
Abstract
Rising incidences of dry eye, often attributed to modern lifestyle and environmental factors, highlight the need for knowledge, attitudes, and practices (KAP) studies to inform tailored interventions. This study evaluated patients’ KAP concerning lifestyle-related dry eye at the Ophthalmology Hospital of the China Academy of Chinese Medical Sciences from July 1 to July 26, 2024. A self-designed questionnaire was used to gather demographic data and assess KAP scores, yielding 556 valid responses (98.93%). Among participants, 342 (61.51%) were female, with a mean age of 39.26 ± 13.56 years. Mean KAP scores were 7.44 ± 4.65 (knowledge), 35.20 ± 4.10 (attitude), and 35.77 ± 6.15 (practice). Mediation analysis indicated direct influences of age and familial dry eye history on knowledge, with knowledge impacting attitude, and various factors influencing practice. While patients exhibited limited knowledge, they generally held positive attitudes and engaged in proactive practices. Enhancing patient education on lifestyle factors related to dry eye is essential to boost knowledge and foster effective prevention and management strategies.
Similar content being viewed by others


Introduction
Dry eye is a prevalent chronic eye disease, and its incidence has been rising steadily in recent years. Globally, the prevalence of dry eye ranges from 5 to 50%, with higher rates observed in women than in men1,2. In China, the incidence among adults is reported to be 21–30%, with regional variations3,4. Mild to moderate dry eye is increasingly prevalent, impacting daily activities and work performance, while severe cases may result in significant visual impairment or blindness5.
This increase in incidence is attributed to advances in clinical diagnosis and treatment, as well as changes in modern lifestyle. Considerable evidence indicates that dry eye is increasingly being recognized as a lifestyle disease6,7. Unhealthy habits such as overuse of digital devices, insufficient sleep, lack of physical activity, and prolonged sedentary behavior contribute to the development of dry eye8. Furthermore, environmental pollution and lifestyle changes have exacerbated the condition in China, where the incidence of dry eye continues to rise9.
The Knowledge, Attitude, and Practices (KAP) survey serves as an important diagnostic tool, helping to evaluate a group’s understanding, beliefs, and actions regarding health issues. It is based on the principle that knowledge positively influences attitudes, which in turn shape behaviors10,11. Research shows that lifestyle interventions such as regular exercise12 and dietary habits, including the use of supplements like vitamins A, B complexes, C, E, and omega-3 fatty acids, can positively impact tear stability, tear production, and alleviate symptoms of dry eye13,14,15,16.
There is currently a lack of KAP studies focusing on lifestyle-related dry eye. This study aims to fill that gap by assessing patients’ KAP on this condition, which could help develop more effective, tailored interventions to address the specific lifestyle factors contributing to dry eye.
Methods
Study design and participants
This cross-sectional study was conducted at the Ophthalmology Hospital of the China Academy of Chinese Medical Sciences from 1 July 2024 to 26 July 2024, with patients serving as the study participants. Inclusion Criteria: (1) Patients diagnosed with dry eye by an experienced ophthalmologist, following the diagnostic criteria outlined in the Chinese Clinical Diagnosis and Treatment Guidelines for Dry Eye edited by Liu Zuguo (China Science and Technology Press, 2023); (2) Aged 18 to 80 years, inclusive, regardless of gender; (3) Capable of understanding and voluntarily participating in the survey; (4) Willing and able to cooperate with eye examinations. Those disagree with this study were excluded. After a detailed study protocol was finalized (before participants are recruited), we submit an ethics application to the Ethics Committee. This study protocol was approved by the Ethics Committee of the Ophthalmology Hospital of the China Academy of Chinese Medical Sciences (YKEC-KT-2022-012-P004), and all participants provided written informed consent which was issued along with the first page of the questionnaire.
Questionnaire design
The questionnaire was developed based on relevant guidelines and expert consensus, specifically drawing from the Chinese Dry Eye Expert Consensus: Lifestyle-Related Dry Eye (2022)17 and the Chinese Clinical Diagnosis and Treatment Guidelines for Dry Eye (2023), edited by Liu Zuguo (China Science and Technology Press). After drafting the initial version, the questionnaire was revised according to expert feedback and underwent a pilot test with 44 participants, resulting in a Cronbach’s α of 0.916, indicating strong internal consistency.
The final questionnaire, written in Chinese (an English translation is provided in the online Appendix), comprised five dimensions with a total of 51 items. These included 14 items for basic demographic information, 8 items for the knowledge dimension (with item 3 containing two sub-items), 9 items for the attitude dimension, and 10 items for the practice dimension. For statistical analysis, scores were assigned based on the number of items and the options selected.
In the knowledge dimension, responses were scored as follows: “Very knowledgeable” = 2 points, “Heard of it” = 1 point, and “Unfamiliar” = 0 points, with a possible total score ranging from 0 to 18 points. Both the attitude and practice dimensions employed a five-point Likert scale, ranging from very positive (5 points) to very negative (1 point). In the attitude dimension, items 2–9 were scored from a = 5 to e = 1, while item 1 was reverse-scored, with a = 1 to e = 5, allowing for a total score range of 9 to 45 points. For the practice dimension, all 10 items were scored from a = 5 to e = 1, yielding a total score range of 10 to 50 points.
After participants completed the questionnaire, the average scores were categorized as follows: for the knowledge dimension, 0–9 points indicated insufficient knowledge, 10–12 points indicated moderate knowledge, and 13–18 points indicated sufficient knowledge. In the attitude dimension, scores of 9–22 points indicated a negative attitude, 23–31 points indicated a neutral attitude, and 32–45 points indicated a positive attitude. For the practice dimension, scores of 10–25 points indicated negative practice, 26–35 points indicated moderate practice, and 36–50 points indicated positive practice. Scores exceeding 70% of the maximum in each section indicated adequate knowledge, a positive attitude, and proactive practices18.
Questionnaire quality control
The questionnaire data were collected through electronic questionnaires, using WeChat QR code scanning in both WeChat groups and clinics. Prior to the survey, research assistants received training on the study’s objectives and the survey method. Patients were informed about the study’s purpose, potential risks, and the Ethics Review Committee’s approval before participating. Participation was entirely voluntary, and after obtaining patients’ consent, they were assured that any personal privacy information would be strictly confidential and not disclosed. Research assistants were instructed not to provide any mandatory guidance during the questionnaire process, ensuring that patients answered truthfully based on their own circumstances.
To maintain quality control during the survey, a quality control manager ensured that all personnel followed standard operating procedures and monitored the quality control process throughout the study. Additionally, a data manager was responsible for data entry, editing, and management. The Cronbach’s α coefficient for the overall valid questionnaire was 0.875, indicating good internal consistency further.
Sample size
Sample size was calculated using the formula for cross-sectional studies: α = 0.05,\(\:\:\text{n}={\left(\frac{{Z}_{1-\alpha\:/2}}{\delta\:}\right)}^{2}\times\:p\times\:\left(1-p\right)\) where \(\:{Z}_{1-\alpha\:/2}\)=1.96 when α = 0.05, the assumed degree of variability of p=0.5 maximizes the required sample size, and δ is admissible error (which was 5% here). The theoretical sample size of 480 included an additional 20% to account for potential dropouts.
Statistical analysis
Descriptive analysis was performed on the demographic data and KAP scores, with normally distributed variables presented as mean ± SD, and categorical data as n (%). For KAP score comparisons, continuous variables were tested for normality. If normally distributed, mean ± SD and t-tests were used; if not, the median (range) and Mann-Whitney U tests were applied. ANOVA was used for comparisons across three or more groups when applicable. Pearson correlation analysis assessed the relationships between the three KAP dimensions. Path analysis explored the mediation effects between KAP and demographic characteristics. A 1st round fitting for the path analysis model: Inclusion of all variables with differences and continuous variables. The 2nd round fitting for the path analysis model (adjustement): Removal of non-significant paths and MI adjustment. A two-sided P-value less than 0.05 was considered statistically significant.
Results
Demographic characteristics
Among the 562 enrolled participants, 556 provided valid responses after excluding incomplete or rapid submissions, yielding a validity rate of 98.93%. Of the participants, 342 (61.51%) were female, with a mean age of 39.26 ± 13.56 years and a mean BMI of 24.14 ± 5.05 kg/m². A total of 334 participants (60.07%) held a college or bachelor’s degree, 212 (38.13%) had relatives or friends with dry eye, 143 (25.72%) reported other eye conditions, 157 (28.24%) had sleep disorders, 147 (26.44%) had makeup habits, and 264 (47.48%) engaged in regular physical exercise. The mean scores for knowledge, attitudes, and practices were 7.44 ± 4.65, 35.20 ± 4.10, and 35.77 ± 6.15, respectively. Significant differences in knowledge scores were observed among participants with varying levels of education (P < 0.001), employment status (P < 0.001), household monthly per capita income (P = 0.017), presence of dry eye in relatives or friends (P < 0.001), and makeup habits (P = 0.015). Differences in attitude scores were significant for participants with different BMI (P = 0.045), education levels (P < 0.001), employment status (P < 0.001), household monthly per capita income (P = 0.005), smoking status (P = 0.003), and dry eye in relatives or friends (P = 0.035). In terms of practice scores, significant differences were found based on gender (P < 0.001), household monthly per capita income (P = 0.016), smoking status (P = 0.002), alcohol consumption (P < 0.001), dry eye status in relatives or friends (P = 0.027), and engagement in regular physical exercise (P < 0.001) (Table 1).
Knowledge, attitude, and practice
The distribution of knowledge dimensions shown that the three questions with the highest number of participants choosing the “Not Clear” option were “Dry eye related to diet: This mainly involves dry eye caused by inadequate nutritional intake, high-fat diets, and excessive alcohol consumption.” (K3.2) with 37.59%, “As lifestyle-related dry eye is often a mixed type, patients should actively seek information from doctors about the clinical characteristics of their dry eye condition and consider a comprehensive treatment plan that includes both medication and non-medication treatments.” (K4) with 35.61%, and “Non-pharmacological treatments mainly include physical therapies, the use of moisture chamber glasses, punctual plugs, intense pulsed light therapy, and thermal pulsation therapy.” (K6) with 35.43% (Table S1).
When it comes to related attitudes, 10.25% strongly agreed or agreed that dry eye is not a major concern and does not require much attention (A1), while another 18.53% were neutral. Meanwhile, 44.61% strongly agreed or agreed that adequate fluid intake is not directly related to dry eye (A7), also another 29.68% were neutral (Table S2).
Responses to the practice dimension showed that 46.04% strongly agreed or agreed that they rarely take the initiative to adjust their eye habits even when they feel uncomfortable (P3). On the other hand, 17.63% disagreed or strongly disagreed that they would take regular eye breaks and massages (P4), and 19.97% disagreed or strongly disagreed that they would try to follow the Mediterranean dietary pattern (P7) (Table S3).
Correlations between KAP
Correlation analysis revealed significant positive correlations between knowledge and attitude (r = 0.255, P < 0.001) and between knowledge and practice (r = 0.333, P < 0.001). Additionally, a significant correlation was observed between attitude and practice (r = 0.351, P < 0.001) (Table 2).
Interactions among KAP and demographic characteristics
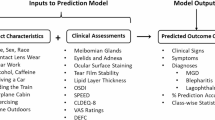
Path analysis was performed and the coefficients for each path were shown in Table S4. The fitting index of CMIN/DF = 4.013, RMSEA = 0.074; IFI = 0.875; TLI = 0.817; CFI = 0.873, signifying that the data satisfactorily fit the structural model (Table S5). Moreover, the mediation analysis based on the path analysis revealed that age (β = -0.172, P = 0.010) and the presence of dry eye in relatives or friends (β = -0.228, P = 0.009) directly influenced knowledge. Attitude was directly influenced by knowledge (β = 0.233, P = 0.007), smoking (β = 0.095, P = 0.027), and education (β = 0.248, P = 0.014). Practice was directly influenced by knowledge (β = 0.260, P = 0.014), attitude (β = 0.267, P = 0.004), regular physical exercise (β = 0.173, P = 0.012), and gender (β = 0.124, P = 0.009). Additionally, age (β = -0.040, P = 0.005) and the presence of dry eye in relatives or friends (β = 0.053, P = 0.006) indirectly influenced attitude. Practice was indirectly influenced by knowledge (β = 0.062, P = 0.003), age (β = -0.055, P = 0.005), the presence of dry eye in relatives or friends (β = -0.073, P = 0.007), smoking (β = 0.025, P = 0.015), and education (β = 0.066, P = 0.003) (Table 3 and Fig. 1).

Path analysis model depicting the relationships between demographic characteristics and knowledge, attitudes, and practices (KAP) regarding lifestyle-related dry eye. The structural equation modeling (SEM) results illustrate the direct and indirect relationships between demographic variables, knowledge, attitudes, and practices. Solid arrows indicate significant direct paths, with standardized path coefficients displayed along each path. Knowledge was directly influenced by age and the presence of dry eye in relatives or friends, suggesting that younger individuals and those with prior exposure to the condition exhibited greater awareness. Attitude was shaped by knowledge, education level, and smoking status, with higher education contributing to more positive attitudes and smoking associated with less favorable perceptions. Practice was directly influenced by knowledge and attitude, reinforcing the theoretical KAP model, where awareness and perception facilitate behavioral change. Regular physical exercise and gender were also significant predictors of practice, with physically active individuals and females more likely to adopt protective behaviors. Smoking had a direct negative effect on both attitude and practice, highlighting its detrimental impact on health-related behaviors. Indirect pathways were also observed, as age and family history of dry eye influenced practice through their effects on knowledge and attitude. The error terms (e1–e9) represent unexplained variance within the model. The model fit indices (CMIN/DF, RMSEA, IFI, TLI, and CFI) indicate an acceptable fit, supporting the robustness of the proposed relationships.
Discussion
Patients demonstrated inadequate knowledge, yet exhibited generally positive attitudes and proactive practices regarding lifestyle-related dry eye. Clinically, it is recommended to enhance patient education on lifestyle-related risk factors for dry eye, focusing on bridging the knowledge gaps to further improve preventive behaviors.
The main findings of this study reveal that while patients generally displayed positive attitudes and proactive practices toward lifestyle-related dry eye, their overall knowledge levels were insufficient. This imbalance in KAP results is consistent with previous studies, which suggest that a lack of adequate knowledge prevents patients from correctly associating their symptoms with dry eye before a formal diagnosis19. Patients have expressed the need for information presented in clear, accessible language to better understand their condition. To bridge the knowledge gap and enhance patient adherence, targeted educational interventions should include structured patient education sessions, digital health tools such as mobile reminders, and interactive workshops. These approaches can reinforce key information on preventive and therapeutic measures, facilitating sustained behavioral change. Moreover, the mediation analysis provides deeper insights into the complex interactions among demographic characteristics and KAP dimensions. Knowledge was influenced by both individual factors and external exposures, highlighting the role of prior awareness and access to health-related information. Attitude was directly shaped by knowledge, education level, and health-related behaviors, reinforcing the idea that higher awareness contributes to more positive perceptions. Smoking status, in particular, was associated with less favorable attitudes, suggesting a potential barrier to preventive engagement. Practice was strongly associated with both knowledge and attitude, supporting the theoretical KAP model, where higher awareness and positive perceptions facilitate behavioral change. Additionally, lifestyle habits such as regular physical activity played a key role in proactive practices, indicating that individuals who engage in overall healthier routines are more likely to adopt protective behaviors for dry eye management. Gender differences were also observed, with certain groups demonstrating a greater inclination toward preventive behaviors, which is consistent with previous research on health-seeking behaviors. Indirect pathways further emphasized the influence of background characteristics on KAP. Younger individuals exhibited higher knowledge levels, which in turn contributed to more favorable attitudes and practices. Having relatives or friends with dry eye was associated with increased awareness, but this did not necessarily translate into stronger attitudes or adherence to recommended practices, suggesting that exposure to the condition alone may not be sufficient to drive behavior change.
The knowledge distribution shows a clear deficiency in patient understanding, especially regarding the role of diet and non-pharmacological treatments for dry eye. Notably, over one-third of participants were unclear about the impact of diet on dry eye and the role of non-pharmacological treatments. These findings align with studies where insufficient patient knowledge was similarly observed, particularly in areas related to lifestyle modifications20,21. To address these gaps, educational interventions should incorporate targeted materials such as patient-friendly brochures, digital infographics, and video tutorials explaining the role of nutrition, hydration, and alternative therapies in dry eye management. Additionally, structured educational workshops within ophthalmology clinics could provide interactive learning opportunities, allowing patients to ask questions and receive tailored guidance from healthcare professionals. Tailored interventions that focus on raising awareness among groups with lower educational attainment or less access to healthcare, such as rural residents and those with lower incomes, could be particularly impactful, as supported by findings from other studies22,23,24.
Regarding attitudes, the majority of participants held positive views about the importance of maintaining good lifestyle habits to manage dry eye. However, nearly half of the participants were neutral or uncertain about the relationship between fluid intake and dry eye. To address this, clinical practice should incorporate hydration education as part of routine ophthalmic consultations. Brief counseling sessions could emphasize the importance of fluid intake for tear production, supported by visual aids or mobile health applications that provide daily hydration reminders. Healthcare providers should deliver clear messages regarding the link between hydration and eye health, reinforced through visual aids or mobile health reminders25,26. Additionally, integrating smoking cessation advice into ophthalmology visits may help improve patient attitudes toward lifestyle-related risk factors, as smoking was identified as a negative predictor of attitude and practice in this study.
In terms of practices, although participants generally reported proactive behaviors, some areas still require improvement, particularly in taking regular eye breaks and following dietary recommendations. Over half of the respondents did not regularly take action to adjust their eye habits or follow dietary patterns, such as the Mediterranean diet. This finding is consistent with other research showing that even when patients have knowledge or positive attitudes, translating this into effective practice remains challenging27,28. To promote sustainable behavioral change, structured reminder systems such as smartphone applications sending notifications for screen breaks, eye massages, and hydration tracking could be implemented. Clinics could also distribute simple lifestyle checklists that encourage patients to self-monitor their adherence to protective habits, reinforcing positive behaviors. For individuals with identified risk factors like smoking or alcohol consumption, integrating these into broader wellness programs that address both dry eye and other health conditions may yield better adherence outcomes29,30.
The correlation analyses showed significant relationships between all three KAP dimensions, with stronger correlations observed between knowledge and practice, and attitude and practice. This finding aligns with previous research showing that while knowledge is a precursor to attitude development, practice is most influenced by both knowledge and attitudes31,32.
Both the correlation analysis and SEM results showed that smoking had a direct impact on patient attitudes and practices. Patients who smoked tended to have more negative attitudes and were less likely to engage in positive practices related to dry eye management. These findings are consistent with prior research that links smoking to poorer health behaviors and eye health outcomes33,34. Gender differences were also evident in both the correlation and SEM analyses, with females exhibiting more proactive practices compared to males. This gender disparity may be partly due to differences in health-seeking behaviors, as women tend to be more proactive in managing health-related issues35,36.
Regular physical exercise had a strong direct effect on practice, as demonstrated by both the correlation and SEM analyses. Participants who engaged in regular exercise were more likely to adopt positive practices related to managing dry eye. This finding aligns with existing literature that shows a correlation between physical activity and improved adherence to healthy behaviors37,38. Given this, ophthalmology clinics could promote exercise-based interventions, such as including exercise recommendations in patient education materials or collaborating with fitness programs to highlight the benefits of physical activity for eye health. While income and education levels showed some influence on knowledge and attitudes, these factors did not significantly impact practice in the SEM model. This discrepancy might suggest that even though higher income and education contribute to better knowledge and more positive attitudes, they do not automatically translate into action. This could be due to various barriers, such as a lack of time, access to resources, or the presence of other competing health priorities39,40. To overcome these barriers, future interventions should focus on integrating eye health recommendations into daily routines through simple, practical strategies that accommodate different socioeconomic backgrounds.
This study has several limitations. First, the cross-sectional design prevents the establishment of causal relationships between knowledge, attitudes, and practices and the incidence or severity of dry eye. While associations were identified, longitudinal or interventional studies are needed to determine whether improving knowledge and attitudes leads to sustained changes in preventive behaviors and clinical outcomes. Second, the use of self-reported questionnaires may introduce recall bias or social desirability bias, potentially affecting the accuracy of responses. Third, the study was conducted at a single ophthalmology hospital in China, which may limit the generalizability of the findings to broader populations. While the sample size was sufficient for statistical analysis, the study setting may not fully represent patients with different healthcare access, socioeconomic backgrounds, or cultural perspectives. Future research should consider multi-center studies or nationally representative samples to enhance the applicability of the findings across diverse populations.
In conclusion, patients demonstrated inadequate knowledge but exhibited generally positive attitudes and proactive practices regarding lifestyle-related dry eye. To improve patient outcomes, healthcare providers should implement structured education programs, integrate lifestyle counseling into routine ophthalmic care, and leverage digital health tools to enhance patient engagement and adherence. Educational interventions should be tailored to different demographic groups, particularly those with lower knowledge levels, to ensure accessibility and effectiveness.
Data availability
All data generated or analyzed during this study are included in this article and supplementary information files.
References
de Paiva, C. S. Effects of aging in dry eye. Int. Ophthalmol. Clin. 57, 47–64 (2017).
Stapleton, F. et al. TFOS DEWS II epidemiology report. Ocul Surf. 15, 334–365 (2017).
Du, J. & Liang, Q. Risk factors of dry eye. Int. Ophthalmol. Overv. 42, 189–193 (2018).
Liu, Z. G. [Emphasis on standardization and refinement in the diagnosis and treatment of dry eye]. Zhonghua Yan Ke Za Zhi. 53, 641–644 (2017).
Clayton, J. A. Dry eye. N Engl. J. Med. 378, 2212–2223 (2018).
Hanyuda, A. et al. Relationship between unhealthy sleep status and dry eye symptoms in a Japanese population: the JPHC-NEXT study. Ocul Surf. 21, 306–312 (2021).
Kojima, T., Dogru, M., Kawashima, M., Nakamura, S. & Tsubota, K. Advances in the diagnosis and treatment of dry eye. Prog Retin Eye Res. 100842 (2020).
Hanyuda, A. et al. Physical inactivity, prolonged sedentary behaviors, and use of visual display terminals as potential risk factors for dry eye disease: JPHC-NEXT study. Ocul Surf. 18, 56–63 (2020).
Wang, N. et al. Questionnaire analysis on incidence and risk factors of dry eye in children from a myopia outpatient clinic. Front. Med. (Lausanne). 9, 846709 (2022).
Basheikh, A., Alattas, A., Alshareef, R. & Bamahfouz, A. Dermatologists’ knowledge and attitudes toward dry eye disease, refractive surgery, and contact lenses when prescribing isotretinoin in Saudi Arabia. Clin. Ophthalmol. 14, 4519–4522 (2020).
Kharel Sitaula, R., Khatri, A. & Knowledge Attitude and practice of computer vision syndrome among medical students and its impact on ocular morbidity. J. Nepal. Health Res. Counc. 16, 291–296 (2018).
Navarro-Lopez, S., Moya-Ramón, M., Gallar, J., Carracedo, G. & Aracil-Marco, A. Effects of physical activity/exercise on tear film characteristics and dry eye associated symptoms: A literature review. Cont. Lens Anterior Eye. 46, 101854 (2023).
Asbell, P. A., Maguire, M. G., Peskin, E., Bunya, V. Y. & Kuklinski, E. J. Dry eye assessment and management (DREAM©) study: Study design and baseline characteristics. Contemp. Clin. Trials. 71, 70–79 (2018).
Huang, J. Y., Yeh, P. T. & Hou, Y. C. A randomized, double-blind, placebo-controlled study of oral antioxidant supplement therapy in patients with dry eye syndrome. Clin. Ophthalmol. 10, 813–820 (2016).
Jackson, M. A., Burrell, K., Gaddie, I. B. & Richardson, S. D. Efficacy of a new prescription-only medical food supplement in alleviating signs and symptoms of dry eye, with or without concomitant cyclosporine A. Clin. Ophthalmol. 5, 1201–1206 (2011).
Ziemanski, J. F., Wolters, L. R., Jones-Jordan, L., Nichols, J. J. & Nichols, K. K. Relation between dietary essential fatty acid intake and dry eye disease and meibomian gland dysfunction in postmenopausal women. Am. J. Ophthalmol. 189, 29–40 (2018).
[Chinese expert consensus on. Dry eye: Lifestyle-related dry eye (2022)]. Zhonghua Yan Ke Za Zhi. 58, 573–583 (2022).
Lee, F. & Suryohusodo, A. A. Knowledge, attitude, and practice assessment toward COVID-19 among communities in East Nusa Tenggara, Indonesia: A cross-sectional study. Front. Public. Health. 10, 957630 (2022).
Caffery, B. et al. Patient perspectives on dry eye disease and chronic ocular surface pain: Insights from a virtual community-moderated dialogue. Eur. J. Ophthalmol. 11206721221125263 (2022).
Lutala, P. & Muula, A. Brief behaviour change counselling in non-communicable diseases in Mangochi, Southern Malawi: A hypothetical acceptability study. Pilot Feasibility Stud. 8, 69 (2022).
Zeng, X. et al. A randomized controlled clinical study on Zuo’s acupuncture treatment for prediabetes. Med. (Baltim). 101. e28824 (2022).
Huang, R. et al. Dry eye syndrome: Comprehensive etiologies and recent clinical trials. Int. Ophthalmol. 42, 3253–3272 (2022).
Messmer, E. M. et al. Management of inflammation in dry eye disease: Recommendations from a European panel of experts. Eur. J. Ophthalmol. 33, 1294–1307 (2023).
Sheppard, J., Shen Lee, B. & Periman, L. M. Dry eye disease: Identification and therapeutic strategies for primary care clinicians and clinical specialists. Ann. Med. 55, 241–252 (2023).
Nagino, K. et al. Smartphone App-based and paper-based patient-reported outcomes using a disease-specific questionnaire for dry eye disease: randomized crossover equivalence study. J. Med. Internet Res. 25, e42638 (2023).
Nagino, K. et al. Diagnostic ability of a smartphone app for dry eye disease: Protocol for a multicenter, open-label, prospective, and cross-sectional study. JMIR Res. Protoc. 12, e45218 (2023).
Boydell, K. M. & Croguennec, J. A. Creative approach to knowledge translation: The use of short animated film to share stories of refugees and mental health. Int. J. Environ. Res. Public. Health 19. (2022).
Mtuy, T. B., Mepukori, J., Lankoi, J. & Lees, S. Empowering Maasai women behind the camera: Photovoice as a tool for trachoma control. Res. Involv. Engagem. 7, 51 (2021).
Mittal, R., Patel, S. & Galor, A. Alternative therapies for dry eye disease. Curr. Opin. Ophthalmol. 32, 348–361 (2021).
Mohamed, H. B., El-Hamid, A. & Fathalla, B. N. Fouad E. A. Current trends in pharmaceutical treatment of dry eye disease: A review. Eur. J. Pharm. Sci. 175, 106206 (2022).
Khalid, A. et al. Promoting health literacy about cancer screening among Muslim immigrants in canada: Perspectives of imams on the role they can play in community. J. Prim. Care Community Health. 13, 21501319211063051 (2022).
Liao, L., Feng, H., Jiao, J., Zhao, Y. & Ning, H. Nursing assistants’ knowledge, attitudes and training needs regarding urinary incontinence in nursing homes: A mixed-methods study. BMC Geriatr. 23, 39 (2023).
Heckman, C. J. et al. Cigarette relighting: A series of pilot studies investigating a common yet understudied smoking behavior. Int. J. Environ. Res. Public. Health 18. (2021).
Li, X. et al. Comparison of cytotoxicity effects induced by four different types of nanoparticles in human corneal and conjunctival epithelial cells. Sci. Rep. 12, 155 (2022).
Hasemann, L. et al. Effectiveness of a multi-component community-based care approach for older people at risk of care dependency - results of a prospective quasi-experimental study. BMC Geriatr. 22, 348 (2022).
Tiguman, G. M. B., Silva, M. T. & Galvão, T. F. Health services utilization in the Brazilian Amazon: Panel of two cross-sectional studies. Rev. Saude Publica. 56, 2 (2022).
Ward, L. J. et al. Resistance training decreases plasma levels of adipokines in postmenopausal women. Sci. Rep. 10, 19837 (2020).
Yusefi, A. R. et al. Health literacy and health promoting behaviors among inpatient women during COVID-19 pandemic. BMC Womens Health. 22, 77 (2022).
Millett, G. A. New pathogen, same disparities: Why COVID-19 and HIV remain prevalent in U.S. Communities of colour and implications for ending the HIV epidemic. J. Int. AIDS Soc. 23, e25639 (2020).
Silva Rocha, E. D. et al. On usage of artificial intelligence for predicting mortality during and post-pregnancy: A systematic review of literature. BMC Med. Inf. Decis. Mak. 22, 334 (2022).
Acknowledgements
None.
Funding
This study was supported by Central High-Level Traditional Chinese Medicine Hospital Project of eye Hospital China Academy of Chinese medical science(GSP5-49).
Author information
Authors and Affiliations
Contributions
Ke Song, Shanshan Ye, Shujiao Li, Ningling Wu and Zefeng Kang carried out the studies, participated in collecting data, and drafted the manuscript. Ke Song and Shanshan Ye performed the statistical analysis and participated in its design. Ke Song and Zefeng Kang participated in acquisition, analysis, or interpretation of data and draft the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This work has been carried out in accordance with the Declaration of Helsinki (2000) of the World Medical Association. This study was approved by the Ethics Committee of the Ophthalmology Hospital of the China Academy of Chinese Medical Sciences (YKEC-KT-2022-012-P004), and all participants provided written informed consent.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Song, K., Ye, S., Li, S. et al. Patients’ knowledge, attitudes, and practices regarding lifestyle related dry eye. Sci Rep 15, 12050 (2025). https://doi.org/10.1038/s41598-025-97290-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-97290-y
