
Abstract
The aim of this study was to evaluate the features of the root canals cross-sectional shape at the coronal, middle, and apical levels using cone beam computed tomography (CBCT) among residents of Moscow region. CBCT images of 560 patients were analysed. The cross-sectional shape was determined in the horizontal plane at the coronal, middle and apical thirds of the root canal on intact teeth. The root canal shape was determined as follows: round, oval, and ribbon-like. The root canals of the maxillary anterior teeth belong to the canals with a constant cross-sectional shape from the coronal to the apex, while for mandibular anterior teeth it might change in the apical area. In premolars, oval shape was found in almost 70.0%, ribbon-like shape in 30.0%. For maxillary molars, a changing shape in the middle and apical thirds was established in the mesio-buccal and disto-buccal canals. In the mandibular molars, the shape of the canals changed in the middle and apical thirds of mesial and distal roots. The high occurrence of oval and ribbon-shaped canals, especially in the apical region, may be a problem in their processing and requires further study.
Similar content being viewed by others

Introduction
Endodontic treatment is one of the most common treatments in dental fields, which treat pulp diseases1. The success of endodontic treatment relies on several important factors, one of them the precise knowledge of the anatomy and morphology of the root canals2,3,4,5. The anatomy and morphology of root canal system varies among races and populations; this variation could be caused by the continuous growth of inner and outer enamel epithelial cells6,7. Insufficient knowledge of these variations could result in missing canals and cause treatment failure due to the presence of microorganisms and necrotic tissues8,9. The variation in the root canal system is not limited to the number of roots and root canal configuration; it also includes the cross-sectional root canal shape, which might not be consistent along the entire length.
The cross-sectional root canal shape differs from the ideal round. Root canals have various shapes: round, oval, long oval, ribbon-like shaped, C-shaped, and irregular shape. Jou et al. (2004) has classified cross-sectional shapes as round, oval, long oval, ribbon-like10. The oval canal has wider diameters than round ones, while long ovals have 2 times long diameter than oval ones and was observed in 50% in the apical third of the mandibular incisors11. Ribbon like canals belong to the canals that have isthmus, like mesial canals of mandibular molars and mesio-buccal canals of maxillary molars12. Several research in the literature have studied the anatomy and root canal morphology according to Vertucci classification, in which the canals configuration was identified while, few of them have studied the cross-sectional shape of the canals13,14,15,16,17,18,19.
To study the root canal shape, different techniques were used, like micro-CT and CBCT. In Brazil 2014, Fumes et al. used micro-CT to study the shape of root canal in the apical third of the first and second molars and found that oval shape was observed in 30% and 10% of mesio-buccal root of first and second molars, respectively, and a ribbon-like shape was found in more than 40% of both teeth, while in palatal and disto-buccal root the oval shape was mostly found20. Another study by Marceliano-Alves et al. (2018) determined that the root canal morphology of single-rooted canines varied greatly at different root levels21.
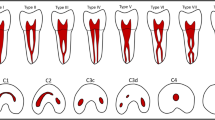
In our previous study, we confirmed that canal shape might change along the root canal, and a new classification was presented as follows: Type (1) Unchanging root canal shape from orifice to apex, Type (2) Changing shape of the canal in the middle part, Type (3) Changing shape of the canal in the apical part, Type (4) Changing shape of the canal in the middle and apical parts22. In the study, we evaluated the root canal shape at the coronal, middle and apical levels.
Materials and methods
This cross-sectional study was conducted to assess the cross-sectional shape of the root canal in three parts, coronal, middle and third among residents of the Moscow region.
Sample size was determined according to other studies of Hu et al.23,24, this study included 560 CBCT scans for people, aged (20–70) years. The study was performed according to the Helsinki Declaration of 1975, as revised in 2013, and was approved by the ethical committee of the Peoples’ Friendship University of Russia University (Protocol 6 at 21.02.2019). CBCT for patients were analysed from the archive of the university clinic and three-dimensional radiologic centre in Moscow. Informed consent was obtained from all subjects, whose CBCT was evaluated.
Inclusion Criteria were intact teeth without decay, fillings or restorations. Teeth treated endodontically or with large restoration or crowns were excluded from the study.
The CBCT scans were taken using a 3D eXam (KaVo, Biberach, Germany) with standard exposure settings (23 cm × 17 cm field of view, 0.3 mm voxel size, 110 kv, 1.6–20 s) and were viewed by the examiners in a semi-dark room using I-CAT viewer software (version 10, Hatfield, UK).
The CBCT scans were analysed by three examiners separately, and the disagreement between the results were discussed and reevaluated until a consensus was reached. For reproducibility, 4 weeks after the first evaluation, the examiners re-analysed 50 randomly scans and the results showed no statistically significant difference between the three examiners.
The root canal shape was determined in the axial plane at the level of coronal, middle third and in the apical third. The levels of the sections of anterior teeth were determined in the sagittal plane, for premolars and molars coronal plane was used to determine the levels of the sections. The levels were as follow: Coronal third: at the cementoenamel junction; Middle third was determined by the middle of the distance from the coronal to the apical points of all groups of teeth (the length of the root was measured and the middle third was determined according to that); Apical third: 3 mm from the apical foramen in teeth with a straight root, 3–5 mm from the apical foramen in case of apical root curvature especially in molar teeth.
The cross-sectional shape of the anterior group of teeth was assessed in the axial plane perpendicular to the axis of the tooth root. For molars and premolars, especially in the maxillary molars, the canal shape was assessed in each root separately. In this case, the cross-section of the coronal, middle and apical thirds was assessed in the axial plane perpendicular to the axis of each root. The cross-sectional shape was described as round if the measurements in two diameters were close in value, oval if the two perpendicular diameters differed by no more than 1 to 2. A ribbon-shaped shape was determined when the ratio of two diameters was more than 1 to 2 and in the presence of an isthmus.
When determining the root canal shape, the following terms were used: round—close in shape to a circle, oval—with a transverse size less than the longitudinal size by half, and ribbon-like—the longitudinal size is more than 2 times larger than the transverse one. Ribbon-like canals were described according to the classification of Hsy and Kim12. C-canals have been described as ribbon-like. The cross-sectional shape of the root canal of single-rooted and multi-rooted teeth was analysed. Only intact teeth were included in the study.
C-shaped canals were described as ribbon-like according to Hsy and Kim classification12:
-
Ribbon type 1: incomplete isthmus; weak connection between two canals.
-
Ribbon type 2: a continuous isthmus between 2 canals.
-
Ribbon type 3: 2 canals with very short, complete isthmus.
-
Ribbon type 4: complete or incomplete isthmus between three or more canals.
-
Ribbon type 5 is indicated by two or three canals with no visible connections between them.
For multi-rooted teeth, the shape of the root canal was studied for each root separately.
Statistical analysis was performed using IBM SPSS Statistics Version 22 for Windows (IBM®, NY, USA). The prevalence of the root canal shapes was analysed as percent. The asymmetry between the root canal shape of the teeth in the same arch was compared using Independent t-test. Statistical significance was set at 0.05.
Results
The study of root canal shape at the coronal, middle and apical parts showed that the shape is not constant; it changes depending on the number of canals in the root, the presence or absence of isthmuses. When analysing the maxillary anterior teeth, it was found that the shape of the central and lateral incisors in the upper jaw in 100% is round throughout its entire length (Table 1). The canines of the upper jaw and low jaw are characterized by an oval shape in 100%, which is preserved throughout its entire length (Table 1; Fig. 1). An analysis of the root canal shape of maxillary first and second two-rooted pre-molar showed that in the coronal third round shape was in 37.7% of cases, and oval in 62.3%. In the single-rooted maxillary premolars, in the coronal third, an oval shape, a ribbon-like type 1 and ribbon-like type 5 were revealed. In the middle and apical thirds, the ribbon-like type 1 changes into ribbon-like type 5 (Table 2; Figs. 1 and 2). In the maxillary molars, In MB in the coronal and middle thirds, a ribbon-like type 1 was detected and changed to oval or round in some cases in the apical third (Table 3; Fig. 2).

Cross-sectional root canal shape of maxillary anterior and premolar teeth, (A) Coronal third, (B) Middle Third, (C) Apical third.

Cross-sectional root canal shape of maxillary premolar and molars, (A) Coronal third, (B) Middle Third, (C) Apical third.
The mandibular central and lateral incisors are characterized by an oval shape of the root canal, which does not change throughout its entire length in 99% (Table 4; Fig. 3). In the mandibular premolars, the oval shape was found to change in some cases to round or ribbon-like in the apical third (Table 5). For mandibular molars the distal root was found to have an oval or ribbon-like shape of the 1st and 5th types, which changed in some cases in the apical third. For the mesial root in the coronal third ribbon-like shape of the 1st and 2nd types were observed. In the middle third, the number of type 1 ribbon-like decreased by 7 times and they were not detected in the apical part, while the number of ribbon-like of the 5th type in the middle and apical thirds has increased (Table 6; Figs. 4 and 5).

Cross-sectional root canal shape of mandibular anterior teeth, (A) Coronal third, (B) Middle Third, (C) Apical third. In incisors, the oval canal changed to ribbon shape in middle and apical thirds.

Cross-sectional root canal shape of mandibular premolars and first molar, (A) Coronal third, (B) Middle Third, (C) Apical third.

Cross-sectional root canal shape of mandibular second molar where oval canal was observed in both roots, (A) Coronal third, (B) Middle Third, (C) Apical third.
For maxillary and mandibular anterior and premolar teeth, no asymmetry was found between the teeth in the same arche (P ˃ 0.05), also no asymmetry was observed for disto-buccal, palatal root of maxillary molars, and for distal roots of mandibular molars (P ˃ 0.05). The asymmetry of root canal shape was observed in the apical third for mesio-buccal roots of first and second molar (P = 0.02) and for mesial roots of mandibular molars (P = 0.03).
Discussion
Planning for endodontic treatment and predicting its results could be achieved nowadays by the development of three-dimensional radiological methods. These techniques expand the knowledge of root canal systems and minimize the failure rate after endodontic treatment, as they could be used to identify the missing canals, the canal configuration and shape25,26.
An analysis of the cross-sectional root canal shape and the changes along its entire length, made it possible to establish constant canals that don’t change their shape and canals with a change shape. A change in the root canal shape was observed in the middle part, in the apical, as well as in both the middle and apical parts. This change in the root canal shape to oval or ribbon-like, especially in the middle or apical parts, makes it problematic to prepare this part of the root canal with a round instrument (Fig. 6).

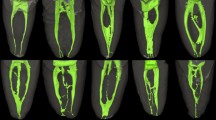
Example of cross-sectional root canal shape change from coronal third in mandibular second molars. (A–C) A case of changing shape from ribbon-like in mesial root to round in the apical third and from oval to round in distal root. (D–F) A case of changing oval shape in mesial root coronal third to ribbon like in middle and apical thirds.
In this study, on the upper jaw oval shape in the apical third was found in canines 100%, premolars 70%, molars 20–30% in the MB, and 14–19% in the DB. The ribbon-like shape of root canal was determined in 14.9% of premolars and in 70.5% of the mesio-buccal root. On the lower jaw, incisors in 99.2%, canines in 100%, premolars in 29.4%, molars in 94.8% have an oval shape in the apical third of the root canal. The ribbon-like shape of root canal was determined in incisors 0.8%, in premolars 6.6%, and in molars: in the distal root 8.8% and in the mesial 95.8%. The data were presented in Table 7.
In 2015, Batyukov et al.27 studied the anatomy of maxillary molars in the Russian population. Ribbon-like canals were detected in the MB canal of the first (43.7%) and second (34.3%) molars. In the mandibular molars, the cross-sectional shape was determined in the distal root as long oval in 32.3%, ribbon-like in 67.6%, these results coincide with our results.
In 2019, Kacharaju et al. studied the root canal morphology of mandibular premolars in a Malaysian population. The study was carried out on extracted teeth and, according to the results, at the coronal part oval shape was observed in 52%, round shape in 1% and in 46% undefined shape. While in the middle part, an oval canal was found in 36%, round in 21%, undefined shape in 30%, ribbon-like with an isthmus in 7%, and ribbon-like without isthmus in 6%. The shape of the root canal has changed in the apical third, oval canal was observed in 22%, a round in 37%, an undefined in 25%, ribbon-like with an isthmus in 8%, and ribbon-like without an isthmus in 8%28. The differences from our study could be related to genetics factors.
Bueno (2020) studied the cross-sectional shape of root canals at three levels: coronal, middle and apical, using a special CBCT program that improved the visualization of the canal shape. The authors concluded that in human permanent teeth, the cross section of the canals varies depending on the group of teeth and the third of the root. The highest frequency of round canal at a distance of 1 and 2 mm from the apex was found in the mandibular central incisors and first and second premolars. Oval-shaped canals were found in almost all groups of teeth and thirds of the roots29.
A high percentage of oval and ribbon-like canals in the upper and lower jaws, especially in the apical area, makes it difficult to perform high-quality instrumentation with a round instrument. The results of this study coincide with the results of Fumes19 and Bueno29, which noted that canals with an oval shape were found in almost all groups of teeth and thirds of the roots.
The planning for endodontic treatment and treatment protocol should be based on an accurate knowledge of the anatomy of the root canal system. Choosing the instruments and the root canal preparation technique will determine the efficacy and validity of this stage, and that will lead to a better prognosis30,31. Knowledge of root canal morphology and the changes of its shape and configuration is considered a basic requirement for successful endodontic treatment32,33.
Different variants of root canal shapes require different root canal preparation and obturation techniques. Canals could have various shapes in cross-section, round, oval, ribbon-like. The preparation of oval and ribbon-like canals with round instruments cannot give its round shape and can potentially lead to complications during endodontic treatment34,35,36,37,38,39,40.
Within the limitation of this study, we can conclude that oval or ribbon-like shape at the apical third of the canal makes it impossible to instrument them with round instruments. The ribbon-like shape might not be effectively prepared by rotary instruments as the taper of the root canals is higher than most preparation instruments. Therefore, irrigation becomes an important aspect. The use of traditional irrigants (sodium hypochlorite 3%) must be combined with activation that ensures efficiency in the apical zone (laser activation, sound activation), and this should be investigated in future studies, as not too many studies in the literature have investigated the instrumentation according to root canal shape.
Conclusions
Within the limitation of this study, a high percentage of the incidence of oval and ribbon-like canals, especially in the apical region, is a problem in their processing and obturation, which requires a revision of the relevant protocols and further study of the issue.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
References
Wu, D. et al. Root canal morphology of maxillary and mandibular first premolars analyzed using cone-beam computed tomography in a Shandong Chinese population. Medicine (Baltimore) 99 (20), e20116 (2020).
Dou, L., Li, D., Xu, T., Tang, Y. & Yang, D. Root anatomy and canal morphology of mandibular first premolars in a Chinese population. Sci. Rep. 7 (1), 750 (2017).
Tang, L., Sun, T. Q., Gao, X. J., Zhou, X. D. & Huang, D. M. Tooth anatomy risk factors influencing root canal working length accessibility. Int. J. Oral Sci. 3 (3), 135–140 (2011).
Wolf, T. G., Waber, A. L. & Marroquín, B. Morphology of the physiological foramen: II. Maxillary and mandibular premolars. J. Endod. 50 (6), 807–813 (2024).
Ginjeira, A. et al. Influence of root shape on canal complexity at the mandibular molar apical surgical resection level: A micro-CT study. Arch. Oral Biol. 164, 105983 (2024).
Tamanna, S., Rehman, A., Tewari, R. K. & Mishra, S. K. A segmental root development as an unusual healing response to the revitalization of mandibular second premolar. J. Indian Soc. Pedod. Prev. Dent. 40 (1), 94–97 (2022).
Kumakami-Sakano, M., Otsu, K., Fujiwara, N. & Harada, H. Regulatory mechanisms of Hertwig׳s epithelial root sheath formation and anomaly correlated with root length. Exp. Cell. Res. 325 (2), 78–82 (2014).
Buchanan, G. D., Gamieldien, M. Y., Tredoux, S. & Vally, Z. I. Root and canal configurations of maxillary premolars in a South African subpopulation using cone beam computed tomography and two classification systems. J. Oral Sci. 62 (1), 93–97 (2020).
Desai, K. S., Arora, A. V., Kapoor, S. V., Shah, P. B. & Rathore, Y. R. Cone-beam computed tomographic analysis of canal convolution in mesial root of mandibular second molars and a proposed new classification. J. Conserv. Dent. Endod. 27 (7), 714–718 (2024).
Jou, Y. T., Karabucak, B., Levin, J. & Liu, D. Endodontic working width: current concepts and techniques. Dent. Clin. North Am. 48 (1), 323–335 (2004).
Wu, M. K., R’oris, A., Barkis, D. & Wesselink, P. R. Prevalence and extent of long oval canals in the apical third. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 89 (6), 739–743 (2000).
Hsu, Y. Y. & Kim, S. The resected root surface. The issue of canal isthmuses. Dent. Clin. North Am. 41 (3), 529–540 (1997).
Jonker, C. H., L’Abbé, E. N., Van der Vyver, P. J., Zahra, D. & Oettlé, A. C. A micro-computed tomographic evaluation of maxillary first molar root canal morphology in black South Africans. J. Oral Sci. 66 (3), 151–156 (2024).
Mohammadzadeh-Akhlaghi, N., Mehrvarzfar, P., Hossein, M. & Dds, Z. Incidence, location, and type of isthmus in mandibular second molars among individuals of an Iranian population. J. Oral Health Oral Epidemiol. 7, 59–63 (2018).
Mohammadzadeh Akhlaghi, N. et al. Root canal anatomy and morphology of mandibular first molars in a selected Iranian population: an in vitro study. Iran. Endod. J. 12 (1), 87–91 (2017).
Džanković, A. et al. Exploring the root canal morphology of third molars in the Bosnia and Herzegovina population. Acta Stomatol. Croat. 58 (3), 255–266 (2024).
Suresh, S., Kalhoro, F. A., Rani, P. & Memon, M. Root canal morphology of premolars in population of Hyderabad, Pakistan: A cone beam computerised tomographic analysis. J. Coll. Physicians Surg. Pak. 34 (10), 1238–1244 (2024).
Vedula, P. et al. Root canal widths of mandibular molars in predicting the legal age threshold 18 years in a sample of juveniles and sub-adults of south-Indian origin: an orthopantomographic study. Int. J. Legal Med. 138 (6), 2499–2506 (2024).
Howait, M. et al. Characterizing the root canal configuration of mandibular incisors in a Western Saudi Arabian sub-population using cone beam computed tomography. Cureus 16 (5), e60650 (2024).
Fumes, A. C. et al. Root canal morphology of primary molars: A micro-computed tomography study. Eur. Arch. Paediatr. Dent. 15 (5), 317–326 (2014).
Marceliano-Alves, M. F. et al. The internal root canal morphology of single-rooted mandibular canines revealed by micro-computed tomography. J. Conserv. Dent. 21 (6), 588–591 (2018).
Razumova, S. et al. Evaluation of cross-sectional root canal shape and presentation of new classification of its changes using cone-beam computed tomography scanning. Appl. Sci. 10, 4495 (2020).
Hu, R. C., Xie, W., Hu, Y. Q. & Piao, Z. G. Root canal anatomy of maxillary second premolars at variousages observed by cone-beam CT. Zhonghua Kou Qiang Yi Xue Za Zhi. 54, 733–738 (2019).
Hu, R. C., Cao, L. L., Xie, W. & Hu, Y. Q. Aging changes of the root canal morphology in maxillary first premolars observed by cone-beam computerized tomography. Zhonghua Kou Qiang Yi Xue Za Zhi 51, 224–229 (2016).
Restrepo-Restrepo, F. et al. Prognosis of root canal treatment in teeth with preoperative apical periodontitis: A study with cone-beam computed tomography and digital periapical radiography. Int. Endod. J. 52 (11), 1533–1546 (2019).
Al-Fouzan, K. S., Ounis, H. F., Merdad, K. & Al-Hezaimi, K. Incidence of canal systems in the mesio‐buccal roots of maxillary first and second molars in Saudi Arabian population. Aust. Endod. J. 39 (3), 98–101 (2013).
Batyukov, N. M. et al. Optimization of endodontic treatment based on the use of a set of technologies taking into account the complexity of the anatomical structure of the canals. Inst. Dentistry 2, 36–37 (2015).
Kacharaju, K. R., Hari, P., Yee, A., Ngo, J. & Ismail, M. F. Analysis of mandibular premolars root canal morphology using radiographic and cross-sectional techniques in Malaysian population. Dent. Hypotheses 10, 9–14 (2019).
Bueno, M. R., Estrela, C., Azevedo, B. C. & Junqueira, C. Root canal shape of human permanent teeth determined by new cone-beam computed tomographic software. J. Endod. 46 (11), 1662–1674 (2020).
Razumova, S. et al. An in vitro evaluation study of the geometric changes of root canal preparation and the quality of endodontic treatment. Int. J. Dent. 12, 8883704 (2020).
Yanık, D. & Özel, Ş. Shaping ability of three instrumentation system in moderately curved canals: A micro-CT study. Microsc. Res. Tech. 87 (10), 2399–2407 (2024).
Almansour, M. I., Al-Zubaidi, S. M., Enizy, A. S. & Madfa, A. A. Comprehensive evaluation of root and root canal morphology of mandibular second molars in a Saudi subpopulation evaluated by cone-beam computed tomography. BMC Oral Health 22, 267 (2022).
Furri, M. Differences in the confluence of mesial canals in mandibular molar teeth with three or four root canals. Int. Endod J. 41, 777–780 (2008).
Santos-Junior, A. O., De Castro Pinto, L., Mateo-Castillo, J. F. & Pinheiro, C. R. Success or failure of endodontic treatments: A retrospective study. J. Conserv. Dent. 22 (2), 129–132 (2019).
De-Deus, G. et al. Micro-CT evaluation of non-instrumented canal areas with different enlargements performed by NiTi systems. Braz. Dent. J. 26 (6), 624–629 (2015).
Espir, C. G. et al. Shaping ability of rotary or reciprocating systems for oval root canal preparation: A micro-computed tomography study. Clin. Oral Investig. 22 (9), 3189–3194 (2018).
Xavier, S. R. et al. Shaping ability of two root canal instrumentation systems in oval-shaped canals: A microcomputed tomography study. Aust. Endod. J. 47 (2), 252–259 (2021).
Siqueira Junior, J. F., Rôças, I. D. N., Marceliano-Alves, M. F., Pérez, A. R. & Ricucci, D. Unprepared root canal surface areas: causes, clinical implications, and therapeutic strategies. Braz. Oral Res. 32 (suppl 1), e65 (2018).
Lopes, R. M. V. et al. Untouched canal areas and debris ac-cumulation after root canal preparation with rotary and adaptive systems. Aust. Endod. J. 44 (3), 260–266 (2018).
Zuolo, M. L. et al. Micro-CT assessment of the shaping ability of four root canal instrumentation systems in oval-shaped canals. Int. Endod. J. 51 (5), 564–571 (2018).
Acknowledgements
The authors declare no acknowledgments. This paper has been supported by the RUDN University Strategic Academic Leadership Program.
Author information
Authors and Affiliations
Contributions
Conceptualization, S.R. and A.B.; methodology, H.B. and N.R.; software, A.M. and Z.G; validation, S.R. and A.M.; formal analysis, Z.G. and E.A.; investigation, H.B. and E.A.; resources, A.B. and H.B.; data curation, S.R and N.R.; writing—original draft preparation, H.B. and Z.G.; writing—review and editing, S.R. and A.B.; visualization, A.M.; supervision, S.R.; project administration, S.R and A.B.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
The study was performed according to the Helsinki Declaration of 1975, as revised in 2013, and was approved by the ethical committee of the Peoples’ Friendship University of Russia University (Protocol 6 at 21.02.2019). Informed consent was obtained from all subjects.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Razumova, S., Brago, A., Barakat, H. et al. Evaluation the root canal shape among residents of Moscow region using cone beam computed tomography scanning. Sci Rep 15, 11643 (2025). https://doi.org/10.1038/s41598-025-94877-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-94877-3
