
Abstract
Despite the decline in the overall birth rate, increasing preterm births and associated medical costs pose a national concern. We analyze hospitalization costs covered by national public insurance for preterm infants. Population-based data, obtained from the National Health Insurance Service (NHIS), which is operated by the Health Insurance Review and Assessment Service, were used for the study. Preterm births from January 1, 2008 to December 31, 2020 were included, using International Classification of Diseases and Related Health Problems, 10th edition (P07.2, extremely preterm < 28 weeks gestational age, P07.3, non-extremely preterm). The primary outcomes related to cost from the first hospitalization due to preterm births and medication, and laboratory, radiological, and functional tests by gestational age and birth weight. Additionally, we assessed the readmission rates of preterm infants and the associated medical costs. A total of 5,312,886 live infants were born, of which 90,575 were claimed as preterm birth hospitalization. The total medical cost per patient increased almost three-fold from $7,390.90 to $20,209.59 from 2008 to 2020; for the extremely preterm group, it increased four-fold ($13,961.03 to $55,984.47). The readmission rate within 90 days of discharge was 62.5%; however, a greater proportion of the extremely preterm, as compared to the non-extremely preterm (16.1% vs. 8.32%, P < 0.001) group was readmitted within 30 days. The extremely preterm group also incurred higher costs associated with readmission (mean $4293.8 vs. $2975.4, P < 0.001). This study reveals not only the increase in preterm birth rate in South Korea, but also in the associated medical costs. Further attention should be paid to efficient resource allocation at the national level to relieve the medical burden of preterm births.
Similar content being viewed by others

Introduction
Neonatal diseases account for the largest share of pediatric hospital stays and costs in the United States1. Of these, premature birth is still the leading cause of neonatal mortality and morbidities in developed countries2. The rate of preterm birth in the United States increased steadily to 12.3% in 20043,4. The global burden of disease reported that neonatal disorders, still one of the leading causes of death among children under five years, accounted for 2.1–2.2 million deaths in 20155.
Some worldwide cohort studies reported that the increasing trend of preterm birth has been mitigated6,7,8. However, our study group reported, in a previous study, that even during COVID-19 pandemics, the preterm birth rate in South Korea increased consistently, until recently9.
Additionally, hospital fees per single preterm infant have also increased, according to annual reports from the United States2. Korean data have not been investigated; however, we can assume that trends in neonatal practice in Korea have moved commensurately with technical advancement. National health insurance coverage should be considered as one of the factors for total expenditure on hospitalization, as financial accessibility has increased the availability of medical practice and examinations.
The objective of this study is to estimate the preterm infant hospitalization costs covered by national public insurance in South Korea, and to compare the yearly changes from the data and indicated annual events, such as changes in the government’s insurance coverage policies.
Methods
Data source
We used population-based data from the National Health Insurance Service (NHIS), operated by the Health Insurance Review and Assessment Service, a universal health reimbursement insurer that covers 98% of the Korean population. The database includes information on not only the clinical characteristics of the cohort, but also the prescribed diagnostic tests and treatments covered by the NHIS. The information from the first inpatient claims data, registered with diagnostic codes related to preterm births, was used.
Study design
This is a retrospective cohort study to assess the trends in healthcare utilization and medical costs associated with preterm births, covered by the NHIS from January 1, 2007, to February 28, 2021. Neonates, who were registered with diagnostic codes related to prematurity in 2007, were excluded as a washout period owing to possible delays in receipt registration. Additionally, because the 2021 data included information for only two months, we excluded that year from the study as well. Further, multiple claims data from the same patient were excluded to include only the claims data for the first prematurity-related hospitalization.
The outcomes on length of hospitalization and medical costs using operational definitions, such as medication and laboratory, radiological, and functional examinations, were analyzed using gestational age (GA) and birth weight.
Study population
We included those with prematurity-related codes of International Classification of Diseases and Related Health Problems, 10th edition (ICD-10), and included multiple births. As extreme preterm birth or birth at < 28 weeks of GA is associated with higher mortality and morbidity, we categorized prematurity into extremely preterm (P07.2 on ICD-10) and non-extremely preterm (P07.3 on ICD-10).
Statistical analysis
We divided preterm infants into extreme (less than 28 gestational weeks) and non-extreme (gestational weeks between 28 and 37) preterm birth groups. Thereafter, we compared these two groups according to baseline characteristics, length of hospitalization, medical costs, and proportion of re-hospitalization. Categorical variables were expressed as frequencies and percentages (%) and were compared using the chi-square test. Continuous variables were expressed as mean and standard deviation (SD) or medians (first quartile(Q1), third quartile(Q3)), and compared using the independent t-test or Wilcoxon rank-sum test, respectively. Statistical significance was defined as a two-sided P-value of < 0.05. Statistical analyses were performed using the SAS Enterprise Guide version 7.1 (SAS Institute Inc., Cary, NC, USA).
Ethics statement
This study was conducted in accordance with the World Medical Association and the Declaration of Helsinki, and the Institutional Review Board (IRB) of Severance Hospital, Yonsei University, Seoul, Republic of Korea (No. 4-2021-0416) approved the study. The IRB of Severance Hospital has waived the requirement for informed consent due to the minimal-risk nature of the research.
Data availability
The data that support the findings of this study are available from National Health Insurance Service (NHIS), operated by the Health Insurance Review and Assessment Service of Government of Republic of Korea. But restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the corresponding author upon reasonable request and with permission of NHIS.
Results
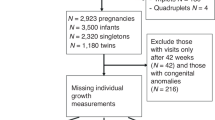
From 2008 to 2020, a total of 5,312,886 live births were declared, among which 137,214 infants were claimed as diagnosis of premature born infant. We excluded 46,639 infants who were only claimed as outpatient clinics and have not been hospitalized (Fig. 1). Table 1 shows the characteristics of preterm births. A slight male predominance was observed in preterm neonates (54.0%, P < 0.001). The number of preterm births more than doubled from 3722 (4%) in 2008 to 9,009 (9.9%) in 2020 (P < 0.001), with a similar frequency across the seasons. About 99% of the preterm births, were covered by the NHIS, and 47% of preterm birth deliveries were observed in the main urban areas in Korea, such as Seoul and the suburban Gyeonggi province.

Flow chart of the study population.
Medical burden of preterm singleton birth hospitalization
We analyzed the medical costs associated with hospitalization for preterm births at 28 weeks GA and birth weight. The median length of hospitalization for extremely preterm singleton neonates was almost twice that for preterm infants older than 28 weeks GA (40 days, IQR 28–60 vs. 21 days, IQR 11–35, P < 0.001) (Table 2). The mean medical cost per patient was higher for the extremely preterm group than for those born after 28 weeks ($33,872.2, SD $24,369.2 vs. $12,713, SD $13,078.8). When the cost was categorized according to medication and type of diagnostic examination, the former accounted for the majority of the cost in both, extremely preterm and other preterm neonates ($2383.5, SD $1486.2 vs. $802.0, SD $1136.1), but at a slightly higher proportion in the extremely preterm group (43.2% vs. 37.4%, P < 0.001). Moreover, the cost of laboratory examinations was the major source of expenses for diagnostic tests, such as radiological and functional examinations, in both the GA groups (63.7% vs. 59.4%, P < 0.001).
Trend in healthcare costs of preterm singletons
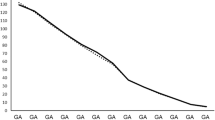
Figure 2 illustrates the annual trends in healthcare-related costs from the hospitalization of preterm neonates between 2008 and 2020. Overall, the total medical cost per patient almost tripled in all preterm newborns ($7,390.90 to $20,209.59), but that of extremely preterm < 28 weeks increased fourfold ($13,961.03 to $55,984.47), Fig. 2A). The medication cost was constant for all preterm births over time; however, it increased in case of the extremely preterm group (Fig. 2B). In contrast, laboratory examination costs were minimal until 2017, after which they increased significantly, especially in the extremely preterm group (Fig. 2C). Expenses due to radiological examinations showed a similar trend, increasing after 2016 (Fig. 2D). Finally, the cost of functional examination showed a steady increase over time, with a more prominent slope for the extremely preterm group (Fig. 2E).

Trends in healthcare costs of preterm infants by year, 2008–2021. (A) Total medical cost ($) (B) medication cost ($), (C) laboratory diagnostic test cost ($) (D) radiological/imaging exam cost ($), (E) functional examination cost ($).
Readmission rate in preterm singleton neonates
Among 90,575 preterm births, 56,600 (62.5%) were readmitted within 90 days of the initial discharge (Table 3). The readmission rates were relatively similar between the extreme and non-extreme preterm groups (65.9% vs. 62.2%). However, the proportion of the extremely preterm group readmitted within 30 days of discharge was twice that of the non-extremely preterm group (16.1% vs. 8.32%; P < 0.001). The odds of readmission within 30 days of extremely preterm group were more than twice as non-extremely preterm group. Regarding the expenses due to rehospitalization, the total cost was approximately 1.5 times greater in the extremely preterm group (mean $4,293.8 vs. $2,975.4, P < 0.001).
Discussion
The preterm birth rate has increased, whereas the total number of live births in South Korea has decreased. The total number of preterm infants has increased slightly. Preterm births under 28 weeks of GA increased until 2015, to 752 infants, and declined after 2015. Earlier GA was strongly associated with increased healthcare resource utilization and medical costs in Korea, especially in the extremely preterm group10.
The total medical costs of preterm infants steadily increased throughout the study period. In 2008, the Korean Ministry of Health and Welfare established “The Service for National Support of NICU Installation and Management.” An agreement for raising the admission fee for the NICU was signed in 2013, which included a zero-deductible payment for the patient and the entire admission fee for patients requiring incubators. This development solved chronic deficits for hospitals running the NICU and contributed significantly to the healthcare of preterm infants by lowering neonatal mortality11,12. In the 2016 policy revision (The 14th National Healthcare Insurance Policy Board Congress), guaranteed admission fees were increased again and provided an expanded non-benefit practice. This increase remains significant when considering the Gross Domestic Product (GDP) per capita, which rose from $21,350 to $32,721 between 2008 and 202013.
Additionally, the costs of diagnostic tests and treatments have changed over time. However, the cost of medication has remained constant over time, including that of pulmonary surfactants and respiratory syncytial virus monoclonal antibodies (Synagis®, palivizumab), which are covered by national insurance since 201011,14,15. In 2018, more diverse surfactant agents were included in the national health coverage (other than Curosurf). Laboratory diagnostic costs have increased steeply since 2017. A new laboratory methodology called next-generation sequencing was included in the national insurance coverage for newborn congenital diseases from March 201716. Also, respiratory viral panel by polymerase chain reaction study has been included in the coverage since 2016. The expansion of laboratory studies performed in NICU has led to a dramatic increase in the costs in the laboratory category.
Ultrasonography is a useful imaging modality for neonates. Sonographic examinations have been covered by national insurance since 2016 and are routinely performed through discretionary grant payments from each patient. This coverage contributed to a steep increase in radiological costs from 2016. Other functional examinations, including electroencephalography, echocardiography, or video fluoroscopic swallowing studies, remained steady because fees were not raised during the study period.
Several previous works about economic burden with preterm birth have been investigated. Canada runs national health insurance model which is comparable with South Korea. Johnston et al., estimated in his paper that it costed $CAD 67,467 for each early preterm infant (less than 28 gestational weeks), $CAD 54,554 for moderately preterm (28–32 gestational weeks) and $CAD 10,010 for late preterm (32 to 36 gestational weeks) in year 201217. Rolnistsky et al., published 2 papers related to expenses of the NICU care in Canada. In these studies, extremely preterm infants (less than 28 gestational weeks) accounted $CAD 66,669 in 2011 through 2015 and in year 2010 through 2017, and total median cost per all NICU infant was $CAD 77,13218,19. Healthcare spendings in U.S. was even larger than national covered nations. Beam et al., reported median $291,029 expenditure was spent for each preterm infant born with 27 to 28 gestational weeks of age, $418,191 for 25–26 gestational weeks and $9,864 for 35 to 36 gestational weeks in year 2008 to 201620. Beam et al., also suggested that total cost has been rising through recent years as well.
Comparing with our data, it costed $29,101 for extremely preterm infant which is less than Northern American nations. But it is also noticeable that in non-extreme preterm, expense was $9,181 per infant, which was similar amount compared to previous studies from other nations. As total burden of preterm medical cost increases, we need more wisdom to invest strategies to address more portion to target earlier born infants.
While increasing medical burdens has been displayed throughout the entire study period, patient outcome improvement also been noted from Korean Neonatal Network (KNN) reports21. According to the KNN 10-year anniversary report, the survival rate increased from 84.9 to 89.3% between 2014 and 2020 and associated preterm morbidities have significantly decreased over the past decade. The 2020 Canadian Neonatal Network (CNN) report indicated a mortality rate of 90.5%.22 Given that the lower limit for resuscitation has remained consistent between two national cohorts past years, generally around 22–23 weeks of gestational age, this represents a significant improvement and is comparable to international standards.
Jin et al., studied first 6 years medical costs in preterm infants after discharge from NICU in Korea10. Rate of hospital admission was 75.6% in infants born less than 28 gestational weeks in 6 years and most of the costs was spent in the first year after discharge. In our data, we focused more on advanced period and re-admission happened 16% in 30 days, 24% in 60 days and 29% in 90 days after discharge in extremely preterm infants.
This study has multiple strengths including large population size, distribution of birth location and categorized expenditure by different purpose of medical utilization. However, several limitations should be acknowledged. Korean national insurance coverage is not 100% and there could be missing expenditure from uninsured portion from arbitrary out-of-pocket expenses. Second limitation is from weakness of the large claim data. We utilized ICD-10 codes to search preterm admission bills, but codes may not be perfect as incomplete data input may occur from different units. Third, large scale national data does not include patient’s individual data other than gestational age other than 28 weeks cut-offs and specific birth weight information. Fourth, different neonatal intensive care circumstances, clinical features, and disease spectrums may vary between countries. Our data only includes the South Korean population, which could make our results less generalizable to countries with different circumstances outside of South Korea. Lastly, our data claim started from the baby’s perspective, which limited the inclusion of maternal healthcare data. According to the Korean National Statistics Agency, the average maternal delivery age in South Korea has increased from 31.4 to 33.4 over the past ten years23. This change may have affected the overall outcomes and expenditures of neonatal intensive care. However, integrating maternal data was restricted due to unresolved confidentiality issues during our investigation. Recently, improved methodologies have been developed. Future studies that integrate maternal data will be more promising in terms of better adjustment of confounders.
Conclusion
Preterm births have increased, while the total number of live births in Korea has been declining to concerning levels. In recent decades, medical costs and national insurance coverage for preterm infants have risen across all categories. This increase can be attributed not only to the growing rate of preterm births but also to advancements in medical technology and rising parental demand. Further attention should be paid to improving preterm healthcare and alleviating the medical burden of preterm births at a national level.
References
Boardman, J. P. Preterm birth: Causes, consequences and prevention. J. Obstet. Gynaecol. 28, 559–559 (2009).
Russell, R. B. et al. Cost of hospitalization for preterm and low birth weight infants in the United States. Pediatrics 120, e1–9 (2007).
Martin, J. A. et al. Births: Final data for 2003. Natl. Vital Stat. Rep. 54, 1–116 (2005).
Goldenberg, R. L., Culhane, J. F., Iams, J. D. & Romero, R. Epidemiology and causes of preterm birth. Lancet 371, 75–84 (2008).
Mortality, G. B. D. & Causes of Death, C. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 388, 1459–1544 (2016).
Chawanpaiboon, S. et al. Global, regional, and national estimates of levels of preterm birth in 2014: A systematic review and modelling analysis. Lancet Global Health 7, e37–e46 (2019).
Juan, J. et al. Effect of coronavirus disease 2019 (COVID-19) on maternal, perinatal and neonatal outcome: SYstematic review. Ultrasound Obstet. Gynecol. 56, 15–27 (2020).
Hedermann, G. et al. Danish premature birth rates during the COVID-19 lockdown. Arch. Dis. Child. Fetal Neonatal Ed. 106, 93–95 (2021).
Hwang, J. et al. Changes in preterm birth and birthweight during the SARS-CoV-2 pandemic: A nationwide study in South Korea. Sci. Rep. 12, 16288 (2022).
Jin, J. H., Lee, S. A. & Yoon, S. W. Medical utilization and costs in preterm infants in the first 6 years of life after discharge from neonatal intensive care unit: A nationwide population-based study in Korea. J. Korean Med. Sci. 37, e93 (2022).
Bae, C. W. The history of neonatology in Korea. J. Korean Med. Assoc. 59 (2016).
Shim, J. W., Jin, H. S. & Bae, C. W. Changes in survival rate for very-low-birth-weight infants in Korea: Comparison with other countries. J. Korean Med. Sci. 30(Suppl 1), 25–34 (2015).
World Bank Open Data & Washington DC, USA. Available from: https://www.worldbank.org/.
Singh, D., Rana, K. S. & Mathai, S. Role of prophylactic surfactant in preterm infants. Med. J. Armed Forces India 67, 138–141 (2011).
Park, S. K. et al. Effect of synagis® (palivizumab) prophylaxis on readmission due to respiratory syncytial virus in very low birth weight infants. Korean J. Pediatr. 53 (2010).
OECD. (Health at a Glance, 2017).
Johnston, K. M. et al. The economic burden of prematurity in Canada. BMC Pediatr. 14, 93 (2014).
Rolnitsky, A., Unger, S., Urbach, D. & Bell, C. M. The price of neonatal intensive care outcomes - in-hospital costs of morbidities related to preterm birth. Front. Pediatr. 11, 1068367 (2023).
Rolnitsky, A., Unger, S. L., Urbach, D. R. & Bell, C. M. Cost of neonatal intensive care for extremely preterm infants in Canada. Transl. Pediatr. 10, 1630–1636 (2021).
Beam, A. L. et al. Estimates of healthcare spending for preterm and low-birthweight infants in a commercially insured population: 2008–2016. J. Perinatol. 40, 1091–1099 (2020).
KNN 10th Anniversary Report 2013–2022. The Korean Neonatal Network. (2022).
CNN 2020 Annual Report. The Canadian Neonatal Network. (2020).
Microdata integrated service & Daejeon Korea: MDIS [cited 2022 Jun 21]. (2022). Available from: https://mdis.kostat.go.kr/index.do).
Acknowledgements
We used data from the National Health Information Database (M20210702352) of the Health Insurance Review and Assessment Services.
Funding
This study was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. 2022R1G1A100844111) and the faculty research grant of Yonsei University College of Medicine (6-2021-0145). The study sponsor was not involved in the study design, analysis and interpretation of data, writing of the report, or the decision to submit the study results for publication
Author information
Authors and Affiliations
Contributions
Conceptualization: All authors. Data Curation: M.L. and M.H. Formal analysis: M.L., M.H., and I.J. Funding acquisition: J.G.A. Investigation: All authors. Methodology: M.L., M.H., I.J., J.G.A., and M.S.P. Software: M.L., M.H. Validation: J.P., J.G.A., J.Y.L., I.J., and M.S.P. Visualization: M.L. Writing the original draft: J.P. and J.Y.L. Writing, review, and editing: J.P., J.Y.L., and M.L.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Lee, J.Y., Park, J., Lee, M. et al. Rising public costs of preterm infant hospitalization in South Korea from a nationwide observational study. Sci Rep 15, 14357 (2025). https://doi.org/10.1038/s41598-025-98868-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-98868-2
