
Abstract
An objective method to evaluate patient suitability for cognitive behavioral therapy (CBT) for chronic low back pain (LBP) is currently lacking. Inappropriate application can result in prolonged hospital visits and increased medical costs. Therefore, identifying an objective biomarker for evaluating suitability is crucial. This study focused on electroencephalogram (EEG) complexity as a potential biomarker for evaluating CBT suitability for chronic LBP, assessing its discriminative ability and identifying factors that impede treatment. Complexity was analyzed as multiscale fuzzy sample entropy (MFSE). Fifty patients with suspected psychosocial factors causing LBP along with 20 healthy volunteers were included. The analysis included 25 responders and 25 non-responders for CBT. MFSE showed significant effects of scale factor [F(19,171) = 14.82, p < 0.01, partial η2 = 0.622] and interaction between group and scale factor [F(38,171) = 7.34, p < 0.01, partial η2 = 0.620]. The low-frequency band MFSE score had an odds ratio of 10.768 (95% confidence interval: 8.263–10.044, p < 0.001). The low-frequency band showed a high discriminative ability (area under the curve: 0.825), with a cut-off value of 1.25. The low-frequency FMSE is a superior biomarker for predicting suitability for CBT. This method can quickly evaluate suitability, reducing the burden on medical professionals and patients, and lowering medical costs.
Similar content being viewed by others


Introduction
The lifetime prevalence of low back pain (LBP) in Japan is 83%1. Although more than 75% of cases have a clear cause, approximately 22% are classified as non-specific LBP with unknown causes2, suggesting the involvement of psychosocial factors3,4,5,6. According to the International Association for the Study of Pain, pain is an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage7. Functional magnetic resonance imaging (fMRI) studies have shown that patients with acute LBP exhibit activation in brain regions related to pain discrimination, whereas those with chronic LBP show activation in areas associated with emotion/cognition, such as the amygdala and the orbitofrontal and medial prefrontal cortices8,9. Besides drug and exercise therapies, cognitive behavioral therapy (CBT), which addresses psychosocial factors, has been incorporated into the treatment guidelines for chronic LBP in Japan10. However, its efficacy has been reported to be limited11,12,13,14, suggesting that factors such as personality and intelligence level may affect treatment outcomes15. Furthermore, the absence of standardized guidelines for CBT suitability often results in reliance on clinical judgment, leading to potential oversight of patient groups that may not benefit from CBT, prolonged hospital visits, and increased medical costs. To address these issues, our previous research identified treatment-impeding factors for CBT in chronic LBP, including borderline verbal intelligence quotient (IQ), developmental disorders, dependence on medical care, and long-term psychosocial stress15. However, evaluating these factors across multiple domains requires substantial time and effort.
Therefore, we focused on electroencephalogram (EEG) complexity as a potential biomarker for quickly assessing CBT suitability. EEG complexity is thought to reflect functional brain connectivity. Chronic back pain is often caused by psychosocial stress, patients with depression and anxiety disorders, which activate the behavioral inhibition system, show a marked decrease in functional connectivity in the frontal lobe16. Functional connectivity refers to the synchronicity of information networks between multiple brain regions, with strong functional connectivity supporting advanced cognitive functions and flexible responses to environmental changes17. Patients with depression or anxiety disorders often have difficulty responding flexibly to psychological stress events. When the behavioral inhibition system is activated, behavior becomes passive towards uncertain outcomes or unexpected new situations, leading to a tendency to avoid everything, which is consistent with the fear and avoidance model observed in chronic LBP18. In other words, it is hypothesized that patients with chronic low back pain caused by psychosocial stress also have low functional connectivity of the frontal lobe, similar to patients with depression and anxiety disorders. Additionally, Autism spectrum disorder have been identified as a background factor in chronic LBP19, which may be related to obsession with details, lower intelligence levels, and reduced imagination. We conducted this study because we thought that the differences in the effectiveness of cognitive behavioral therapy among patients were influenced by the abundance of the variables mentioned above, such as brain wave complexity, intelligence, attention to detail, and imagination.
In other words, chronic LBP may be associated with issues related to intelligence, obsession, and flexibility, which could affect functional connectivity in the frontal lobe and be reflected as a decrease in EEG complexity. Since neural activity in each frequency band reflects different brain functions20,21,22, EEG is considered to be extremely advantageous for broadly evaluating the functional connectivity of neural networks23,24. In recent years, multiscale sample entropy (MSE) analysis has become a popular approach for EEG complexity analysis25. In this study, we used multiscale fuzzy sample entropy (MFSE) analysis, which further eliminates arbitrariness26,27,28,29. This study aimed to examine the usefulness of EEG complexity evaluation in screening for CBT suitability in patients with chronic LBP.
Methods
Study design and participants
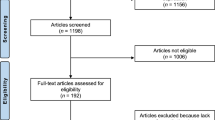
This is a case–control study that focused on EEG complexity, IQ, and developmental disorder tendencies as neuropsychological markers to predict suitability for CBT in patients with chronic low back pain. Table 1 presents the demographic characteristics of the participants. A detailed study protocol can be found in Fig. 1. This study included 50 patients with chronic LBP who were referred to the Departments of Orthopedics, Anesthesiology, and Pain Center at Chiba University Hospital between April 2022 and March 2024. Inclusion criteria were: Chronic low back pain lasting for more than 3 months, Patients with psychosocial factors as the cause of low back pain, No clear organic cause of pain suggested by MRI examination, Ineffectiveness of medication or injections, No history of surgery related to low back pain. Exclusion criteria were:

Flow diagram for the study. The study flow, inclusion criteria, exclusion criteria, and evaluation items of the research collaborators are shown.
Significant cognitive impairment or dementia, Severe mental disorders. They were evaluated by four spine surgeons who confirmed the absence of major organic factors contributing to their LBP symptoms based on MRI images and neurological symptoms. Additionally, these patients had not benefited from standard orthopedic treatments, including drug therapy (such as non-steroidal anti-inflammatory drugs [NSAIDs], opioids, α2δ ligands, gabapentinoids, and antidepressants) and various block injections. Moreover, 20 healthy volunteers were included in the study, with no dropouts reported. Patients with chronic LBP who underwent CBT were divided into responder and non-responder groups based on a threshold of 20 mm on the visual analog scale (VAS), which is considered the minimum score showing significant improvement according to previous studies30. This resulted in 25 participants in each group. No significant differences were observed in age or sex between groups. Healthy volunteers only provided EEG data for MFSE comparison. Registered cases were confirmed by senior physicians in a conference to ensure that MRI findings did not match the patient's symptoms and that no organic abnormalities were present. Whether or not low back pain is psychosocial was evaluated using the Brief Scale for Psychiatric Problems in Orthopaedic Patients (BS-POP)31. Standard orthopedic treatment was continued during the intervention trial; however, no medication changes were made. Then, a one-way ANOVA was performed on the IQ (WAIS-IV) and developmental disorder tendency (AQ) of the participants divided into two groups, and the mean differences of each sub-test, not just the total score, were compared. Next, a repeated measures ANOVA was performed on the EEG complexity (MFSE) between the three groups, the responder group, the non-responder group, and the control group, to examine the mean differences between electrode placement, groups, and scale factors. In addition, a binary logistic regression analysis was performed to calculate odds ratios to examine which factor, IQ, developmental disorder tendency, or MFSE, contributed most to the effect of CBT. A multiple regression analysis was then performed to confirm the extent to which the MFSE, the main measurement variable, could explain other factors. Finally, the cutoff value of MFSE for the adaptation of CBT was analyzed using ROC analysis.
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki for medical research involving human participants. The research protocol was approved by the Ethics Committee of Chiba University, and all trials were conducted in accordance with these guidelines and regulations. All patients were given a detailed explanation of the study and provided written informed consent before the start of the study. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines.
EEG device, recordings, and analysis
This study used the wearable device Muse2 (InteraXon Inc., Toronto, Canada; https://choosemuse.com/muse-2/) to facilitate simple and clinical-grade EEG measurements. Figure 2 shows the specifications and electrode placement of Muse 2. Participants were seated in a soundproof room with controlled indoor lighting, and measurements were taken with their eyes closed. Muse2 is a headband-type wearable EEG device that fits on the forehead, with the band ends hooked over both ears, and has been used in past studies by our research team32. Although EEG can be easily measured without special pretreatment of the scalp or forehead, EEG paste was applied in this study for accurate measurement. Muse2 has four active electrodes and one reference electrode, based on the international 10–10 system, with electrodes placed at four locations: TP9, AF7, AF8, and TP10. Two silver chloride active electrodes were placed on both sides of the forehead, two conductive silicone rubber electrodes were placed on the back of both earlobes, and the reference electrode was placed between the two active electrodes on the forehead. The sampling rate was set at 256 Hz, and the recorded data were immediately transferred to a tablet device (iPad, Apple Inc., California, USA) via Bluetooth. EEG recordings were performed using the default function of NeuroSwitch ver. 2.9.0 (Mediaseek Inc., Tokyo, Japan, https://www.mediaseek.co.jp/alpha-switch/, available on the App Store). Signal processing and analysis were performed using MATLAB Ver.9.10.0 (The Mathworks, Natick, USA). As shown in previous studies, the EEG signals were appropriately preprocessed, including band-pass filtering33,34. The recorded EEG data were down-sampled to 200 Hz, 50 Hz AC noise was removed, and re-referencing was performed to remove measurement errors due to the reference electrode position.

Specs for the Muse2. The specifications of the Muse2 electroencephalograph used in the study, such as the electrode placement and sample rate.
Multiscale fuzzy sample entropy
MFSE was calculated by reconstructing the original data through non-overlapping moving averages and calculating the sample entropy of the reconstructed data for multiple addition numbers (scale factor τ), where the scale factor corresponds to the target EEG frequency (frequency = 200 [Hz]/τ), with low scale factors reflecting the complexity of high-frequency bands and high scale factors reflecting the complexity of low-frequency bands. Let the original EEG time series be \(Y = \left\{ {y_{1} ,y_{2} , \ldots ,y_{M} } \right\}\). Then, the coarse-grained EEG time series \(X = \left\{ {x_{1} , x_{2} , \ldots ,x_{N} } \right\}\) coarsened by the time scale factor τ was defined as follows:
Next, the template vector \(X_{i}^{m}\) of dimension m was defined as follows:
Then, the infinity norm distance \(d_{ij}^{m}\) between template vectors was defined as follows:
The function \(\phi^{m}\) was defined as follows:
Using this \(\phi^{m}\), MFSE was calculated as follows:
The two parameters c and r are constants that can be arbitrarily determined. Following previous studies, c was set to 0.01, and r was set to 0.15 as the assumed standard deviation (SD). Signal processing and analysis were performed using MATLAB Ver.9.10.0 (The Mathworks, Natick, USA).
Examination items
For the 50 patients, the pain VAS was conducted at the initial consultation and after eight CBT sessions to evaluate changes in pain. At the initial consultation, the Japanese version of the autism-spectrum quotient (AQ)35,36, the Wechsler Adult Intelligence Scale-IV (WAIS-IV) intelligence test37,38,39,40, and MFSE were evaluated. For the 20 control participants, only MFSE was measured. The WAIS calculated four index scores: verbal comprehension index (VCI), perceptual reasoning index (PRI), working memory index (WMI), and processing speed index (PSI), along with the full-scale IQ (FSIQ). IQ scores were normally distributed around 100, with an SD of 15. The AQ was a questionnaire assessing developmental disorder tendencies, covering social skills, attention switching, local detail, communication, and imagination. Each item was scored from 1 to 10 points, with higher scores indicating a higher tendency and lower scores indicating a lower tendency.
Statistical analysis
In our study, comparison was made in a total of 50 cases, 25 in the responder group and 25 in the non-responder group. No statistical sample size calculations were conducted. However, using GPower (3.1) to perform the power analysis, we obtained a high-test power of 0.86, 0,79, 0.77 for IQ, AQ Score, MFSE when comparing the results between each group (2-sided, a = 0.05, ANOVA). It was judged that the test power remained high in this study. One-way analysis of variance (ANOVA) was used to compare mean differences in AQ and WAIS-IV scores between the responder and non-responder groups classified according to the improvement rate on the VAS. Tukey's method was adopted for post-hoc tests. For MFSE, repeated measures ANOVA was performed for each of the 20 scale factors across the four electrodes (AF7, AF8, TP9, and TP10) to evaluate differences between groups. The Greenhouse–Geisser test was adopted for degrees of freedom, and the significance level was set at 0.05. To identify the factors that most influenced the effectiveness of CBT, odds ratios (ORs) were calculated using logistic regression analysis. A multiple regression analysis was performed to examine the influence of multiple factors affecting treatment efficacy on FMSE scores. Receiver operating characteristic (ROC) analysis was performed to evaluate the discriminative ability of MFSE for CBT suitability, with the discriminative accuracy measured by the area under the ROC curve (AUC).
CBT
CBT was conducted by three clinical psychologists with over 10 years of experience. The CBT techniques incorporated psychoeducation, cognitive restructuring, relaxation (abdominal breathing and progressive muscle relaxation), stress management, pacing, and behavioral activation, commonly used in chronic LBP treatment41,42. Due to appointment slot limitations, the sessions were conducted once a week for 50 min, totaling eight sessions.
Results
Assessing cognitive abilities using the WAIS-IV and AQ
Figure 3 shows the results of the WAIS-IV and AQ. One-way ANOVA revealed no significant differences between the groups in FSIQ, PRI, WMI, and PSI, with both groups showing average intellectual levels. However, the VCI of the non-responder group was 89.36 (7.04), slightly below the normative average for their age group and significantly lower compared to the responder group (F(1,48) = 51.65, p < 0.01). VCI represents the ability to understand words, the amount of knowledge, and the ability to express one's thoughts using words or infer what others want to say.

Assessment of cognitive abilities using the WAIS-IV and AQ. Results of two-way ANOVAs of WAIS and AQ results by group are shown. The significance level was set at 0.05. AQ, autism-spectrum quotient; WAIS-IV, Wechsler Adult Intelligence Scale-IV.
One-way ANOVA for the AQ showed no significant differences in social skills, or communication, although significant differences were found in attention switching (F(1,48) = 14.87, p < 0.01), local details (F(1,48) = 17.87, p < 0.01) and imagination (F(1,48) = 13.29, p < 0.01), indicating that the non-responder group had difficulty switching attention, stronger obsession to details and lower imagination.
Comparison of multiscale fuzzy sample entropy
Figure 4 shows a plot of the average MFSE values for the non-responder, responder, and control groups. Repeated measures ANOVA revealed a main effect of scale factor (F (19,171) = 14.82, p < 0.01, partial η2 = 0.622) and an interaction between group and scale factor (F (38,171) = 7.34, p < 0.01, partial η2 = 0.620). Post-hoc Tukey’s multiple comparison tests showed that the non-responder group had significantly lower values across all scale factors compared to the control and responder groups (p < 0.01), whereas the responder group had significantly lower values in the high-frequency band (scale factors 1–5) compared to the control group (p < 0.01). Regarding electrodes, only the responder group showed significantly lower values in the high-frequency band for the frontal electrodes AF7 and AF8 (F (19,52) = 0.57, p < 0.01, partial η2 = 0.176).

Comparison of MFSE between groups. Results of MFSE with repeated measures ANOVA for each group are shown. The significance level was set at 0.05. The scale factor corresponds to the target EEG frequency (frequency: 200 [Hz]/τ), with low scale factors reflecting the complexity of high-frequency bands and high scale factors reflecting that of low-frequency bands. ANOVA, one-way analysis of variance; EEG, electroencephalogram; MFSE, multiscale fuzzy sample entropy.
Multivariate analysis of factors influencing the effectiveness of CBT
A binary logistic regression analysis was performed with the presence or absence of the CBT effect as the dependent variable and each IQ index, AQ Subtest, MFSE as covariates. MFSE was divided into high-MFSE (scale factor 1–5) and low-MFSE (scale factor 15–20). Table 2 shows the binary logistic regression analysis of the CBT effect and each variable. Multicollinearity was checked and VIF was confirmed to be no greater than 5. The results are summarized in Fig. 5 as a forest plot. Patients aged 60 years or older had an OR of 1.95 (95% CI 1.68–2.22. p < 0.05), VCI (≦ 89) had an OR of 6.92 (95% CI 5.83–2.99. p < 0.01), VCI (≧ 120) had an OR of 0.65 (95% CI 0.43–0.97. p < 0.01), attention switching had an OR of 3.26 (95% CI 1.93–5.50. p < 0.01), local details had an OR of 2.24 (95% CI 1.49–3.36. p < 0.01), imagination had an OR of 6.76 (95% CI 4.39–8.00. p < 0.01), high-MFSE had an OR of 8.75 (95% CI 6.60–11.61. p < 0.01), and low-MFSE had an OR of 10.76 (95% CI 8.26–14.03. p < 0.01). Being over 60 years old, having a verbal IQ below 89, having difficulty switching attention, being particular about details, and having a lack of imagination are factors that decrease the effectiveness of CBT treatment.

Forest Plot of factors decreasing the effectiveness of CBT treatment. Factors influencing the effectiveness of CBT are illustrated based on the results of the logistic regression analysis. The odds ratios and P values of items with significant effects are shown in red. CBT, cognitive behavioral therapy.
Stepwise multiple linear regression analysis for MFSE
A multiple regression analysis was conducted to evaluate the relationship between the MFSE and other factors. WAIS-IV (FSIQ, VCI, PRI, WMI, PSI) and AQ (social skills, attention switching, local details, communication, imagination) were included in the multivariate analysis. The values for each factor are listed in Table 3. The results indicated that the model could explain 79.2% of the MFSE (R = 0.832, adjusted R2 = 0.792, p < 0.01). VCI (β = − 0.006, p < 0.05), local details (β = − 0.026, p < 0.05), imagination (β = − 0.041, p < 0.01), and attention switching (β = − 0.041, p < 0.001) were the factors influencing MFSE. The lower the verbal IQ, the stronger the attention to detail, the worse the switching of thoughts, and the poorer the imagination, the lower the MFSE score. These results were similar to those corresponding to the logistic regression analysis on factors that influence the effectiveness of CBT. In other words, it is inferred that by evaluating the MFSE, it is possible to evaluate the suitability of CBT for chronic low back pain.
ROC curve
The ROC analysis results for discriminative ability regarding CBT suitability for low-MFSE and high-MFSE are shown in Fig. 6. Low-MFSE showed high accuracy, with an AUC of 0.825 at a cut-off of 1.25, whereas high-MFSE showed moderate accuracy, with an AUC of 0.716 at a cut-off of 1.08, indicating that low-MFSE had a higher discriminative ability for determining CBT suitability.

MFSE ROC curve and cutoff value. Cut-off values for MFSE scores predicting suitability for CBT are shown. AUC is an index of discriminatory ability, and a value higher than 0.8 is considered highly accurate. AUC, area under the curve; CBT, cognitive behavioral therapy; MFSE, multiscale fuzzy sample entropy; ROC, receiver operating characteristic.
Discussion
In this study, patients with chronic LBP were divided into responder and non-responder groups based on their response to CBT, and the discriminative ability of MFSE as a biomarker for CBT suitability was evaluated. As a result, the low-frequency band MFSE has a higher discriminatory ability for CBT suitability than other variables and is useful. Previous research has suggested that variables such as developmental disorder tendencies and intelligence also have an influence, but the low-frequency band MFSE has a strong correlation with these and a high explanatory rate.
The influence of intelligence level and developmental disorders on CBT suitability
The WAIS-IV results revealed that the non-responder group had a lower VCI, which was borderline compared to the age-matched average and significantly different from the responder group. This suggests that CBT, which relies on verbal expression, may be less effective for individuals with lower verbalization abilities. Regarding the AQ, although previous reports indicated low autistic tendencies in patients with chronic LBP32, this study found significant differences in subtests. Specifically, the non-responder group scored higher on attention switching, local details and imagination, reflecting a strong focus on details and limited imaginative capacity despite similar total AQ scores.
Relationship between MFSE and CBT suitability
In the MFSE comparison, the healthy group showed consistent average values across scale factors. In the high-frequency band (scale factor 1–5), the pattern was non-responder group = responder group < control group, indicating lower values for patients with chronic LBP. Conversely, in the low-frequency band (scale factor 15–20), the pattern was non-responder group < responder group = control group, suggesting that CBT suitability is strongly influenced by MFSE in the low-frequency band. The low-frequency band reflects widespread brain network activity and tends to be higher in groups with high cognitive functions43,44. In this study, the VCI was low in the non-responder group, suggesting that a certain level of intelligence is necessary for compatibility with CBT. Thus, MFSE evaluation in the low-frequency band is useful for evaluating compatibility with CBT. Conversely, the low-MFSE in the high-frequency band in the chronic LBP group suggests a possible decrease in the function of gamma-aminobutyric acid (GABA)-ergic inhibitory interneurons in the gamma band. GABA has a stress-relieving effect on inhibitory neurons in humans45, and its decreased function causes psychosocial pain46,47. This decrease involves a reduction in potassium chloride co-transporter 2 (KCC2) expression due to microglial activation, and increasing KCC2 function may help treat psychosocial chronic pain by enhancing the inhibitory effect of GABA48. GABA transmission dysfunction manifests as γ-band neural oscillation abnormalities, with chronic stress impairing the normal maturation of γ-band neural networks49,50. The low complexity in the γ band observed in this study likely indicates a decrease in GABAergic function against stress.
The degree of influence of factors that affect suitability for CBT
The results of the logistic regression analysis with the effectiveness of CBT as the dependent variable and the multiple regression analysis with the MFSE score as the dependent variable were similar, with verbal IQ, attention switching, local details, and imagination having an influence. The lower the verbal IQ and imagination, and the stronger the obsessions and difficulty in switching thoughts, the lower the effect of CBT and the lower the MFSE. We found that the MFSE can explain 79.2% of the factors that affect the effectiveness of CBT, and it is inferred that evaluating the MFSE is the simplest, quickest, and most appropriate method to evaluate the suitability of CBT for chronic pain.
The discriminatory ability of MFSE for CBT suitability
There was a significant difference in MFSE scores between the low-frequency and high-frequency bands, and it was found that the MFSE in the low-frequency band had a greater influence on the effectiveness of CBT. Therefore, in the ROC analysis, MFSE was analyzed using the average values of the low-frequency and high-frequency bands, respectively. ROC analysis showed high discriminative ability, with a cut-off value of 1.25 for low-MFSE, suggesting that CBT may not be suitable for those with scores below this value.
Limitations and clinical implications
This study had a few limitations. Firstly, the accuracy of the EEG device was a concern. The Muse2 used in this study complied with the international 10–20 system but comprised only four electrodes, and data from specified electrodes could not be obtained. Secondly, although re-referencing was performed to eliminate the influence of the reference electrode position on the frontal electrodes, some of this influence remained.
In this study, we focused on EEG complexity (MFSE) as an objective evaluation of CBT suitability for patients with chronic LBP and assessed its discriminative ability. Low-MFSE in the low-frequency band had the strongest influence on the presence or absence of CBT effects and could be used to evaluate CBT suitability with high sensitivity. This study showed that it is possible to predict the suitability of CBT for patients with chronic low back pain using EEG complexity as a neurological marker, which will reduce medical expenses and personnel costs. The evidence for CBT for patients with chronic low back pain in Japan is still low, and the reason for this is that many patients are being treated who are not suitable for CBT because there were no patient suitability criteria. By clarifying the suitability criteria through this study, it is expected that CBT for patients with chronic low back pain will be closer to being covered by insurance because the reproducibility of the treatment effect will increase. Similar research using complexity has already been conducted on dementia, and it has been shown that using a decrease in complexity as an indicator is effective in predicting Alzheimer's disease and mild cognitive impairment51,52. From these reports, EEG complexity is related to cognitive function, and the same results were obtained in this study, which can be said to be one factor in predicting the effectiveness of CBT. However, this study showed that EEG complexity is not only influenced by cognitive function, but also by factors such as imagination and obsession, and we believe that it is a great finding that these can be substituted by evaluating the EEG complexity of the frontal. As a future perspective of this research, it may be possible to use MFSE to evaluate the suitability of cognitive behavioral therapy for any chronic illness, not just chronic low back pain, and we would like to investigate its discriminatory ability in collaboration with researchers from various fields.
Data availability
Because of the highly personal and sensitive nature of the data, it will not be made publicly available. However, the data can be made available upon reasonable request. Please send a request to the corresponding author via email.
References
Fujii, T. & Matsudaira, K. Prevalence of low back pain and factors associated with chronic disabling back pain in Japan. Eur. Spine J. 22(2), 432–438 (2013).
Suzuki, H. et al. Diagnosis and characters of non-specific low back pain in Japan: The Yamaguchi low back pain study. PLoS ONE 11(8), e0160454. https://doi.org/10.1371/journal.pone.0160454 (2016).
Waddell, G. & Burton, A. K. Occupational health guidelines for the management of low back pain at work: Evidence review. Occup. Med. (Lond.) 51(2), 124–135. https://doi.org/10.1093/occmed/51.2.124 (2001).
Kent, P. M. & Keating, J. L. Can we predict poor recovery from recent-onset nonspecific low back pain? A systematic review. Man. Ther. 13(1), 12–28. https://doi.org/10.1016/j.math.2007.05.009 (2008).
Wertli, M. M. et al. Influence of catastrophizing on treatment outcome in patients with nonspecific low back pain: A systematic review. Spine 39(3), 263–273. https://doi.org/10.1097/BRS.0000000000000110 (2014).
Wertli, M. M. et al. Catastrophizing-a prognostic factor for outcome in patients with low back pain: A systematic review. Spine J. 14(11), 2639–2657. https://doi.org/10.1016/j.spinee.2014.03.003 (2014).
Raja, S. N. et al. The revised international association for the study of pain definition of pain: Concepts, challenges, and compromises. Pain 161(9), 1976–1982. https://doi.org/10.1097/j.pain.0000000000001939 (2020).
Hashmi, J. A. et al. Shape shifting pain: Chronification of back pain shifts brain representation from nociceptive to emotional circuits. Brain 136(9), 2751–2768. https://doi.org/10.1093/brain/awt211 (2013).
Vachon-Presseau, E. et al. Corticolimbic anatomical characteristics predetermine risk for chronic pain. Brain 139(7), 1958–1970. https://doi.org/10.1093/brain/aww100 (2016).
Kawakami, M. et al. Japanese orthopaedic association (JOA) clinical practice guidelines on the management of lumbar spinal stenosis, 2021: Secondary publication. J. Orthop. Sci. 28(1), 46–91 (2021).
Williams, A. C. C., Fisher, E., Hearn, L. & Eccleston, C. Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst. RevCochrane Database Syst. Rev. 8(8), CD007407 (2020).
Pincus, T. et al. OBI Trial Management Team. Delivering an optimised behavioural Intervention (OBI) to people with low back pain with high psychological risk: Results and lessons learnt from a feasibility randomised controlled trial of contextual cognitive behavioural therapy (CCBT) versus physiotherapy. BMC Musculoskelet Disord. 16(16), 147. https://doi.org/10.1186/s12891-015-0594-2 (2015).
Albaladejo, C. et al. The efficacy of a short education program and a short physiotherapy program for treating low back pain in primary care: A cluster randomized trial. Spine 35(5), 483–496. https://doi.org/10.1097/BRS.0b013e3181b9c9a7 (2010).
Cherkin, D. C. et al. Effect of mindfulness-based stress reduction vs cognitive behavioral therapy or usual care on back pain and functional limitations in adults with chronic low back pain: A randomized clinical trial. JAMA 315(12), 1240–1249. https://doi.org/10.1001/jama.2016.2323 (2016).
Shimizu, K. et al. Background factors for chronic low back pain resistant to cognitive behavioral therapy. Sci. Rep. 11(1), 8227. https://doi.org/10.1038/s41598-021-87239-2 (2021).
Kojima, K. et al. Brain 5-HT2A receptor binding and its neural network related to behavioral inhibition system. Brain Imaging Behav. 16(3), 1337–1348. https://doi.org/10.1007/s11682-021-00609-2 (2022).
Onoda, K., Ishihara, M. & Yamaguchi, S. Decreased functional connectivity by aging is associated with cognitive decline. J. Cogn. Neurosci. 24(11), 2186–2198. https://doi.org/10.1162/jocn_a_00269 (2012).
Leeuw, M. et al. The fear-avoidance model of musculoskeletal pain: Current state of scientific evidence. J. Behav. Med. 30(1), 77–94. https://doi.org/10.1007/s10865-006-9085-0 (2007).
Ortiz Rubio, A. et al. Pain experiences of people diagnosed with autism spectrum disorder: A systematic review of case-control studies. Am. J. Occup. Ther. 77(2), 7702185020. https://doi.org/10.5014/ajot.2023.050050 (2023).
Allen, E. A. et al. Tracking whole-brain connectivity dynamics in the resting state. Cereb. Cortex 24(3), 663–676. https://doi.org/10.1093/cercor/bhs352 (2014).
Betzel, R. F., Fukushima, M., He, Y., Zuo, X. N. & Sporns, O. Dynamic fluctuations coincide with periods of high and low modularity in resting-state functional brain networks. Neuroimage 127, 287–297. https://doi.org/10.1016/j.neuroimage.2015.12.001 (2016).
Başar, E., Başar-Eroglu, C., Karakaş, S. & Schürmann, M. Gamma, alpha, delta, and theta oscillations govern cognitive processes. Int. J. Psychophysiol. 39(2–3), 241–248. https://doi.org/10.1016/s0167-8760(00)00145-8 (2001).
Von Stein, A. & Sarnthein, J. Different frequencies for different scales of cortical integration: From local gamma to long range alpha/theta synchronization. Int. J. Psychophysiol. 38(3), 301–313. https://doi.org/10.1016/s0167-8760(00)00172-0 (2000).
Varela, F., Lachaux, J. P., Rodriguez, E. & Martinerie, J. The BrainWeb: Phase synchronization and large-scale integration. Nat. Rev. Neurosci. 2(4), 229–239. https://doi.org/10.1038/35067550 (2001).
Yang, A. C. & Tsai, S. J. Is mental illness complex? From behavior to brain. Prog. Neuropsychopharmacol. Biol. Psychiatry 1(45), 253–257. https://doi.org/10.1016/j.pnpbp.2012.09.015 (2013).
Castiglioni, P., Merati, G., Parati, G. & Faini, A. Sample, fuzzy and distribution entropies of heart rate variability: What do they tell us on cardiovascular complexity?. Entropy (Basel) 25(2), 281. https://doi.org/10.3390/e25020281 (2023).
Xiong, G., Zhang, L., Liu, H., Zou, H. & Guo, W. A comparative study on ApEn, SampEn and their fuzzy counterparts in a multiscale framework for feature extraction. J. Zhejiang Univ. Sci. A 11(4), 270–279. https://doi.org/10.1631/jzus.A0900360 (2010).
Nikulin, V. V. & Brismar, T. Comment on “multiscale entropy analysis of complex physiologic time series”. Phys. Rev. Lett. 92(8), 089803. https://doi.org/10.1103/PhysRevLett.92.089803 (2004).
Costa, M., Goldberger, A. L. & Peng, C. K. Multiscale entropy analysis of complex physiologic time series. Phys. Rev. Lett. 89(6), 068102. https://doi.org/10.1103/PhysRevLett.89.068102 (2002).
Ostelo, R. W. J. G. & de Vet, H. C. W. Clinically important outcomes in low back pain. Best Pract. Res. Clin. Rheumatol. 19(4), 593–607. https://doi.org/10.1016/j.berh.2005.03.003 (2005).
Sato, K., Kikuchi, S., Mashiko, H., Okano, T. & Niwa, S. Liaison consultation psychiatry for spine and spinal cord disease; brief scale for evaluation of psychiatric problems in orthopaedic patients (BS-POP). Clin. Orthop. Surg. 35, 843–852 (2000).
Shimizu, K. et al. New treatment strategy for chronic low back pain with alpha wave neurofeedback. Sci. Rep. 12(1), 14532. https://doi.org/10.1038/s41598-022-18931-0 (2022).
Racz, F. S., Stylianou, O., Mukli, P. & Eke, A. Multifractal dynamic functional connectivity in the resting-state brain. Front. Physiol. 30(9), 1704. https://doi.org/10.3389/fphys.2018.01704 (2018).
Busa, M. A. & van Emmerik, R. E. A. Multiscale entropy: A tool for understanding the complexity of postural control. J. Sport Health Sci. 5(1), 44–51. https://doi.org/10.1016/j.jshs.2016.01.018 (2016).
Wakabayashi, A., Tojo, Y., Baron-Cohen, S. & Wheelwright, S. The autism-spectrum quotient (AQ) Japanese version: Evidence from high-functioning clinical group and normal adults. Shinrigaku Kenkyu Jpn. Vers. 75(1), 78–84. https://doi.org/10.4992/jjpsy.75.78 (2004).
Baron-Cohen, S., Wheelwright, S., Skinner, R., Martin, J. & Clubley, E. The autism-spectrum quotient (AQ): Evidence from Asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. J. Autism. Dev. Disord. 31 (1), 5–17 (2001). https://doi.org/10.1023/a:1005653411471. Erratum in: J Autism Dev Disord 2001 December;31(1):5–17
Wechsler, D. WAIS-IV Administration and Scoring Manual (NCS Pearson, 2008).
Wechsler, D. WAIS-IV Technical and Interpretive Manual (NCS Pearson, 2008).
Ueno, K., Ishimura, T., Dairoku, H., Yamanaka, K. & Matsuda, O. The Japaneseversion of Wechsler Adult Intelligence Scale 4th edn: Administration and Scoring Manual (Nihon Bunka kagakusya, 2018) (in Japanese).
Ueno, K., Ishimura, T., Dairoku, H., Yamanaka, K. & Matsuda, O. The Japaneseversion of Wechsler Adult Intelligence Scale 4th Edn: Theory and Interpretation Manual (Nihon bunka kagakusya, 2018).
Flor, H. & Turk, D. C. Chronic Pain: An Integrated Biobehavioral Approach Vol. 547 (IASP Press, 2011).
Otis, J. D. Managing Chronic Pain: A Cognitive-Behavioral Therapy Approach. Therapist Guide. Translator Seiwa syoten Iyo M, & Shimizu E, editors (2011).
Iinuma, Y. et al. Enhanced temporal complexity of EEG signals in older individuals with high cognitive functions. Front. Neurosci. 21(16), 878495. https://doi.org/10.3389/fnins.2022.878495 (2022).
McIntosh, A. R. et al. Spatiotemporal dependency of age-related changes in brain signal variability. Cereb. Cortex 24(7), 1806–1817. https://doi.org/10.1093/cercor/bht030 (2014).
Abdou, A. M. et al. Relaxation and immunity enhancement effects of gamma-aminobutyric acid (GABA) administration in humans. BioFactors 26(3), 201–208. https://doi.org/10.1002/biof.5520260305 (2006).
Kobayashi, S. et al. Hyper-formation of GABA and glycine co-releasing terminals in the mouse cerebellar nuclei after deprivation of GABAergic inputs from Purkinje cells. Neuroscience 1(426), 88–100. https://doi.org/10.1016/j.neuroscience.2019.11.030 (2020).
Eto, K. et al. Enhanced GABAergic activity in the mouse primary somatosensory cortex is insufficient to alleviate chronic pain behavior with reduced expression of neuronal potassium-chloride cotransporter. J Neurosci 32(47), 16552–16559. https://doi.org/10.1523/JNEUROSCI.2104-12.2012 (2012).
Kosaka, Y. et al. Development and persistence of neuropathic pain through microglial activation and KCC2 decreasing after mouse tibial nerve injury. Brain Res. 15(1733), 146718. https://doi.org/10.1016/j.brainres.2020.146718 (2020).
Kanao-Kanda, M. et al. Viral vector-mediated gene transfer of glutamic acid decarboxylase for chronic pain treatment: A literature review. Hum. Gene Ther. 31(7–8), 405–414. https://doi.org/10.1089/hum.2019.359 (2020).
Dricks, S. Effects of neonatal stress on gamma oscillations in hippocampus. Sci. Rep. 6, 29007. https://doi.org/10.1038/srep29007 (2016).
Ando, M., Nobukawa, S., Kikuchi, M. & Takahashi, T. Identification of electroencephalogram signals in Alzheimer’s disease by multifractal and multiscale entropy analysis. Front. Neurosci. 28(15), 667614. https://doi.org/10.3389/fnins.2021.667614 (2021).
Nobukawa, S. et al. Atypical instantaneous spatio-temporal patterns of neural dynamics in Alzheimer’s disease. Sci. Rep. 14, 88. https://doi.org/10.1038/s41598-023-50265-3 (2024).
Acknowledgements
This research was conducted with support from Mediaseek Inc. (https://www.mediaseek.co.jp/), which provided the Signal processing codes for EEG complexity and analysis application used in the present study during the research period. We are grateful to Editage (https://www.editage.jp) for their professional editing and proofreading services, which significantly enhanced the clarity and readability of this manuscript.
Role of the funder/sponsor
The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Funding
This work was supported by JSPS KAKENHI Grant Number JP 23K08667.
Author information
Authors and Affiliations
Contributions
KS had full access to all the data in the study and takes responsibility for its integrity and for the accuracy of the data analysis. Concept and design: KS, AI, AO, MM. Acquisition, analysis, or interpretation of data: KS, KI, HC, SuO, YS, YE, MI. Drafting of the manuscript: KS. Critical review of the manuscript for important intellectual content: All authors. Statistical analysis: KS. Funding acquisition: KS. Administrative, technical, or material support: KI. Supervision: SeO, HC, KI.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Shimizu, K., Inage, K., Chikubu, H. et al. Screening system for assessing suitability of cognitive behavioral therapy for chronic low back pain. Sci Rep 15, 11491 (2025). https://doi.org/10.1038/s41598-025-95948-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-95948-1
