
Abstract
Stool specimen is commonly used for mycobacterial culture to provide critical microbiological evidence for diagnosing tuberculosis (TB) in pediatric patients, especially when obtaining sputum specimens is challenging. However, the utilization of stool specimens for mycobacterial culture continues to face significant challenges in clinical practice, mainly owing to the relatively low diagnostic sensitivity and the frequent contamination by intestinal flora during specimen processing. This study evaluated the effectiveness of power ultrasound (PU) method in improving the recovery of Mycobacterium tuberculosis (M. TB) from stool specimens collected from children suspected of pulmonary tuberculosis (PTB). A total of 252 stool specimens were collected, and each specimen was subsequently divided into approximately three equal groups. One stool specimen was subjected to direct acid-fast bacilli (AFB) smear microscopy, while the other two stool specimens were processed using different decontamination methods(NaOH-NALC method vs. PU method). Out of the 252 specimens, positive cultures were observed in 14 (5.56%) stool specimens treated with the NaOH-NALC method, including M. TB (n = 11, 4.37%) and non-tuberculous mycobacteria (NTM; n = 3, 1.19%). Similarly, among the stool specimens subjected to the PU method, culture positivity was found in 36 (14.28%), comprising of M. TB (n = 24, 9.52%) and NTM (n = 12, 4.76%). The statistical analysis revealed a significant difference in the isolation rate of M. TB and NTM between the two methods (P<0.001). Furthermore, the contamination rate of stool treated with the PU method (14.28%) is significantly lower than that of the NALC-NaOH method (22.62%). In conclusion, our findings indicate that the PU method is a rapid and effective decontamination method for stool in children, improving the detection of active TB among pediatric populations when compared to the NALC-NaOH method.
Similar content being viewed by others



Introduction
Tuberculosis (TB) continues to rank among the top 10 causes of global mortality and was the leading cause of death attributed to a single infectious disease prior to the COVID-19 pandemic. According to the Global tuberculosis report 2023, it was estimated that there were 1.27 million new cases of pediatric TB and approximately 208,000 deaths caused by childhood TB in 20221. Timely and accurate diagnosis of pulmonary tuberculosis (PTB) in children is essential for reducing its prevalence and transmission. However, this task is challenging due to the fact that children often present with paucibacillary disease and may have difficulty producing sputum for microbiological confirmation of Mycobacterium tuberculosis (M. TB)2. Therefore, alternative specimens such as bronchoalveolar lavage fluid, gastric lavage fluid, or induced sputum are necessary. However, these specimens have several drawbacks including invasiveness, high cost, and the requirement for specialized equipment that may not be readily available in resource-limited settings3,4.
The findings of various studies indicate that M. TB can be transported from the lungs to the oropharynx and subsequently swallowed. This transport occurs via mucociliary clearance, a physiological process where cilia in the airways move mucus containing particles and pathogens toward the throat, thereby maintaining airway cleanliness independently of coughing5. Additionally, M. TB is an acid-fast bacilli (AFB) that effectively withstands the corrosive effects of gastric acid, enabling it to pass through the digestive tract and be excreted in stool2,3,4,6,7,8,9. Consequently, M. TB can be detected in stool by mycobacterial culture. Stool mycobacterial culture may serve as an alternative diagnostic method for pediatric PTB in situations where obtaining sputum specimens from children is challenging2,3,4,7. Moreover, considering the limited diagnostic options available for confirming tuberculosis in children residing in high-burden settings, stool culture remains a crucial adjunctive measure in PTB diagnosis4. The primary advantage of stool as an experimental specimen lies in its non-invasive nature and ease of collection. However, the limited sensitivity and significant contamination issues associated with stool mycobacterial culture restrict the utility of stool specimens due to intestinal flora. Therefore, prior to performing mycobacterial culture, it is necessary to digest and decontaminate stool specimens. The N-Acetyl-L-Cysteine (NALC)-sodium hydroxide (NaOH) method is widely used in stool decontamination; however, it may not be the optimal procedure due to several limitations10. In recent years, numerous strategies have been employed to enhance the decontamination of stool specimens for Mycobacterium isolation; however, none has achieved significant breakthroughs11,12,13. Consequently, there is an imperative for the development of a novel decontamination procedure specifically tailored to stool specimens.
Power ultrasound (PU, 20 to 100 kHz) has been widely used in biomedical research due to its bactericidal properties14,15. However, the susceptibility of different pathogens to PU varies, indicating pathogen-specific efficacy of PU in causing destruction16,17,18,19. This finding suggests the potential application of PU as a decontamination procedure in mycobacterial culture10. Recently, our team has demonstrated the applicability of the PU method in stool mycobacterial culture for suspected cases of PTB. Compared to the NaOH-NALC method, this method effectively eliminates various fast-growing microbiological agents in stool and significantly enhances the isolation rate of M. TB20. However, there is currently no existing report on the diagnostic efficacy of the PU method specifically for stool mycobacterial culture in pediatric patients. Therefore, in this study, we applied PU technology to decontaminate stool specimens obtained from pediatric patients and assessed its efficacy. Furthermore, a comparative analysis was conducted to evaluate its performance when compared with the NALC-NaOH decontamination method.
Materials and methods
Subjects
The prospective study was conducted at the Katharine Hsu International Research Center of Human Infectious Diseases, Shandong Public Health Clinical Center, Shandong University. From April 2023 to March 2024, children aged 14 years or younger suspected of PTB were consecutively enrolled in the study. Children were eligible if they presented with at least one of the following criteria: (i) a persistent cough lasting for two weeks or longer; (ii) an unexplained fever; (iii) inadequate growth or weight loss over the preceding three months; (iv) exposure to a confirmed TB source case within the past 12 months; (v) positive results on tuberculin skin test (TST) or Interferon Gamma Release Assay (IGRAs); (vi) a chest X-ray (CXR) suggestive of TB as assessed by the attending clinician. Exclusion criteria comprised the absence of assent from guardians, lack of stool specimen, sole diagnosis of extrapulmonary tuberculosis (EPTB), or prior administration of anti-TB therapy. The attending clinicians utilized composite clinical reference standards (CCRSs) to diagnose PTB, EPTB, and nontuberculous mycobacterial (NTM) disease among the enrolled patients. If these criteria were not met, alternative diagnoses would be considered. Specifically, for this study, CCRSs included “WS 288–2017 Diagnosis of Pulmonary Tuberculosis21” for diagnosing both PTB and EPTB, as well as “Guidelines for the Diagnosis and Treatment of Nontuberculous Mycobacterial Disease (2020 Edition22)” for diagnosing NTM disease.
Stool specimens collection
Stool specimens were collected in accordance with practical manual of processing stool specimens for the diagnosis of childhood TB (2022)23. Subsequently, each stool specimen was divided into approximately three equal portions. One stool specimen was subjected to direct AFB smear microscopy, while the other two stool specimens were processed using different decontamination methods (NaOH-NALC method vs. PU method). Stool mycobacterial culture was conducted using the MGIT 960 system (Becton Dickinson, Franklin Lakes, NJ, USA). The isolates were identified through Matrix-Assisted Laser Desorption/ Ionization Time of Flight Mass Spectrometry (Bruker Daltonics, Bremen, Germany) or sequencing of the 16 S rRNA gene.
Direct AFB smear microscopy (Auramine O method)
Briefly, 0.5 g of stool specimen was suspended in 10 mL of sterile phosphate buffer (PBS; pH 6.8) and homogenized using vortexing, followed by settling for 30 min24. A drop of supernatant was placed on a microscope slide for smearing, followed by staining using the Auramine O method. Subsequently, it was examined under a microscope.
Digestion and decontamination methods (DDMs)
NaOH-NALC method23: (a) 0.5 g of stool specimen was suspended in 10 mL of sterile PBS and homogenized using vortexing, followed by settling for 30 min. (b) The resulting supernatant (2 mL) was mixed with an equal volume of a NaOH-NALC solution, which consisted of a 1:1 mixture of 4% NaOH and 2.9% sodium citrate, supplemented with NALC. Subsequently, the mixture (a final concentration of 1% NaOH) was vortexed for 30 s and then incubated at room temperature for a duration of 15 min. (c) After incubation, the mixture was subjected to centrifugation at 3000×g for 15 min following the addition of 40 mL sterile PBS. (d) The supernatant was discarded, and the pellet was resuspended in 200 µL of sterile PBS using a vortex mixer for brief homogenization lasting 5 s. (e) A 500 µL aliquot of the resuspended specimen was utilized for MGIT culture, while a single droplet was employed for AFB smear microscopy using Auramine O staining.
PU method: (a) 0.5 g of stool specimen was suspended in 10 mL of sterile PBS within a 15 mL BD Falcon centrifuge tube. The centrifuge tube was subsequently securely fastened onto a specialized tube rack and positioned inside the non-contact PU meter (Fig. 1A). It underwent treatment with an input power of 100 W (ultrasonic frequency, 20 kHz; power density, 20 W/mL; power intensities, 7.96 W/cm2) and sonication for a duration of 1 min. After sonication, the tube was promptly removed from the PU meter and allowed to settle for a duration of 10 min. (b) 2 mL of the supernatant was combined with an equal volume of 2% NaOH in a 50 mL BD Falcon centrifuge tube. The mixture was subsequently subjected to PU meter treatment (input power: 19 W; ultrasonic frequency: 20 kHz; power density: 4.75 W/mL; power intensities: 1.51 W/cm2 ; duration: 1 min), followed by incubation at room temperature for a period of 10 min. The subsequent steps of the procedure followed the protocol outlined in (c) to (e) of the NaOH-NALC method.(Fig. 1B).

The non-contact PU meter and The PU method procedure. (All the photographs were captured directly by our team using a HUAWEI Mate 60 Pro at the Katharine Hsu International Research Center for Human Infectious Diseases and processed using WPS Office software.)
Statistical analysis
The statistical analysis was conducted using IBM SPSS Statistics (version 26.0, Armonk, NY, USA). Continuous variables were summarized using the median (interquartile range, IQR) and compared using the Wilcoxon signed-rank test. The effect size was quantified by the Hodges-Lehmann median difference (HLδ). Categorical variables were presented as frequencies (percentages) and compared using McNemar’s test. Cohen’s g (g) was incorporated to provide a precise measure of the effect size for differences between paired categorical variables. Sensitivity was calculated against CCRSs, and the contamination rate of each method was reported. McNemar’s test was used to compare the sensitivity and contamination rates between the two methods. Agreement between the NaOH-NALC and PU methods was assessed by calculating the Kappa value. The significance level was set at 0.05 for the P value.
Results
Baseline characteristics
A total of 252 children (median age: 11.33 years, IQR: 6.58; boys: 44.05%, 111/252) were recruited for this study. Among them, 57 (22.62%) were diagnosed with PTB (including PTB with EPTB in 34 cases), while NTM diseases were diagnosed in 22 children (8.73%). The remaining 173 children (68.65%) received an alternative diagnosis. Stool specimens were collected from all participants for treatment, as described in Fig. 1. The recruitment process and characteristics of the cohort are summarized in Table 1; Fig. 2.
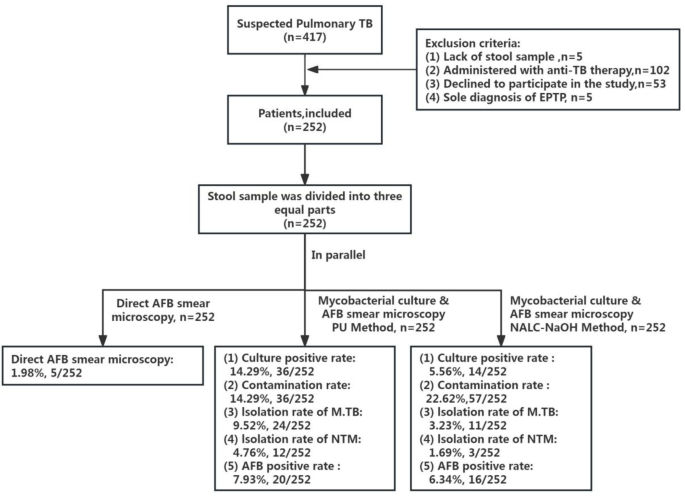
Patient selection.
Diagnostic efficacy (NaOH-NALC vs. PU methods)
Out of the 252 specimens, positive cultures were obtained from 14 (5.56%) stool specimens decontaminated using the NaOH-NALC method, comprising 11 cases of M. TB (4.37%) and 3 cases of NTM (1.19%). In contrast, the PU method yielded positive cultures for 36 (14.28%) stool specimens, including 24 cases of M. TB (9.52%) and 12 cases of NTM (4.76%). Consequently, compared to the NaOH-NALC method, the PU method detected an additional 13 cases of M. TB and 9 cases of NTM (Fig. 3). The statistical analysis revealed a significant difference in the frequency of culture-positive results for M. TB (P < 0.001, g = 0.052) and NTM (P < 0.001, g = 0.036) across the different method groups. The agreement between the NaOH-NALC and PU methods was found to be fairly good with a kappa value of 0.714 (P < 0.001). For detection of M. TB, the PU method exhibited higher sensitivity than that achieved by the NaOH-NALC method according to McNemar test results (P < 0.001). (Table 2).

Culture results comparison: NaOH-NALC method vs. PU method. *In the PU method, an additional 13 specimens were identified as positive for M. TB. In contrast, when the same 13 specimens were processed using the NaOH-NALC method, 6 specimens were classified as negative and 7 specimens were contaminated.**In the PU method, an additional 9 specimens were identified as positive for NTM. In contrast, when the same 9 specimens were processed using the NaOH-NALC method, 3 specimens were classified as negative and 6 specimens were contaminated.
Additionally, among the 252 specimens, only 5 (1.98%) cases exhibited positive results through direct AFB smear microscopy. However, the NALC-NaOH method detected AFB smear microscopy in 16 (6.34%) of the processed specimens, while the PU method identified it in 20 (7.93%). Significantly, AFB smear microscopy detected two additional positive cases in stool specimens following decontamination with the NALC-NaOH method compared to culture results obtained from specimens treated with the same method. However, both stool specimens that showed positive smears were also found to be culture-positive when subjected to decontamination using the PU method (Table 2).
Contamination and time-to-culture-positive (TTP, NaOH-NALC vs. PU methods)
The contamination rates of stool specimens were 22.62% (57/252) and 14.28% (36/252) when decontaminated with the NALC-NaOH method and the PU method, respectively (Table 2)(Fig. 3C). A statistically significant difference was observed between these two methods (P < 0.001, g = 0.083).
Among the 252 stool specimens, a total of 14 (4.92%) yielded culture-positive results when subjected to decontamination using both methods, including M. TB (n = 11, 4.37%) and NTM (n = 3, 1.19%). The median time to positivity for M. TB detection using the PU method was shorter at 10.75 days (4.87), compared to the NALC-NaOH method which had a median time to positivity of 10.92 days (7.34). This disparity in detection time exhibited statistical significance(Z=-2.668, P = 0.008). The Hodges-Lehmann estimator further quantified this difference as a median reduction of 0.33 days (95% CI: 0.083–3.416), when using the PU method compared to the NALC-NaOH method.
Discussion
Stool specimens offer the advantages of being non-invasive and easy to collect for testing. However, the use of stool specimens for mycobacterial culture continues to encounter significant challenges in clinical practice, primarily due to relatively low diagnostic sensitivity and frequent contamination by intestinal flora during specimen processing. Enhanced DDMs can effectively reduce contamination in stool cultures, thus facilitating more accurate assessments of their diagnostic efficacy2. In the past few decades, a significant number of studies have been conducted on the enhancement of DDMs; however, the majority of these investigations have predominantly focused on decontamination agents. Research findings indicate that, in comparison to NALC-NaOH, neither sulfuric acid, chlorhexidine, nor Cetylpyridinium chloride has achieved substantial advancements in addressing the issues of low sensitivity and high contamination rates associated with stool mycobacterial culture10,11,12,13. In our study, we discovered that the PU method, a novel decontamination technique, markedly increased the isolation rates of both M. TB (9.52% vs. 4.37%, P < 0.001) and NTM (4.76% vs. 1.19%, P < 0.001) from pediatric stool specimens compared to the NaOH-NALC method. Although the effect sizes for detecting MTB (g = 0.052) and NTM (g = 0.036) were relatively small, the PU method substantially improved the sensitivity of MTB detection (42.11% vs. 19.30%, P < 0.001) and NTM detection (54.55% vs. 13.64%, P < 0.001) compared to the NaOH-NALC method. These findings indicate that the PU method offers significant advantages for mycobacterial culture in stool specimens from pediatric patients. In addition, the processed stool specimens using the PU method exhibited a significantly shorter median TTP (10.75 days vs. 10.92 days, P < 0.001) in detecting M. TB. The TTP, which serves as an indicator of the metabolic activity of M. TB in a liquid medium, exhibits an inverse correlation with the bacterial activity upon inoculation24. These intriguing findings suggest that the PU method surpasses the routine NaOH-NALC method in the decontamination process, potentially improving the diagnostic yield of mycobacterial culture in children. However, it should be noted that these observed outcomes could potentially be ascribed to the pre-digestion and decontamination procedure employed in the PU method. This procedure entails subjecting stool specimens to ultrasonic dispersion at a power output of 100 W with an aim to enhance optimal dispersal of Mycobacteria contained within the specimens, thus aiding their isolation20. In this study, the ultrasonic parameters for processing adult stool reported in our team’s prior publications were adopted(Fig. 1A). Our previous findings indicated that, irrespective of whether sputum10 or stool20 specimens were used, the ultrasonic decontamination achieved by applying this set of ultrasonic parameters combined with the digestive effect of NaOH was relatively stable in terms of protecting mycobacteria while effectively eliminating contaminating bacteria.
Contamination significantly delays the timely diagnosis of pediatric PTB by impeding the successful cultivation of M. TB in stool specimens4. The data from our study reveals that stool specimens treated with the PU method (14.28%) exhibited a significantly reduced contamination rate compared to those treated with the NALC-NaOH method (22.62%). In previous studies, the contamination rate of stool specimens treated with NALC and NaOH ranged from 14 to 41%2,3,4,5,6,7,8,9,10. In our preliminary investigations, the contamination rate obtained via PU method treatment was 13.23%, indicating a level of contamination comparable to that observed in the present study20. Notably, to improve the detection rate of mycobacteria, this study utilized an increased amount of stool specimen (0.5 g compared to the 0.1 g used in prior studies). However, the results showed that the contamination rate did not change significantly. The more intriguing aspect of our data lies in the fact that specimens contaminated with the NALC-NaOH method exhibited 7 cases of M. TB and 6 cases of NTM when undergoing the PU method treatment(Fig. 3). The results demonstrate that, despite the reduction in decontamination time for the PU method (from 15 min to 10 min), it exhibited superior performance in terms of contamination removal rate compared to the NALC-NaOH method.
The AFB smear microscopy is extensively utilized as a pivotal method for the early detection of tuberculosis; however, it is an insensitive test for TB in children25. In this study, only 5 cases (1.98%) showed positive results in direct AFB smear microscopy. Following centrifugation to collect bacteria using either the NaOH-NALC method (6.34%) or the PU method (7.93%), an increase in the positivity rate of stool smear was observed. Additionally, the present study revealed a finding whereby AFB smear microscopy demonstrated the detection of two additional positive cases in stool specimens, as compared to culture after decontamination using the NALC-NaOH method (Table 2). However, the two stool specimens with positive smears were found to be culture-positive after decontamination using the PU method. This interesting finding suggests that the NALC-NaOH method may kill mycobacteria in the two stool specimens, while the PU method may protect their activity.
The PU method, furthermore, facilitated the identification of additional cases of NTM infection in pediatric patients. Considering the escalating prevalence of NTM diseases26, the PU method demonstrates significant potential for widespread adoption. Additionally, due to a limited number of cases where both methods successfully identified NTM (only three cases), a detailed investigation into TTP for isolated NTM was not pursued in this study.
From a cost perspective, although the PU method necessitates an additional purchase of a PU meter valued at approximately USD 500, it obviates the expense associated with fresh preparation of NALC in comparison to the NALC-NaOH method.
The present study has produced intriguing findings; however, it is important to acknowledge its limitations. Firstly, the initial design of the PU parameters was based on our previous studies of sputum and fecal specimens, without conducting any preliminary experiments specifically tailored to the pediatric population. Therefore, it is imperative to further optimize these parameters as they may not be the most optimal choice in this context. Secondly, comprehensive validation of our findings necessitates additional large-scale and rigorous multi-center studies.
Conclusion
In conclusion, our findings suggest that the PU method represents a more expedient and efficacious approach for stool mycobacterial culture in the detection of active tuberculosis in pediatric patients when compared to the NALC-NaOH method.
Data availability
All data supporting the findings of this study are available within the paper.
References
World Health Organization (WHO). Global Tuberculosis Report. http://www.who.int/tb/publications/global_report/en/. (Accessed 7 May 2024). (2023).
Walters, E. et al. Stool culture for diagnosis of pulmonary tuberculosis in children. J. Clin. Microbiol. 55 (12), 3355–3365. https://doi.org/10.1128/JCM.00801-17 (2017).
Nicol, M. P. & Zar, H. J. Advances in the diagnosis of pulmonary tuberculosis in children. Paediatr. Respir. Rev. 36, 52–56. https://doi.org/10.1016/j.prrv.2020.05.003 (2020).
DiNardo, A. R. et al. Culture is an imperfect and heterogeneous reference standard in pediatric tuberculosis. Tuberculosis. 101S, S105–S8 (2016).
Sturm, R. A three-dimensional model of tracheobronchial particle distribution during mucociliary clearance in the human respiratory tract. Z. Med. Phys. 23(2), 111-9. https://doi.org/10.1016/j.zemedi.2013.02.004. (2013).
El Khéchine, A., Henry, M., Raoult, D. & Drancourt, M. Detection of Mycobacterium tuberculosis complex organisms in the stools of patients with pulmonary tuberculosis. Microbiology. 155 (Pt 7), 2384–2389. https://doi.org/10.1099/mic.0.026484-0 (2009).
Donald, P. R. et al. Stool microscopy and culture to assist the diagnosis of pulmonary tuberculosis in childhood. J. Trop. Pediatr. 42(5), 311-2. https://doi.org/10.1093/tropej/42.5.311. (1996).
Abaye, G. E. et al. Detection of Mycobacterium tuberculosis from the stool of HIV sero-positive individuals suspected of pulmonary tuberculosis. PLoS One. 12 (5), e0177529. https://doi.org/10.1371/journal.pone.0177529 (2017).
Oramasionwu, G. E. et al. The utility of stool cultures for diagnosing tuberculosis in people living with the human immunodeficiency virus. Int. J. Tuberc. Lung Dis. 17 (8), 1023–1028. https://doi.org/10.5588/ijtld.13.0061 (2013).
Wang, J. et al. Comparison of sputum treated with power ultrasound and routine NALC-NaOH methods for mycobacterial culture: A prospective study. J. Clin. Med. 11 (16), 4694. https://doi.org/10.3390/jcm11164694 (2022).
Allen, B. W. Comparison of three methods for decontamination of faeces for isolation of Mycobacterium tuberculosis. Tubercle. 72(3), 214-217. https://doi.org/10.1016/0041-3879(91)90011-g (1991).
Chatterjee, M., Bhattacharya, S., Karak, K. & Dastidar, S. G. Effects of different methods of decontamination for successful cultivation of Mycobacterium tuberculosis. Indian J. Med. Res. 138 (4), 541–548. (2013).
Rajendran, P. et al. Standardization of a stool concentration method for Mycobacterium tuberculosis detection in the pediatric population. Int. J. Mycobacteriol. 11(4), 371–377. https://doi.org/10.4103/ijmy.ijmy_126_22 (2022).
Joyce, E., Mason, T. J., Phull, S. S. & Lorimer, J. P. The development and evaluation of electrolysis in conjunction with power ultrasound for the disinfection of bacterial suspensions. Ultrason. Sonochem. 10(4–5), 231-234. https://doi.org/10.1016/S1350-4177(03)00109-3 (2003).
Mason, T. J., Joyce, E., Phull, S. S. & Lorimer, J. P. Potential uses of ultrasound in the biological decontamination of water. Ultrason. Sonochem. 10(6), 319 -323. https://doi.org/10.1016/S1350-4177(03)00102-0 (2003).
Gao, S., Hemar, Y., Ashokkumar, M., Paturel, S. & Lewis, G. D. Inactivation of bacteria and yeast using high-frequency ultrasound treatment. Water Res. 60, 93–104. https://doi.org/10.1016/j.watres.2014.04.038. (2014).
Gao, S., Lewis, G. D., Ashokkumar, M. & Hemar, Y. Inactivation of microorganisms by low-frequency high-power ultrasound: 2. A simple model for the inactivation mechanism. Ultrason. Sonochem. 21 (1), 454–460. https://doi.org/10.1016/j.ultsonch.2013.06.007 (2014).
Akdeniz, V. & Akalın, A. S. Recent advances in dual effect of power ultrasound to microorganisms in dairy industry: activation or inactivation. Crit. Rev. Food Sci. Nutr. 62 (4), 889–904. https://doi.org/10.1080/10408398.2020.1830027 (2022).
Alvarez, I., Mañas, P., Sala, F. J. & Condón, S. Inactivation of Salmonella enterica serovar enteritidis by ultrasonic waves under pressure at different water activities. Appl. Environ. Microbiol. 69 (1), 668–672. https://doi.org/10.1128/AEM.69.1.668-672.2003 (2003).
Tian, P. et al. Comparison of power ultrasound and NALC-NaOH decontamination methods for stool mycobacterial culture: A prospective study. Microorganisms 12 (9), 1799. https://doi.org/10.3390/microorganisms12091799 (2024).
National Health Commission of the People’s Republic of China. WS 288–2017 diagnosis of pulmonary tuberculosis. J. Tuberc. Pulm. Dis. 5, 376–378. https://doi.org/10.19983/j.issn.2096-8493.2024022 (2024).
Chinese Medical Association Tuberculosis Division. Guidelines for the Diagnosis and Treatment of Non-tuberculous Mycobacterial Disease. Chin. J. Tuberc. Respir. Dis. 43, 918–946. https://doi.org/10.3760/cma.j.cn112147-20200508-00570 (2020).
World Health Organization (WHO). Practical manual of processing stool specimens for the diagnosis of childhood TB. http://www.who.int/publications/i/item/9789240042650 (Accessed 7 May 2024). (2022).
Diacon, A. H. et al. Time to detection of the growth of Mycobacterium tuberculosis in MGIT 960 for determining the early bactericidal activity of antituberculosis agents. Eur. J. Clin. Microbiol. Infect. Dis. 29(12), 1561-5. https://doi.org/10.1007/s10096-010-1043-7 (2010).
DiNardo, A. R. et al. Use of string test and stool specimens to diagnose pulmonary tuberculosis. Int. J. Infect. Dis. 41, 50–52. https://doi.org/10.1016/j.ijid.2015.10.022 (2015).
Xu, N., Li, L. & Wu, S. Epidemiology and laboratory detection of non-tuberculous mycobacteria. Heliyon 10 (15), e35311. https://doi.org/10.1016/j.heliyon.2024.e35311 (2024).
Funding
This research was funded by Department of Science and Technology of Shandong Province (No. 2021SFGC0504), and Shandong Provincial Key Projects in Traditional Chinese Medicine Technology (No. M-2023161).
Author information
Authors and Affiliations
Contributions
J.W., Z.Z. and F.W. had the idea for and designed the study and had full access to all data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. Z.Z. and F.W. wrote and revised the manuscript. J.W., Z.Z., F.W. and M.C. participated in data collection. Z.Z., F.W. and M.C. performed the data analysis. P.T. and X.W. contributed to critical revision of the manuscript for important intellectual content.All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The experimental protocol was developed in accordance with the ethical guidelines of the Helsinki Declaration and received approval from the Ethical Committee of Shandong Public Health Clinical Center (Approval No. GWLCZXEC2023-61). Written informed consent was obtained from all individual participants and their guardians.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, Jl., Zhang, Zj., Wang, F. et al. A prospective study on enhanced recovery of Mycobacterium tuberculosis from children’s stool using novel power ultrasound decontamination. Sci Rep 15, 13309 (2025). https://doi.org/10.1038/s41598-025-98037-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-98037-5
