
Abstract
Flow diverters (FDs) have been employed in the treatment of unruptured intracranial vertebral artery dissecting aneurysms (IVADAs), yielding seemingly favorable outcomes. Despite FD treatment, aneurysm persistence (incomplete occlusion post-initial treatment) can occur in some patients, potentially leading to recurrent symptoms or complications. This study aims to explore the risk factors associated with the persistence of unruptured IVADAs that have undergone treatment with FDs. The study encompassed 77 unruptured IVADAs from 75 consecutive patients who received treatment with FDs. At a median follow-up of 13 months, 31.2% (24/77) of IVADAs exhibited persistence. Upon multivariate logistic regression analysis, significant pre-procedural stenosis adjacent to aneurysmal dilatation (odds ratio [OR] 17.02, 95% confidence interval [CI] 2.01–144.24, p = 0.009) and posterior inferior cerebellar artery involvement (OR 7.06, 95% CI 1.40–35.50, p = 0.018) were independently associated with aneurysm persistence; while follow-up duration (OR 0.91, 95% CI 0.84–0.97, p = 0.005) was adversely associated with aneurysm persistence. Significant pre-procedural stenosis adjacent to aneurysmal dilatation and posterior inferior cerebellar artery involvement could serve as independent risk factors contributing to the persistence of unruptured IVADAs after FD treatment.
.
Similar content being viewed by others


Introduction
Intracranial vertebral artery dissecting aneurysms (IVADAs) are an important cause of subarachnoid hemorrhage (SAH) and posterior circulation ischemia in young and middle-aged people1. Endovascular treatment has been accepted as the mainstream approach for preventing SAH and ischemic stroke in patients with IVADAs2,3,4,5,6,7,8,9. In recent years, the practice of flow diverters (FDs) has been extended to unruptured IVADAs with favorable outcomes4,6,10,11,12,13,14. However, IVADAs may persist after flow diversion, potentially leading to delayed rupture or an increased mass effect15.
Understanding the risk factors contributing to this phenomenon is crucial for optimizing patient selection and treatment strategies. This study aims to identify the risk factors associated with the persistence of unruptured IVADAs treated with FDs. By examining clinical, morphological, and procedural variables, we seek to elucidate the underlying mechanisms that may influence treatment efficacy.
Methods
This study received approval from the Institutional Review Board of Beijing Tiantan Hospital (KY 2021-038-02), which waived the requirement for informed consent from patients due to the retrospective nature of the study design. All procedures were carried out in accordance with the relevant guidelines and regulations.
Patients
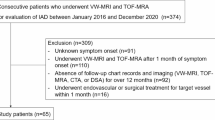
This study received approval from the Institutional Review Board. It retrospectively analyzed a consecutive series of patients with unruptured IVADAs who underwent treatment with first-ever FDs at Beijing Tiantan Hospital (Beijing, China) from January 2016 to February 2021. The diagnosis of IVADAs was based on clinical manifestations and radiological findings obtained either from three-dimensional digital subtraction angiography (3D-DSA) alone or 3D-DSA combined with CT angiography, MR angiography, and/or high- resolution MRI. Inclusion criteria were: (1) unruptured IVADAs with or without clinical manifestations, including posterior circulation ischemia and mass effect; (2) dissecting aneurysms involving but not limited to the V4 segment of the vertebral artery (VA); and (3) first-ever treated with FDs. The exclusion criteria were: (1) VA dilatation and/or stenosis without the signs of dissection, including a double lumen, intimal flap, or intramural hematoma; (2) previous history of surgical or endovascular treatment; (3) ruptured IVADAs; (4) history of using medications known to significantly affect platelet function; and (5) lack of follow-up data. Clinical data included age, sex, current smoking (within the past 6 months), hypertension, hyperlipidemia, diabetes mellitus (Type II), coronary artery disease, and pre-procedural modified Rankin Scale (mRS) scores > 2.
Morphological characteristics
All the morphological characteristics were well evaluated by using 3D-DSA images from a Siemens Artis Zee System (Siemens Healthcare, Erlangen, Germany), which included dominant VA, significant stenosis, the entirely involved circumference, posterior inferior cerebellar artery (PICA) involvement, basilar artery (BA) involvement, and maximum diameter. Two experienced researchers blinded to the patient’s clinical information independently interpreted the images and made consensus decisions. These morphological characteristics were defined as documented in previous studies16,17. Significant stenosis was defined as 50–99% stenosis of the parent artery adjacent to the aneurysmal dilatation.
Treatment protocol
FDs used in this study were the Pipeline Embolization Device (PED; Medtronic, Irvine, CA, USA) and the Tubridge flow diverter (TFD; MicroPort, Shanghai, China). Before endovascular treatment, the neurointervention team discussed each case.
Before the procedure, patients diagnosed with unruptured IVADAs were administered dual antiplatelet therapy, which included 100 mg of aspirin and 75 mg of clopidogrel daily for a period of 5 days. After the procedure, this regimen was maintained for an additional 6 months. The patients’ responses to aspirin and clopidogrel were evaluated. In instances where hyporesponsiveness to clopidogrel was identified, ticagrelor was introduced as an alternative. Upon completion of the dual antiplatelet therapy, a maintenance regimen of 100 mg of aspirin daily was advised for a further 6 to 9 months.
Endovascular treatment was performed transfemorally when patients were under general anesthesia. Heparin was administered when the FDs were ready for deployment. The entire dissecting segment of the parent artery, including stenosis, was reconstructed. We tried reconstructing the involved segment of the parent artery with a single FD. Multiple FDs were considered when the involved segment was too long to be reconstructed by a single one. Coiling in conjunction with FD placement was selected for some giant IVADAs or complex IVADAs with both fusiform and saccular components. Balloon dilation was chosen for significant stenosis within the dissecting segment of the parent artery to ensure that the degree of stenosis after FD deployment was less than 50%.
Immediate occlusion status
We classified immediate occlusion status into complete and incomplete occlusion. Two experienced researchers blinded to clinical information independently interpreted the immediate occlusion status and achieved a consensus.
Radiological and clinical follow-up
The follow-up angiography included 3D-DSA, CT angiography, and MR angiography, preferably 3D-DSA. The first follow-up angiography was often scheduled between 3 and 6 months after endovascular treatment. Subsequent follow-up was conducted every 6 to 12 months. Follow-up occlusion status was classified into complete or incomplete occlusion. Aneurysm persistence was defined as incomplete occlusion ever since FD treatment.
Two experienced researchers, blinded to clinical information, independently assessed the occlusion status and subsequently reached a final consensus. The final clinical outcome was assessed using an mRS. The favorable clinical outcome was defined as mRS 0–2.
Statistical analysis
Continuous variables are reported as median values along with the interquartile range (IQR), while categorical variables are expressed as frequency and percentage. The normality of the distribution for continuous variables was assessed using the Shapiro-Wilk test. To compare continuous variables, the Mann–Whitney U test was utilized. For categorical variables, either Pearson’s Chi-squared test or Fisher’s exact test was conducted. Inter-observer agreement regarding the interpretation of IVADA morphological characteristics and immediate or follow-up occlusion status was evaluated. Cohen’s κ coefficient was employed to assess inter-observer agreement in interpreting qualitative characteristics, whereas the intraclass correlation coefficient was utilized for quantitative characteristics. An agreement represented by Cohen’s κ coefficient or intraclass correlation coefficient greater than 0.75 was deemed excellent. Univariate and multivariate logistic regression models were employed to explore the variables associated with aneurysm persistence. Significant variables (p < 0.10) identified in univariate analyses were included in the multivariate logistic regression model. Results are presented as odds ratios (OR) with corresponding 95% confidence intervals (CI). All statistical analyses were conducted using IBM SPSS Statistics for Windows, version 26.0 (IBM Corporation, Armonk, NY, USA), with two-tailed p-values of less than 0.05 considered statistically significant.
Results
Clinical and morphological characteristics
A total of 77 unruptured IVADAs treated with FDs for 75 patients were included in this study. There were 61 (79.2%) men and 16 (20.8%) women, with a median age of 53 years (age range interval 10–70 years). The median maximum diameter of IVADAs was 10.8 mm. The baseline characteristics of all the patients are shown in Table 1. Interobserver agreement of the measurements of all the morphological parameters was considered excellent. Cohen κ coefficients for dominant VA, significant stenosis, BA involvement, entirely involved circumference, and PICA involvement were 0.842, 0.885, 1.000, 0.870, and 0.964, respectively. The intraclass correlation coefficient for maximum diameter was 0.970. Hypertension was less prevalent in the persistence group than in the complete occlusion group (37.5% vs. 62.3%, p = 0.043). Pre-procedural significant stenosis was more prevalent in the persistence group than in the complete occlusion group (25.0% vs. 5.7%, p = 0.023). While PICA involvement was more prevalent in the persistence group than in the complete occlusion group (37.5% vs. 17.0%, p = 0.049). There was no significant difference between the two groups with respect to age, sex, smoking, hyperlipidemia, diabetes mellitus, coronary artery disease, pre-procedural mRS > 2, dominant VA, BA involvement, entirely involved circumference, or maximum diameter.
Treatment selection and results
All 77 procedures were successfully performed. Multiple FDs and conjunction with coils were used in 9.1% (7/77) and 13.0% (10/77) of the IVADAs, respectively. Immediate complete occlusion was achieved in 5.2% (4/77) of the IVADAs. The overall median follow-up duration of patients was 13 months. By the final follow-up, 31.2% (24/77) of the IVADAs showed persistent filling, which included one case of recanalization that had initially presented as incomplete occlusion. Cohen κ coefficient for complete occlusion was 0.941. The rate of mRS 0–2 was 98.7% (76/77).
A comparison of treatment selection and results are shown in Table 2. The median follow-up duration was significantly longer in the complete occlusion group than in the persistence group (19 vs. 7 months, p < 0.001). There were no significant between-group differences with respect to multiple FDs, conjunction with coils, immediate complete occlusion, or mRS 0–2.
Variables associated with aneurysm persistence
The results of univariate and multivariate logistic regression analyses for aneurysm persistence are shown in Table 3. In univariate analyses, hypertension, significant stenosis, PICA involvement, and follow-up duration were significant variables (p < 0.10). Upon multivariate regression analysis, significant stenosis adjacent to aneurysmal dilatation (OR 17.02, 95% CI 2.01–144.24, p = 0.009) and PICA involvement (OR 7.06, 95% CI 1.40–35.50, p = 0.018) were independently associated with aneurysm persistence; while follow-up duration (OR 0.91, 95% CI 0.84–0.97, p = 0.005) was adversely associated with aneurysm persistence.
Discussion
In this study, we investigated the risk factors for the persistence of unruptured IVADAs following FD treatment. Our findings indicated that significant stenosis adjacent to aneurysmal dilatation and PICA involvement are independent risk factors for aneurysm persistence. Conversely, a longer duration of follow-up serves as an independent protective factor against aneurysm persistence.
A stenosis adjacent to aneurysmal dilatation is common in IVADAs18. A previous study reported that parent artery stenosis could cause inadequate opening and poor apposition of FDs in the stenosis regions when treating anterior circulation non-dissecting aneurysms19. Another study indicated that stenosis > 50% of the parent artery next to the aneurysm restricted the opening of FDs and caused malapposition; at the median follow-up of 5.5 months, pre-procedural stenosis tended to be associated with incomplete aneurysmal occlusion20. We hypothesize that this mechanism may also account for persistent filling of IVADAs after flow diversion. We suggest that significant stenosis adjacent to the aneurysmal dilation is likely to result in inadequate apposition of FDs. Furthermore, smaller FDs may be preferentially chosen for IVADAs with significant stenosis to enhance deployment maneuverability and minimize the risk of arterial injury associated with balloon dilation. As traditional stents that are smaller than the vessel diameter can cause malapposition21. the use of smaller FDs may similarly contribute to malapposition.
After flow diversion, the endothelialization of FDs begins at the interface with the arterial wall. This initial process establishes a cellular substrate that promotes the subsequent endothelialization of areas of the FDs not directly in contact with the artery wall22. Consequently, malapposition of FDs can hinder endothelialization by decreasing the contact interface with the arterial wall, potentially leading to the persistence of aneurysms19,23,24,25.
The PICA is a crucial branch of the VA, and preserving its patency is essential during the endovascular treatment of IVADAs. Occlusion of the PICA can result in significant neurological deficits due to impaired blood flow to the cerebellum and brainstem. FDs facilitate the maintenance of the patency of covered branch arteries. However, when a branch artery is incorporated into the target aneurysm, its blood flow may continue to contribute to the aneurysm’s persistent filling, which can lead to incomplete occlusion despite the implementation of flow diversion techniques15. Previous studies have extensively documented the presence of aneurysms with incorporated branches, suggesting that these features may be the most significant contributor to persistent aneurysm filling after flow diversion26. However, the association between PICA involvement and persistent filling of IVADAs following flow diversion has not been well explored. Our findings indicate that PICA involvement is an independent risk factor for the persistent filling of IVADAs after flow diversion. This phenomenon underscores the importance of careful preoperative imaging and planning to assess the involvement of PICA in the IVADAs.
A prior study investigating flow diversion for the treatment of posterior circulation cerebral aneurysms reported a complete occlusion rate of 68% at six months, which increased to 78% at twelve months27. Additionally, a systematic review on predictors of aneurysm occlusion following FD treatment found that longer follow-up durations were associated with complete occlusion28. In our study, the duration of follow-up also demonstrated a predictive effect on the occlusion of IVADAs, aligning with findings from prior research27,28. We propose that two mechanisms may elucidate this phenomenon: (1) following flow diversion treatment, the endothelialization of areas of the FDs not directly in contact with the arterial wall improves over the follow-up period22; and (2) once complete occlusion of the aneurysm is achieved after flow diversion treatment, the likelihood of recurrence is minimal29,30.
Several limitations of our study should be acknowledged. First, the retrospective single-center design may have introduced potential bias. Second, we did not assess the association between malapposition and the persistence of IVADAs. Third, the tortuosity or curvature of the parent artery was not analyzed, which could represent a confounding factor. Fourth, information regarding complications and procedure time was not stated and analyzed. Additionally, the relatively small number of cases exhibiting immediate complete occlusion and those involving the use of additional coils may have limited our ability to detect significant correlations with aneurysm occlusion outcomes during the follow-up period. This limitation indicates that a larger dataset is necessary to draw more definitive conclusions.
We identified significant pre-procedural stenosis adjacent to aneurysmal dilatation and PICA involvement as potential independent risk factors for the persistence of unruptured IVADAs treated with FDs. These findings may facilitate the prediction of radiological outcomes for unruptured IVADAs following flow diversion and inform the development of strategies aimed at promoting aneurysm occlusion.
Data availability
The corresponding author can be contacted for inquiries, and anonymized data will be made available upon reasonable request from any qualified investigator. Correspondence and requests for materials should be addressed to A.L. or Y.X.
References
Arnold, M. et al. Vertebral artery dissection: presenting findings and predictors of outcome. Stroke 37, 2499–2503. https://doi.org/10.1161/01.STR.0000240493.88473.39 (2006).
Yoon, W. et al. Dissection of the V4 segment of the vertebral artery: clinicoradiologic manifestations and endovascular treatment. Eur. Radiol. 17, 983–993. https://doi.org/10.1007/s00330-006-0272-8 (2007).
Kim, B. M. et al. Incidence and risk factors of recurrence after endovascular treatment of intracranial vertebrobasilar dissecting aneurysms. Stroke 42, 2425–2430. https://doi.org/10.1161/STROKEAHA.111.617381 (2011).
Kuhn, A. L. et al. Endovascular reconstruction of unruptured intradural vertebral artery dissecting aneurysms with the pipeline embolization device. J. Neurointerv Surg. 8, 1048–1051. https://doi.org/10.1136/neurintsurg-2015-012028 (2016).
Guan, J. et al. Endovascular treatment for ruptured and unruptured vertebral artery dissecting aneurysms: a meta-analysis. J. Neurointerv Surg. 9, 558–563. https://doi.org/10.1136/neurintsurg-2016-012309 (2017).
Cerejo, R. et al. Flow diverter treatment of intracranial vertebral artery dissecting pseudoaneurysms. J. Neurointerv Surg. 9, 1064–1068. https://doi.org/10.1136/neurintsurg-2017-013020 (2017).
Wang, K. et al. Risk factors of recurrence after Stent(s)-Assisted coiling of intracranial vertebrobasilar dissecting aneurysms: A multicenter study. Front. Neurol. 8, 482. https://doi.org/10.3389/fneur.2017.00482 (2017).
Tanoue, S. et al. Delineability and anatomical variations of perforating arteries from normal vertebral artery on 3D DSA: implications for endovascular treatment of dissecting aneurysms. Neuroradiology 63, 609–617. https://doi.org/10.1007/s00234-020-02549-y (2021).
Aihara, M. et al. Predictive factors of medullary infarction after endovascular internal trapping using coils for vertebral artery dissecting aneurysms. J. Neurosurg. 129, 107–113. https://doi.org/10.3171/2017.2.JNS162916 (2018).
Bhogal, P. et al. Treatment of posterior circulation non-saccular aneurysms with flow diverters: a single-center experience and review of 56 patients. J. Neurointerv Surg. 9, 471–481. https://doi.org/10.1136/neurintsurg-2016-012781 (2017).
Kan, P., Sweid, A., Srivatsan, A. & Jabbour, P. Expanding indications for flow diverters: Ruptured aneurysms, blister aneurysms, and dissecting aneurysms. Neurosurgery 86, S96–S103. https://doi.org/10.1093/neuros/nyz304 (2020).
Catapano, J. S. et al. Endovascular treatment of vertebral artery dissecting aneurysms: a 20-year institutional experience. J. Neurointerv Surg. https://doi.org/10.1136/neurintsurg-2020-017089 (2021).
Fang, Y. B. et al. Long-Term outcome of Tubridge flow Diverter(S) in treating large vertebral artery dissecting Aneurysms-A pilot study. Clin. Neuroradiol. 27, 345–350. https://doi.org/10.1007/s00062-015-0494-8 (2017).
Lee, W. et al. Flow diverter for the treatment of large (> 10 mm) vertebral artery dissecting aneurysms. Acta Neurochir. (Wien). 164, 1247–1254. https://doi.org/10.1007/s00701-021-04965-2 (2022).
Shapiro, M., Becske, T. & Nelson, P. K. Learning from failure: persistence of aneurysms following pipeline embolization. J. Neurosurg. 126, 578–585. https://doi.org/10.3171/2015.12.JNS152065 (2017).
Hong, J. M. et al. Vertebral artery dominance contributes to Basilar artery curvature and peri-vertebrobasilar junctional infarcts. J. Neurol. Neurosurg. Psychiatry. 80, 1087–1092. https://doi.org/10.1136/jnnp.2008.169805 (2009).
Han, J. et al. Morphological characteristics associated with ruptured intracranial vertebral artery dissecting aneurysms. J. Neurointerv Surg. https://doi.org/10.1136/neurintsurg-2022-018744 (2022).
Han, J. et al. Morphological characteristics associated with ruptured intracranial vertebral artery dissecting aneurysms. J. Neurointerv Surg. 15, 321–324. https://doi.org/10.1136/neurintsurg-2022-018744 (2023).
Cherian, J. et al. Balloon-Mounted stents for treatment of refractory flow diverting device wall malapposition. Oper. Neurosurg. (Hagerstown). 19, 37–42. https://doi.org/10.1093/ons/opz297 (2020).
Liang, F. et al. Use of pipeline embolization device for posterior circulation aneurysms: Single-Center experiences with comparison with anterior circulation aneurysms. World Neurosurg. 112, e683–e690. https://doi.org/10.1016/j.wneu.2018.01.129 (2018).
Attizzani, G. F., Capodanno, D., Ohno, Y. & Tamburino, C. Mechanisms, pathophysiology, and clinical aspects of incomplete stent apposition. J. Am. Coll. Cardiol. 63, 1355–1367. https://doi.org/10.1016/j.jacc.2014.01.019 (2014).
Kadirvel, R. et al. Cellular mechanisms of aneurysm occlusion after treatment with a flow diverter. Radiology 270, 394–399. https://doi.org/10.1148/radiol.13130796 (2014).
Rouchaud, A. et al. Wall apposition is a key factor for aneurysm occlusion after flow diversion: A histologic evaluation in 41 rabbits. AJNR Am. J. Neuroradiol. 37, 2087–2091. https://doi.org/10.3174/ajnr.A4848 (2016).
Panchendrabose, K., Muram, S. & Mitha, A. P. Promoting endothelialization of flow-diverting stents: a review. J. Neurointerv Surg. 13, 86–90. https://doi.org/10.1136/neurintsurg-2020-015874 (2021).
King, R. M. et al. Communicating malapposition of flow diverters assessed with optical coherence tomography correlates with delayed aneurysm occlusion. J. Neurointerv Surg. 10, 693–697. https://doi.org/10.1136/neurintsurg-2017-013502 (2018).
Dong, L. et al. Predicting persistent aneurysm filling after pipeline embolization device treatment in patients with intracranial aneurysm: development and external validation of a nomogram model. Transl Stroke Res. https://doi.org/10.1007/s12975-023-01222-9 (2023).
Bender, M. T. et al. Flow diversion of posterior circulation cerebral aneurysms: A Single-Institution series of 59 cases. Neurosurgery 84, 206–216. https://doi.org/10.1093/neuros/nyy076 (2019).
Meyer, L. et al. Predictors of aneurysm occlusion after treatment with flow diverters: a systematic literature review. J. Neurointerv Surg. 16, 482–490. https://doi.org/10.1136/jnis-2022-019993 (2024).
Catapano, J. S. et al. Endovascular treatment of vertebral artery dissecting aneurysms: a 20-year institutional experience. J. Neurointerv Surg. 14, 257–261. https://doi.org/10.1136/neurintsurg-2020-017089 (2022).
Chua, M. M. J. et al. Flow diversion for treatment of intracranial aneurysms: mechanism and implications. Ann. Neurol. 85, 793–800. https://doi.org/10.1002/ana.25484 (2019).
Author information
Authors and Affiliations
Contributions
J.H. conceptualized and designed the study; collected, analyzed, and interpreted the data; and drafted the manuscript. X.L. interpreted the data. H.N. and L.L. collected the data. A.L. and Y.X. conceptualized, designed and supervised the study, and revised the manuscript. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Han, J., Li, X., Niu, H. et al. Risk factors for the persistence of unruptured intracranial vertebral artery dissecting aneurysms treated with flow diverters. Sci Rep 15, 13677 (2025). https://doi.org/10.1038/s41598-025-98737-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-98737-y
