
Abstract
The single nucleotide polymorphism rs12979860 is associated with the production of IFNλ4, a type III interferon, which offers protection from viral infection via its proinflammatory properties. We investigated if a genetically determined increase in IFNλ4 affects disease progression in SARS-CoV-2. This prospective, single-center study involved critically ill SARS-CoV-2 patients admitted to the intensive care unit. We performed genotyping for rs12979860 and analyzed daily laboratory data. Genotype frequencies were compared with an external validation cohort. Critically ill individuals with COVID-19 (n = 184; 29.3% women) were included. Median age was 63 years. The TT genotype was present in 11%, CT in 48% and CC in 41%. At baseline, CRP, ferritin, transferrin and neopterin did not differ significantly between groups. Longitudinal analysis revealed significant genotype-dependent differences in CRP, ferritin and neopterin with the highest peak in TT patients after 10–15 days. A higher need for renal replacement therapy (31.6% vs. 11.7%, p = 0.044) and mechanical ventilation (22 days vs. 15 days, p = 0.018) was observed in the TT group. The SNP rs12979860 near IFNL4 is associated with distinct inflammatory trajectories in critically ill COVID-19 patients. Genetic determinants of the immune response influence the severity of inflammation and clinical outcomes in severe COVID-19.
Similar content being viewed by others


Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections range from asymptomatic cases to severe illness requiring intensive care unit (ICU) admission1. Numerous therapeutic interventions have been investigated to reduce mortality and the burden on healthcare systems2,3,4,5. Among these, systemic glucocorticoids have shown a beneficial effect on mortality in patients requiring invasive mechanical ventilation (IMV) or supplemental oxygen, but not in those without respiratory support6. These findings highlight the significant impact of immunologic interactions in SARS-CoV-2 infection on disease progression, especially in critically ill patients.
The host’s response to coronavirus disease 2019 (COVID-19) involves several phases, starting with an asymptomatic incubation period (I), followed by activation of innate immunity (II) acting as the host’s first line of defense7. This includes local recognition of the viral infection by pattern recognition receptors (PRR), leading to the release of interferons (IFNs) and interferon-stimulated genes. This is followed by the pro-inflammatory (III) phase, which includes the release of cytokines and chemokines, ultimately leading to a cytokine storm (IV)8. This cytokine storm is characterized by the overproduction of pro-inflammatory cytokines such as IL-6, IL-1β, and TNF-α. The dysregulated immune activation may ultimately lead to endothelial dysfunction, increased vascular permeability, coagulopathy, and multi-organ failure, significantly contributing to disease severity and mortality9.
Differences in the disease course have been linked to predisposing risk factors such as sex, age, or various comorbidities10. As this explains only part of the variation, efforts have been made to understand genetic factors potentially influencing the host response and susceptibility11,12,13. The strongest genome-wide predictor of outcome was identified on chromosome 314,which was later fine-mapped to the leucine zipper transcription factor like 1 gene (LZTFL1)15. The gain-of-function risk allele in position rs17713054G > A was associated with altered mesenchymal to epithelial transition during regeneration from lung injury during COVID-19. Other common polymorphisms that reached genome-wide significance include genetic determinants of the ABO blood group system16. These large genome-wide analyses of genetic risk factors for disease severity included infection, hospitalization and admission to ICU as clinical endpoints. Considering the complex interaction of viral infection and host immune response, we asked if a prominent genetic determinant of innate immune response, namely a common polymorphism that determines the production of human interferon lambda 4 (IFNλ4) encoded by IFNL4 on chromosome 19 was associated with the clinical and immunological course of patients with severe COVID-19.
IFNλ4 has only been discovered in 2013, when Prokunina-Olsson et al. reported a new gene region (IFNL4) that was associated with hepatitis C virus (HCV) clearance17. Previous studies in HCV patients have shown that the single nucleotide polymorphisms (SNP) rs12979860 and rs809991 were genetic predictors of sustained virological response after treatment with interferon-alpha in patients with chronic HCV infection. These polymorphisms are located in the human interferon lambda gene cluster on chromosome 19. This cluster contains IFNL1 (formerly called IL29), IFNL2 (formerly called IL28A), IFNL3 (formerly called IL28B) and IFNL418. In the majority of the European population, IFNL4 is not expressed. However, a polymorphism in IFNL4, specifically rs368234815, which is in strong linkage disequilibrium with rs12979860 and rs809991 results in a frameshift due to a ΔG/TT substitution. This frameshift polymorphism is present in approximately 30% of the European population, as inferred from its linkage disequilibrium with rs1297986019.
IFNL4 has also been shown to play an important role in host response to various RNA viruses such as HIV, rhinovirus, coronavirus, influenza A and B virus20. Expression of IFNL4 It also appears to be involved in the host mucosal response to respiratory viral infections, positioning it as a potential target in COVID-1921. The same single SNP has been studied in the context of COVID-19 and results regarding the association with symptomatic disease and disease severity have been inconsistent22,23,24,25.
Due to the intricate role of IFNλ in the downstream regulation of the immune response, we hypothesized that this may result in differences in inflammatory parameters during the critical phase of SARS-CoV-2 infection. Therefore, we aimed to investigate the effect of IFNL4 rs12979860 genotypes on inflammatory parameters in critically ill COVID-19 patients during the ICU stay.
Results
Overall baseline characteristics and laboratory findings at ICU admission
A total of 184 critically ill COVID-19 patients treated at the intensive care unit in Innsbruck, Austria from March 2020 to December 2021 were included. Baseline characteristics and laboratory parameters at ICU admission are shown in Table 1. In addition, 122 critically ill COVID-19 patients from Milan, Italy were analysed as an external validation cohort (Supplemental Table 1). The median age in the Innsbruck cohort was 63 years, and 29.3% (n = 54) were female. The most common comorbidities were obesity (37.5%), hypertension (48.9%), cardiovascular disease (28.8%), diabetes mellitus type 2 (22.8%), and kidney disease (16.8%). The Sequential Organ Failure Assessment (SOFA) score and Simplified Acute Physiology Score (SAPS) III at ICU admission were 5 and 50, respectively. COVID-19-typical radiological findings were present in 96.7% of patients. The median c-reactive protein (CRP) at the time of ICU admission was 12.2 mg/dl. Laboratory parameters at the time of admission to ICU are shown in Table 1. Baseline characteristics and laboratory findings were similar in the Innsbruck cohort and the 122 patients in the Milan cohort (Supplemental Table 1).
The allele frequencies and genotype distributions of rs12979860 genotypes were also similar in both cohorts (Innsbruck and Milan, Table 2) and not different from the reported frequencies in the 1000 Genomes phase_3: central European population26.
Baseline characteristics and laboratory findings for different IFNL4 rs12979860 genotypes
When patients were grouped by IFNL4 genotype in high-risk (rs12979860:TT) or low-risk (rs12979860: CC/CT, also named non-TT) demographic variables were not significantly different in either the Innsbruck or the Milan cohort. Patients with the TT genotype had a median age of 58 years compared to 63 years in patients with the CC/CT genotype. Diabetes mellitus type 2 was more prevalent among TT patients than in CC/CT patients (52.6% [n = 10] vs. 19.5% [n = 30], p = 0.003). When the patient cohort was stratified by the presence of diabetes, no significant differences in inflammatory parameters were present at baseline, day 10 and day 20 (Supplemental Table 3). All other comorbidities were equally distributed between the genotype groups and no significant differences in baseline laboratory parameters were found (Supplemental Table 2).
Dynamics of inflammatory parameters during the ICU stay
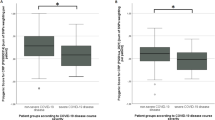
At baseline, CRP, serum iron parameters and neopterin did not differ between the groups (Supplemental Table 2 and Fig. 1). Procalcitonin (PCT) and interleukin 6 (IL-6) levels were highly variable at baseline, as reflected by the wide confidence intervals (Fig. 1).

(A)–(F) Dynamics of inflammatory parameters during first 20 days after ICU admission.
On longitudinal analysis, median CRP concentration decreased in all patients, regardless of their IFNL4 genotype for the first 5 days after ICU admission. This initial decline was followed by an increase, which was highest in patients homozygous for the T allele and reached a peak between day 10 and 15 (Fig. 1A). Ferritin and neopterin showed even more pronounced differences on longitudinal analysis. Ferritin of TT patients showed a strong upward trend peaking around hospital day 15, followed by a decline. For neopterin, we also found a distinct pattern of development in TT patients, who had a peak around 10 days after ICU admission, which is in contrast to non-TT patients, who exhibited a steady decline during the first 5–7 days after admission (Fig. 1A–C). PCT and IL-6 serum concentrations did not show the same temporal trends and varied widely over the course of the first 20 days with no significant differences present between IFNL4 genotype groups (Fig. 1D and E). The concentrations of transferrin were lower in the TT group compared to the CT and CC genotypes, yet failed to reach statistical significance during the first 20 days after ICU admission (Fig. 1F). In addition, a similar pattern was observed for D-Dimer with higher levels in the TT group, as shown in Supplemental Fig. 1.
Treatment at the ICU
The duration of mechanical ventilation was significantly longer in patients with the TT genotype (22 vs. 15 days, p = 0.018) and they required significantly more often renal replacement therapy (RRT, 31.6% vs. 11.7%, p = 0.044, Table 3; OR [odds ratio] 3.49 [95% CI 1.11–10.07], 0.024). Multivariable adjustment for the presence of diabetes did not affect this outcome (Supplemental Table 4). The majority of patients (85.9%) received corticosteroid treatment, regardless of their IFNL4 genotype with no significant difference between groups. Antiviral treatment was used in 82–84% of patients and 10–13% of patients were treated with remdesivir with no significant differences between patient groups. Vasopressors (57.6%) and invasive mechanical ventilation (IMV, 60.9%) were also required in the majority of patients with no significant differences.
Survival probability, hospital length of stay (LOS) and mortality
Genotype-dependent differences in the course of inflammation and the duration of ventilation did not translate into significant differences in survival between IFNL4 genotypes (Fig. 2) and no difference in ICU mortality (Table 3). Hospital mortality was higher in TT patients, but not statistically significant (31.6% vs. 19.5%, p = 0.354, OR 1.91 [0.62–5.26], p = 0.226). ICU and hospital length of stay (LOS) were not statistically different between the two groups (ICU LOS; CC/CT: 16 days vs. TT: 23 days, p = 0.218, hospital LOS; CC/CT: 27 days vs. TT: 30 days, p = 0.169). There were no significant differences in treatment and outcome when applying a dominant model (CC vs. no CC, Supplemental Table 5).

Kaplan–Meier Survival Curves for the different IFNL4 genotypes.
Discussion
The natural disease course of severe COVID typically follows three sequential phases, in which an initial pulmonary phase is followed by a proinflammatory state before the risk for thrombotic complications increases in the third phase27. The present study identified a genetic determinant for very severe inflammation in the second phase of COVID-19: homozygosity for the T allele in rs12979860, which is associated with high IFNλ4 production. In this group, severe inflammation was also linked with a higher need for RRT and longer duration of IMV. Both complications could result from a more severe immune response to SARS-CoV-2 infection7. Organ cross-talk between the lungs and kidneys plays an important role in critical illness, with severe inflammation serving as a key driver of this interaction28,29. The TT genotype and the enhanced pro-inflammatory responses potentially lead to more severe systemic inflammation, together with endothelial dysfunction, and immune dysregulation. These mechanisms could contribute to an increased risk of organ dysfunction, including worsening kidney injury requiring RRT and more severe respiratory failure necessitating prolonged mechanical ventilation.
Mitigation of the immune response to SARS-CoV-2 infection is also the primary rationale for dexamethasone treatment, which was found to positively impact survival in patients with severe COVID-196. Studies in large European cohorts of patients with COVID-19 have identified several risk factors for viral susceptibility and survival, but have not shown any association with the IFNL4 locus14,30,31. This difference between the present study and previous large genome wide association studies can be explained by distinct endpoints. In our study no significant differences in markers of inflammation (C-reactive protein, ferritin or procalcitonin) were present on the day of admission to ICU. When grouped by genotype, differences especially in ferritin emerged over the first 5–10 days after admission, showing that rs12979860 determines the host immune response to infection in the second phase of the infection.
Patients homozygous for the T allele in rs12979860 also harbour a frameshift mutation in the IFNL4 gene, which re-activates expression of this cytokine that is genetically inactivated in the majority of individuals with European ancestry. This relationship is less pronounced in populations of non-European descent19. Unlike type I IFNs, which have systemic effects via IFN alpha receptors 1 and 2 that are ubiquitously expressed in all cells, IFNλ4 signals through the IFNλ receptor complex that consists of heterodimers of the IL-10 receptor and the IFNλ receptor 1 (IL10R2 and IFNLR1)32. The latter has a more restricted expression pattern limited to epithelial cells and only some immune cells including monocyte-lineage cells33. Individuals with the TT genotype produce more IFNλ4, which can act as a proinflammatory cytokine and potentially cause over-activation of the immune response, beyond its antiviral properties33. Macrophages, as key responders to IFNλs, play a crucial role in this process by promoting cytotoxicity, phagocytosis, and the secretion of pro-inflammatory cytokines and chemokines34. Activation of monocytes and macrophages, in turn, is associated with a large increase in ferritin gene expression35. This might explain the distinct ferritin peak seen in our study in the TT genotype in the proinflammatory phase. Such hyperferritinemic states are not unique in COVID-19 and can also be seen in other viral infections and conditions such as macrophage activation syndrome/ hemophagocytic lymphohistiocytosis (HLH), adult-onset Still’s disease, catastrophic antiphospholipid syndrome or septic shock36. HLH is a condition with excessive immune activation and hyperinflammation, that is often triggered by infectious agents such as Epstein-Barr virus, and has also been described in cases in COVID-19. Inflammasome activation in infected macrophages has been shown to be a key driver of pathology in COVID-1938. Stronger macrophage activation in patients with the TT genotype in rs12979860 is also highlighted by the finding that neopterin was significantly higher in this patient group. Macrophages also produce neopterin after being stimulated by interferon gamma (IFNγ), which has been shown to predict disease severity in COVID-1939. IFNγ is mainly produced by natural killer (NK) cells, which are key mediators in the pathogenesis of COVID-1940. NK cells have also been linked to IFNλ, though it is unclear whether IFNλ can activate them directly or indirectly via mucosal cells and macrophages33. This interaction might explain the higher neopterin concentration observed in the TT genotype in our cohort. Of note, patients with the TT genotype had a higher prevalence of diabetes mellitus. Similar findings have been reported in other cohorts, where the CC genotype was found to be protective against insulin resistance41 and the development of new-onset diabetes mellitus after liver transplantation42. However, it is unlikely that the higher rate of diabetes mellitus in the TT group significantly determined our results.
Interferons are paradigmatic host cytokines released in response to viral infections including COVID-19. This family of cytokines, mainly type I IFNs (alpha interferons) and type III IFNs (lambda interferons) have been investigated in clinical trials. Three major trials investigating type I IFNs (WHO-Solidarity/Discovery43; IFN-β1a, ACTT344; IFN-β1a and Sprinter45; Nebulised interferon-β1a) were all negative regarding their primary endpoint. The Together trial investigated IFNλ and was able to demonstrate a significant reduction in emergency department visits and hospitalization in primarily vaccinated COVID-19 patients46. IFNλ exerts antiviral effects by binding to a specific receptor complex IFNLR1 and IL10RB. This binding triggers the expression of interferon-stimulated genes (ISGs) that inhibit viral replication. This process is localized to epithelial cells and tries to limit systemic inflammation, which might explain the positive effects of IFNλ46. The interferon used in this trial is PEG-rIL-29, which is IFNλ1 (IFNL1), as opposed to IFNλ4 (IFNL4), whose genetics was investigated in this study. In SARS-CoV-2 infections genetic variants of IFNL4 (SNP rs12979860) have been investigated and were associated with the occurrence of COVID-1922. Sapono-Cortes et al. compared 177 COVID-19 with 445 non-COVID-19 patients and found a higher frequency of the T allele in COVID-19 patients compared to the general population. Other studies have shown an association with disease severity47. However, a meta-analysis on genetic polymorphisms and their association with COVID-19 infection and outcomes included three studies on rs12979860 and found no significant connection between rs12979860 and the severity of the disease48. This is in line with our results. We included only critically ill COVID-19 patients in our analysis and the genotype frequency was comparable to that expected in the general population. This has been confirmed by the results of our validation cohort (Table 2).
An important limitation that must be considered when interpreting our results is the limited sample size, particularly in the TT genotype group, which does not allow for more complex statistical testing. Therefore, our findings require further validation in larger cohorts.In conclusion, the TT genotype in position rs12979860 SNP is linked to severe inflammation in COVID-19. This genotype is associated with higher levels of inflammatory markers such as ferritin and neopterin, suggesting an inflammatory subphenotype with a distinct immune response.
Methods
Study design and patients
This is a single-center prospective study including patients with a SARS-CoV-2 infection in Innsbruck from March 2020 until December 2021. Patients with a positive SARS-CoV-2 polymerase chain reaction (PCR) test and admission to the medical intensive care unit were included in this analysis. A validation cohort from Milan was retrospectively assessed to compare genotype frequencies. The study was performed in accordance with the Declaration of Helsinki and the European Data Policy. The study protocol was approved by the ethics committee of the medical university Innsbruck (Nr. 1107/2020). Informed consent was obtained from all participants according to local regulations.
Definitions and data collection
Patient characteristics, clinical parameters and details about the ICU stay were extracted from the Tyrolean COVID-19 intensive care registry; a prospective registry study including all critically ill COVID-19 patient treated in Tyrol, Austria. The methods of this registry previously have been described in detail49,50.
Daily laboratory parameters during the ICU stay were extracted from the hospital’s electronic health records. Inflammation parameters (CRP, procalcitonin [PCT], ferritin, interleukin-6 [IL-6], transferrin and neopterin) were analyzed in daily clinical routine. For this study, time points were defined relative to ICU admission (day 0).
Acute kidney injury (AKI) was defined and staged according to Kidney Disease: Improving Global Outcome (KDIGO) using both creatinine and urine output criteria.
For the duration of IMV, a day was counted, if ventilation was performed for more than 2 h.
Genotyping
Genotyping for rs12979860 was performed as previously described51. Briefly, DNA was extracted from EDTA blood on a Diasorin Arrow Liason/IXT using the GXT blood extraction kit (Bruker).
Genotyping for the DNA polymorphism rs12979860 near the IFNL4 gene was carried out using an internally validated TaqMan allelic discrimination assay (TaqMan SNP Genotyping Assay, Assay ID C___7820464_10/rs12979860, Thermo Fisher, Vienna, Austria).
Statistical analysis
Categorical variables are presented as numbers with corresponding percentages and continuous variables are presented as median with interquartile range (IQR). Normal distribution of continuous data was checked with the Shapiro–Wilk test. Normally distributed data was compared using a two-sample t-test. Not normally distributed data was compared using Mann–Whitney-U test or χ2-test. Odds ratios (OR) are presented with 95% confidence interval (95% CI).
We used a locally estimated scatterplot smoothing (LOESS) to smoothen time trends of inflammatory parameters for each IFNL4 rs12979860 genotype. LOESS is a non-parametric method to fit multiple regressions in local neighborhood. The span (parameter alpha), which controls the degree of smoothing was set at 0.75 and graphs are presented with 95% confidence intervals.
Kaplan–Meier survival analysis was used to calculate the probability of hospital survival for the different genotypes. Differences were assessed by the log-rank test.
A p-value < 0.05 was considered statistically significant and all statistical tests were 2-sided. Statistical analysis was performed using R Software 4.4.052.
Data availability
The data that support the findings of this study are available on reasonable request from the corresponding author.
References
Huang, C. et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet 395, 497–506 (2020).
Kalil, A. C. et al. Baricitinib plus remdesivir for hospitalized adults with Covid-19. N. Engl. J. Med. 384, 795–807 (2020).
Beigel, J. H. et al. Remdesivir for the treatment of Covid-19—final report. N. Engl. J. Med. 383, 1813–1826 (2020).
Misset, B. et al. Convalescent plasma for Covid-19-induced ARDS in mechanically ventilated patients. N. Engl. J. Med. 389, 1590–1600 (2023).
O’Halloran, J. A. et al. Abatacept, cenicriviroc, or infliximab for treatment of adults hospitalized with COVID-19 pneumonia: A randomized clinical trial. Jama 330, 328–339 (2023).
Horby, P. et al. Dexamethasone in hospitalized patients with Covid-19. N. Engl. J. Med. 384, 693–704. https://doi.org/10.1056/NEJMoa2021436 (2021).
Diamond, M. S. & Kanneganti, T.-D. Innate immunity: The first line of defense against SARS-CoV-2. Nat. Immunol. 23, 165–176 (2022).
Liu, B. M., Martins, T. B., Peterson, L. K. & Hill, H. R. Clinical significance of measuring serum cytokine levels as inflammatory biomarkers in adult and pediatric COVID-19 cases: A review. Cytokine 142, 155478 (2021).
Fajgenbaum, D. C. & June, C. H. Cytokine storm. N. Engl. J. Med. 383, 2255–2273 (2020).
Zheng, Z. et al. Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis. J. Infect. 81, e16–e25 (2020).
Kanai, M. et al. A second update on mapping the human genetic architecture of COVID-19. Nature 621, E7–E26 (2023).
Zhang, Q. et al. Inborn errors of type I IFN immunity in patients with life-threatening COVID-19. Science 370, eabd4570 (2020).
Zhang, Q., Bastard, P., COVID Human Genetic Effort, Cobat, A. & Casanova, J.-L. Human genetic and immunological determinants of critical COVID-19 pneumonia. Nature 603, 587–598 (2022).
Severe Covid-19 GWAS Group et al. Genomewide association study of severe Covid-19 with respiratory failure. N. Engl. J. Med. 383, 1522–1534 (2020).
Downes, D. J. et al. Identification of LZTFL1 as a candidate effector gene at a COVID-19 risk locus. Nat. Genet. 53, 1606–1615 (2021).
Wu, B.-B., Gu, D.-Z., Yu, J.-N., Yang, J. & Shen, W.-Q. Association between ABO blood groups and COVID-19 infection, severity and demise: A systematic review and meta-analysis. Infect. Genet. Evol. J. Mol. Epidemiol. Evol. Genet. Infect. Dis. 84, 104485 (2020).
Prokunina-Olsson, L. et al. A variant upstream of IFNL3 (IL28B) creating a new interferon gene IFNL4 is associated with impaired clearance of hepatitis C virus. Nat. Genet. 45, 164–171 (2013).
Ge, D. et al. Genetic variation in IL28B predicts hepatitis C treatment-induced viral clearance. Nature 461, 399–401 (2009).
O’Brien, T. R., Prokunina-Olsson, L. & Donnelly, R. P. IFN-λ4: the paradoxical new member of the interferon lambda family. J. Interferon Cytokine Res. Off. J. Int. Soc. Interferon Cytokine Res. 34, 829–838 (2014).
Rugwizangoga, B. et al. IFNL4 genotypes predict clearance of RNA viruses in Rwandan children with upper respiratory tract infections. Front Cell Infect. Microbiol. 9, 340 (2019).
Broggi, A., Granucci, F. & Zanoni, I. Type III interferons: Balancing tissue tolerance and resistance to pathogen invasion. J. Exp. Med. 217, e20190295 (2020).
Saponi-Cortes, J. M. R. et al. IFNL4 genetic variant can predispose to COVID-19. Sci. Rep. 11, 21185 (2021).
Agwa, S. H. A. et al. Association between Interferon-Lambda-3 rs12979860, TLL1 rs17047200 and DDR1 rs4618569 variant polymorphisms with the course and outcome of SARS-CoV-2 patients. Genes Basel 12, 830 (2021).
Zahid, W. et al. Association of interferon Lambda 3 and 4 gene SNPs and their expression with COVID-19 disease severity: A cross-sectional study. Infect Drug Resist. 16, 6619–6628 (2023).
Rahimi, P. et al. The association between interferon lambda 3 and 4 gene single-nucleotide polymorphisms and the recovery of COVID-19 patients. Virol. J. 18, 221 (2021).
Auton, A. et al. A global reference for human genetic variation. Nature 526, 68–74. https://doi.org/10.1038/nature15393 (2015).
Lee, C. & Choi, W. J. Overview of COVID-19 inflammatory pathogenesis from the therapeutic perspective. Arch. Pharm. Res. 44, 99–116 (2021).
Husain-Syed, F., Slutsky, A. S. & Ronco, C. Lung-kidney cross-talk in the critically ill patient. Am. J. Respir. Crit. Care Med. 194, 402–414 (2016).
Mayerhöfer, T., Perschinka, F. & Joannidis, M. Akute Nierenschädigung und COVID-19: Pulmorenaler crosstalk unter massiver inflammation. Med. Klin. Intensivmed. Notfallmedizin 117, 342–348 (2022).
Alsaedi, S. B., Mineta, K., Gao, X. & Gojobori, T. Computational network analysis of host genetic risk variants of severe COVID-19. Hum. Genomics 17, 17 (2023).
Niemi, M. E. K. et al. Mapping the human genetic architecture of COVID-19. Nature 600, 472–477 (2021).
Prokunina-Olsson, L. et al. COVID-19 and emerging viral infections: The case for interferon lambda. J. Exp. Med. 217, e20200653 (2020).
Liu, Y.-G. et al. Interferon lambda in respiratory viral infection: Immunomodulatory functions and antiviral effects in epithelium. Front. Immunol. 15, 1338096 (2024).
Read, S. A. et al. Macrophage coordination of the interferon lambda immune response. Front. Immunol. 10, 2674 (2019).
Rosário, C., Zandman-Goddard, G., Meyron-Holtz, E. G., D’Cruz, D. P. & Shoenfeld, Y. The hyperferritinemic syndrome: Macrophage activation syndrome, Still’s disease, septic shock and catastrophic antiphospholipid syndrome. BMC Med. 11, 185 (2013).
Ruscitti, P. et al. Severe COVID-19, another piece in the puzzle of the hyperferritinemic syndrome. An immunomodulatory perspective to alleviate the storm. Front. Immunol. 11, 1130 (2020).
Molina, G. et al. Hemophagocytic lymphohistiocytosis following COVID-19 infection. Cureus 15, e34307 (2023).
Sefik, E. et al. Inflammasome activation in infected macrophages drives COVID-19 pathology. Nature 606, 585–593 (2022).
Bellmann-Weiler, R. et al. Neopterin predicts disease severity in hospitalized patients with COVID-19. Open Forum Infect. Dis. 8, ofaa521 (2021).
Lee, M. J. & Blish, C. A. Defining the role of natural killer cells in COVID-19. Nat. Immunol. 24, 1628–1638 (2023).
Petta, S. et al. Effects of IL28B rs12979860 CC genotype on metabolic profile and sustained virologic response in patients with genotype 1 chronic hepatitis C. Clin. Gastroenterol. Hepatol. 11, 311-317.e1 (2013).
Duca, A. M. et al. CC genotype at rs12979860 of IL28B is associated with lower risk of new-onset diabetes after transplantation in adult patients with liver transplantation for hepatitis C cirrhosis. Transplant. Proc. 46, 3114–3116 (2014).
Pan, H. et al. Remdesivir and three other drugs for hospitalised patients with COVID-19: Final results of the WHO Solidarity randomised trial and updated meta-analyses. The Lancet 399, 1941–1953 (2022).
Kalil, A. C. et al. Efficacy of interferon beta-1a plus remdesivir compared with remdesivir alone in hospitalised adults with COVID-19: A double-bind, randomised, placebo-controlled, phase 3 trial. Lancet Respir. Med. 9, 1365–1376 (2021).
Monk, P. D. et al. Nebulised interferon-β1a (SNG001) in hospitalised COVID-19: SPRINTER phase III study. ERJ Open Res. https://doi.org/10.1183/23120541.00605-2022 (2023).
Reis, G. et al. Early treatment with pegylated interferon lambda for Covid-19. N. Engl. J. Med. 388, 518–528 (2023).
Amodio, E. et al. SARS-CoV-2 viral load, IFNλ polymorphisms and the course of COVID-19: An observational study. J. Clin. Med. 9, 3315 (2020).
Ren, H. et al. Association of genetic polymorphisms with COVID-19 infection and outcomes: An updated meta-analysis based on 62 studies. Heliyon 10, e23662 (2024).
Mayerhöfer, T. et al. Incidence, risk factors and outcome of acute kidney injury in critically ill COVID-19 patients in Tyrol, Austria: A prospective multicenter registry study. J. Nephrol. https://doi.org/10.1007/s40620-023-01760-3 (2023).
Mayerhöfer, T. et al. Changes in characteristics and outcomes of critically ill COVID-19 patients in Tyrol (Austria) over 1 year. Wien. Klin. Wochenschr. 133, 1237–1247 (2021).
Graziadei, I. W. et al. Early viral load and recipient interleukin-28B rs12979860 genotype are predictors of the progression of hepatitis C after liver transplantation. Liver Transpl. 18, 671–679 (2012).
R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing.
Acknowledgements
The Tyrolean COVID-19 intensive care registry was funded by a grant from the Tyrolean Government. We thank Laura Obholzer for excellent technical support.
Author information
Authors and Affiliations
Contributions
TM, BS and HZ designed the study, collected data, performed data analysis and wrote the first draft of the manuscript. SK, FD, SM, LM, LR, SW, SS, IT, DH, LV and HT collected samples and data and contributed to the critical revision of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Mayerhöfer, T., Joannidis, M., Klein, S. et al. The common genetic variant rs1278960 determining expression of Interferon-lambda predicts inflammatory response in critically ill COVID-19 patients. Sci Rep 15, 15802 (2025). https://doi.org/10.1038/s41598-025-91628-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-91628-2
