
Abstract
Few studies have explored the impact of different primary entry tear sites in acute type A aortic dissection. We aimed to evaluate the effect of the primary entry tear location on presentation, treatment, and outcome in this condition. We retrospectively reviewed acute type A aortic dissection repair surgical records at our institution (2004 and 2020) (n = 213). The patients were classified into the ascending aorta entry (As-E), aortic arch entry (Ar-E), and descending thoracic aorta or downstream entry (Dd-E) groups. The As-E group was the oldest (P < 0.01) and included the fewest males (P < 0.01). Pre-operative neurological complication rates were highest in As-E, 16%; Ar-E, 5%; and Dd-E, 0% (P = 0.03). Malperfusion syndrome rates were as follows: As-E, 10%; Ar-E, 2%; and Dd-E, 0% (P = 0.05). As-E was associated with the highest in-hospital mortality (As-E, 13%; Ar-E, 8%; Dd-E, 0%; P = 0.27). In-hospital mortality risk factors included pre-operative neurological complications, malperfusion syndrome, and concomitant procedures. Subanalysis revealed that ascending aortic entry was an independent risk factor for pre-operative acute neurological complications. The primary entry site may indirectly affect outcomes, by mediating the risks of pre-operative complications, which are linked to mortality.
Similar content being viewed by others


Introduction
Acute type A aortic dissection (ATAAD) is a life-threatening condition with a reported mortality rate of approximately 1–2%/h from its onset if left untreated1. Immediate surgical intervention is required to prevent fatal complications, including aortic rupture and malperfusion. In the widely accepted tear-oriented strategy1,2,3,4, wherein tear resection is the top priority, the extent of aortic replacement is determined based on the tear location. In experimental models, the primary entry tear site has been shown to affect the aortic dissection haemodynamics5,6,7. Specifically, a proximal entry in the ATAAD model can lead to expansion and compression of the true lumen5, resulting in rupture and malperfusion. In clinical settings, a more central entry location can lead to adverse outcomes in acute type B aortic dissection (ATBAD)8.
Nevertheless, few studies have focused on primary entry tear site-related differences in patient presentation, surgical procedures, and outcomes in ATAAD. Considering that emergent surgery is not possible in all patients due to geographical or technological constraints, understanding which primary entry point in ATAAD has a more negative effect in the context of pre-operative characteristics is crucial, given that the pre-operative status in ATAAD significantly impacts prognosis9,10,11,12,13. Although some evidence suggests an association between the entry tear in the distal arch and adverse outcomes, it is based on inconsistent classifications derived from factors other than aortic anatomy14,15 without accounting for the patients’ pre-operative characteristics.
In this study, we hypothesized that a proximally located entry tear is associated with adverse pre-operative conditions and mortality. Therefore, we aimed to clarify the relationship between the primary entry tear sites, classified according to aortic anatomy, and pre-operative patient characteristics, and short- and long-term surgical outcomes.
Methods
Ethical approvalwas secured from Saga University Clinical Research Review Board (Saga, Japan; Approval No. 2022-10-R-01). This study adheres to the 1964 Declaration of Helsinki and its later amendments. Informed consent was waived by Saga University Clinical Research Review Board (Saga, Japan) due to the retrospective nature of the study.
Patients
We included 213 patients with ATAAD who underwent surgery at the study site (January 2004 and December 2020). All data were obtained from medical records and during telephone surveys.
The primary entry tear sites were identified using pre-operative computed tomography scans, intraoperative visual findings, or transoesophageal echocardiography. Sixteen patients were excluded because of unidentified or unconfirmed primary tear locations. One patient was excluded because of an intraoperative dissection. Finally, patients (n = 196) were categorized into three groups based on the primary entry tear site: in the ascending aorta (As-E), in the aortic arch (Ar-E), and in the descending thoracic or downstream aorta (Dd-E) (Fig. 1).

Flowchart of the patient inclusion process. ATAAD, acute type A aortic dissection.
Surgical procedure
A tear-oriented strategy, employing the open distal method, is our institution’s standard surgical treatment for ATAAD16. All surgical repairs were performed using a median sternotomy and standard cardiopulmonary bypass. Experienced surgeons determined the arterial cannulation sites and numbers. Application of antegrade selective or retrograde cerebral perfusion, the degree of hypothermia, and utilization of the frozen elephant trunk technique were at the surgeon’s discretion. Concomitant procedures were performed as required.
Study definitions
ATAAD was defined as any dissection involving the ascending aorta and presenting within 2 weeks of symptom onset. A distal aortic event was defined as a thoracic aortic diameter of > 5.5 cm or an enlargement of 0.5 cm/6 months, new occurrence of distal aortic dissection, aortic aneurysm rupture, sudden death in a patient with noted aortic enlargement, or late aortic surgery.
Statistical analyses
Data were analyzed using the JMP software (version 16.0; SAS Institute, Cary, NC, USA) and EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria). Specifically, EZR is a modified version of R Commander, designed to add statistical functions frequently used in biostatistics17. Continuous variables are expressed as means ± standard deviations or as medians (interquartile ranges) and were assessed using a one-way analysis of variance or the Kruskal–Wallis test. Categorical variables are expressed as the total number and percentage and were compared using the chi-square or Fisher’s exact test. In this study, there were no missing data except for one variable, the time from onset to surgery, and the missing data for this variable were < 8%. Therefore, these were excluded from the analysis. Postoperative survival was assessed using the Kaplan–Meier method. Groups were compared by way of log-rank analysis. Competing risk analysis with the Gray’s test was performed for the long-term aortic events. In multivariable analysis, binomial logistic regression analysis was conducted to investigate risk factors for postoperative in-hospital mortality. Variables were identified using a forward and backward stepwise approach based on P < 0.05. Cox regression analysis was performed to evaluate long-term survival using a similar method.
As subanalysis, logistic regression analysis was conducted to identify risk factors for pre-operative neurological complications, malperfusion syndrome, and shock associated with the proximal entry site. Age, sex, hypertension, diabetes, serum creatinine level, atrial fibrillation, history of ischemic heart disease, history of cerebrovascular disease, history of open-heart surgery, dialysis, chronic obstructive pulmonary disease, time from onset to surgery, and primary entry tear location were included as covariates. In multivariable analysis, multicollinearity was assessed using variance inflation factor (VIF) and all variables had VIF of less than 10. Subgroup analysis was performed to clarify the relationship between the time from onset to surgery, and pre-operative aortic dissection-related major complications and mortality across groups. Patients in each group were divided into two subgroups according to intervention time: ≤5 h and > 5 h. Statistical significance was set at P < 0.05.
Results
Pre-operative variables
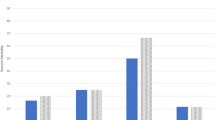
Table 1 presents the patients’ pre-operative characteristics. The primary entry point was the As-E in 119 (60.7%) patients, Ar-E in 64 (32.7%), and Dd-E in 13 (6.6%). The patients were the oldest in the As-E group (As-E, 70 ± 13 years; Ar-E, 65 ± 13 years; Dd-E, 54 ± 11 years; P < 0.001). The As-E group had the fewest male patients (As-E, 36%; Ar-E, 56%; Dd-E, 85%; P < 0.001). The As-E group had a higher prevalence of pre-operative shock, aortic regurgitation, central neurological complications, and malperfusion syndrome than the other two groups (Fig. 2). The time from onset to surgery was comparable among the three groups (P = 0.551).

Relationship between pre-operative aortic dissection-related major complications and surgical procedures across groups. Ar-E aortic arch entry, As-E ascending aorta entry, Dd-E descending thoracic aorta or downstream entry.
Intraoperative variables
Intraoperative characteristics of the groups are presented in (Table 2). Ascending aortic replacement was most frequently performed in the As-E group, whereas total arch replacement (TAR) was most common in the Dd-E group (P < 0.001) (Fig. 2). The entry closure rates were 100, 98.4, and 0% in the As-E, Ar-E, and Dd-E groups, respectively (P < 0.001). Although no significant differences in operative and cardiopulmonary bypass times were observed among the groups, circulatory arrest periods were longer in the Ar-E group than in the other groups (P < 0.001).
Postoperative short-term outcomes
Overall, 13 (6.6%) patients died within 30 days post-surgery. The in-hospital mortality rates were 12.6%, 7.8%, and 0% in the As-E, Ar-E, and Dd-E groups, respectively (P = 0.269). Additionally, the incidence rates of reoperation, new-onset cerebrovascular disease, and tracheostomy were the lowest in the Dd-E group (Table 3).
In binomial logistic regression for in-hospital mortality, the independent risk factors were age (odds ratio [OR] 1.07, 95% confidence interval [CI] 1.00–1.13, P = 0.024), pre-operative acute neurological complications (OR 6.89, 95% CI 1.66–28.6, P = 0.008), malperfusion syndrome (OR 8.84, 95% CI 2.05–38.2, P = 0.004), concomitant procedures (OR 8.15, 95% CI 2.31–28.7, P = 0.001), circulatory arrest time (OR 1.04, 95% CI 1.01–1.08, P = 0.022), and intraoperative use of fresh frozen plasma (OR 1.04, 95% CI 1.00–1.08, P = 0.043) (Table 4). The primary entry tear location was not an independent risk factor for in-hospital mortality.
Postoperative long-term outcomes
The unadjusted long-term survival rate was the lowest in the As-E group (P = 0.004). The 10-year survival rates were 51.9, 69.1, and 90.0% in the As-E, Ar-E, and Dd-E groups, respectively (Fig. 3A). Multivariable Cox regression analysis revealed that age (hazard ratio [HR] 1.09, 95% CI 1.05–1.12, P < 0.001), diabetes (HR 4.00, 95% CI 1.31–12.2, P = 0.015), pre-operative acute neurological complications (HR 4.37, 95% CI 2.08–9.20, P < 0.001), malperfusion syndrome (HR 3.11, 95% CI 1.27–7.61, P = 0.038), concomitant procedures (HR 2.96, 95% CI 1.48–5.90, P = 0.002), and intraoperative use of packed red blood cells (HR 1.03, 95% CI 1.01–1.06, P = 0.012), but not the primary entry tear location, were independent predictors of late mortality (Supplementary Table S1).

(A) Kaplan–Meier survival estimates and (B) competing risk analysis for long-term aortic events (with death as a competing risk) in all patients according to the primary entry tear locations. Ar-E aortic arch entry, As-E ascending aorta entry, Dd-E descending thoracic aorta or downstream entry.
Additionally, the incidence of aortic event rate differed significantly among the groups, with the Dd-E group having the highest event rate. The 10-year event incidence rates were 10.9, 18.2 and 53.0% in the As-E, Ar-E, and Dd-E groups, respectively (Fig. 3B).
Subanalyses
Multiple logistic regression analysis revealed that As-E was an independent predictor of pre-operative acute neurological complications (OR 4.81, 95% CI 1.13–20.5, P = 0.033); however, it did not independently predict malperfusion syndrome, despite a trend toward significance (OR 8.96, 95% CI 0.90–88.9, P = 0.061). Only serum creatinine levels (OR 1.89, 95% CI 1.02–3.50, P = 0.042) independently predicted shock (Supplementary Table S2).
Subgroup analysis demonstrated that patients within 5 h had a higher prevalence of pre-operative major complications than the other group in the As-E group. However, there was no significant difference in in-hospital mortality. In the Ar-E group, there was no significant difference in pre-operative complications between the subgroups, but the mortality rate was significantly higher in the group within 5 h. The Dd-E group did not experience any serious pre-operative complications or deaths (Supplementary Table S3).
Discussion
In this study, we compared the pre-operative characteristics, perioperative outcomes, long-term survival, and aortic events associated with primary entry tears in the ascending aorta, aortic arch, and descending aorta in ATAAD repair. The study revealed two key findings. First, the primary entry tear site was not an independent risk factor for short- or long-term mortality. Second, in the unadjusted cohort, patients with more proximal entry sites were more likely to have worse pre-operative conditions and higher short- and long-term mortality rates.
Takami et al.15 classified the entry sites into proximal, middle, and distal ascending arch and descending or unknown sites and investigated their relationship with computed tomography scan findings. They reported that primary entry into the ascending aorta was the most frequent (65.6%), followed by the arch, which is consistent with our results. They also suggested that pericardial effusion and ascending aortic dilatation predicted primary entry into the ascending aorta. However, the finding that the mortality rate was higher with primary entry in the arch and descending aorta than with the ascending aorta contradicts our results15.
Merkle et al.14 similarly reported that the distal arch entry group had the worst outcome. They classified the entry sites into three groups: ascending aorta, proximal arch, and distal arch. Furthermore, ascending or hemiarch replacement was performed when the entry site was in the ascending or proximal arch and performed TAR when the entry site was in the distal arch14. This outcome was assumed to be due to the surgical procedure rather than the primary entry tear site and referred to studies associating TAR with a mortality rate higher than that associated with aortic replacement18,19,20. However, other investigators have proposed that TAR has similar perioperative outcomes in patients with ATAAD4,21.
In our study, patients with Dd-E had the highest long-term survival, although most patients with Dd-E underwent TAR. Logistic and Cox regression analyses also demonstrated that the surgical procedure was not a risk factor for short- or long-term mortality. Furthermore, Merkle et al.’s study differed from the present study in that the entry site could not be resected in some of their patients, particularly in the distal arch entry group with poor pre-operative conditions14. This may have led to adverse outcomes. Moreover, Merkle et al. found no differences in the pre-operative characteristics among groups14, which was inconsistent with our study. This discrepancy may be due to their patients being relatively young and not including octogenarians or may be due to the time lapse between symptom onset and surgery. Because time was not a focus of their study, it is possible that patients with poor pre-operative conditions died before surgery and were excluded from their study.
The postoperative outcomes of ATAAD are affected by pre-operative malperfusion syndrome, acute neurological complications, and shock9,10,11,12,13. In this study, the As-E group had the highest mortality rate, likely because their pre-operative status was worse than that of the other two groups, although the primary entry tear site was not an independent risk factor for mortality. Hence, our hypothesis that a proximal primary entry site leads to the adverse outcome could not be confirmed. Interactions, in addition to confounding factors, were also evaluated in this study, but no significant differences were observed, likely due to the small study population. Therefore, our results should be interpreted carefully. We further hypothesized that patients with a proximal primary entry would have worse pre-operative status. This hypothesis was based on experimental research in which proximal entry was associated with aortic dissection-related major complications such as rupture and malperfusion5, and a retrospective case study showing a more proximal entry site can lead to adverse outcomes in ATBAD8. We believe that our results supported this hypothesis because As-E was associated with acute neurological complication and an increased trend of malperfusion syndrome in the multivariable analysis. A previous report22 showed that the prognosis of patients with malperfusion and neurological complications improved with medical intervention within 5 h of ATAAD onset. Subgroup analysis in our study revealed that patients in the As-E group developed aortic dissection-related major complications more frequently, such as acute neurological complications and malperfusion syndrome, within 5 h. Despite patients being in serious condition, the mortality in the immediate intervention group was comparable to the late intervention group, which may indicate that this group benefits from immediate surgery. Our results imply that prioritizing patients with ascending aorta entry sites and providing urgent medical intervention can occur may help improve outcomes. Patients with ATAAD are now being diverted to aortic centers, which are high-volume centers, with expertise believed to help improve outcomes23,24,25; however, the time from onset to intervention often exceeds 5 h, and the timing of an intervention depends on the geographical region13,26,27. Meanwhile, retrograde ATAAD with a primary entry tear site in the descending thoracic aorta may require more time before surgery.
However, in the present study, the Dd-E group had a higher incidence of long-term aortic events than the As-E or Ar-E groups for reasons that remain unclear28,29. Kawahito et al.30 reported that residual entry into the downstream aorta was a risk factor for distal aortic events in patients with ATAAD treated with a tear-oriented strategy. However, they did not explain why the entry site was not resected or where it was located. Herein, we performed entry resection in all patients except for one in the Ar-E group and all in the Dd-E group. In the latter case, because the entry was located from the descending aorta to the abdominal aorta, it was not resected because it could not be reached by a median sternotomy approach. In ATBAD, residual entry is a well-known risk factor for long-term adverse aortic events31. Therefore, entry closure involving thoracic endovascular aortic repair is performed to prevent aortic-related complications such as aneurysms and expansion. Early intervention may be desirable when the primary entry tear site cannot be resected in ATAAD32.
This study had some limitations. The most important limitation of this study is the small sample size. Particularly, the Dd-E group had only 13 patients, which may have led to insufficient statistical power. Therefore, our findings should be interpreted with caution, and further research and evaluation is necessary using a larger amount of data in the future. Second, this was a single-center study based in Japan, limiting its generalizability. Third, this study included only patients who survived until the surgery.
In conclusion, the primary entry tear site in ATAAD was not an independent risk factor for mortality but affected the risk of pre-operative malperfusion syndrome and acute neurological complications, which increased mortality risks. Patients with ATAAD with a proximal entry had serious pre-operative conditions and had the highest mortality rate in crude analyses. In contrast, patients with ATAAD with left distal entry had more long-term adverse aortic events. These findings suggest the need for triage and follow-up protocols determined by the location of the primary entry tear site.
Data availability
The datasets generated and/or analysed during the current study are not publicly available due restrictions such as their containing information that could compromise the privacy of research participants, but can available from the corresponding author on reasonable request.
Abbreviations
- Ar-E:
-
Primary entry tear in the aortic arch
- As-E:
-
Primary entry tear in the ascending aorta
- ATAAD:
-
Acute type A aortic dissection
- ATBAD:
-
Acute type B aortic dissection
- CI:
-
Confidence interval
- Dd-E:
-
Primary entry tear in the descending thoracic aorta or downwards
- HR:
-
Hazard ratio
- OR:
-
Odds ratio
- TAR:
-
Total arch replacement
- VIF:
-
Variance inflation factor
References
Khandheria, B. K. Aortic dissection. The last frontier. Circulation 87, 1765–1768 (1993).
Westaby, S., Saito, S. & Katsumata, T. Acute type A dissection: Conservative methods provide consistently low mortality. Ann. Thorac. Surg. 73, 707–713 (2002).
Aizawa, K., Kawahito, K. & Misawa, Y. Long-term outcomes of tear-oriented ascending/hemiarch replacements for acute type A aortic dissection. Gen. Thorac. Cardiovasc. Surg. 64, 403–408 (2016).
Uchida, K. et al. Results of ascending aortic and arch replacement for type A aortic dissection. J. Thorac. Cardiovasc. Surg. 162, 1025–1031 (2021).
Shi, Y., Zhu, M., Chang, Y., Qiao, H. & Liu, Y. The risk of Stanford type-A aortic dissection with different tear size and location: a numerical study. Biomed. Eng. Online 15 (Supplement 2), 128 (2016).
Cheng, Z. et al. Initial findings and potential applicability of computational simulation of the aorta in acute type B dissection. J. Vasc Surg. 57, 35S–43S (2013).
Chung, J. W. et al. True-lumen collapse in aortic dissection: part I. Evaluation of causative factors in phantoms with pulsatile flow. Radiology 214, 87–98 (2000).
Weiss, G. et al. The location of the primary entry tear in acute type B aortic dissection affects early outcome. Eur. J. Cardiothorac. Surg. 42, 571–576 (2012).
Zhang, Y. et al. Risk factors for early death after surgery in patients with acute Stanford type A aortic dissection: a systematic review and meta-analysis. Int. J. Cardiol. 377, 33–41 (2023).
Zindovic, I. et al. Malperfusion in acute type A aortic dissection: an update from the nordic consortium for acute type A aortic dissection. J. Thorac. Cardiovasc. Surg. 157, 1324–1333e6 (2019).
Berretta, P. et al. IRAD experience on surgical type A acute dissection patients: results and predictors of mortality. Ann. Cardiothorac. Surg. 5, 346–351 (2016).
Long, S. M. et al. Preoperative shock determines outcome for acute type A aortic dissection. Ann. Thorac. Surg. 75, 520–524 (2003).
Conzelmann, L. O. et al. Mortality in patients with acute aortic dissection type A: analysis of pre- and intraoperative risk factors from the German registry for acute aortic dissection type A (GERAADA). Eur. J. Cardiothorac. Surg. 49, e44–e52 (2016).
Merkle, J. et al. Impact of different aortic entry tear sites on early outcomes and long-term survival in patients with Stanford A acute aortic dissection. Thorac. Cardiovasc. Surg. 67, 363–371 (2019).
Takami, Y. et al. Can we predict the site of entry tear by computed tomography in patients with acute type A aortic dissection? Clin. Cardiol. 35, 500–504 (2012).
Takahashi, B., Kamohara, K., Amamoto, S. & Kawaguchi, A. Impact of after-hours surgery on outcomes of acute type A aortic dissection repair. Surg. Today 52, 1453–1462 (2022).
Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transpl. 48, 452–458 (2013).
Kim, J. B. et al. Total arch repair versus hemiarch repair in the management of acute debakey type I aortic dissection. Eur. J. Cardiothorac. Surg. 40, 881–887 (2011).
Rylski, B. et al. Acute type A aortic dissection extending beyond ascending Aorta: limited or extensive distal repair. J. Thorac. Cardiovasc. Surg. 148, 949–954 (2014).
Lio, A. et al. Total arch versus hemiarch replacement for type A acute aortic dissection: a single-center experience. Tex. Heart Inst. J. 43, 488–495 (2016).
Kazui, T. et al. Extended total arch replacement for acute type A aortic dissection: experience with Seventy patients. J. Thorac. Cardiovasc. Surg. 119, 558–565 (2000).
Nakai, C. et al. Impact of time from symptom onset to operation on outcome of repair of acute type A aortic dissection with malperfusion. J. Thorac. Cardiovasc. Surg. 165, 984–991e1 (2023).
Izumisawa, Y. et al. Association between prehospital transfer distance and surgical mortality in emergency thoracic aortic surgery. J. Thorac. Cardiovasc. Surg. 163, 28–35e1 (2022).
Umana-Pizano, J. B. et al. Acute type A dissection repair by high-volume vs low-volume surgeons at a high-volume aortic center. Ann. Thorac. Surg. 108, 1330–1336 (2019).
Okita, Y. Current surgical results of acute type A aortic dissection in Japan. Ann. Cardiothorac. Surg. 5, 368–376 (2016).
Ahlsson, A. et al. Is there a weekend effect in surgery for type A dissection? Results from the nordic consortium for acute type A aortic dissection database. Ann. Thorac. Surg. 108, 770–776 (2019).
Arnaoutakis, G. et al. Time of day does not influence outcomes in acute type A aortic dissection: results from the IRAD. J. Card Surg. 35, 3467–3473 (2020).
Zierer, A. et al. Aortic enlargement and late reoperation after repair of acute type A aortic dissection. Ann. Thorac. Surg. 84, 479–486 (2007).
Inoue, Y. et al. Efficacy of entry exclusion strategy for debakey type III retrograde Stanford type A acute aortic dissection. Eur. J. Cardiothorac. Surg. 59, ezaa329 (2020).
Kawahito, K., Aizawa, K., Kimura, N., Yamaguchi, A. & Adachi, H. Influence of residual primary entry following the tear-oriented strategy for acute type A aortic dissection. Eur. J. Cardiothorac. Surg. 61, 1077–1084 (2022).
Lombardi, J. V. et al. Society for vascular surgery (SVS) and society of thoracic surgeons (STS) reporting standards for type B aortic dissections. J. Vasc Surg. 71, 723–747 (2020).
Iida, Y. et al. Extended thoracic endovascular aortic repair for residual aortic dissection after type A aortic dissection repair. Vascular 29, 826–831 (2021).
Acknowledgements
We thank Editage for the English language editing on the initial drafts of the manuscript.
Author information
Authors and Affiliations
Contributions
Baku Takahashi: Conceptualization; Data curation; Formal analysis; Investigation; Project administration; Writing—original draft; Writing—review & editing. Keiji Kamohara: Supervision. Hiroyuki Morokuma: Data curation; Validation. Junji Yunoki: Data curation; Validation. Atsushi Kawaguchi: Data curation; Formal analysis; Investigation; Validation.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Informed consent was waived by Saga University Clinical Research Review Board (Saga, Japan) due to the retrospective nature of the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Takahashi, B., Kamohara, K., Morokuma, H. et al. Impact of primary entry tear locations on outcomes in acute type A aortic dissection. Sci Rep 15, 13981 (2025). https://doi.org/10.1038/s41598-025-98581-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-98581-0
