
Abstract
The epidemiological transition has been characterized by demographic, societal and health changes in societies. Presuming that acute diseases, mostly of communicable etiology, are more important in terms of early-life mortality, whereas chronic diseases are responsible for a greater burden of disease throughout the life course, we attempt to develop an index to measure the stage of the epidemiological transition. Using Global Burden of Diseases, Risk Factors and Injuries (GBD) data available at https://vizhub.healthdata.org/gbd-compare/ on 04/04/2024 to calculate the Epidemiologic Transition Estimate (ETE) index as a ratio of YLD/YLL for the time period of 1990–2019. The values of the index ranged from 0.131 to 1.067 and 0.180 to 2.108 for males and females, respectively, across the 195 included countries. The transition process seems to be faster to females compared to males. The index shows consistently increasing values for five SDI-based country groups, with clear differences among the groups. Although more research and validation studies are needed despite all the uncertainties, the index seems to be robust to assess the progress in epidemiological transition. These findings can help to predict future social care and health system needs to address causes leading to YLD or YLL.
Similar content being viewed by others


Introduction
The epidemiologic transition1 is often perceived as a simplified process of decreasing mortality from communicable diseases followed by an increasing share of chronic, mostly noncommunicable diseases2. The demographic element of this transition leads to the aging of populations, and together with the shifted pattern of disease occurrence in different age groups, health systems face the need to shift health services and social care. National systems for health need to maintain their focus on diseases of infancy and childhood, often of communicable etiology, and at the same time provide services to tackle the growing burden of chronic diseases3; this “double burden” situation is well described in the literature by different authors4,5,6,7,8. Most of this literature is focused on low-income country settings, and little, if any, knowledge is published on epidemiologic transition within high-income countries. With respect to the economic development status of the country, it would be desirable for national health service planners to know the state of transition in their own country to estimate the pace of transition and planning of appropriate health services, including the workforce. In this context, it is good to think about the involvement of social care services, which could bring significant benefits, such as improved health promotion and primary prevention, followed by improved clinical outcomes, reduced hospitalization rates, and positive effects on patient satisfaction9.
The Global Burden of Diseases, Risk factors and Injuries study10, through the concept of disability adjusted life years (DALY) which consist of years of life lost (YLL) due to premature mortality and years of life lost due to disability (YLD), introduced the possibility of analyzing health trends from two different approaches. From a public health angle, the YLL allows us to assess the ability of a health system to keep people alive to older ages11, whereas the YLD shows how healthy a certain population is throughout their lifetime12. In other words, YLL shows how well a health system diagnoses and treats people to avoid premature mortality, and YLD shows how well a health system promotes and protects health, prevents disease, supports avoidance of complications, and provides good rehabilitation services. Hypothetically, this means that changes in the occurrence and fatality of acute diseases should be more common in the YLL subgroup of disease burden, whereas changes in chronic diseases should be more common in the YLD subgroup, although there are differences in the level of prevention (primary prevention should lead to a decrease in YLDs, whereas secondary and tertiary prevention may increase YLDs”). Can this kind of thinking lead to an index that would allow us to estimate the progress of epidemiologic transition?
The objective of this paper is to answer that question by presenting and discussing a simple ratio (index) of YLD/YLL. We hypothesize that in a society with predominantly high mortality in younger age groups, there is a high YLL and low YLD, leading to epidemiologic transition estimate (ETE) values less than 1. This society is at the beginning stage of the epidemiologic transition. In contrast, in a society with low mortality in young age groups, the incidence of chronic, noncommunicable diseases is increasing, leading to higher YLD values and greater ETE values.
Method
As a data source, we used the Compare tool of the GBD study, which is publicly available at https://vizhub.healthdata.org/gbd-compare/; data for 2019 calculations were used. We always used age-standardized values of YLL and YLD calculated per 100 000 to avoid differences caused by different age structures of populations. We calculate a simple index of the ETE as follows:
We used regional categorization (21 regions) presented by the Institute of Health Metrix and Evaluation (IHME)13 of the University of Washington, Seattle, USA. A list of countries belonging to each region is given in Annex I of this manuscript. To provide data for the selected countries, we used countries where the WHO Regional offices had their headquarters.
We selected the sociodemographic index (SDI)-based groups of countries and calculated time trends in the ETE to allow discussion at different development levels. The SDI is a summary measure of development that uses income per person, average educational attainment in the population older than 15 years and the total fertility rate14. We used the SDI and categorization of countries as available on the Compare tool (https://vizhub.healthdata.org/gbd-compare/ visited 04/05/2018) website.
Results
The GBD database constructed with the Compare tool contains data for 200 + countries and territories. The basic descriptive statistics for the ETE index for regions by male and female sex are presented in Tables 1, 2.
The difference between 1990 and 2019 is statistically significant.
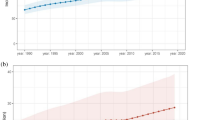
The temporal trends of ETE values across 21 regions in 195 countries throughout the world for the studied period, separately for males and females, are shown in Figs. 1 and 2.

Temporal trend of the ETE index in different regions of the world in males.

Temporal trend of the ETE index in different regions of the world in females.
Three major issues are visible from regional analysis by sex:
-
Not surprisingly Western Europe, Australasia, High-income North America and High-income Asia Pacific regions are the frontrunners of epidemiological transition.
-
There is a substantial difference between males and females; females are presenting higher ETE index values meaning that YLD element overturns the YLL element in burden of disease.
-
The substantial drop of the value of proposed index in Caribbean in 2010 shows the sensitivity of it to major events. The likely reason of that drop is extremely high mortality in Haiti after major earthquake in Hati and Dominican Republic15.
The distribution of ETE values further supported by the significance of the difference between 1990 and 2019 confirmed our basic hypotheses that such an index might provide sensible information. A growing inequality over time among regions both for males and females is another generally noticeable phenomena.
The temporal trend of the development of ETE index values by SDI country group is presented in Fig. 3.

Temporal trend of the ETE by SDI category.
All groups showed a consistent increasing trend in the ETE index, confirming our hypothesis that ETE can be used to indicate the process of epidemiologic transition. The differences among SDI groups further confirm the growing inequality trend noticed on Figs. 1 and 2.
In the second step, we decided to select countries and analyze the temporal trend of the ETE. We choose countries where the regional headquarters of the WHO are located. Figure 4 presents the results.

Temporal trend of the ETE in selected countries.
Despite of very arbitrary, one might say not scientific selection of countries data again show the growing global inequality; Denmark together with USA are progressing much faster as the other four selected countries. It is also interesting that Denmark over 2005–2010 surpassed USA in progress of transition.
To verify the index and our hypothesis, we examined changes in the causes of total DALYs lost by five SDI groups between 1990 and 2019. We downloaded the data from the Compare tool website (https://vizhub.healthdata.org/gbd-compare/ visited 07/05/2018) and used the following standard categories of causes: (1) communicable, maternal, neonatal and nutritional diseases (CMNNs); (2) noncommunicable diseases (NCDs); and (3) injuries. The top 10 causes of lost DALYs were used to create Fig. 5.

Changes in causes of loss of DALYs by SDI group.
CMNNs are not among the top ten causes of disease within high-SDI countries, and their prevalence is decreasing in all SDI groups, presenting the same pattern as the values of the ETE index.
Discussion
The aim of our work was to develop and test a simple index to estimate the progress of epidemiological transition using data from the GBD study. Compared to the GBD study, which developed the SDI, we used a different approach based on the hypothesis that, by moving ahead in epidemiological transition, the share of YLD compared to YLL is changing in favor of YLD. Owing to improved living conditions and the availability of vaccines, societies are better managing the risk of mortality in childhood related to motherhood and reproduction as well as the control of communicable diseases16,17,18. This, in turn, leads to longer life and aging, allowing individuals to experience noncommunicable diseases and injuries. This process reflects the five stages of epidemiologic transition1. The proposed index shows how many YLDs relate to one YLL due to premature mortality. As the value of the ETE index increases, more resources need to be allocated to health promotion, protection, primary, secondary and tertiary prevention of diseases and chronic disease care. In relation to YLDs, it is important to consider that health promotion and primary prevention activities are expected to lead to prolonged health19,20 and thus a decrease in YLD, while secondary and tertiary prevention activities, for example, reducing the severity or duration of a disease leading to longer life with chronic conditions21, are likely to increase the volume of YLDs. Through this, the index adds to discussion on whether to focus on compression of morbidity or compression of mortality22,23. Clearly bot are important and closely inter-twinned as the popular public health formulation is saying “adding years to life is as important as adding life to years”. Studying the role of different health promotion and disease prevention interventions on YLD (and consequently on epidemiologic transition and ETE) requires additional research on specific diseases (e.g., mental health). As the value of the index increases, health systems should be oriented more toward long-term care than toward acute care in the case of low ETE indices.
The presented ETE index shows clear and consistent changes all over the world; there is a statistically significant increase in the value of the index. Comparing the range of values for 2019 to 1990, a difference widening effect is visible, indicating substantial inequalities in the progress of epidemiological transition. Apparently, the progress of epidemiological transition is an exponential/multiplicative process that is accelerated by reaching higher levels. The ETE index seems to offer an opportunity to study in greater depth the temporal relationships and patterns of the transition.
A substantial inequality is identified by sex; females in every regional or development group have higher values of the index. This finding is consistent with known male‒female differences in health24. Other studies also point out that women, despite living longer, are no longer living more disability-free lives than men25. In other words, women have lower mortality but higher morbidity rates than men24. These differences are based on both biological systems and social processes24. This difference is important in terms of health policies especially oriented toward health promotion and disease prevention areas.
Analyzing the index by sex, SDI levels and even by selected countries confirms a major and growing global inequality. On one hand, this corresponds well to Omran’s suggestion that the epidemiological transition is influenced by demographic, economic and sociological determinants1, which are reflected in the SDI12. On other hand however, it is not a positive results taking in account fighting global health (and general) inequalities among countries is on global political agenda for many decades now. Changes in the top ten groups of diseases leading to a decrease in DALYs in the five SDI groups fully support our presumption of moving from communicable to chronic diseases and, to some extent, validate the construct of our index.
The correlation between two indices is quite strong, yet both have slightly different meanings. The SDI has been widely described and discussed in the literature14, and is predominantly addressing societal development stage. Our proposed index should inform health and social policy makers where to orient health policies in respective countries to maximize population health gains.
There are several future research and policy possibilities related to ETE index use. It would be interesting to estimate a kind of cutoff point; what does this mean for population health or a health system in a country if the ETE index reaches a certain value? For example, could one say that reaching value 1, equalizing numbers of YLD and YLL lost, means that a country achieved a turning point in terms of switching to a need for more chronic, compared to acute care? Conducting single-country analysis or comparative multicountry analysis with added policy and health system changes into timelines could provide answers to this research question. Another future research direction could be toward analyzing the time lag between changes in the SDI and changes in indices using the observed/expected ratios for YLD and YLL from the GBD dataset. Analyzing which diseases are turning faster than others to more YLD, compared to YLL, could also be an interesting research topic. Another research agenda should be linked to the role of different public health interventions in YLD, as described above.
Limitations
The most important limitation of the ETE index is its simplified background hypothesis. Naturally, using YLD and YLL as one or one number is risky, as people are dying, for example, due to cardiovascular disease at a young age and therefore contribute to YLL values. Another example could be mortality caused by injuries, which often affect young people and contribute substantially to YLL values. On the other hand, there are infectious diseases that can progress to chronic diseases, such as HIV. Owing to ART treatments, people live many years with HIV, which has contributed to YLD values. Future work could include classifying disease groups more specifically according to YLL and YLD contributions and increasing the precision of the ETE index. In this paper we present only broad disease category analysis (Fig. 5) which is clearly a limitation. Nonetheless, we believe that the recent level of the index provides a useful tool and, certainly, a good starting point for additional research.
Use of regional or SDI group level analysis instead of individual country analysis is another limitation of the manuscript.
Using GBD data from 2019 release could be seen as a limitation at present due to missing out the Covid-19 pandemic impact on YLDs and YLLs. However, this limitation is at same time an opportunity for future research suggesting re-analysis of data after the GBD 2023 will be published.
Conclusions
We developed and presented the first results of a new index, the ETE, based on GBD study data to estimate the progression of epidemiologic transition. The index shows consistent results across time and across countries. After additional research on the issues discussed, it could be recommended that health policy makers assess the level of epidemiologic transition of a country and consider future health and social policy interventions.
Data availability
The source data that support the findings of this study are available from https://vizhub.healthdata.org/gbd-compare/. However, downloaded data are available from the corresponding authors upon reasonable request.
References
Omran, A. R. The epidemiologic transition: A theory of the epidemiology of population change. Milbank Q. 83, 731–757. https://doi.org/10.1111/j.1468-0009.2005.00398.x (2005).
Oni, T. & Unwin, N. Why the communicable/non-communicable disease dichotomy is problematic for public health control strategies: Iimplications of multimorbidity for health systems in an era of health transition. Int. Health. 7, 390–399. https://doi.org/10.1093/inthealth/ihv040 (2015).
Frenk, J. & Moon, S. Governance challenges in global health. N Engl. J. Med. 368, 936–942. https://doi.org/10.1056/NEJMra1109339 (2013).
Agyei-Mensah, S. & de-Graft Aikins, A. Epidemiological transition and the double burden of disease in Accra, Ghana. J. Urban Health. 87, 879–897. https://doi.org/10.1007/s11524-010-9492-y (2010).
Boutayeb, A. The double burden of communicable and non-communicable diseases in developing countries. Trans. R Soc. Trop. Med. Hyg. 100, 191–199. https://doi.org/10.1016/j.trstmh.2005.07.021 (2006).
Bygbjerg, I. C. Double burden of noncommunicable and infectious diseases in developing countries. Science 337, 1499–1501. https://doi.org/10.1126/science.1223466 (2012).
Kuate Defo, B. Beyond the ‘transition’ frameworks: The cross-continuum of health, disease and mortality framework. Glob Health Action. https://doi.org/10.3402/gha.v7.24804 (2014).
Temu, F., Leonhardt, M., Carter, J. & Thiam, S. Integration of non-communicable diseases in health care: Tackling the double burden of disease in African settings. Pan Afr. Med. J. https://doi.org/10.11604/pamj.2014.18.202.4086 (2014).
de Matos, R. C., do Nascimento, G., Fernandes, A. C. & Matos, C. Implementation and impact of integrated health and social care services: An umbrella review. J. Public. Health Pol. 45, 14–29. https://doi.org/10.1057/s41271-023-00465-y (2024).
Murray, C. J. L. (ed) The Global Burden of Disease: Summary; a Comprehensive Assessment of Mortality and Disability from Diseases, Injuries, and Risk Factors in 1990 and Projected To 2020 (Harvard School of Public health on behalf of the World Health organization and the World Bank, 1996).
Martinez, R., Soliz, P., Caixeta, R. & Ordunez, P. Reflection on modern methods: Years of life lost due to premature mortality-a versatile and comprehensive measure for monitoring non-communicable disease mortality. Int. J. Epidemiol. 48, 1367–1376. https://doi.org/10.1093/ije/dyy254 (2019).
Institute of Health Metrix and Evaluation (IHME). Global Burden of Disease (GBD) n.d. accessed May 10, (2024). https://www.healthdata.org/research-analysis/about-gbd
Institute of Health Metrix and Evaluation (IHME). Countries | GHDx n.d. Accessed 10 May (2024). https://ghdx.healthdata.org/countries
Lim, S. S. et al. Measuring the health-related sustainable development goals in 188 countries: A baseline analysis from the global burden of disease study 2015. Lancet 388, 1813–1850. https://doi.org/10.1016/S0140-6736(16)31467-2 (2016).
Pallardy, R. Accessed 13 February 2010 Haiti earthquake | Magnitude, Damage, Map, & Facts | Britannica 2025. (2025). https://www.britannica.com/event/2010-Haiti-earthquake
Clark, S. & Hamplová, D. Single motherhood and child mortality in Sub-Saharan Africa: A life course perspective. Demography 50, 1521–1549. https://doi.org/10.1007/s13524-013-0220-6 (2013).
Li, X. et al. Estimating the health impact of vaccination against ten pathogens in 98 low-income and middle-income countries from 2000 to 2030: A modelling study. Lancet 397, 398–408. https://doi.org/10.1016/S0140-6736(20)32657-X (2021).
Nayİr, T., Nazlican, E., Şahİn, M. & Kara, F. Effects of immunization program on morbidity and mortality rates ofvaccine-preventable diseases in Turkey. Turk. J. Med. Sci. 50, 1909–1915. https://doi.org/10.3906/sag-2008-177 (2020).
Petersen, I., Bhana, A., Lund, C. & Herrman, H. Primary Prevention of Mental Disorders. Early Intervention in Psychiatryp. 117–133 (Wiley, 2014). https://doi.org/10.1002/9781118557174.ch11
Wamba, A. A., Takah, N. F. & Johnman, C. The impact of interventions for the primary prevention of hypertension in Sub-Saharan Africa: A systematic review and meta-analysis. PLOS ONE. 14, e0219623. https://doi.org/10.1371/journal.pone.0219623 (2019).
Simeonsson, R. J. Primary, secondary, and tertiary prevention in early intervention. J. Early Interv. 15, 124–134. https://doi.org/10.1177/105381519101500202 (1991).
Straka, J., Šídlo, L. & Kulhánová, I. Trends in healthy life years between 2005 and 2019 in 31 European countries: The compression or expansion of morbidity?? Int. J. Public. Health. 69, 1607574. https://doi.org/10.3389/ijph.2024.1607574 (2024).
Stallard, E. Compression of morbidity and mortality: New perspectives. N Am. Actuar. J. 20, 341–354. https://doi.org/10.1080/10920277.2016.1227269 (2016).
Rieker, P. P. & Bird, C. E. Rethinking gender differences in health: why we need to integrate social and biological perspectives. J. Gerontol. Ser. B. 60, S40–S47. https://doi.org/10.1093/geronb/60.Special_Issue_2.S40 (2005).
Freedman, V. A., Wolf, D. A. & Spillman, B. C. Disability-Free life expectancy over 30 years: A growing female disadvantage in the US population. Am. J. Public. Health. 106, 1079–1085. https://doi.org/10.2105/AJPH.2016.303089 (2016).
Acknowledgements
None.
Funding
No funding was received.
Author information
Authors and Affiliations
Contributions
GG conceptualized the work, identified and analyzed the data and wrote the first draft of the manuscript. RZ downloaded the data and worked on analysis of data as well as commented on drafts of manuscript. ZM participate in conceptualization of the work, analysis and discussion part and edited the drafts of manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix 1: List of countries by region
Appendix 1: List of countries by region
Central Asia – Armenia, Azerbaijan, Georgia, Kazakhstan, Kyrgyzstan, Mongolia, Tajikistan, Turkmenistan, and Uzbekistan.
Central Europe – Albania, Bosnia and Herzegovina, Bulgaria, Croatia, Czechia, Hungary, Montenegro, North Macedonia, Poland, Romania, Serbia, Slovakia, and Slovenia.
Eastern Europe – Belarus, Estonia, Latvia, Lithuania, Republic of Moldova, Russian Federation, Ukraine.
Australasia – Australia and New Zealand.
High-income Asia Pacific – Brunei Darussalam, Japan, South Korea, Singapore.
High-income North America.- Canada, Greenland, USA.
Southern Latin America – Argentina, Chile, Uruguay.
Western Europe – Andorra, Austria, Belgium, Cyprus, Denmark, Finland, France, Germany, Greece, Iceland, Ireland, Israel, Italy, Luxembourg, Malta, Monaco, Netherlands, Norway, Portugal, San Marino, Spain, Sweden, Switzerland, and the United Kingdom.
Andean Latin America – Bolivia, Ecuador and Peru.
Caribbean – Bahamas, Barbados, Belize, Bermuda, Cuba, Dominican Republic, Grenada, Guyana, Haiti, Jamaica, Puerto Rico, Saint Kitts and Nevis, Saint Lucia, Saint Vincent and the Grenadines, Suriname, Trinidad and Tobago, United States Virgin Islands,
Central Latin America – Colombia, Costa Rica, El Salvador, Guatemala, Honduras, Mexico, Nicaragua, Panama and Venezuela.
Tropical Latin America – Brazil and Paraguay.
North Africa and Middle East – Afghanistan, Algeria, Bahrain, Egypt, Iran (Islamic Republic of), Iraq, Jordan, Kuwait, Lebanon, Libya, Morocco, Oman, Palestine, Qatar, Saudi Arabia, Sudan, the Syrian Arab Republic, Tunisia, Turkey, the United Arab Emirates and Yemen.
South Asia – Bangladesh, Bhutan, India, Nepal, and Pakistan.
East Asia – China, Democratic People’s Republic of Korea and Taiwan (Province of China).
Oceania - American Samoa, Cook Islands, Fiji, Guam, Kiribati, Marshall Islands, Micronesia (Federated States of), Nauru, Niue, Northern Mariana Islands, Palau, Papua New Guinea, Samoa, Solomon Islands, Tokelau, Tonga, Tuvalu, and Vanuatu.
Southeast Asia – Cambodia, Indonesia, Lao People’s Democratic Republic, Malaysia, the Maldives, Mauritius, Myanmar, the Philippines, Seychelles, Sri Lanka, Thailand, Timor-Leste, and Viet Nam.
Central Sub-Saharan Africa – Angola, Central African Republic, Congo, Democratic Republic of the Congo, Equatorial Guinea, and Gabon.
Eastern Sun-Saharan Africa – Burundi, Comoros, Djibouti, Eritrea, Ethiopia, Kenya, Madagascar, Malawi, Mozambique, Rwanda, Somalia, South Sudan, Uganda, the United Republic of Tanzania, and Zambia.
Southern Sub-Saharan Africa. - Botswana, Eswatini, Lesotho, Namibia, South Africa and Zimbabwe.
Western Sub-Saharan Africa – Benin, Burkina Faso, Cabo Verde, Cameroon, Chad, Côte d’Ivoire, Gambia, Ghana, Guinea, Guinea-Bissau, Liberia, Mali, Mauritania, Niger, Nigeria, Sao Tome and Principe, Senegal, Sierra Leone, and Togo.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Gulis, G., Zidkova, R. & Meier, Z. Changes in disease burden and epidemiological transitions. Sci Rep 15, 8961 (2025). https://doi.org/10.1038/s41598-025-94050-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-94050-w
Keywords
This article is cited by
-
The global burden and trends of esophageal cancer caused by smoking among men from 1990 to 2021 and projections to 2040: An analysis of the Global Burden of Disease 2021
European Journal of Medical Research (2025)
