
Abstract
Retrospective Study. This study investigates the effectiveness of preoperative vertebral computed tomography (CT) attenuation value classification in predicting cage subsidence in Oblique lumbar interbody fusion (OLIF) surgeries. This study aims to evaluate the feasibility of using CT attenuation value classification to predict cage subsidence. A retrospective analysis of L4-5 OLIF surgeries from May 2019 to June 2022, with over one year of follow-ups, was performed. Patients were classified into subsidence and non-subsidence groups based on postoperative outcomes. Demographic and perioperative variables, preoperative CT attenuation values, and changes in Oswestry Disability Index (ODI) and Visual Analog Scale (VAS) scores were compared. Of 112 patients (29 in the subsidence group, 83 in the non-subsidence group), significant differences in gender (P = 0.032) and DXA T-value (P = 0.010) were noted, with the subsidence group predominantly female. The consistency of CT attenuation values across L1-L5 vertebral bodies demonstrated strong reliability, with intraclass correlation coefficient (ICC) ranging from 0.76 to 0.91. CT attenuation values, categorized into osteoporosis, osteopenia, and regular bone mass groups, correlated significantly with bone density and subsidence, especially at the L1 vertebra (r = 0.548, P < 0.001). Multivariate logistic regression confirmed the predictive value of vertebral CT stratification, with L1-L5 Odds Ratios (OR) ranging from 0.07 to 0.26. Females are more prone to OLIF-related cage subsidence. The measurement of CT attenuation values demonstrated strong reliability and consistency. Preoperative vertebral CT attenuation value classification correlates with bone density and subsidence risk, particularly at the L1 vertebra, and strongly predicts cage subsidence.
Similar content being viewed by others
Introduction
Oblique Lumbar Interbody Fusion (OLIF) has garnered significant attention in minimally invasive spinal surgery for its benefits, including reduced trauma, minimal bleeding, and expedited recovery1,2. However, its associated postoperative complications, such as vascular injury, psoas muscle weakness, thigh numbness, bowel perforation, obstruction, and, notably, cage subsidence, warrant close attention3. Cage subsidence, with an incidence rate ranging from 8.3 to 46.7%4,5,6,7, presents a clinical conundrum: while some studies imply its detrimental effect on OLIF’s efficacy5,6, others suggest a negligible impact8,9. Regardless, understanding and mitigating cage subsidence remains crucial.
Recent advancements in imaging technology have elevated the role of vertebral body CT attenuation values in orthopedics, particularly in assessing bone strength and density, predicting fracture risk, and anticipating postoperative complications10,11. Despite this, the application of vertebral CT attenuation values in OLIF, especially Stand Alone OLIF (SA-OLIF)2,8,12,13, remains relatively unexplored. Emerging evidence proposes that OLIF, in conjunction with Bilateral Pedicle Screw Fixation (BPSF), enhances intervertebral stability, potentially lowering the likelihood of complications such as cage subsidence or displacement14,15.
Studies have shown that the occurrence of cage subsidence after OLIF surgery is closely associated with factors such as bone mineral density (BMD), cage placement, cage angle, patient age, and osteoporosis16,17,18. Among these, BMD and cage placement are considered the most significant factors. However, in another study, we also explored the impact of cage position and type on the outcomes of OLIF combined with PPSF (OLIF + PPSF) surgery, and the results indicated that the correlation between OLIF outcomes and cage position is relatively weak19. Therefore, this study primarily focuses on the relationship between CT attenuation values, BMD, and cage subsidence after OLIF surgery. We aim to evaluate the predictive ability of preoperative vertebral CT attenuation value classification for cage subsidence in OLIF combined with BPSF surgery, allowing for risk stratification of OLIF patients and identification of those at higher risk for cage subsidence, thereby enabling early intervention.
Materials and methods
Patients’ data
Informed consent Statement
As this study is retrospective in nature, approval was granted by the Ethics Committee of the First Affiliated Hospital of Guangzhou University of Chinese Medicine (No. JY2023-240), and the committee agreed to waive informed consent. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Research data sources
The follow-up data used in this study were primarily obtained from the hospital’s clinical records, imaging data, and patient follow-up files. During data integration, specialized software was employed to eliminate duplicate records and verify any discrepancies, ensuring the accuracy and integrity of the data. After this process, the completeness of the follow-up data was confirmed, with no missing values.
This study retrospectively analyzed 121 patients who underwent L4-5 OLIF in conjunction with BPSF from May 2019 to June 2022. Of these, 112 patients with complete follow-up data were included in the final analysis. We systematically collected demographic and perioperative data, as well as imaging data at preoperative, postoperative,3-month,6-month, and 12-month follow-up stages. Additionally, clinical Visual Analog Scale (VAS) and Oswestry Disability Index (ODI) scores were recorded at each time point for all included patients.
Inclusion and exclusion criteria
Inclusion criteria
(i) Adults diagnosed with mild to moderate lumbar spinal stenosis at the L4-5 level, optionally accompanied by I-II degree lumbar spondylolisthesis and undergone only L4/5 level OLIF and BPSF surgery. (ii) Patients with preoperative lumbar CT imaging and DXA examination. (iii) Those who have regular checkup after surgery and at least 1 year of lumbar CT imaging and clinical follow-up.
Exclusion criteria
(i) Patients who were scheduled for staged surgery; (ii)Patients who also received the cement augmentation at the same time. (iii) Those who have a spinal infection or other spinal destructive disease after surgery; (iv) Patients who have undergone secondary spinal surgery after OLIF for various reasons such as spine fracture, disc herniation recurrence, screws loosening rods broking, cage displacement .
Observation indicators
Imaging indicators
Preoperative and postoperative lumbar spine CT images at each follow-up time point were retrieved from the Picture Archiving and Communication System (PACS). CT attenuation values for each lumbar segment were recorded, and the presence or absence of cage subsidence was assessed.
CT attenuation values and classification
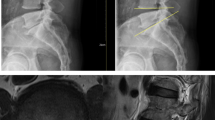
CT attenuation values measurement10: The CT attenuation values of each vertebral body from L1 to L5 were assessed using PACS. Measurements were taken at three sites below the upper endplate, central cancellous bone, and lower endplate. Care was taken to avoid cortical bone, osteophytes, and non-cancellous areas (Fig. 1). The CT attenuation values were obtained by averaging measurements from three professional spinal surgeons.
CT attenuation value classification: Following the methodology of Perry J20, vertebral CT attenuation values were classified into categories based on osteoporosis severity thresholds: values below 110 Hounsfield Units (HU) indicated osteoporosis, between 110 and 160 HU indicated osteopenia, and values above 160 HU signified average bone mass. This classification corresponds with the World Health Organization’s (WHO) defined bone density grading, where a T-score ≤ −2.5 indicates osteoporosis, a T-score between − 2.5 and − 1 indicates osteopenia and a T-score ≥ −1indicates normal bone mass21.
Cage subsidence diagnostic criteria
As per the criteria established by Pisano AJc22, cage subsidence was identified if postop.erative imaging revealed the fusion device penetrating the upper or lower endplate by a depth of 2 mm or more at any postoperative time point.
Measurement Method: Postoperative follow-up CT images in the sagittal plane were reviewed for all patients. The slices showing cage subsidence were identified, and the maximum distance between the cage and the endplate was measured, with the largest value recorded as the subsidence depth. This assessment was performed by two trained specialists, and discrepancies were resolved by consulting a third senior spine surgeon. Patients with subsidence were categorized into the subsidence group, while the rest were classified as non-subsidence. Illustrative examples of cage subsidence are shown in Fig. 2.
Dual-Energy X-Ray absorptiometry (DEXA)
All included patients routinely underwent dual-energy X-ray absorptiometry (DEXA) for bone mineral density assessment. The lumbar spine T-scores from the bone density reports of all included patients were retrieved and recorded.
Clinical indicators
Clinical Assessment: The study utilized the Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI) to evaluate clinical outcomes. VAS was bifurcated into back pain (VASb) and leg pain (VASl) components, recorded preoperatively and at one week, three months, six months, and twelve months postoperatively.
Perioperative Metrics: Collected data included Symptom duration, intraoperative blood loss, total operation time, and length of hospital stay.
Surgical method
The surgeries were conducted by three of the four senior spinal surgeons from our hospital. Surgical Procedure: Under anesthesia, patients were positioned in the right lateral decubitus posture, with the left abdominal side up to allow gravity-assisted displacement of abdominal contents. The knees were flexed to ease abdominal muscle tension. Supportive cushions were placed strategically for optimal positioning, and straps were used for spinal stability. Fluoroscopic guidance facilitated precise targeting of the intervertebral disc, followed by a 4–5 cm incision on the left lateral abdomen. A meticulous approach was taken to free abdominal muscles, blood vessels, and organs, with retractors used to expose the target disc. Post-disc and endplate clearance, an interbody fusion device loaded with artificial bone was inserted. Fluoroscopy confirmed device placement, and the incision was closed in layers. The patient was then repositioned for Bilateral Pedicle Screw Fixation (BPSF) on the fused segments.
Statistical methods
Data were analyzed using SPSS 25.0 (SPSS Inc.USA). Independent samples T-tests and Mann-Whitney tests were used to compare continuous variables between groups, and the Chi-square test for categorical variables. Consistency testing was employed to assess the accuracy of CT Attenuation Value measurements by different physicians. Spearman’s correlation analysis explored the relationship between preoperative L1-L5 vertebral body CT attenuation value classification and bone density grading. Multivariate logistic regression investigated the impact of preoperative L1-L5 vertebral body CT attenuation value classification on postoperative cage subsidence. Statistical significance was set at a p-value of less than 0.05.
Results
Preoperative baseline and perioperative data comparison
From the original cohort of 121 patients, nine were excluded due to non-compliance with follow-up, reoperation, mortality, and other factors, leading to the inclusion of 112 participants. Among the total cases, a notable 56 patients were diagnosed with lumbar spondylolisthesis. During the comprehensive one-year follow-up period, we did not observe any instances of failed fusion or inadequate integration of implanted prostheses.
There were 29 cases of cage subsidence postoperatively, constituting the subsidence group (25.89% incidence), with 4 males and 25 females, average age 61.62 ± 10.33 years, and bone density (T-value) of −2.27 ± 1.08. The non-subsidence group consisted of 83 individuals (29 males, 54 females), with an average age of 60.12 ± 8.93 years and a mean T-value of −1.75 ± 1.10. Notable statistical differences were observed in gender distribution and bone density between the two groups (P = 0.032, P = 0.010). No significant differences were observed between the groups in age, BMI, symptom duration, intraoperative blood loss, total operation time, or length of hospital stay (Table 1).
ICC analysis of CT attenuation value measurements
In this study, the inter-rater reliability of CT attenuation value measurements by three experienced spine surgeons was evaluated using the Intraclass Correlation Coefficient (ICC). The results showed that the ICC values for L1 and L2 were 0.91 (95% CI: 0.94, 0.88) and 0.94 (95% CI: 0.94, 0.87), respectively. For L3, the ICC was 0.90 (95% CI: 0.94, 0.85), for L4 it was 0.76 (95% CI: 0.82, 0.68), and for L5, it was 0.80 (95% CI: 0.85, 0.73). These results indicate high reliability in the CT attenuation value measurements for the L1-L5 vertebrae, with the highest consistency observed for L1 and L2.(Table 2).
Relationship between CT attenuation values and bone density (DXA T-values)
A significant correlation was identified between preoperative vertebral body CT attenuation value classification and bone density grading for L1-L5 vertebrae (P < 0.001). The correlation coefficients ranged from 0.457 for L5 to 0.548 for L1, with L1 exhibiting the strongest correlation (Table 3).
Relationship between CT attenuation value classification and postoperative cage subsidence
Multivariate logistic regression was performed using the CT attenuation value thresholds of 110 HU and 160 HU for preoperative L1-L5 vertebral body CT attenuation value classification, in conjunction with postoperative cage subsidence. The scatter plot depicting the distribution of CT attenuation value classifications for each segment and cage subsidence is shown in Fig. 3. The analysis indicated a statistically significant impact of preoperative CT attenuation values on cage subsidence (L1-L3:P < 0.001, L4:P = 0.001, L5:P = 0.002). Higher preoperative CT attenuation values were associated with a reduced risk of cage subsidence. The odds ratios (OR) were 0.07 for L1 (95% CI: 0.02–0.24), 0.12 for L2 (95% CI: 0.04–0.36), 0.08 for L3 (95% CI: 0.02–0.27), 0.22 for L4 (95% CI: 0.09–0.55), and 0.26 for L5 (95% CI: 0.11–0.61) (Table 4). Although age showed some differences in the multivariate regression analysis between L1-L3 CT attenuation value classifications and cage subsidence, their odds ratio (OR) were very close to 1, suggesting that their impact on subsidence is negligible in this study.
Comparison of clinical outcomes
Postoperative clinical assessments showed significant improvements in both groups compared to preoperative values, with a downward trend over time, reflecting positive surgical outcomes. A slight difference in VAS-back pain (VASb) scores was noted at the 12-month follow-up (P = 0.028) (Table 5).
Discussion
This study’s primary aim was to evaluate the efficacy of preoperative vertebral body CT attenuation value classification in predicting the risk of cage subsidence following OLIF combined with BPSF. Fang et al.‘s research indicates that OLIF with BPSF can alleviate stress on endplates of the fusion segment, potentially reducing cage subsidence compared to Stand Alone OLIF (SA-OLIF)23. Despite this, the risk of cage subsidence post-surgery remains a pertinent concern, Existing literature highlights that cage subsidence can lead to a progressive decrease in intervertebral space, spinal alignment imbalance, recurrence of nerve compression, and possibly poorer clinical outcomes, thereby increasing the likelihood of reoperation24. Thus, the ability to predict the risk of cage subsidence post-OLIF with BPSF through preoperative vertebral body CT attenuation value classification holds substantial clinical significance for perioperative planning and risk assessment.
Higher incidence of cage subsidence in females
The average age of patients in both study groups was around 60, with a higher proportion of females than males. Notably, in the subsidence group, the proportion of females was significantly higher than in the non-subsidence group. Given the age demographics, this gender disparity might be attributable to postmenopausal estrogen withdrawal, leading to osteoporosis in women25. Hao Chai et al.‘s research found that 33.2% of Chinese women post-menopause experience varying degrees of osteoporosis26. Moreover, men in the same age bracket generally have higher bone density in the trunk27. This gender-based discrepancy suggests that women are more prone to require lumbar spine surgery and are at a higher risk for cage subsidence due to osteoporosis, as the vertebral endplates in contact with the interbody fusion device may be more prone to collapse.
Correlation between cage subsidence, bone density and CT Attenuation value classification
Our findings indicate a significant difference in bone density T-values between subsidence and non-subsidence groups (P = 0.010) (Table 1). There was a marked statistical relationship between bone density T-value grading and vertebral body CT attenuation value classification (P < 0.001), particularly at L1 (r= 0.548) (Table 3). This consistency between vertebral CT attenuation values and DXA bone density measurements in osteoporosis detection and their close correlation suggests that preoperative measurement and classification of L1 vertebral body CT attenuation values can assess the degree of osteoporosis in patients, consistent with Gerety EL et al.‘s finding that L1 vertebral body bone density can represent the overall lumbar spine bone density28.
Preoperative Vertebral CT Attenuation Value Classification is an Effective Predictor of Cage Subsidence After OLIF Surgery
Postoperative cage subsidence in lumbar fusion surgery may relate to factors like bone mineral density (BMD), intervertebral space height, and cage positioning7. This study primarily investigated the cause from a bone density perspective. Although DXA has certain limitations in osteoporosis detection, it remains the internationally accepted gold standard for osteoporosis diagnosis29. Numerous studies have demonstrated that CT attenuation values can replace DXA in assessing vertebral bone density10,30,31. Our study demonstrates that in clinical settings, CT Attenuation Value measurements exhibit high consistency and reliability (Table 2), with ICC values of L1-5 ranging from 0.76 to 0.91. Furthermore, the CT Attenuation Value levels are closely correlated with bone density classifications (Table 3, P < 0.001).
Based on a large sample, Perry J et al.‘s research concluded that CT attenuation values are highly sensitive and specific for bone density, especially when thresholds of 110 HU and 160 HU are utilized20. Deshpande N et al. also identified ≤ 110HU and >160HU as crucial thresholds for vertebral osteoporosis assessment29. Besides, while VBQ is indeed a promising tool, its application is still in the exploratory phase. Hiyama A et al.’s study indicated that compared to CT attenuation values, VBQ shows a weaker correlation with bone mineral density and is less reliable in assessing bone quality32. Consequently, our study primarily relied on CT imaging and other clinical assessments to evaluate bone quality.
Accordingly, we categorized vertebral CT attenuation values into osteoporosis, osteopenia, and normal bone mass groups and conducted multivariate logistic regression analysis with cage subsidence. The results indicated a significant impact of preoperative L1-L5 vertebral body CT attenuation value classification on postoperative cage subsidence (P≤ 0.001), with higher preoperative CT attenuation values potentially acting as a protective factor against cage subsidence (OR values for L1-L5 were 0.07, 0.12, 0.08, 0.22, and 0.26, respectively) (Table 4). This study’s findings underscore that cage subsidence is intricately linked to osteoporosis severity, likely due to compromised bone quality in osteoporotic patients, causing increased stress on the fusion device within the fusion segment33.
The impact of cage subsidence on clinical outcomes May be evident only with Long-Term Follow-Up
In this study, most cases of cage subsidence OLIF occurred immediately after surgery and the 3–6 month follow-up, consistent with findings by Long Zhao et al.34 For example, a 64-year-old female with chronic back and leg pain underwent L4-5 OLIF for disc herniation. Preoperative assessments showed osteoporosis (bone density T-value of −2.7 and an average L1CT attenuation value of 108.57 HU). Postoperatively, pain relief was significant, with no immediate cage subsidence but slight embedding at L4-5 endplates. At six months, leg pain was resolved, occasional back pain managed with NSAIDs or physical therapy. Imaging revealed cage subsidence between L4-5, with depths of 2.07 mm (L4) and 2.61 mm (L5). (Fig. 4).
Our investigation into clinical effectiveness revealed that subsidence and non-subsidence groups exhibited comparable postoperative recovery and functional improvements in the short term (Table 5). Hiyama A et al. have shown that osteoporosis increases the risk of cage subsidence after lateral surgery, but does not affect short-term pain relief or quality of life improvement, which is consistent with our findings35,36. Although there was a statistical difference in VASb scores between the subsidence and non-subsidence groups at 12 months postoperatively (P = 0.028), the difference was minimal. This suggests that cage subsidence has limited impact on short-term clinical outcomes, with its potential effect likely becoming evident in long-term (> 1 year) follow-up.
CT Attenuation value classification enhances perioperative management in OLIF surgery
By using CT Attenuation Value classifications to identify OLIF patients at risk for postoperative cage subsidence, preoperative interventions, such as bisphosphonates or teriparatide, can be employed to improve bone density and reduce the likelihood of subsidence37,38. Additionally, personalized treatment plans can be developed. For example, in patients at high risk for subsidence, the need for pedicle screw reinforcement during surgery can be evaluated to enhance vertebral stability and prevent endplate collapse and cage subsidence in the short term.
Limitations
The study is subject to certain limitations: First, its retrospective nature inherently carries the risk of selection and recall biases. Second, the manual measurement of CT attenuation values introduces a margin for error. Third, the small sample size and limited follow-up period call for larger-scale, long-term prospective studies for more definitive conclusions.
Conclusions
Preoperative vertebral body CT attenuation value classification demonstrates a robust predictive capability for cage subsidence following OLIF. A higher preoperative CT attenuation value classification mitigates the risk of postoperative cage subsidence. The L1 vertebral body CT attenuation value grade can reflect the overall lumbar spine bone density, allowing for the assessment of a patient’s approximate risk of postoperative cage subsidence through preoperative measurement and grading of L1 vertebral body CT attenuation values. Additionally, our findings indicate that the clinical impact of cage subsidence is minimal in the short term but potentially significant in long-term follow-up. This underscores the importance of preoperative assessment and patient-specific risk classification in planning and executing OLIF procedures.

The method for measuring CT attenuation values, taking the L1 vertebra as an example, involves three different layers: (A) just below the upper endplate, (B) the middle of the vertebral body, and (C) just above the lower endplate. During measurement, areas such as the bone cortex, nutrient foramina, or bone islands should be avoided. The average HU obtained from A, B, and C represents the HU on CT for this vertebra.

(A) and (B): No cage subsidence occurred. (C) and (D): Cage subsidence occurred.

Scatter plot of CT value classifications between cage subsidence and non-cage subsidence groups in L1-L5.

A 64-year-old female patient, suffering from recurrent lower back pain for over ten years, accompanied by bilateral leg pain for two years, was diagnosed with lumbar disc herniation and underwent an OLIF surgery at the L4-5 level. (A): Preoperative sagittal lumbar CT; (B): Postoperative lumbar CT, demonstrated satisfactory decompression of the spinal canal, with the cage securely in place. (C): Six-month postoperative lumbar CT showed that the cage had penetrated the endplates, becoming embedded between the lower endplate of L4 and the upper endplate of L5.
Data availability
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
References
Li, R., Shao, X., Li, X., Liu, Y. & Jiang, W. Comparison of clinical outcomes and spino-pelvic sagittal balance in degenerative lumbar spondylolisthesis: minimally invasive oblique lumbar interbody fusion (OLIF) versus transforaminal lumbar interbody fusion (TLIF). Med. (Baltim). 100, e23783 (2021).
Liu, A. F. et al. Efficacy and safety of oblique lumbar interbody fusion versus transforaminal lumbar interbody fusion for degenerative lumbar spondylolisthesis: A systematic review and Meta-Analysis. World Neurosurg. 158, e964–964e974 (2022).
Cheng, C., Wang, K., Zhang, C., Wu, H. & Jian, F. Clinical results and complications associated with oblique lumbar interbody fusion technique. Ann. Transl Med. 9, 16 (2021).
He, D. et al. Clinical and radiographic comparison of oblique lateral lumbar interbody fusion and minimally invasive transforaminal lumbar interbody fusion in patients with L4/5 grade-1 degenerative spondylolisthesis. Orthop. Surg. 15, 1477–1487 (2023).
Kotheeranurak, V. et al. Subsidence of interbody cage following oblique lateral interbody fusion: an analysis and potential risk factors. Global Spine J. 13, 1981–1991 (2023).
Lefèvre, E. et al. Implications of cage impactions in single-level OLIF treatment of degenerative spondylolisthesis. Orthop. Traumatol. Surg. Res. 109, 103385 (2023).
Yao, Y. C. et al. Risk factors of cage subsidence in patients received minimally invasive transforaminal lumbar interbody fusion. Spine (Phila Pa. 1976). 45, E1279–1279E1285 (2020).
Wu, H. et al. The role of Hounsfield unit in intraoperative endplate violation and delayed cage subsidence with oblique lateral interbody fusion. Global Spine J. 13(7), 1829–1839. https://doi.org/10.1177/21925682211052515 (2023). PMID: 34736351; PMCID: PMC10556897.
Zhou, J., Zhou, L., Liu, C., Yuan, C. & Wang, J. [CT Attenuation value of vertebral body predicting cage subsidence after stand-alone oblique lumbar interbody fusion]. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 35, 1449–1456 (2021).
Schreiber, J. J., Anderson, P. A., Rosas, H. G., Buchholz, A. L. & Au, A. G. Hounsfield units for assessing bone mineral density and strength: a tool for osteoporosis management. J. Bone Joint Surg. Am. 93, 1057–1063 (2011).
Zaidi, Q., Danisa, O. A. & Cheng, W. Measurement Techniques and Utility of Hounsfield Unit Values for Assessment of Bone Quality Prior to Spinal Instrumentation: A Review of Current Literature. Spine (Phila Pa 1976). ;44:E239-239E244. (2019).
Zhou, J. et al. Assessment of vertebral bone mineral density and stand-alone oblique lumbar interbody fusion for adjacent segment disease and primary lumbar degenerative diseases. J. Orthop. Surg. (Hong Kong). 30, 10225536221091846 (2022).
Zhou, J., Yuan, C., Liu, C., Zhou, L. & Wang, J. Hounsfield unit value on CT as a predictor of cage subsidence following stand-alone oblique lumbar interbody fusion for the treatment of degenerative lumbar diseases. BMC Musculoskelet. Disord. 22, 960 (2021).
Guo, H. Z. et al. Stability evaluation of oblique lumbar interbody fusion constructs with various fixation options: A finite element analysis based on Three-Dimensional scanning models. World Neurosurg. 138, e530–530e538 (2020).
Song, C. et al. Biomechanical evaluation of oblique lumbar interbody fusion with various fixation options: A finite element analysis. Orthop. Surg. 13, 517–529 (2021).
Shen, S., You, X., Ren, Y. & Ye, S. Risk factors of cage subsidence following oblique lumbar interbody fusion: A Meta-analysis and systematic review. World Neurosurg. 183, 180–186 (2024).
Chen, K. J. et al. The impact of cage and end plate-Related factors on cage subsidence in oblique lateral interbody fusion. World Neurosurg. 173, e629–629e638 (2023).
Ran, L., Xie, T., Zhao, L., Huang, S. & Zeng, J. Low Hounsfield units on computed tomography are associated with cage subsidence following oblique lumbar interbody fusion (OLIF). Spine J. 22, 957–964 (2022).
Chen, X. et al. Oblique lumbar interbody fusion combined with posterior percutaneous pedicle screw internal fixation: does variability in cage position influence clinical outcomes. World Neurosurg. 189, e904–904e911 (2024).
Pickhardt, P. J. et al. Opportunistic screening for osteoporosis using abdominal computed tomography scans obtained for other indications. Ann. Intern. Med. 158, 588–595 (2013).
Yu, J. S. et al. ACR appropriateness Criteria® osteoporosis and bone mineral density: 2022 update. J. Am. Coll. Radiol. 19, S417–417S432 (2022).
Pisano, A. J. et al. Lumbar disc height and vertebral Hounsfield units: association with interbody cage subsidence. Neurosurg. Focus. 49, E9 (2020).
Fang, G. et al. Biomechanical comparison of Stand-Alone and bilateral pedicle screw fixation for oblique lumbar interbody fusion Surgery-A finite element analysis. World Neurosurg. 141, e204–204e212 (2020).
Rentenberger, C. et al. Perioperative risk factors for early revisions in Stand-Alone lateral lumbar interbody fusion. World Neurosurg. 134, e657–657e663 (2020).
Liang, G., Kow, A., Tham, C. L., Ho, Y. C. & Lee, M. T. Ameliorative effect of tocotrienols on Perimenopausal-Associated Osteoporosis-A review. Antioxid. (Basel). 11, 2179 (2022).
Chai, H., Ge, J., Li, L., Li, J. & Ye, Y. Hypertension is associated with osteoporosis: a case-control study in Chinese postmenopausal women. BMC Musculoskelet. Disord. 22, 253 (2021).
Nieves, J. W. et al. Males have larger skeletal size and bone mass than females, despite comparable body size. J. Bone Min. Res. 20, 529–535 (2005).
Gerety, E. L., Hopper, M. A. & Bearcroft, P. W. The reliability of measuring the density of the L1 vertebral body on CT imaging as a predictor of bone mineral density. Clin Radiol. ;72:177.e9-177.e15. (2017).
Deshpande, N. et al. Alternatives to DEXA for the assessment of bone density: a systematic review of the literature and future recommendations. J. Neurosurg. Spine. 38, 436–445 (2023).
Hendrickson, N. R., Pickhardt, P. J., Del Rio, A. M., Rosas, H. G. & Anderson, P. A. Bone mineral density T-Scores derived from CT Attenuation numbers (Hounsfield Units): Clinical Utility and Correlation with Dual-energy X-ray Absorptiometry. Iowa Orthop. J. 38, 25–31 (2018).
Lee, S., Chung, C. K., Oh, S. H. & Park, S. B. Correlation between bone mineral density measured by Dual-Energy X-Ray absorptiometry and Hounsfield units measured by diagnostic CT in lumbar spine. J. Korean Neurosurg. Soc. 54, 384–389 (2013).
Hiyama, A., Sakai, D., Katoh, H., Sato, M. & Watanabe, M. Hounsfield unit values as an adjunct diagnostic tool: investigating its relationship with bone mineral density and vertebral bone quality in lumbar degenerative disease patients. World Neurosurg. 183, e722–722e729 (2024).
Liu, Z. X. et al. Effects of osteoporosis on the biomechanics of various supplemental fixations co-applied with oblique lumbar interbody fusion (OLIF): a finite element analysis. BMC Musculoskelet. Disord. 23, 794 (2022).
Zhao, L. et al. Clinical and radiological evaluation of cage subsidence following oblique lumbar interbody fusion combined with anterolateral fixation. BMC Musculoskelet. Disord. 23, 214 (2022).
Hiyama, A., Sakai, D., Katoh, H., Sato, M. & Watanabe, M. Does bone density affect outcomes in lateral lumbar interbody fusion?? A propensity Score-Matched analysis of preoperative Hounsfield units. J. Clin. Med. 13, 6374 (2024).
Hiyama, A., Sakai, D., Katoh, H., Sato, M. & Watanabe, M. Impact of osteoporosis on Short-Term surgical outcomes in lumbar degenerative disease patients undergoing lateral lumbar interbody fusion: A retrospective analysis. World Neurosurg. 188, e424–424e433 (2024).
Hudson, M. et al. Evaluating osteoporosis and bone quality in the aging spine: modern considerations for surgical management in the geriatric population. Geroscience 46, 5287–5301 (2024).
McClung, M. R. Role of bone-forming agents in the management of osteoporosis. Aging Clin. Exp. Res. 33, 775–791 (2021).
Author information
Authors and Affiliations
Contributions
Conceptualization: Wanyan Chen, Guangye Zhu, Zefeng Song, De Liang, Xiaobing Jiang. Formal Analysis: Guangye Zhu, Xingda Chen, Guibo Liang. Data curation: Wanyan Chen, Zefeng Song, Xingda Chen, Riwei Tan, Guibo Liang, RUEISHIUAN JIANG. Methodology: Wanyan Chen, Zefeng Song, Zelin Zhou, Jingjing Tang. Project Administration: Guangye Zhu, Zelin Zhou, Hui Ren, Jingjing Tang, Xiaobing Jiang. Writing-Original Draft: Wanyan Chen, Guangye Zhu, Riwei Tan, RUEISHIUAN JIANG. Writing-Review&Editing: Wanyan Chen, Zefeng Song, Hui Ren, De Liang, Xiaobing Jiang.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the First Affiliated Hospital of Guangzhou University of Chinese Medicine (No. JY2023-240) and the ethics committee agreed to waive informed consent.
Consent for publication
This work has not been published previously, it is not under consideration for.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Chen, W., Zhu, G., Song, Z. et al. Preoperative CT attenuation value classification assesses cage subsidence risk in 112 OLIF surgery cases. Sci Rep 15, 10276 (2025). https://doi.org/10.1038/s41598-025-94696-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-94696-6
