
Stähli, B. E. et al. Outcomes after percutaneous coronary intervention for chronic total occlusion according to baseline renal function. Clin. Res. Cardiol. 107, 259–267. https://doi.org/10.1007/s00392-017-1179-x (2018).
Lautamäki, A. et al. Outcome after coronary artery bypass grafting and percutaneous coronary intervention in patients with stage 3b-5 chronic kidney disease. Eur. J. Cardiothorac. Surg. 49, 926–930. https://doi.org/10.1093/ejcts/ezv233 (2016).
Shimura, T. et al. Rates of future Hemodialysis risk and beneficial outcomes for patients with chronic kidney disease undergoing recanalization of chronic total occlusion. Int. J. Cardiol. 222, 707–713. https://doi.org/10.1016/j.ijcard.2016.08.019 (2016).
Flores-Umanzor, E. et al. Impact of chronic kidney disease in chronic total occlusion management and clinical outcomes. Cardiovasc. Revasc Med. 38, 75–80. https://doi.org/10.1016/j.carrev.2021.07.018 (2022).
Webster, A. C., Nagler, E. V., Morton, R. L. & Masson, P. Chronic kidney disease. Lancet 389, 1238–1252. https://doi.org/10.1016/s0140-6736(16)32064-5 (2017).
O’Neill, W. C. & Lomashvili, K. A. Recent progress in the treatment of vascular calcification. Kidney Int. 78, 1232–1239. https://doi.org/10.1038/ki.2010.334 (2010).
Yen, C. L. et al. Association of low-density lipoprotein cholesterol levels during Statin treatment with cardiovascular and renal outcomes in patients with moderate chronic kidney disease. J. Am. Heart Assoc. 11, e027516. https://doi.org/10.1161/jaha.122.027516 (2022).
Lo, H. Y., Lin, Y. S., Lin, D. S., Lee, J. K. & Chen, W. J. Association of Statin therapy with major adverse cardiovascular and limb outcomes in patients with end-stage kidney disease and peripheral artery disease receiving maintenance dialysis. JAMA Netw. Open 5, e2229706. https://doi.org/10.1001/jamanetworkopen.2022.29706 (2022).
Author information
Authors and Affiliations
Contributions
Chuan-Tsai Tsai and Tse-Min Lu were involved in conceptualization. Chuan-Tsai Tsai and Ya-Wen Lu cured data. Formal analysis was performed by Wei-Chieh Huang and Ya-Wen Lu. Funding was acquired by Chuan-Tsai Tsai. Investigation was performed by Chuan-Tsai Tsai and Yi-Lin Tsai. Methodology was performed by Chuan-Tsai Tsai and Hsin-I Teng. Project administrator was Chuan-Tsai Tsai. Resources was arranged by Tse-Min Lu. Software was performed by Wei-Chieh Huang. Project was supervised by Tse-Min Lu, Shao-Sung Huang and Wen-Lieng Lee. Visualization was performed by Chuan-Tsai Tsai and Tse-Min Lu. Original draft was written by Chuan-Tsai Tsai and reviewed by Chuan-Tsai Tsai, Wei-Chieh Huang, Hsin-I Teng, Yi-Lin Tsai, and Tse-Min Lu.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Tsai, CT., Lu, YW., Huang, WC. et al. Revascularization of coronary chronic total occlusion in patients with end stage renal disease. Sci Rep 15, 13472 (2025). https://doi.org/10.1038/s41598-025-91447-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-91447-5
