
Abstract
Occupational burnout (OB) among healthcare workers (HCWs) has significant implications for workforce sustainability and patient care. The COVID-19 pandemic exacerbated existing stressors, highlighting the urgent need to investigate burnout prevalence and associated factors among HCWs in Central Asia (CA). This study aimed to assess burnout levels, explore contributing factors, and evaluate the impact of job satisfaction and pandemic-related stressors. A cross-sectional online survey was conducted between July and November 2022 among physicians and nurses in Kazakhstan, Kyrgyzstan, and Uzbekistan. The survey included the Copenhagen Burnout Inventory (CBI), a validated job satisfaction scale, and a measure assessing the impact of COVID-19 on work and personal life. Burnout prevalence and associated factors were analyzed using regression modeling and mediation analysis. Among 2685 HCWs (Kazakhstan: 67.7%, Kyrgyzstan: 19.9%, Uzbekistan: 12.4%), the overall prevalence of OB was 28.3%. Physicians had higher burnout levels than nurses, with job satisfaction playing a mediating role in this disparity in Kazakhstan and Kyrgyzstan. A poor work environment and high job demands were strongly linked to OB (p < 0.001). HCWs with severe COVID-19 histories experienced significantly greater burnout (OR 1.346–2.270, p < 0.05). Pandemic-related stressors, including social stigma, excessive workload, and lack of appreciation, were significant predictors of burnout. OB remains a critical issue among HCWs in CA, with job satisfaction, workplace conditions, and pandemic-related stressors playing key roles. Targeted interventions, such as workload optimization, institutional support, and mental health resources, are essential to mitigate OB and improve HCW well-being.
Similar content being viewed by others
Introduction
The healthcare industry puts much on healthcare providers, including workload, lack of control over work processes, inadequate financial, institutional, or social reward, and challenges in relationships with leadership or clients1. These pressures contribute to occupational burnout, a syndrome characterized by emotional exhaustion, psychological distress, and diminished well-being2. In turn, occupational burnout among healthcare workers (HCWs) is associated with concerns about patient safety and poor quality of care. It also affects the physical and mental health of healthcare providers, employee turnover, and emigration rates3. Consequently, occupational burnout has personal, collective, organizational, and economic consequences for both HCWs and the entire healthcare system. The World Health Organization (WHO) has recognized burnout as a major occupational health crisis, reporting that at least one in four HCWs experienced burnout, anxiety, or depression between 2020 and 20224. In response, WHO has emphasized improved working conditions, adequate staffing, and mental health support to sustain the global healthcare workforce.
The COVID-19 pandemic exacerbated pre-existing stressors, leading to unprecedented levels of burnout among HCWs. The crisis resulted in excessive workloads, inadequate pandemic preparedness, loss of colleagues, and infection risks to both HCWs and their families5,6,7,8. In Kazakhstan, studies have identified key challenges faced by frontline HCWs, including insufficient financial support, lack of protective equipment, and severe psychological distress. Notably, HCWs without financial support reported significantly higher levels of burnout, depression, and anxiety than those who received assistance, highlighting the importance of institutional support in mitigating pandemic-related stress9. Even after the acute phase of the pandemic, COVID-19 continues to affect healthcare systems and HCW mental health10.
Global studies have consistently reported high burnout prevalence among HCWs during the pandemic, with estimates ranging from 31 to 68%, depending on occupational role and healthcare setting11,12. In the United States alone, burnout rates among HCWs rose from 32% in 2018 to 46% in 202213. Similarly, a large-scale study found that emotional exhaustion among HCWs increased from 31.8% in 2019 to 40.4% in 2021–2022, with nurses experiencing the highest burnout levels (49.2%)14. Beyond pandemic-related stress, job dissatisfaction has been strongly linked to burnout, particularly among ICU staff15. Additionally, moral injury—the distress caused by ethical dilemmas and witnessing suffering—has been identified as a significant contributor to burnout, depression, and anxiety16. Moreover, studies highlight gender disparities, with female HCWs and nurses exhibiting higher vulnerability to burnout than their male counterparts11,17.
Unlike high-income countries with well-established social health insurance systems, Central Asia’s healthcare sector, shaped by its post-Soviet legacy, remains underfunded. The region relies heavily on hospital-based specialized care rather than community-centered primary healthcare, leading to workforce shortages, financial instability, and high workloads18,19. While reforms aim to strengthen primary care and achieve universal health coverage, significant challenges remain20, directly impacting HCW well-being and increasing burnout risks. Despite the global focus on burnout, Central Asia remains understudied, with most existing research focusing on high-income settings. At the same time, cultural, institutional, and economic differences influence burnout experiences, making direct comparisons with high-income settings challenging3.
Until recently, research on burnout in Kazakhstan was limited, with only a few studies examining burnout among cardiologists and oncologists21,22. However, recent national-level studies have expanded knowledge on burnout among primary healthcare workers in Kazakhstan, identifying factors such as age, gender, work experience, and geographic region as significant contributors23,24. Additionally, studies focusing on hospital-based nurses and physicians have shown high emotional exhaustion and depersonalization rates, with burnout prevalence varying based on workplace location and employment status25.
Despite these advances, there is still no comprehensive cross-country analysis of burnout among HCWs in Central Asia, making it difficult to compare how systemic and socio-demographic factors contribute to occupational stress across different national healthcare settings. This study aims to fill this gap by investigating the prevalence and characteristics of occupational burnout among HCWs in three Central Asian countries—Kazakhstan, Kyrgyzstan, and Uzbekistan. The study further explores key sociodemographic factors, job satisfaction levels, and the impact of the COVID-19 pandemic on burnout. Additionally, we compare burnout levels between HCWs who worked on the COVID-19 frontline and those who did not, providing insights into the long-term psychological impact of frontline exposure. By conducting a cross-country analysis, this research provides novel insights into the mental health challenges faced by HCWs in Central Asia, offering critical evidence to guide interventions aimed at mitigating burnout and improving healthcare working conditions in the region.
Methods
Study design and setting
This cross-sectional questionnaire-based study was conducted between July and November 2022 as part of an initiative project to assess the psychological well-being of healthcare workers (HCWs) in Central Asia.
Survey platform and Language
The survey was administered using the EnKlikAnketa platform (http://www.1ka.si). The study was conducted in Russian, as it is widely spoken alongside native languages in Central Asian countries, ensuring accessibility for the majority of HCWs. By blocking repeated IP addresses, the study was protected from duplicate responses.
Participant recruitment and sampling
The study employed a convenience sampling approach, targeting healthcare workers (HCWs) in Central Asia. Participants were recruited through multiple digital and institutional channels. The survey link was distributed via medical professional groups on Facebook and WhatsApp chat groups of healthcare staff from various clinics. Additionally, organizational leaders received official notifications about the survey through formal letters from the research institutions, encouraging participation among their employees. Moreover, in Kazakhstan, regional healthcare departments also distributed survey invitations via official letters, ensuring broader outreach.
To confirm participant eligibility, the survey included a section where respondents specified their country of work, type of organization, and the organization’s source of funding. Given that healthcare institutions employ various professionals beyond physicians and nurses, respondents could also indicate other roles. However, for the final analysis, only responses from physicians and nurses were retained.
The required sample size was estimated using Cochran’s formula for a 95% confidence level and a 5% margin of error, based on WHO data. To account for the total number of HCWs in each country, we applied a finite population correction. Since the total number of HCWs in each country is large, the required sample size stabilizes at approximately 384 participants per country, ensuring sufficient statistical power for the analyses.
Response rate and sample characteristics
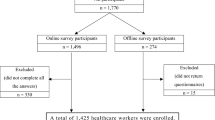
A total of 6903 HCWs accessed the survey link, of whom 4372 provided informed consent. Among them, 3083 fully completed the survey, and 2685 responses from physicians and nurses were included in the final analysis. The overall response rate (percentage of participants who fully completed the survey out of those who accessed the link) was 44.7%, while the completion rate among those who consented was 70.5%. The final response rate, considering only physicians and nurses, was 38.9%.
Measures
The questionnaire included:
-
Items on sociodemographic and occupational characteristics: sex, age, job (physicians or nurses, organization and financing type), family status, frontline work during the COVID-19 pandemic, COVID-19 infection history and vaccination status. In this study, managerial positions refer to physicians and nurses who hold leadership roles within their respective departments, such as department heads, senior physicians, or head nurses. This classification does not include administrative or executive personnel working at the organizational management level, such as hospital directors or administrative officers. This distinction ensures that the analysis focuses on HCWs actively involved in clinical decision-making and team supervision.
-
Occupational burnout was assessed using the previously validated Copenhagen Burnout Inventory (CBI)26,27. The CBI consists of 19 items that represent three dimensions: Personal Burnout (PB), Work-Related Burnout (WRB), and Client-Related Burnout (CRB). The CBI focuses exclusively on burnout symptoms, distinguishing it from other tools like the Maslach Burnout Inventory and the Oldenburg Burnout Inventory, which integrate potential causes and consequences of burnout. Its conceptual simplicity and broad applicability allow for the assessment of general exhaustion beyond workplace settings. The scale measured exhaustion and emotional strain using a 5-point Likert scale, where responses ranged from “Never/almost never” (0%) to “Always” (100%) for most items. Items 18 and 19, assessing client-related burnout, used a slightly different scale ranging from “To a very low degree” (0%) to “To a very high degree” (100%). Higher scores indicated greater burnout symptoms. Item 10 was reverse-scored to align with the burnout construct. A burnout level (severity) was assessed according to Kristensen’s criteria28. The scale demonstrated reliable to excellent internal consistency, with a Cronbach’s alpha of 0.932 for the full sample (ranging from 0.907 to 0.939 across countries)29. Its free availability makes it a practical tool for large-scale and cross-cultural research, particularly in resource-limited settings.
-
Job satisfaction was assessed using a scale originally developed by Okaro, Eze, and Ohagwu30 and later expanded by Khamlub et al.31 to capture its multifaceted nature. The scale reflects the concept of job satisfaction as a positive emotional state derived from job appraisal, while also accounting for its complexity and the lack of a universally accepted definition. Job satisfaction consisted of 18 items with a 6-point Likert-type satisfaction scale. Job satisfaction was assessed using a five-factor scale identified through Exploratory Factor Analysis (EFA): job autonomy and task variety, work environment and job demands, opportunities for growth and development, workplace support and involvement, and salary and financial rewards. The scale demonstrated excellent reliability, with Cronbach’s alpha ranging from 0.937 to 0.952 across countries. Confirmatory Factor Analysis (CFA) supported the five-factor structure with good model fit across samples (CFI = 0.930–0.959, TLI = 0.914–0.950, RMSEA = 0.062–0.077). Detailed reliability and validity results are presented in Suppl. Tables 1 and 2. Mean values were calculated for each subscale and the total scale, with higher scores indicating greater job satisfaction.
-
The impact of COVID-19 on the personal life and work of HCWs was assessed using the scale created by Pham et al. (2021)32. The scale consisted of 14 items with a 5-point Likert-type agreement scale. The scale demonstrated high reliability, with Cronbach’s alpha ranging from 0.816 to 0.896 across countries. EFA identified a three-factor structure: social stigma and psychological burden, lack of appreciation, and workload and job demands. CFA supported the three-factor structure, showing good model fit across all samples (CFI = 0.907–0.952, TLI = 0.880–0.938, RMSEA = 0.061–0.094). Detailed reliability and validity results are presented in Suppl. Tables 3 and 4. Mean values were calculated for each subscale and the total scale, with higher scores indicating a greater perceived impact of COVID-19 on personal and professional life.
Statistical analysis
The validity of the scales used was assessed using reliability, Exploratory Factor Analysis (EFA), and Confirmatory Factor Analysis (CFA). Internal consistency was assessed using Cronbach’s alpha, and values of 0.70 or above were considered good reliability29. EFA was conducted to identify the underlying factor structure using minimum residuals axis factoring with oblimin rotation, considering eigenvalues > 1 and scree plot inspection. CFA was performed to confirm the model identified in EFA. Model fit was evaluated using the Comparative Fit Index (CFI, > 0.90), Tucker-Lewis Index (TLI, > 0.90), and Root Mean Square Error of Approximation (RMSEA, < 0.08)33.
Statistics included descriptive methods [frequency, means (M), and standard deviations (SD)], comparative analysis using the t-test or ANOVA with posthoc test (when more than two groups were compared), frequency analysis, and determination of independent associations between variables using chi-square, correlation, and binomial regression analysis. Mediation analysis was conducted to examine whether job satisfaction components explained the relationship between occupational role (physician vs. nurse) and burnout levels. This approach was chosen to assess whether differences in burnout between physicians and nurses were driven by disparities in perceived job satisfaction. Identifying significant mediators helps to determine whether improving workplace conditions could serve as an intervention point to reduce burnout among HCWs. Statistical analysis was performed using Jamovi version 2.2.5. The level of statistical significance adopted was 5% (p < 0.05).
Ethical consideration
The study was approved by the Local Ethics Committees of “University Medical Center” Corporate Fund (extract from protocol No. 11 of December 30, 2021) and I.K. Akhunbaev Kyrgyz State Medical Academy (extract from protocol No. 13 of December 08, 2021). All methods were performed by the relevant guidelines and regulations.
Participation in the study was voluntary and all participants had the opportunity to get acquainted with the study’s aim and objectives. After reading the information about the study, HCWs were asked to go to the next page, thereby expressing their informed consent to participation.
Results
The study involved 2,685 healthcare workers from Central Asian countries (Fig. 1A): Kazakhstan (n = 1817, 67.7%), Kyrgyzstan (n = 534, 19.9%), and Uzbekistan (n = 334, 12.4%). Socio-demographic data are presented in Table 1. The majority of the study participants were female (n = 2211, 82.3%) The average age of the participants was M = 41.1 (SD = 13.0, Me = 38, ranging from 18 to 73). According to marital status, most of the study participants were either married (57.8%) or single (25.4%), at the same time the number of divorced was 314 (11.7%), and 136 (5.1%) remained widows. More than six-tenths (64.8%) of respondents were nurses. Moreover, 267 (9.9%) persons holding managerial positions took part in the study. The distribution of HCWs by type of organization varied significantly across countries (p < 0.001), with outpatient facilities being the most common workplace (47.4%), followed by inpatient settings (34.8%), emergency medical services (EMS, 13.7%), and national-level centers (4.1%). Regarding organization financing, the majority of HCWs worked in government-funded institutions (public, 94.3%), while private sector employment was most prevalent in Uzbekistan (27.8%), compared to Kazakhstan (3.0%) and Kyrgyzstan (1.3%) (p < 0.001).
40% of respondents (n = 1075) participated in front-line work during the COVID-19 pandemic. COVID-19 vaccination coverage among HCWs was 90.7% overall, but significantly lower in Uzbekistan (59.0%) compared to Kyrgyzstan (87.3%) and Kazakhstan (97.6%) (p < 0.001). Regarding COVID-19 history, 43.6% of HCWs never reported a COVID-19 infection, while severe cases were most prevalent in Uzbekistan (9.9%) and Kyrgyzstan (7.7%), compared to Kazakhstan (3.1%) (p < 0.001). The most common severity level was mild to moderate illness (43.5%), with significant variations across countries.
It should be noted that the data for Kazakhstan and Kyrgyzstan are similar in terms of most age-sex and professional characteristics. In Uzbekistan, they differ somewhat due to the relatively high prevalence of surveyed men and young age, hence in this sample, there were more single and fewer participants with children. Also noteworthy is the high percentage (29.0%) of managers compared to Kazakhstan (5.5%) and Kyrgyzstan (13.6%).
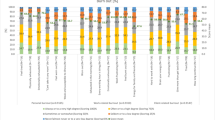
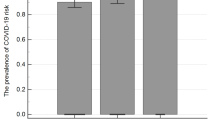
In general, the prevalence of burnout was 28.3%, and by dimensions: PB—43.3%, WRB—36.3%, CRB—28.0%. The overall level of burnout was 39.1 ± 18.2 and by dimensions: PB—43.6 ± 21.1, WRB—41.1 ± 20.4, CRB—32.5 ± 21.0. The prevalence and level of burnout by countries are shown in Table 2; Fig. 1B. The overall prevalence of burnout did not differ significantly in the three countries and varied between 27.3 and 32.3%. At the same time, the burnout level was significantly lower among HCWs in Kazakhstan compared to workers in Kyrgyzstan. Examining the individual components of burnout, it was noted that the highest rates and values of PB were noted among respondents from Kyrgyzstan (49.4%), and the lowest in Uzbekistan (36.5%), p < 0.001. Work-related burnout did not differ in the countries studied. Client-related burnout was significantly higher among HCWs in Uzbekistan in comparison with others (p < 0.001).

Overview of occupational burnout among healthcare workers (HCWs) in Kazakhstan (KZ), Kyrgyzstan (KG), and Uzbekistan (UZ). (A) Study population and prevalence of occupational burnout by country, presented as percentages of HCWs meeting burnout criteria. (B) Mean burnout levels (Personal Burnout, Work-Related Burnout, and Client-Related Burnout) across the three countries, with error bars representing standard deviations. Statistical significance between groups was determined using ANOVA (F) tests, with significant differences indicated as p < 0.05, p < 0.01, and *p < 0.001. (C) Forest plot of predictors of burnout based on logistic regression analysis for HCWs in each country. Odds ratios (OR) and 95% confidence intervals (CI) are presented, with a reference line at OR = 1. Significant predictors are highlighted as p < 0.05, p < 0.01, and *p < 0.001.
Occupational burnout and gender
The level and prevalence of burnout, depending on gender, had no significant differences in the three countries. However, in the overall study population, the burnout rate among women was slightly higher than among men, p < 0.05 (Table 3). As presented in Suppl. Tables 5–7, the level and prevalence of PB were significantly higher among female HCWs compared to men in Kazakhstan and Kyrgyzstan. At the same time, women in Uzbekistan were more vulnerable to WRB. Although the level of burnout associated with clients did not have a gender difference by country, in the overall structure, men HCWs were more susceptible to this dimension of burnout compared to women. In the regression model, female HCWs in Kazakhstan and Uzbekistan exhibited a significantly higher likelihood of experiencing occupational burnout compared to their male counterparts (Table 4; Fig. 1C). The odds ratio (OR) for female HCWs was 1.927 in Kazakhstan (p < 0.001) and 1.883 in Uzbekistan (p < 0.05). In the overall sample, being female was significantly associated with higher odds of burnout, with an OR of 1.750 (95% CI 1.324–2.312), p < 0.001.
Occupational burnout and family
In general, in Central Asian countries there were no differences in the level and prevalence of burnout depending on marital status among HCWs. However, among HCWs in Uzbekistan, single or married employees had lower burnout rates compared to divorced or widowed ones. Moreover, the prevalence of PB was higher among divorced or widowed people in three countries. Among HCWs, the presence of children was associated with lower levels of burnout, this was especially noticeable for CRB and Kyrgyzstani and Uzbekistani HCWs (Table 3, Suppl. Tables 5–7).
Regression analysis revealed significant associations between marital and parental statuses with burnout among HCWs, particularly in Kazakhstan. In Kazakhstan, married, divorced, and widowed HCWs demonstrated a significantly higher risk of burnout compared to single HCWs (p < 0.05). Additionally, HCWs with children exhibited a significantly lower likelihood of experiencing burnout compared to those without children (p < 0.001).
Occupational burnout and work
In general, physicians were more prone to burnout compared to nurses (p < 0.001). In Kazakhstan and Kyrgyzstan, the level and prevalence of burnout were significantly higher among doctors compared to nurses (p < 0.001). However, the burnout level among nurses was significantly higher compared to doctors in Uzbekistan (p < 0.05). Such differences were also noted for PB and WRB. Moreover, physicians in Kazakhstan were more prone to client-related burnout compared to nurses, p < 0.001 (Table 3, Suppl. Tables 5–7).
Analysis of burnout levels based on organization type revealed significant variations across countries. In Kazakhstan, outpatient HCWs exhibited significantly higher levels of burnout compared to those in inpatient settings (p < 0.05), with the most pronounced differences observed in PB and WRB. In Kyrgyzstan and Uzbekistan, the highest levels of burnout were recorded among HCWs working in national-level centers and outpatient settings, suggesting increased stress exposure in these healthcare environments.
Regarding organizational financing, no significant differences were observed in burnout levels between public and private healthcare organizations. However, in Kyrgyzstan, HCWs in private organizations exhibited higher levels of WRB, whereas in Uzbekistan, CRB was more pronounced among HCWs in private healthcare settings. These findings highlight potential country-specific workplace stressors influencing burnout levels. During the study, it was also found that management personnel was more prone to occupational burnout, this was especially noticeable in Uzbekistan (Table 3, suppl. Tables 5–7).
Regression analysis revealed significant associations between occupational role, organization type, and financing conditions with burnout among HCWs across the studied countries (Table 4). In Kazakhstan, physicians demonstrated significantly higher odds of experiencing burnout compared to nursing staff (OR = 2.359, p < 0.001). Additionally, HCWs from national-level health centers exhibited lower burnout levels compared to those in EMS (OR = 0.318, p < 0.05). At the same, no significant differences in burnout levels were observed between EMS and inpatient or outpatient settings. In Kyrgyzstan, HCWs working in private-sector healthcare organizations were significantly more likely to experience burnout (OR = 7.152, p < 0.05). In Uzbekistan, HCWs in outpatient settings and national-level centers exhibited significantly higher burnout levels compared to those in EMS, with odds ratios of 3.895 and 3.513, respectively. When analyzing the cumulative sample, only occupational role remained a significant predictor of burnout, with physicians demonstrating higher odds of experiencing burnout compared to nurses (OR = 1.647, 95%CI: 1.333–2.034, p < 0.001).
Occupational burnout and job satisfaction
Job satisfaction was evaluated using a five-factor scale derived from EFA and confirmed by CFA, which included: autonomy and task diversity, work environment and job demands, opportunities for professional growth and development, workplace support and engagement, and salary and financial compensation. The analysis of job satisfaction among HCWs in Kazakhstan, Kyrgyzstan, and Uzbekistan revealed significant differences across multiple dimensions (p < 0.05) (Fig. 2A, Suppl. Table 8). HCWs in Kazakhstan reported the highest overall job satisfaction (3.80 ± 0.99), followed by Kyrgyzstan (3.69 ± 0.88), and Uzbekistan (3.59 ± 0.91). Across all dimensions, HCWs in Uzbekistan reported the lowest satisfaction levels, particularly in work environment and job demands, and professional growth opportunities. Satisfaction with salary and financial compensation was lowest in Kyrgyzstan and highest in Uzbekistan, with significant differences across all post-hoc tests (p < 0.001).

Job Satisfaction, Impact of COVID-19 on Healthcare Workers, and Occupational Burnout in Central Asia. (A) Differences in job satisfaction and its components (autonomy and task diversity, work environment and job demands, professional growth opportunities, workplace support, and salary/financial compensation) among HCWs across the three countries. (B) Correlation between job satisfaction and occupational burnout. (C) Differences in job satisfaction between nurses and physicians across the three countries. (D) Job satisfaction among frontline and non-frontline HCWs across the three countries. (E) Impact of COVID-19 on personal life and work, including social stigma, psychological burden, lack of appreciation, and workload across the three countries. (F) Correlation between the impact of COVID-19 and occupational burnout. (G) Differences in the impact of COVID-19 on personal and professional life among frontline and non-frontline HCWs across the three countries. Statistical significance is indicated as follows: *p < 0.05, **p < 0.01, ***p < 0.001.
The correlation analysis revealed a negative association between occupational burnout (CBI) and job satisfaction, as well as its sub-dimensions (Fig. 2B, Suppl. Table 9). Overall job satisfaction showed a moderate negative correlation with burnout (r = − 0.430), indicating that higher levels of job satisfaction were associated with lower burnout levels. Among the job satisfaction factors, work environment and job demands (r = − 0.423) exhibited the strongest negative correlations with burnout. At the same time, salary and financial compensation demonstrated the weakest negative correlation (r = − 0.295).
The regression analysis examining the association between job satisfaction factors and burnout among HCWs revealed significant findings (Table 4). In Kazakhstan and Kyrgyzstan, a better work environment and lower job demands were significantly associated with lower levels of burnout (OR = 0.545, and OR = 0.422, respectively, p < 0.001). In the total sample, this association remained significant. Additionally, greater workplace support and involvement was linked to lower burnout risk in the total sample (OR = 0.832, p = 0.007), although this relationship was not significant within individual country samples. Other job satisfaction components, including autonomy, professional growth opportunities, and financial rewards, showed no significant associations with burnout across countries.
The analysis of job satisfaction between nurses and physicians revealed significant differences across several dimensions (Fig. 2C, Suppl. Table 10). Nurses reported higher overall job satisfaction (3.81 ± 0.95) compared to physicians (3.65 ± 0.98, p < 0.001). Nurses also had significantly higher satisfaction levels in autonomy and task diversity, work environment and job demands, and opportunities for professional growth and development (p < 0.001). However, no significant differences were observed in workplace support and engagement (p = 0.128) or salary and financial compensation (p = 0.677). At the same time, when assessing the overall job satisfaction between doctors and nurses in the three countries using the Bayesian ANOVA, the occupational role + country influence model is more likely (BF10 = 247.39) than other models (null model, only place of role, or only country, BF10 = 1-–172.45). Thus, the level of overall job satisfaction was higher among nurses in Kazakhstan and Kyrgyzstan, while in Uzbekistan this indicator was higher among doctors (Fig. 2C, Suppl. Table 11).
As shown in Table 3, the rate and level of burnout were higher among physicians than among nurses (p < 0.001). Next, we conducted a mediation analysis to examine the role of job satisfaction components in mediating the relationship between occupational role (physician vs. nurse) and burnout across three countries (Suppl. Tables 12–14). The analysis aimed to determine whether specific job satisfaction factors explain the association between occupational role and burnout levels. In Kazakhstan and Kyrgyzstan, only the work environment and job demands component demonstrated a significant mediating effect. The occupational role had a significant negative effect on the work environment and job demands (p < 0.001), and this factor was strongly associated with lower burnout levels (p < 0.001). These results suggest that a poor work environment and high job demands may contribute to burnout among healthcare workers in these countries, with differences between physicians and nurses being partially explained by workplace conditions. However, in Uzbekistan, none of the job satisfaction components showed a significant mediating effect, suggesting that the association between occupational role and burnout in this country may be influenced by other unmeasured factors. These findings highlight the importance of work environment and job demands in mitigating burnout among HCWs in Kazakhstan and Kyrgyzstan, particularly in explaining differences between physicians and nurses. However, in Uzbekistan, alternative mechanisms may be driving burnout, warranting further investigation into contextual workplace factors.
Occupational burnout and the COVID-19 pandemic
The analysis of COVID-19 infection history demonstrated a clear relationship between infection severity and burnout levels, where more severe COVID-19 cases were associated with more pronounced burnout (Tables 3 and 4, Suppl. Tables 5–7). In Kazakhstan, HCWs who experienced severe COVID-19 reported the highest burnout levels, followed by those with moderate illness (p < 0.001). Similar trends were observed in Kyrgyzstan (p < 0.05) and the total sample (p < 0.001), while in Uzbekistan, severe COVID-19 cases had significantly higher burnout levels compared to mild or asymptomatic cases (p < 0.001). Regression analysis confirmed that moderate to severe COVID-19 cases were significantly associated with an increased risk of burnout, particularly in Kazakhstan (OR = 1.700–3.555, p < 0.001) and the overall sample (OR = 1.346–2.270, p < 0.05).
COVID-19 vaccination did not show a significant association with burnout levels in Kazakhstan and Kyrgyzstan (p = 0.614, p = 0.385, respectively). However, in Uzbekistan, vaccinated HCWs exhibited significantly lower burnout levels and had a lower likelihood of experiencing burnout (OR = 0.485, p = 0.008), with this effect being primarily driven by lower client-related burnout (CRB), suggesting a potential protective role of vaccination in reducing patient-related emotional exhaustion (Tables 3 and 4, Suppl. Tables 5–7).
The perceived impact of COVID-19 on personal and work life varied significantly across countries (p < 0.001, Fig. 2E, Suppl. Table 15). Uzbekistan reported the highest levels of social stigma and psychological burden, followed by Kyrgyzstan and Kazakhstan, with all post-hoc comparisons significant (p < 0.001). Lack of appreciation was significantly lower in Kazakhstan compared to Kyrgyzstan and Uzbekistan (p < 0.05). COVID-19-related workload and job demands were rated significantly higher in Kyrgyzstan than in Kazakhstan (p < 0.001). Overall, the impact of COVID-19 was perceived as most severe in Uzbekistan, followed by Kyrgyzstan and Kazakhstan, with all post-hoc comparisons significant (p < 0.001). These results indicate that HCWs in Uzbekistan experienced the greatest psychological burden and perceived impact of the pandemic, while those in Kazakhstan reported lower levels of these stressors.
Correlation analysis revealed a significant negative association between job satisfaction and COVID-19-associated social stigma and psychological burden, lack of appreciation, workload and job demands (p < 0.05). Additionally, burnout showed significant positive correlations with social stigma (r = 0.280, p < 0.001), lack of appreciation (0.378, p < 0.001), workload (0.310, p < 0.001), and the overall impact of COVID-19 (0.420, p < 0.001), suggesting that these stressors contribute to increased burnout levels (Fig. 2F, Suppl. Table 16). Regression analysis demonstrated that social stigma and psychological burden, lack of appreciation, and workload and job demands were significant predictors of burnout across countries (Table 4). In Kazakhstan, all components of the perceived impact of COVID-19 on personal and work life were significantly associated with higher burnout levels. In Kyrgyzstan, social stigma and psychological burden (p = 0.003) and workload and job demands (p = 0.001) were also significant burnout predictors, whereas lack of appreciation did not show a significant effect. In Uzbekistan, only social stigma and psychological burden (p = 0.009) remained a significant predictor of burnout. In the combined sample, all three factors were significant predictors of burnout, with social stigma (OR = 1.290, p < 0.001), lack of appreciation (OR = 1.412, p < 0.001), and workload and job demands (OR = 1.614, p < 0.001) demonstrating strong associations. These findings highlight that the psychological burden of social stigma, perceived lack of appreciation, and excessive job demands are key contributors to burnout, though their impact varies across countries.
Among HCWs, 40% of respondents indicated that they were on the frontlines in the fight against the pandemic. HCWs working on the frontline in Kyrgyzstan and Uzbekistan reported significantly higher burnout levels compared to non-frontline workers (p < 0.05, Table 3), this was especially pronounced for personal and work-related burnout and among HCWs in Kyrgyzstan and Uzbekistan (Suppl. Tables 5 and 6). At the same time, frontline HCWs from Kazakhstan were more prone to client-related burnout (Suppl. Table 7). Regression analysis also indicated that frontline workers in Kyrgyzstan had a significantly higher risk of burnout (OR = 1.909, p = 0.015), while no significant differences were found in Kazakhstan, Uzbekistan, or the overall sample.
The impact of frontline work during the COVID-19 pandemic on social stigma, psychological burden, job satisfaction, and workplace stressors varied across countries (Fig. 2D and G, Suppl. Tables 17–19). In Kazakhstan, frontline HCWs reported significantly higher social stigma and psychological burden, and workload and job demands compared to non-frontline workers. However, job satisfaction was significantly lower among non-frontline HCWs compared to frontline workers. In Kyrgyzstan, similar patterns were observed, where frontline HCWs reported significantly higher social stigma and psychological burden than non-frontline workers. However, differences in workload and job demands, lack of appreciation, and job satisfaction were not statistically significant. In Uzbekistan, non-frontline HCWs reported significantly higher social stigma and psychological burden, lack of appreciation, and workload and job demands than non-frontline workers. Additionally, job satisfaction was significantly lower among non-frontline HCWs than frontline workers, indicating a reverse trend compared to Kazakhstan. These findings suggest that frontline workers in Kazakhstan and Kyrgyzstan experienced higher job-related stress and perceived burden of COVID-19, while in Uzbekistan, non-frontline HCWs reported greater psychological distress and lower job satisfaction. The differences in job satisfaction trends across countries highlight potential variations in work environments, institutional support, and pandemic-related challenges faced by different HCW groups.
Discussion
This cross-sectional study describes for the first time with a unified methodology the prevalence of occupational burnout, as well as the role of various factors associated with this syndrome among healthcare workers in Central Asian countries. Although researchers were unable to collect data from Tajikistan and Turkmenistan due to various organizational barriers, health workers from Kazakhstan, Kyrgyzstan, and Uzbekistan participated in the current study, with a total sample of 2685 respondents.
Prevalence of occupational burnout in central Asian countries
The prevalence of occupational burnout in the studied countries ranged from 27.3 to 32.3% and did not have significant differences. These values were lower than in other low- and middle-income countries, such as China (86.2%), Zambia (51.2%), Cameroon (42.4%), Egypt (41.8%), Mexico (39.7–42.3%); at the same level as Brazil (24.1–29.3%); and more than in Thailand (10.7%), West Bank and Gaza Strip (10.6%), Ethiopia (4.6%)3,34,35,36,37,38,39,40,41,42,43,44. In turn, these data are not comparable due to the different years of the study, the use of other scales, and the different categories of HCWs. Moreover, the researchers also noticed that studies that used the CBI scales recorded higher burnout compared to studies that used the Maslach Burnout Inventory45. If we take into account those studies where the CBI scale was used, regardless of income level, then among Italian HCWs, the prevalence of burnout was as much as 71.6%, 48% in Saudi Arabia, 46% in Sri Lanka, and India − 39.3%10,46,47. Thus, the authors of the study emphasize that due to different research methods and methodologies, it is still difficult to compare data on the prevalence of burnout by country.
Personal burnout was more common among HCWs in Kyrgyzstan, and least common in Uzbekistani HCWs. The authors suggest that this difference may be due to the relatively young sample and a greater degree of satisfaction with salary among HCWs in Uzbekistan (Suppl. Table 5). At the same time, HCWs in Uzbekistan were more than half a tare times more likely to experience client-related burnout compared to HCWs in the other two countries.
Socio-demographic factors and occupational burnout
According to the UN Human Development Reports gender inequality index for countries involved in the study was at a medium level (GII KZ = 0.161, UZ = 0.227, KG = 0.370) in 202148. Our findings revealed that overall burnout prevalence and severity did not significantly differ between men and women HCWs in any of the three countries. However, when analyzing burnout by its components, distinct gender-related patterns emerged. In Kazakhstan and Kyrgyzstan, female HCWs reported significantly higher levels and prevalence of PB compared to their male counterparts, suggesting that women may experience greater emotional and physical exhaustion in these settings. In Uzbekistan, women exhibited a higher prevalence of WRB, indicating that occupational demands may disproportionately affect female HCWs in this country. In contrast, CRB did not significantly differ between men and women in any of the three countries. However, when analyzing the total sample, male HCWs demonstrated higher levels and prevalence of CRB, suggesting that male professionals may perceive lower social support from colleagues or experience greater interpersonal strain at work. Regression analysis further highlighted country-specific gender differences in burnout risk. In Kazakhstan and Uzbekistan, female HCWs had significantly higher odds of experiencing burnout compared to male HCWs (OR = 1.927 in Kazakhstan, OR = 1.750 in Uzbekistan, p < 0.001), indicating a greater vulnerability among women in these healthcare settings. However, in Kyrgyzstan, no significant gender differences in burnout risk were observed, suggesting that other contextual factors may influence burnout dynamics in this country.
The higher prevalence of burnout among female healthcare workers HCWs may be influenced by a combination of professional and personal stressors. Women in healthcare often struggle with work-life integration due to additional caregiving responsibilities, which may contribute to greater emotional exhaustion. They are also more likely to engage in emotionally demanding tasks, which increases psychological strain. Workplace inequities, such as limited career advancement opportunities and lower professional autonomy, may increase the risk of burnout49. Additionally, excessive job demands with inadequate institutional support place a disproportionate burden on female HCWs, exacerbating stress and emotional exhaustion. Differences in coping mechanisms and emotional sensitivity to stress may also make women more vulnerable to burnout50. In our study, these disparities were particularly evident in the higher prevalence of PB among women in Kazakhstan and Kyrgyzstan and WRB among women in Uzbekistan, aligning with previous findings that highlight gender-specific stressors in healthcare settings.
Burnout was 1.7 times more prevalent among female physicians compared to their male counterparts (95% CI 1.24–2.31, p < 0.001), whereas no significant gender differences were observed among nurses. When analyzing individual components of burnout by gender and occupation, personal burnout was significantly more common among women regardless of their job role, with female physicians showing an OR of 2.22 (95% CI 1.65–2.98, p < 0.001) and female nurses an OR of 1.71 (95% CI 1.25–2.33, p < 0.001). Work-related burnout was also more prevalent among female physicians compared to males (OR = 2.05, 95% CI 1.52–2.77, p < 0.001), while client-related burnout showed no significant differences based on gender or occupation. A meta-analysis by Rotenstein et al. concluded that the association between gender and burnout among physicians remains inconclusive51. However, two systematic reviews found that female physicians tend to experience higher levels of burnout52,53. In contrast, a meta-analysis by López-López et al. on nurses suggested that male nurses were more likely to experience burnout54.
Our study found no significant differences in the overall prevalence and severity of occupational burnout across marital and parental status in the three countries. However, when analyzing burnout components and adjusting for potential confounders, distinct patterns emerged. Thus, in Kazakhstan and Kyrgyzstan, divorced and widowed HCWs exhibited a significantly higher prevalence of PB compared to single or married individuals (p < 0.05). In Uzbekistan, single HCWs had higher levels of CRB compared to their married counterparts (p < 0.05). Furthermore, results from the regression analysis in Kazakhstan indicated that married, divorced, and widowed HCWs had a significantly higher risk of burnout compared to single individuals (p < 0.05). The association between marital status and burnout aligns with previous research indicating that while marriage can provide emotional and social support, it may also introduce additional stressors, particularly for those balancing work and family responsibilities55. Family support has been shown to mitigate emotional exhaustion, which may explain why divorced and widowed HCWs in our study exhibited higher levels of personal burnout56.
Parental status also played a significant role in burnout levels. HCWs with children exhibited lower overall burnout levels in Kyrgyzstan and Uzbekistan (p < 0.05). More specifically, in Uzbekistan, those with children had significantly lower levels of PB (p < 0.05), indicating that parenthood may provide emotional fulfillment or a sense of purpose that mitigates exhaustion. In both Kyrgyzstan and Uzbekistan, WRB was lower among HCWs with children (p < 0.05), suggesting that parental responsibilities may shift professional stress perception or coping mechanisms. In Kazakhstan and Kyrgyzstan, CRB levels were lower among HCWs with children (p < 0.05), which could be attributed to improved interpersonal skills, patience, or perspective gained through parenting. Moreover, on the regression model having children was associated with a lower level of burnout (p < 0.001) in Kazakhstan, reinforcing the idea that parenthood may offer a psychological buffer against occupational stress. Therefore, the protective role of parenthood observed in our findings is consistent with evidence suggesting that family support enhances resilience and reduces stress among HCWs56.
Occupational factors and burnout
According to a meta-analysis conducted by Rotenstein et al., the burnout rate among physicians was 67%, another meta-analysis showed that among European physicians’ burnout prevalence rates ranged from 2.5 to 72.0%51,57. Among nurses, a meta-analysis based on data from 49 countries found that the overall pooled prevalence of burnout symptoms among global nurses was 11.23%58. Comparing oncologists and oncology nurses, HaGani et al. concluded that the level of depersonalization is more common among physicians59. Similarly, in our study, the prevalence and level of burnout were significantly higher among doctors compared to nurses. However, in Uzbekistan, the level of burnout among nurses was higher in comparison to doctors; this was especially noticeable for personal and work-related burnout.
Our study highlights significant variations in burnout levels among HCWs across different organizational settings and financing structures. Overall, burnout was significantly higher among outpatient HCWs compared to those in inpatient settings, particularly in PB and WRB. This may be attributed to higher patient volumes, administrative burdens, medicolegal concerns, and limited teamwork opportunities in outpatient settings, whereas inpatient physicians may benefit from shift work flexibility and stronger team collaboration, both of which have been associated with lower levels of burnout60. Moreover, in Kyrgyzstan and Uzbekistan, burnout levels were also higher among HCWs in national-level centers, which requires further detailed comparative analysis.
Regarding organizational financing, no significant differences in burnout levels were observed between public and private healthcare organizations at the aggregate level. However, country-specific differences emerged in Kyrgyzstan, HCWs in private organizations reported higher WRB, while in Uzbekistan, CRB was more pronounced among private sector HCWs. These results suggest that workplace stressors in the private sector may vary by country, potentially influenced by factors such as job security, financial pressure, and patient expectations.
A notable finding was the higher susceptibility to burnout among management personnel, particularly in Uzbekistan. This aligns with prior research suggesting that healthcare leaders often experience increased occupational stress due to administrative pressures, workforce shortages, and institutional responsibilities. The authors suggest that a large share of responsibility among department heads carries a risk of emotional exhaustion since the distribution of responsibility can lead to a decrease in burnout61. Previous research indicates that healthcare managers face higher stress and lower well-being than regular HCWs due to increased administrative burdens and decision-making pressures. Factors such as heightened work demands during the pandemic, team conflicts, staff shortages, and a lack of recognition from hospital management further increase the risk of depression, anxiety, and stress symptoms, emphasizing the need for targeted leadership support strategies62.
Job satisfaction and occupational burnout
Job satisfaction is an individualized positive feeling and attitude toward a job and consists of many working environment factors63. Moreover, organizational culture can affect burnout64. This study analyzed and compared the job satisfaction of HCWs in three Central Asian countries. Our findings highlight significant variations in job satisfaction across countries and occupational roles, with Kazakhstan reporting the highest satisfaction levels and Uzbekistan the lowest. The strongest dissatisfaction among Uzbekistani HCWs was observed in the work environment, job demands, and professional growth opportunities, suggesting structural and systemic workplace challenges. Interestingly, salary satisfaction was highest in Uzbekistan, yet it had the weakest correlation with burnout, indicating that financial compensation alone does not mitigate occupational stress. At the same time, correlation analysis showed a significant negative relationship between satisfaction with salary and the level of burnout (Suppl. Table 9), which is also reflected in other studies65,66,67.
The observed negative correlation between job satisfaction and burnout aligns with previous research68,69,70, emphasizing that improving workplace conditions can play a crucial role in reducing HCW exhaustion. Regression analysis confirmed that better work environments and lower job demands were significantly associated with lower levels of burnout risk, particularly in Kazakhstan and Kyrgyzstan. However, other job satisfaction dimensions, such as autonomy, professional growth, and financial rewards, showed no significant protective effect against burnout, underscoring the dominant role of workplace conditions over personal career advancement factors.
Regarding occupational role differences, nurses reported higher overall job satisfaction than physicians, particularly in autonomy, task diversity, and professional development opportunities. Mediation analysis further demonstrated that work environment and job demands significantly explained the burnout gap between nurses and physicians in Kazakhstan and Kyrgyzstan, highlighting the impact of occupational stressors specific to physicians. However, in Uzbekistan, no job satisfaction components significantly mediated the relationship between occupational role and burnout, suggesting that alternative workplace factors may influence burnout risks in this setting.
These findings underscore the critical role of workplace environment and job demands in mitigating burnout, particularly in differentiating physician and nurse experiences. Interventions aimed at improving working conditions, optimizing workloads, and fostering organizational support may be key strategies to enhance HCWs’ well-being71,72. Further research is needed to explore country-specific drivers of burnout in CA countries to develop contextually relevant interventions.
Occupational burnout and the COVID-19 pandemic
Our findings reveal a significant relationship between COVID-19 infection severity and burnout levels, with moderate to severe COVID-19 cases being associated with higher burnout risk, particularly in Kazakhstan and the overall sample. This aligns with prior research showing that prolonged illness and post-COVID-19 complications can contribute to emotional exhaustion and work-related stress73. Moreover, high levels of burnout have been strongly associated with an increased risk of COVID-19 infection, indicating a possible link between burnout and susceptibility to infection among high-risk HCWs74.
Vaccination status was not significantly associated with burnout levels in Kazakhstan and Kyrgyzstan, while in Uzbekistan, vaccinated HCWs exhibited lower burnout, primarily due to CRB. This association suggests that vaccination may be linked to a lower level of patient-related emotional exhaustion, though further exploration is needed to confirm a potential protective effect. On the other side, previous research has shown that COVID-19-related burnout can reduce vaccination willingness, suggesting that exhaustion and emotional strain may contribute to vaccine hesitancy among HCWs75.
The COVID-19 pandemic and the associated changes in work and daily life have undoubtedly affected the mental health of HCWs. According to one systematic review, the following factors increased the risk of burnout among nurses: reducing social support, low readiness of family members and colleagues to cope with the COVID-19 outbreak, an increased perceived threat of COVID-19, longer working time in quarantine, work among high risk, work in hospitals with inadequate and insufficient material and human resources, increased workload and lower level of specialized training on COVID-1976. Data from another systematic review among HCWs argued that the relationship between burnout development and frontline work was controversial77.
The perceived impact of COVID-19 on personal and professional life varied across countries, with Uzbekistan reporting the highest levels of social stigma and psychological burden, followed by Kyrgyzstan and Kazakhstan. A lack of appreciation from management and high workload demands were significantly associated with burnout, with variations across countries. Regression analysis confirmed that social stigma, workload, and lack of appreciation were significantly associated with burnout, suggesting that workplace perceptions and organizational support may play an important role in occupational stress.
Frontline work further influenced burnout patterns, with notable country-specific variations. In Kyrgyzstan and Uzbekistan, frontline HCWs experienced significantly higher burnout levels, particularly in personal and work-related domains, likely due to elevated social stigma, psychological burden, and increased job demands associated with COVID-19 response efforts. In contrast, in Kazakhstan, CRB was more pronounced among frontline workers, which may be attributed to lower job satisfaction and a greater perceived impact of COVID-19 on work and daily life (Suppl. Table 20), possibly reflecting differences in healthcare system organization and patient care dynamics. Interestingly, in Uzbekistan, non-frontline HCWs reported greater psychological distress, lack of appreciation, heavier workloads, and lower job satisfaction compared to frontline workers. This suggests that non-frontline staff in Uzbekistan may have faced unique workplace stressors, such as unclear roles, inadequate institutional support, or an uneven distribution of pandemic-related workload, which could be linked to systemic challenges in healthcare administration. These country-specific differences in burnout patterns highlight the influence of healthcare infrastructure, institutional responses to the pandemic, and variations in workplace stressors across different healthcare settings. Addressing these challenges through targeted workplace interventions, improved institutional support, and equitable workload distribution may help mitigate burnout risk among HCWs.
These findings emphasize the complex interplay between infection history, workplace stressors, and perceived support in shaping burnout levels. Addressing social stigma, ensuring recognition of HCWs’ efforts, and optimizing workload distribution are essential for reducing burnout and improving job satisfaction. Given the country-specific variations observed, further research is needed to identify tailored interventions that address the unique challenges faced by HCWs in different healthcare settings.
Study limitations
Several limitations should be acknowledged in this study. First, the cross-sectional design prevents the establishment of causal relationships between the examined factors and burnout levels. Longitudinal studies are needed to assess the long-term impact of occupational stressors and COVID-19 on HCWs well-being. Second, the study relied on an online survey, which, while convenient for reaching a broad sample, may introduce sampling bias by excluding HCWs with limited internet access or those less familiar with digital platforms. Additionally, the survey was conducted only in Russian, potentially limiting participation among HCWs who primarily speak national languages, thereby affecting the representativeness of the sample. Third, key variables such as years of work experience, pre-existing illnesses, and the amount of time frontline HCWs spent working at the frontline were not collected, which could have provided additional insights into factors influencing burnout. Furthermore, the study was conducted during a specific period, capturing only a snapshot of burnout levels rather than long-term trends. Fourth, the sample size in Uzbekistan was lower than the estimated minimum requirement, potentially reducing the statistical power for country-specific comparisons. Additionally, non-response bias may have influenced the findings, as HCWs who chose not to participate may have had different burnout levels or workplace experiences compared to respondents. Fifth, the absence of HCWs from Tajikistan and Turkmenistan limits the generalizability of the findings across Central Asia. Future studies should aim for broader regional representation to provide a more comprehensive understanding of burnout patterns in the region. Sixth, the study assessed burnout using only the Copenhagen Burnout Inventory CBI. While the CBI is a validated and widely used tool, incorporating other established burnout measures could provide complementary insights and allow for broader comparisons with international studies. Lastly, the results presented in this study are generalizable to the overall sample, but further targeted research is needed to explore burnout dynamics among specific subgroups of HCWs. Investigating burnout predictors across different healthcare roles, workplace settings, and hierarchical positions would enhance the applicability of these findings and inform tailored interventions.
Conclusion
The overall prevalence of occupational burnout among HCWs in Central Asia was 28.3%, highlighting the urgent need for interventions to mitigate this issue. Occupational burnout not only affects HCWs’ well-being but also has organizational, economic, and systemic implications for healthcare institutions and governments in the region. Our findings demonstrate that gender, occupational and leadership roles, frontline work during the COVID-19 pandemic, family status, parental responsibilities, and COVID-19 infection history were associated with burnout risk. Additionally, job satisfaction components and the perceived impact of COVID-19 on personal and professional life significantly influenced burnout levels, though with varying effects across countries.
Given these findings, future research should focus on longitudinal studies to track burnout progression over time and evaluate the long-term effects of workplace interventions. Moreover, targeted research among specific healthcare professions and settings, including specialists, rural HCWs, and emergency care providers, is needed to develop tailored strategies for burnout prevention. Addressing burnout through systematic policy measures, organizational support, and workplace improvements can not only enhance HCWs’ well-being but also strengthen patient care quality, workforce retention, and the overall resilience of healthcare systems in Central Asia.
Data availability
All data available by request to corresponding author.
References
Bridgeman, P. J., Bridgeman, M. B. & Barone, J. Burnout syndrome among healthcare professionals. Am. J. Health-Syst. Pharm. 75 (3), 147–152. https://doi.org/10.2146/ajhp170460 (2017).
Romani, M. & Ashkar, K. Burnout among physicians. Libyan J. Med. 9 (1), 23556. https://doi.org/10.3402/ljm.v9.23556 (2014).
Wright, T. et al. Burnout among primary health-care professionals in low- and middle-income countries: systematic review and meta-analysis. Bull. World Health Organ. 100 (6), 385–401A. https://doi.org/10.2471/BLT.22.288300 (2022).
World Health Organization. Protecting health and care workers’ mental health and well-being: Technical Consultation Meeting. https://www.who.int/news/item/25-04-2024-202404_protecthw_mentalhealth (2024).
Leo, C. G. et al. Burnout among healthcare workers in the COVID 19 era: A review of the existing literature. Front. Public. Health. 9, 750529. https://doi.org/10.3389/fpubh.2021.750529 (2021).
Alsulimani, L. K. et al. Health care worker burnout during the COVID-19 pandemic: A cross-sectional survey study in Saudi Arabia. Saudi Med. J. 42 (3), 306–314. https://doi.org/10.15537/smj.2021.42.3.20200812 (2021).
Antoniadou, M. Estimation of factors affecting burnout in Greek dentists before and during the COVID-19 pandemic. Dent. J. 10 (6), 108. https://doi.org/10.3390/dj10060108 (2022).
Aljabri, D. et al. Sociodemographic and occupational factors associated with burnout: A study among frontline healthcare workers during the COVID-19 pandemic. Front. Public. Health. 10, 854687. https://doi.org/10.3389/fpubh.2022.854687 (2022).
Bolatov, A., Baikanova, R., Igenbayeva, B. & Seisembekov, T. Health care providers have faced the pandemic altruistically, but financial support is important for their well-being and motivation to work. Public. Health. 240, 119–124. https://doi.org/10.1016/j.puhe.2025.01.023 (2025).
Fiabane, E. et al. Prevalence and determinants of Italian physicians’ burnout in the post-COVID-19 era. Int. Arch. Occup. Environ. Health. 96 (3), 377–387. https://doi.org/10.1007/s00420-022-01929-6 (2023).
Ching, S. M. et al. Psychological distress among healthcare providers during COVID-19 in Asia: systematic review and meta-analysis. PLoS One. 16 (10), e0257983. https://doi.org/10.1371/journal.pone.0257983 (2021).
Huang, J., Huang, Z. T., Sun, X. C., Chen, T. T. & Wu, X. T. Mental health status and related factors influencing healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. PLoS One. 19 (1), e0289454. https://doi.org/10.1371/journal.pone.0289454 (2024).
Health Worker Mental Health Crisis. Centers for Disease Control and Prevention. https://www.cdc.gov/vitalsigns/health-worker-mental-health/index.html (2023).
Sexton, J. B. et al. Emotional exhaustion among US health care workers before and during the COVID-19 pandemic, 2019–2021. JAMA Netw. Open. 5 (9), e2232748. https://doi.org/10.1001/jamanetworkopen.2022.32748 (2022).
Quesada-Puga, C. et al. Job satisfaction and burnout syndrome among intensive-care unit nurses: A systematic review and meta-analysis. Intensive Crit. Care Nurs. 82, 103660. https://doi.org/10.1016/j.iccn.2024.103660 (2024).
Coimbra, B. M. et al. Moral injury and mental health among health-care workers during the COVID-19 pandemic: meta-analysis. Eur. J. Psychotraumatol. 15 (1), 2299659. https://doi.org/10.1080/20008066.2023.2299659 (2023).
Busch, I. M., Moretti, F., Mazzi, M., Wu, A. W. & Rimondini, M. What we have learned from two decades of epidemics and pandemics: A systematic review and Meta-Analysis of the psychological burden of frontline healthcare workers. Psychother. Psychosom. 90 (3), 178–190. https://doi.org/10.1159/000513733 (2021).
Asian Development Bank. Central and West Asia health sector approach 2025. https://www.adb.org/sites/default/files/publication/890891/central-west-asia-health-sector-approach-2025.pdf (2025).
Semenova, Y., Lim, L., Salpynov, Z., Gaipov, A. & Jakovljevic, M. Historical evolution of healthcare systems of post-soviet Russia, Belarus, Kazakhstan, Kyrgyzstan, Tajikistan, Turkmenistan, Uzbekistan, Armenia, and Azerbaijan: A scoping review. Heliyon 10 (8), e29550. https://doi.org/10.1016/j.heliyon.2024.e29550 (2024).
Rechel, B. et al. Primary care reforms in central Asia—On the path to universal health coverage? Health Policy Open. 5, 100110. https://doi.org/10.1016/j.hpopen.2023.100110 (2023).
Vinnikov, D. et al. Occupational burnout and lifestyle in Kazakhstan cardiologists. Arch. Public. Health = Archives Belges De Sante Publique. 77 (13). https://doi.org/10.1186/s13690-019-0345-1 (2019).
Vinnikov, D. et al. Occupational burnout in oncologists in Kazakhstan. Occup. Med. (Oxford England). 71 (8), 375–380. https://doi.org/10.1093/occmed/kqab121 (2021).
Lее, S. et al. Prevalence and factors ofprofessional burnout among primary healthcare workersaccepted manuscript.Accepted manuscript in the Republic of Kazakhstan: results of a national study.Georgian medical news 352–353, 59–68 (2024).
Migina, L., Myssayev, A., Meirmanov, S. & Uristemova, A. Professional burnout in primary health care workers of the Republic of Kazakhstan. Clin. Epidemiol. Glob. Health. 23. https://doi.org/10.1016/j.cegh.2023.101359 (2023).
Maxudova, M. et al. Burnout Among Hospital Nurses in Kazakhstan. https://doi.org/10.20944/preprints202501.1410.v1 (2025).
Kristensen, T. S., Borritz, M., Villadsen, E. & Christensen, K. B. The Copenhagen burnout inventory: a new tool for the assessment of burnout. Work Stress. 19, 192–207. https://doi.org/10.1080/02678370500297720 (2005).
Seisembekov, T., Brimkulov, N., Taalaikanova, A., Smailova, G. & Bolatov, A. Validation of the Russian version of the Copenhagen burnout inventory among the nurses in Kazakhstan and Kyrgyzstan. Int. J. Nurs. Sci. https://doi.org/10.1016/j.ijnss.2025.02.004 (2025).
Borritz, M. et al. Burnout among employees in human service work: design and baseline findings of the PUMA study. Scand. J. Publ. Health. 34 (1), 49–58. https://doi.org/10.1080/14034940510032275 (2006).
Taber, K. S. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res. Sci. Educ. 48 (6), 1273–1296. https://doi.org/10.1007/s11165-016-9602-2 (2018).
Okaro, A. O., Eze, C. U. & Ohagwu, C. C. Survey of job satisfaction among Nigerian radiographers in South-Eastern. Nigeria. Eur. J. Sci. Res. 39, 448–456 (2010).
Khamlub, S. et al. Job satisfaction of health-care workers at health centers in Vientiane capital and Bolikhamsai Province, Lao PDR. Nagoya J. Med. Sci. 75 (3–4), 233–241 (2013).
Pham, Q. T. et al. Impacts of COVID-19 on the life and work of healthcare workers during the nationwide partial lockdown in Vietnam. Front. Psychol. 12, 563193. https://doi.org/10.3389/fpsyg.2021.563193 (2021).
Field, A. Discovering Statistics Using IBM SPSS Statistics: And Sex and Drugs and Rock N Roll, 4th Edition, Sage, Los Angeles, London, New Delhi (2013).
Mandengue, S. H. et al. Syndrome de burnout Chez les médecins généralistes de La région de Douala (Cameroun): les activités physiques peuvent-elles être Un facteur Protecteur ? [Burnout syndrome among generalist medical doctors of Douala region (Cameroon): Can physical activities be a protective factor?]. Rev. Med. Brux. 38 (1), 10–15 (2017).
López-León, E., Rodríguez-Moctezuma, J. R., López-Carmona, J. M., Peralta-Pedrero, M. L. & Munguía-Miranda, C. Desgaste profesional En médicos familiares y Su asociación Con factores sociodemográficos y laborales. Rev. Med. Inst. Mex Seguro Soc. 45(1), 13–19 (2007).
Kotb, A. A., Mohamed, K. A., Kamel, M. H., Ismail, M. A. R. & Abdulmajeed, A. A. Comparison of burnout pattern between hospital physicians and family physicians working in Suez Canal University Hospitals. Pan. Afr. Med. J. 18(2), 164. https://doi.org/10.11604/pamj.2014.18.164.3355 (2014).
Charoentanyarak, A., Anothaisintawee, T., Kanhasing, R. & Poonpetcharat, P. Prevalence of burnout and associated factors among family medicine residency in Thailand. J. Med. Educ. Curric. Dev. 287, 1–8. https://doi.org/10.1177/2382120520944920 (2020).
Aranda, C., Pando, M., Aranda, M., Guadalupe Salazar, J. & Torres, T. Síndrome de burnout y Apoyo social En Los médicos familiares de base Del Instituto Mexicano Del Seguro social (IMSS) Guadalajara, México. Rev. Psiquiatr. Fac. Med. Barc. 31 (4), 142–150 (2004). Spanish.
Hu, H. X. et al. Factors related to job burnout among community nurses in Changchun, China. J. Nurs. Res. 23 (3), 172–180. https://doi.org/10.1097/jnr.0000000000000072 (2015).
Alshawish, E. & Nairat, E. Burnout and psychological distress among nurses working in primary health care clinics in West Bank–Palestine. Int. J. Ment. Health. 49 (4), 321–335. https://doi.org/10.1080/00207411.2020.1752064 (2020).
da Silva, A. T. C. & Menezes, P. R. Burnout syndrome and common mental disorders among community-based health agents. Rev Saude Publica. 42(5), 921–929. https://doi.org/10.1590/S0034-89102008000500019 (2008).
Kruse, G. R. et al. Burnout and use of HIV services among health care workers in Lusaka district, Zambia: a cross-sectional study. Hum. Resour. Health. 7(1), 55. https://doi.org/10.1186/1478-4491-7-55 (2009).
Mota, C. M., Dosea, G. S. & Nunes, P. S. Avaliação da presença da síndrome de burnout em agentes comunitários de saúde no município de Aracaju, Sergipe, Brasil. Cien Saude Colet. 19(12), 4719–4726. https://doi.org/10.1590/1413-812320141912.02512013 (2014).
Selamu, M., Hanlon, C., Medhin, G., Thornicroft, G. & Fekadu, A. Burnout among primary healthcare workers during implementation of integrated mental healthcare in rural Ethiopia: a cohort study. Hum. Resour. Health. 17(1), 58. https://doi.org/10.1186/s12960-019-0383-3 (2019).
Alahmari, M. A. et al. Prevalence of burnout in healthcare specialties: A systematic review using Copenhagen and Maslach burnout inventories. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 28, e938798. https://doi.org/10.12659/MSM.938798 (2022).
Kulkarni, S. et al. Stress and professional burnout among newly graduated dentists. J. Int. Soc. Prev. Community Dent. 6 (6), 535–541 (2016).
Fernando, B. M. & Samaranayake, D. L. Burnout among postgraduate Doctors in Colombo: prevalence, associated factors and association with self-reported patient care. BMC Med. Educ. 19 (1), 373 (2019).
United Nations. (n.d.). Gender Inequality Index. Human Development Reports. https://hdr.undp.org/data-center/thematic-composite-indices/gender-inequality-index#/indicies/GII
Karakcheyeva, V., Willis-Johnson, H., Corr, P. G. & Frame, L. A. The Well-Being of women in healthcare professions: A comprehensive review. Glob. Adv. Integr. Med. Health. 13, 27536130241232929. https://doi.org/10.1177/27536130241232929 (2024).
Nagle, E. et al. Factors affecting healthcare workers burnout and their conceptual models: scoping review. BMC Psychol. 12 (1), 637. https://doi.org/10.1186/s40359-024-02130-9 (2024).
Rotenstein, L. S. et al. Prevalence of burnout among physicians: A systematic review. JAMA 320 (11), 1131–1150. https://doi.org/10.1001/jama.2018.12777 (2018).
Galaiya, R., Kinross, J. & Arulampalam, T. Factors associated with burnout syndrome in surgeons: a systematic review. Ann. R. Coll. Surg. Engl. 102 (6), 401–407. https://doi.org/10.1308/rcsann.2020.0040 (2020).
Hoff, T. & Lee, D. R. Burnout and physician gender: what do we know?? Med. Care. 59 (8), 711–720. https://doi.org/10.1097/MLR.0000000000001584 (2021).
López-López, I. M. et al. Prevalence of burnout in mental health nurses and related factors: a systematic review and meta-analysis. Int. J. Ment. Health Nurs. 28 (5), 1032–1041. https://doi.org/10.1111/inm.12606 (2019).
Chen, Y. H. et al. Effect of marriage on burnout among healthcare workers during the COVID-19 pandemic. Int. J. Environ. Res. Public Health. 19 (23), 15811. https://doi.org/10.3390/ijerph192315811 (2022).
Shin, Y., Hur, W. M. & Park, K. The power of family support: the Long-Term effect of Pre-COVID-19 family support on Mid-COVID-19 work outcomes. Int. J. Environ. Res. Public Health. 18 (19), 10524. https://doi.org/10.3390/ijerph181910524 (2021).
Hiver, C., Villa, A., Bellagamba, G. & Lehucher-Michel, M. P. Burnout prevalence among European physicians: a systematic review and meta-analysis. Int. Arch. Occup. Environ. Health. 95 (1), 259–273. https://doi.org/10.1007/s00420-021-01782-z (2022).
Woo, T., Ho, R., Tang, A. & Tam, W. Global prevalence of burnout symptoms among nurses: A systematic review and meta-analysis. J. Psychiatr. Res. 123, 9–20. https://doi.org/10.1016/j.jpsychires.2019.12.015 (2020).
HaGani, N., Yagil, D. & Cohen, M. Burnout among oncologists and oncology nurses: A systematic review and meta-analysis. Health Psychol. 41 (1), 53–64. https://doi.org/10.1037/hea0001155 (2022).
Roberts, D. L., Cannon, K. J., Wellik, K. E., Wu, Q. & Budavari, A. I. Burnout in inpatient-based versus outpatient-based physicians: a systematic review and meta-analysis. J. Hosp. Med. 8 (11), 653–664. https://doi.org/10.1002/jhm.2093 (2013).
Liu, Y. et al. Internal corporate social responsibility and employee burnout: an employee management perspective from the healthcare sector. Psychol. Res. Behav. Manag. 16, 283–302. https://doi.org/10.2147/PRBM.S388207 (2023).
Seisembekov, T. et al. Mental health and well-being of healthcare workers in central Asia. F1000Research 13, 872. https://doi.org/10.12688/f1000research.153832.1 (2024). version 1; peer review: 1 not approved.
Alrawashdeh, H. M. et al. Occupational burnout and job satisfaction among physicians in times of COVID-19 crisis: a convergent parallel mixed-method study. BMC Public. Health. 21 (1), 811. https://doi.org/10.1186/s12889-021-10897-4 (2021).
Johnson, T. & Shamroukh, S. Predictive modeling of burnout based on organizational culture perceptions among health systems employees: a comparative study using correlation, decision tree, and bayesian analyses. Sci. Rep. 14, 6083. https://doi.org/10.1038/s41598-024-56771-2 (2024).
Ogresta, J., Rusac, S. & Zorec, L. Relation between burnout syndrome and job satisfaction among mental health workers. Croatian Med. J. 49 (3), 364–374. https://doi.org/10.3325/cmj.2008.3.364 (2008).
Yan, H. et al. Mediation role of perceived social support and burnout on financial satisfaction and turnover intention in primary care providers: a cross-sectional study. BMC Health Serv. Res. 21 (1), 252. https://doi.org/10.1186/s12913-021-06270-1 (2021).
Kabir, M. J. et al. Job burnout, job satisfaction, and related factors among health care workers in Golestan Province. Iran. Electron. Phys. 8 (9), 2924–2930. https://doi.org/10.19082/2924 (2016).
Alves, D. F. & Guirardello, E. B. Safety climate, emotional exhaustion and job satisfaction among Brazilian paediatric professional nurses. Int. Nurs. Rev. 63 (3), 328–335. https://doi.org/10.1111/inr.12276 (2016).
Myhren, H., Ekeberg, O. & Stokland, O. Job satisfaction and burnout among intensive care unit nurses and physicians. Crit. Care Res. Pract. 2013, 786176. https://doi.org/10.1155/2013/786176 (2013).
Oliveira, A. M., Silva, M. T., Galvão, T. F. & Lopes, L. C. The relationship between job satisfaction, burnout syndrome and depressive symptoms: an analysis of professionals in a teaching hospital in Brazil. Medicine 97 (49), e13364. https://doi.org/10.1097/MD.0000000000013364 (2018).
Galanis, P. et al. Increased job burnout and reduced job satisfaction for nurses compared to other healthcare workers after the COVID-19 pandemic. Nurs. Rep. (Pavia Italy). 13 (3), 1090–1100. https://doi.org/10.3390/nursrep13030095 (2023).
Çivilidağ, A., Durmaz, Ş. & Uslu, B. The effect of coronavirus (COVID-19) on job satisfaction, work stress and burnout of healthcare workers: A systematic review and Meta-Analysis. Iran. J. Public. Health. 53 (7), 1482–1495. https://doi.org/10.18502/ijph.v53i7.16043 (2024).
Selvaskandan, H. et al. Burnout and long COVID among the UK nephrology workforce: results from a National survey investigating the impact of COVID-19 on working lives. Clin. Kidney J. 15 (3), 517–526. https://doi.org/10.1093/ckj/sfab264 (2021).
Kim, H. et al. COVID-19 illness in relation to sleep and burnout. BMJ Nutr. Prev. Health. 4 (1), 132–139. https://doi.org/10.1136/bmjnph-2021-000228 (2021).
Galanis, P. et al. Social support mediates the relationship between COVID-19-Related burnout and booster vaccination willingness among fully vaccinated nurses. Vaccines 11 (1), 46. https://doi.org/10.3390/vaccines11010046 (2022).
Galanis, P., Vraka, I., Fragkou, D., Bilali, A. & Kaitelidou, D. Nurses’ burnout and associated risk factors during the COVID-19 pandemic: A systematic review and meta-analysis. J. Adv. Nurs. 77 (8), 3286–3302. https://doi.org/10.1111/jan.14839 (2021).
Meira-Silva, V. S. T. et al. Burnout syndrome in healthcare workers during the COVID-19 pandemic: a systematic review. Revista Brasileira De Med. Do Trabalho: Publicacao Oficial Da Associacao Nac. De Med. Do Trabalho-ANAMT. 20 (1), 122–131. https://doi.org/10.47626/1679-4435-2022-849 (2022).
Acknowledgements
The authors thank the administration of the following institutions and organizations for their support in conducting the study: Astana Medical University, University Medical Center, Ministry of healthcare of the Republic of Kazakhstan (Astana, Kazakhstan), Asfendiyarov Kazakh National Medical University, Kazakhstan’s Medical University “Kazakhstan School of Public Health” (Almaty, Kazakhstan), Kazakhstani Regional Departments of Public Health and Healthcare (Kazakhstan), I. K. Akhunbaev Kyrgyz State Medical Academy (Bishkek, Kyrgyzstan), and Bukhara state medical institute, Bukhara, Uzbekistan.
Funding
The authors received no specific funding for this article.
Author information
Authors and Affiliations
Contributions
Conceptualization and methodology: A.B. and T.S.; Formal analysis: A.B.; Investigation and data curation: N.B., G.J., A.T., R.Y., S.K., D.S.; Writing—original draft preparation: A.B.; Writing—review and editing: T.S.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval consent to participate
The study was approved by the Local Ethics Committees of “University Medical Center” Corporate Fund (extract from protocol No. 11 of December 30, 2021) and I.K. Akhunbaev Kyrgyz State Medical Academy (extract from protocol No. 13 of December 08, 2021).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Bolatov, A.K., Brimkulov, N., Jarylkasynova, G. et al. Occupational burnout among healthcare workers in Central Asia during the COVID-19 pandemic. Sci Rep 15, 12432 (2025). https://doi.org/10.1038/s41598-025-96905-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-96905-8
