
Abstract
The main objective of this study was to analyze the effect of a resistance training program using outdoor fitness equipment (OFE) on sagittal spine disposition and pelvic tilt in middle-aged and older adults. One hundred and twenty-eight middle-aged and older adults were randomly assigned to the training (TG) or control group (CG). The TG trained for 8 weeks, with 2 weekly sessions of one hour of resistance circuit training with OFE. Before and after the intervention, the sagittal spine disposition and pelvic tilt in the relaxed standing and sitting positions were analyzed. The results showed that the TG obtained a significant reduction (p < 0.001) in all the curvatures of the sagittal spine disposition and pelvic tilt in the standing position after the intervention, in contrast to the CG, which only showed a significant reduction in pelvic tilt (p = 0.005). Regarding the sitting position, only the TG presented a significant decrease in lumbar lordosis (p < 0.001). In conclusion, resistance training with OFE may be useful in improving sagittal spine disposition in middle-aged and older adults. Given the availability of free OFE in parks, the present research provides elders with an accessible and effective training program to curb the effects of ageing on the sagittal spine disposition.
Similar content being viewed by others
Introduction
Current scientific evidence describes an increase in thoracic curvature while standing as a person ages1,2,3, without a clear trend for lumbar curvature in the standing position in this population. While some studies find that it often flattens during this stage, other studies show that it increases4,5,6. Not surprisingly, previous studies have found that 20–40% of older adults have thoracic hyperkyphosis in the standing position7,8,9, with the incidence of older adults showing hyperlordosis in the standing position also being high9.
This increase has been linked to a poorer health status, characterized by respiratory problems, greater loss of physical function, lack of mobility, risk of falling, back pain in general, and low back pain in particular, and even mortality1,10,11,12,13,14,15. In addition, pathologies such as spondylolysis, spondylolisthesis or degenerative changes in the intervertebral discs have also been linked to spine misalignments16,17.
One of the factors that could be associated with the increase in sagittal curvatures of the spine beyond the normal range with age is the loss of physical conditioning1. A relationship has also been found between changes occurring in the sagittal spine disposition and loss of strength12,18,19,20,21. Specifically, it has been found that a deficit in the strength of the extensor muscles of the trunk is related to an increase in thoracic hyperkyphosis and hyperlordosis or rectification of the lumbar area, as well as an alteration of the lumbo-pelvic dynamics1,13,19,20. In addition, strength deficits in the trunk muscles, with the subsequent changes in the sagittal spine disposition, increase the risk of suffering from some pathologies such as herniated discs11.
As a result of the aforementioned factors, various studies have suggested the implementation of comprehensive exercise training programs, with a specific emphasis on resistance training to enhance sagittal spinal disposition22,23,24. Thus, most of these studies have implemented multicomponent programs, usually including stretching or postural hygiene exercises together with resistance work as well14,25. Therefore, the effect of exclusive resistance training on the sagittal spine disposition is lightly studied but promising14,26,27,28. In addition, very few of these studies have focused on the adult/older population26,27,28,29. Likewise, reviews on the effect of strength training on spinal disposition have shown that a full body circuit based on different types of overload training, such as using gym equipment, dumbbells, or weighted backpacks, can improve thoracic aligment in elders as long as sufficient overload and training volume is achieved30. This could be due to the fact that in most of these interventions, the trunk musculature is not worked on exclusively, but most of the exercises focus on the upper and lower limb musculature, with the trunk musculature being involved as a synergist, so that the generation of sufficient overload seems to be a limiting factor in the effects of these interventions on the sagittal spine disposition30. However, these interventions have been focused on different methodologies used for strength training, such as gym equipment, self-loading exercises, dumbbells, weighted backpacks or elastic bands, with very different results reported between them, which could be due to the differences in the training programs proposed, the training volume, the overloading of the different training systems used, or the characteristics of the population included30.
In this line, despite the many investigations carried out with different types of equipment, including traditional machines31,28, it should be noted that none of these previous studies have used outdoor fitness equipment (OFE) for resistance training. In general, OFE machines are specially designed for adults and older adults, with a friendly design and a simple operation32,33. Many public entities worldwide have used them with the aim of achieving a healthy aging of the population by making access to OFE simple and free of charge34,35. The location of these machines in public spaces and their free-of-charge use, provide greater availability and accessibility as compared to traditional machines. In addition, although they are more oriented towards the elderly population, they are commonly used by people of all age groups33, so that a larger population group in multiple countries34 could benefit from their use over traditional gym machines. In fact, this type of installation has been booming in recent years.
OFE is a very interesting option for guided resistance training with exercise equipment. Theoretically, training with OFE should influence the sagittal spine disposition by strengthening the adjoining and stabilizing trunk and back musculature such as abdominal obliques, rectus abdominis, multifidus, transverse abdominal, quadratus lumborum, erector spinae or dorsal, among others36,37,38. These muscles act as synergists when pulling or pushing with the upper limb, or movements involving hip flexions or extensions, movements for which many OFE are designed39. In fact, previous studies have shown that training on OFE-like machines such as guided gym machines can improve sagittal spine posture as a result of the activation generated by these machines in synergist muscles that act as stabilizing musculature of the trunk and back25,30,40,41,42. However, although OFE machines are training devices with certain similarities to traditional gym machines, unlike traditional gym machines in the OFE the user’s own weight is used as the load by means of a system of levers37,43. Previous studies have shown that their use can improve body composition and functionality, and increase strength in arms and legs39. Furthermore, OFEs have been designed without regard to safety or ergonomic principles35. This therefore raises the question of whether the OFE machines can achieve long-term beneficial effects on the sagittal disposition of the spine despite their design, or provide sufficient stimulus, as has been found with other strength training systems27. It is therefore essential to know the effects of training with this type of equipment on the sagittal spine disposition.
Therefore, the aim of the present study was to analyze the effect of a resistance training program using OFE on the sagittal spine disposition and pelvic tilt of middle-aged and older adults. The hypothesis of the present study is that resistance training with OFE will improve the sagittal spine disposition and pelvic tilt of middle-aged and older adults.
Materials and methods
Study design
The present study is an 8-week randomized controlled trial. The trial design was registered with ClinicalTrial.gov (identifier: NCT04958499) and followed the Consolidated Standards of Reporting Trials (CONSORT) guidelines and the Template for Intervention Description and Replication (TIDieR) checklist. The research was conducted in accordance with the Declaration of Helsinki. Approval was obtained from the Ethics Committee of the Universidad Católica San Antonio de Murcia (Ethical Application Ref: CE111908) before the start of the project. All participants were informed of the study evidence as well as any potential risks and possible adverse effects, and voluntarily signed an informed consent form prior to the measurements and intervention, and also provided their consent to have their photographs taken for subsequent publications.
Participants
The minimum sample size necessary for the study’s development was calculated using Rstudio 3.15.0 software (Rstudio Inc., USA), and followed the methodology employed in previous studies44, which also provided the standard deviation (SD) from prior studies that measured thoracic kyphosis in standing position for a sample of older adults (SD = 8.5º)26. This standard deviation was chosen after selecting a study that showed a sample similar to the present one. In addition, to be conservative, a standard deviation that was slightly higher than the norm was used to ensure the sample and power size. With an estimated error (d) of 2.12, a confidence interval of 95%, a significance power of 95% (1-β = 0.95), and a significance level of 0.05, the required sample size was determined to be 62 volunteers. To be cautious and to avoid a high sample loss after the end of the intervention, a dropout rate of 20% was assumed, based on previous studies26,45 that had similar characteristics to the present one. Thus, a minimum of 74 participants per group was required.
The participants were recruited on a voluntary basis through informative conferences and advertising in different senior centers in the Region of Murcia (Spain). The inclusion criteria were: a) being over 50 years of age; and b) not performing resistance training or physical exercise regularly. The exclusion criteria were: a) suffering from any spinal disorder or injury that prevented the performance of the measurements and/or training; b) having undergone surgery that prevents/poses a risk towards performing any of the tests and/or training; c) presenting any neurological, cardiovascular, musculoskeletal or metabolic alterations at the time of the measurement/training; d) missing the post-test evaluations; and e) starting to perform physical exercise systematically during the time of the study. The final sample consisted of 128 middle-aged and older adults, 46 men (mean age: 60.50 ± 5.96 years) and 82 women (mean age: 58.04 ± 7.62). They were randomized into the training group (TG) (n = 64; 24 males and 40 females; mean age: 60.02 ± 7.25 years) and control group (CG) (n = 64; 22 males and 42 females; mean age: 57.83 ± 6.92 years). The CONSORT flow diagram is shown in Fig. 1.

CONSORT flow diagram. CONSORT flow diagram showing the flow of participants through each stage of the study.
Randomization and blinding
After the recruitment and selection of the sample, the participants were assigned to the different groups. The group assignment was blinded and was carried out using a computer-generated random number table by a researcher in the presence of other researchers unrelated to the present investigation. Two groups were established according to the thoracic curve, as in previous research46, and then a random sequence was generated to create the groups by stratified randomization. The researchers who performed the spinal measurements were not present at the training sessions. The two researchers involved in data collection were also cross-blinded in the measurements, where one carried out the measurement using the device, while the other was only responsible for verifying the correct recording of the data. During randomization, an attempt was made to keep married couples in the same group, as well as social groups, to increase adherence, following the methodology from previous studies47.
Measurements
The measurements were performed in a sports science laboratory at a standardized temperature of 24 ºC between 10:00 and 14:00 h. The participants were requested to not stretch or warm up prior to the tests. During the measurements, the participants remained barefoot on an insulating mat.
First, the basic variables of body mass and height were measured according to the protocol from the International Society for the Advancement of Anthropometry (ISAK)48. All the measurements were performed by an ISAK Level 1 accredited anthropometrist. A Tanita BC-545N scale (Tanita, Arlington Heights, Illinois, USA) was used to measure body mass. A HR001 portable stadiometer (Tanita, Arlington Heights, Illinois, USA) was used to measure height.
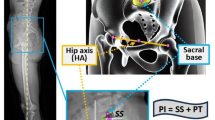
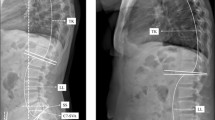
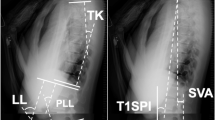
Subsequently, the sagittal spine disposition and pelvic tilt were measured using the Spinal Mouse® system (Idiag, Fehraltdorf, Switzerland). This device allows the angular measurement of the different spinal curvatures in a non-invasive way by means of a wireless device connected to a computer. This tool has shown high intra- and inter observer validity and reliability, with the following correlation coefficients, respectively (0.61–0.96; 0.70–0.93)49. An assessment of the sagittal spine disposition and pelvic tilt in relaxed standing and sitting positions was performed, following the protocol from previous studies50,51. In the standing position, the volunteers stood with their shoulders relaxed, looking forward, with their arms along their trunk, and their feet hip-width apart. For the sitting position, the volunteers were placed in a relaxed sitting position on a box, without thoracic or lumbar support, with their hands resting on their thighs, and with their knees bent at 90º. A positive value implied a pelvic kyphosis/anteversion, while a negative value implied a pelvic lordosis/retroversion. All the assessments were performed by the same measurer, who had previous experience in performing similar interventions.
Intervention
The intervention program was carried out in an OFE circuit, consisting of eight OFE machines (Bonny rider, Air Walker, Surfboard, Row, Parallel bars, Gemini, Flyers wheels and Swing) from the company Entorno Urbano S.L.U (Murcia, Spain), which was located in a private and reserved area for study within the Universidad Católica San Antonio de Murcia, Murcia, Spain.
The TG participants performed a training program using the OFE for 8 weeks, with 2 weekly sessions lasting one hour per session on non-consecutive days. CG participants did not perform any training and were asked to maintain their usual lifestyle. The researchers in charge of conducting the training sessions recorded attendance using Excel software. Average program attendance was 92.75% (min: 78.57%, max: 100%).
The training sessions consisted of resistance circuit training with 11 self-loaded exercises (Table 1) to be performed on the eight OFE machines, following the example from previous research52. In the selection of exercises, it was taken into account that there were exercises that involved the dorsal musculature, hip extensors, scapular approximators or abdominal muscles, among others. The execution speed was set by a metronome53. The training program was designed and supervised by Sports Science graduates with Master’s degrees in Strength and Conditioning Training, Healthy Aging, and Physical Activity and Health. The training protocol performed is described in Table 2. The training load was regulated by time under tension. A digital metronome was used to set the execution rhythm of the concentric and eccentric phases in each OFE54.
Statistical analysis
After analyzing the normality of the variables using the Kolmogorov–Smirnov test, as well as kurtosis, skewness, and variance, Mauchly´s W-test was used to evaluate the sphericity of the data. Two-way ANOVAs with one-way repeated measures were carried out to analyze inter- and intra-group differences. Partial eta squared (η2) was used to calculate the effect size and was defined as small: ES ≥ 0.10; moderate: ES ≥ 0.30; large: ≥ 1.2; or very large: ES ≥ 2.0, with an error of p < 0.0555. A value of p < 0.05 was set to determine statistical significance.
The statistical analysis was performed with the SPSS statistical package (v. 25.0; SPSS Inc., IL).
Results
Regarding the intergroup baseline differences, Table 3 shows homogeneity in the variables age, gender, marital status, level of education, occupation, who they live with, and number of falls in the last year (p > 0.05).
Table 4 shows the pre-post intervention differences in the sagittal spine disposition and pelvic tilt in each of the groups. In the standing position, there was a significant reduction in thoracic kyphosis, lumbar lordosis and pelvic anteversion of the TG after the intervention (p < 0.001). In contrast, the CG showed no significant differences in thoracic or lumbar curvatures (p = 0.863; p = 0.053), although a significant decrease in pelvic tilt (p = 0.005) was observed. There were no significant changes in either the TG or CG in the sitting position results, except for a decrease in lumbar lordosis in the TG (p < 0.001). These results are shown in Fig. 2.

Sagittal spine disposition and pelvic tilt in standing and sitting positions in both measurements for the training group and the control group. Sagittal spine curvatures and pelvic tilt in the pre-test and the post-test for each group. * indicates that the pre-post differences are p < 0.05.
Table 5 shows the differences between the TG and CG in the pre-post change. The TG showed a significantly greater reduction than the CG in thoracic curvature, lumbar curvature, and pelvic tilt in the standing position (p = 0.024–< 0.001). In the sitting position, a greater reduction in thoracic and lumbar curvature was found in the TG than in the CG (p = 0.023–0.002). There was no difference in the change that occurred in the pelvic tilt when sitting between groups (p = 0.607).
Table 6 shows the differences in pre- and post-test changes between standing and sitting positions. Significantly greater reductions in thoracic and lumbar curvatures and pelvic tilt were observed in the standing position than when sitting (p < 0.001).
Discussion
The main objective of the present investigation was to analyze the effect of a resistance training program using OFE on the sagittal spine disposition and pelvic tilt of middle-aged and older adults. The results showed a significant reduction in all curvatures of the sagittal spine disposition in the standing position of the TG after the intervention. In contrast, the CG showed no significant differences in thoracic or lumbar curvatures. In both thoracic and lumbar curvatures, as well as in pelvic tilt, the reduction in the TG was significantly greater than that of the CG.
In accordance with the findings of the current study, previous studies have shown that the systematic performance of multicomponent programs that include general resistance exercises, trunk muscle strengthening, joint mobility exercises, and stretches that target the muscles associated to the trunk, lead to a reduction in sagittal curvatures while in a standing position, following an 8-week training period14,25,56. Similarly, a recent systematic review with meta-analysis concluded that structured physical exercise combining thoracic strength/stabilization, mobility, and flexibility, was an effective intervention for reducing the occurrence of thoracic hyperkyphotic curvatures. However, it suggested that utilizing a multicomponent approach may not be the most optimal strategy for maximizing the desired changes, as the studies reviewed were of low to moderate quality, and more studies on the subject were therefore needed14.
The same trend is found in the older population, where most studies have analyzed the effects of a multicomponent intervention on spinal alignment14,56. However, few studies have demonstrated the effect of a training program based exclusively on guided equipment-based resistance training on the reduction of the sagittal spine disposition in the standing position of middle-aged and older adults28. In that study it was found that a full body work with guided machines can improve thoracic kyphosis, but that on the contrary, a poor selection of guided machines such as core pull and vertical lift exercises and their isometric execution can lead to vertebral fractures28. Another study reported no significant differences, perhaps attributed to the low intensity of the strength program performed with elastic bands27. On the contrary, studies performed on postmenopausal women and men over 45 years of age with a low bone mineral density found that after training similar muscle groups by means of exercises using 80–85% of one maximum repetition, a significant improvement of -6.7 ± 8.2° and -2.3 ± 0.8° respectively, of thoracic kyphosis was observed after eight weeks of training26,28. In contrast, they did not report the effect size using eta squared, so it could not be compared. A previous review indicated that the key to generating changes in the sagittal disposition of the thoracic spine could lie on the volume of training and the selection of devices that provide a sufficient load, especially when the trunk musculature is worked in this type of circuit as a synergistic factor with the rest of the exercises29,30. In light of the results of the present research, this also seems to be the case with OFE, which could provide a sufficient stimulus to generate adaptations in the spine.
The analysis of the sagittal disposition of the spine in the standing position is essential. It is the most used position especially in older people, due to the consequences it has on aspects such as balance and the probability of falling57. It has been observed that an increase linearity can improve people’s balance57,58, and therefore, in our case, the improvement in linearity after training could reduce the risk of falling.
The reduction in sagittal curvatures and pelvic tilt in the standing position after resistance training found in the present study could be due to the fact that during the training session, different strengthening exercises were performed, where the trunk musculature was involved as an agonist or synergist, especially the paravertebral muscles, spinal erectors, latissimus dorsi, rhomboids, and the upper back. In addition, the pectoral and shoulder musculature were involved to improve the function of these muscles and to gain a greater range of joint mobility, with these factors associated with a lower thoracic hyperkyphosis36,43. Previous studies have found that trunk musculature exercises are essential for the correction of spinal misalignments24,25,38,39, which in addition to the results presented in this work, demonstrates that the effects of this type of training can also be extrapolated to the older population. Considering the high incidence of hyperkyphosis and hyperlordosis in this population9, and their consequences on different areas of health10, resistance training could be a great resource that could be used by the older population to reduce the incidence of these pathologies10. In addition, it has been proven that its effect lasts over time; studies in which the strengthening of the spinal extensors was performed, along with other types of exercise, showed that hyperkyphotic women maintained improvements in kyphosis, spinal extensor strength, and physical performance one year after the intervention59. Another study based on a 3-month intervention using low-load training and elastic bands found that 3 years after the intervention, sagittal spine curvatures did not worsen with ageing60. For this reason, training by means of OFE, which in young people has been proven to provide a stimulus similar to low loads37,43, may involve a greater effort in adults, generating an intensity that may result in benefits on the sagittal spine disposition that are maintained over time, with this becoming a topic to be studied in future research.
One of the novelties of the present study was that it assessed the influence of training on the sagittal spine disposition and pelvic tilt also in the sitting position. Sitting is one of the most commonly used positions for spine analysis. It is important to analyze the disposition in this body position in older adults, as this population usually spends long periods sitting, up to 60% of their waking time61. It has been shown that the sitting position produces greater intradiscal pressure than when standing, and that the loss of spinal linearity further increases the stress on the annulus fibrosus, nucleus pulposus, and cortical bone62. Other studies also found that greater lumbar flexion increased intradiscal pressure and antero-posterior compressive and shear stress, which together with prolonged sedation with an inversion of the lumbar spine, increases the capacity for intervertebral flexion due to the viscoelastic deformation of the ligaments of the posterior arch of the vertebrae63. It is for this reason that poor ergonomic positions when sitting can compromise the inversion of the lumbar area to a greater extent, and increase the laxity of the thoracolumbar ligament, which can lead to acute deformations, or chronic ones in the case of being maintained over time, as in the case of the elderly and the long periods of time spent sitting61. These aspects may influence the health of middle-aged and older adults38. For all of these reasons, previous studies have pointed out that it is necessary to analyze the sagittal spine disposition and pelvic tilt in different positions, beyond the exclusive evaluation in the standing position9.
Previous studies showed that OFEs force their users to adopt certain postures with the sagittal spine disposition and pelvic tilt involved during their use35, but this is the first study to verify the effects of their continued use. In the present study, when sitting, a decrease in lumbar lordosis was found in the TG, with a greater disposition in the participants who performed the resistance work as compared to those who did not train. The results found, such as those in the standing position, could be due to the fact that the implementation of a muscle strengthening program reduces the incidence of spinal misalignments24,25,56,64, although this is the first study to demonstrate that this improvement in spinal alignment goes beyond the standing position. In light of these results, resistance training in middle-aged and older adults could improve the sagittal spine disposition in both standing and sitting positions, and may also result in less disc tension62 and viscoelastic deformation of the ligaments of the posterior arch of the vertebrae63.
This study also compared the evolution of the curvatures in standing and sitting positions. It was found that the changes produced in the spine through training with OFE were observed, to a greater extent, in the standing position than in the sitting position. The standing position depends to a great extent on muscular tolerance65,66. Previous studies have suggested that low muscle tolerance of the extensor and stabilizing muscles of the trunk is related to poorer postural hygiene in standing65,66. This could be because, as these muscles fatigue, the latency of muscle activation increases, and fewer bundles of muscle fibers are activated66,67. This leads to less muscular opposition to the effect of gravity, resulting in misalignments from the sagittal spine disposition68. Muscle tolerance can be modified with training65,68. More specifically, previous studies have found that resistance training with machines, by generating an activation of the stabilizing muscles of the trunk as synergists maintained over time, increases the muscular tolerance of these muscles69. This could lead to greater tolerance of these muscles in their tonic function of maintaining adequate postural hygiene when standing, improving the sagittal spine disposition in this position68.
On the contrary, the sitting position usually depends directly on postural hygiene and more specifically the pelvis disposition70,71. Previous studies have suggested that the pelvis tilt is the main factor determining factor for the sagittal spine disposition in a sitting position70,71. This could lead to the tolerance of the extensor muscles of the trunk having less influence on the sagittal spine disposition in this position72. Therefore, programms that only work on muscle strengthening, as is the case with the present intervention, could have little effect on the sagittal spine disposition when sitting. And the fact is that, unlike other studies, the focus of this intervention was not the direct work on postural hygiene but the strengthening of the musculature.
Because of all of the above, the improvement of the sagittal spine disposition in sitting position could depend on the ergonomics and postural hygiene of the person rather than on other intrinsic aspects such as muscle tolerance73. On the other hand, the changes could depend more on muscle tolerance in standing65,66. This could explain why changes shown in the present research are reflected to a greater extent in the relaxed standing position. However, in the absence of previous studies that analyzed the effects of strength training on the sagittal spine disposition in both standing and sitting positions in older people, further studies on this topic are needed.
Regarding the clinical relevance of the changes found in the current study, previous studies showed that an improvement of 2.8º in the thoracic curvature angulation was relevant from a clinical point of view46. Therefore, since the changes produced by the training were greater than 2.8º of angulation, OFE are deemed as an effective means to achieve an alignment of the sagittal spine disposition. In addition, given that the angle of kyphosis thoracic can increase by 2.6º in three years, 3.9º in four years, and 7º in fifteen years in elders74; a reduction close to 5º, as was found in the present investigation, could be considered not only a method of restraining the effects of the passage of time, but also an improvement with respect to the change due to ageing. These improvements could bring benefits such as improved balance, a reduced risk of falling, an improved respiratory capacity, increased mobility, reduced back pain, and reduced pain in the entire back1,10,11,12,57,58. On the other hand, an intervention of longer duration with OFE could obtain better results, so it would be important to analyze this in future studies.
In summary, it can be observed that OFE can provide a sufficient stimulus to improve spinal curvatures in the standing position, but with a lesser effect in the sitting position after an 8-week intervention. On the other hand, these machines demonstrated their ease-of-use with the elderly population, achieving a high adherence by the participants. In addition, the availability of OFE facilities in multiple parks makes it possible for older people to train on their own, following the training schedule pattern used in the present research, which could improve the sagittal spine disposition in this population in light of the results of the present research. Nevertheless, there are also some barriers, such as the possible poor condition of public OFE due to banditry, as well as the dependence on the weather for their use. In addition, the lack of knowledge on the proper way to train with this type of machine can lead to their inadequate or inefficient use33.
Regarding the effect size, this study obtained an eta squared of 0.432 in the variable thoracic curvature in relaxed standing position after the intervention performed using OFE. It was found that interventions which consisted of a program of strength, mobility and postural training exercises specifically designed to treat hyperkyphosis in older adults with a similar distribution of training, with two weekly sessions of one hour for 3 months, showed similar value (effect size: 0.419) in the kyphosis variable in standing29. Another study focused on the training of people over 65 performed for 6 months two types of training, one aimed at the extensor muscles of the back and another group that performed an exercise program for the whole body, both using their own body weight and increasing the load with elastic bands or light weights, performing at least a seminal session of between 20 and 30 min75. The results contrasted with those presented in this article, since even though the effect size on thoracic kyphosis was greater in the group that did back extensor strengthening protocol with respect to the OFEs (0.62 VS 0.432), in lumbar curvature and pelvic tilt the OFEs obtained a greater or similar effect respectively ES (0.19 Vs 0.205 and 0.06 Vs 0.434, respectively) with an intervention of only 8 weeks.
Despite the novelty of the present research, it is not without limitations. The first limitation of the present study was the sample size, although it was larger than that found in similar studies14,27. In addition, although participation was not limited, a greater number of female volunteers was present, while the male sample was relatively small. Therefore, it was not possible to analyze differences in the effects of resistance training as a function of sex. Therefore, the present results should be extrapolated with caution and may not be extrapolated to populations other than the one presented in this study. In this line, future studies are needed to analyze whether the effect of OFE training on sagittal spine disposition in elders could be influenced by gender. On the other hand, at the time of blinding, due to the design of the study, it could not be applied to the researchers who conducted the training sessions. Another limitation was that the OFE does not allow the external load to be regulated, as they are mostly machines that work with the user’s own body weight. Therefore, the evolution of training could not be based on an increase in load, which could be a future line of research. On the other hand, in the current study, the control group maintained their usual lifestyle, and they did not carry out any systematic training. Therefore, there was no traditional machine training group. As a consequence, the design of the present investigation did not analyze whether the effects of OFE training on sagittal spine disposition and pelvic tilt may differ from those achieved with conventional resistance training with gym equipment. This precluded determining the strength of the effects of OFE with respect to other machines, but even so, their effect was tested in comparison with the usual life of the control population. This is an important line for future studies.
Based on these limitations and according to the findings of the present study, a recommendation is given to analyze and compare different population groups with special emphasis on differentiation, taking into account the age and the gender of the subjects. It will also be important to perform both standing and seated measurements and to include a comparative analysis. In addition, the use of OFE in interventions where it is combined with other types of exercises, such as stretching or other exercises aimed at improving balance, could enrich our knowledge on OFE. And having a training group with traditional machines in order to compare the strength of the OFE effect could provide more information. Another type of intervention proposed for future research is one in which the load on the OFE can be regulated in order for this factor to be taken into account. Finally, for these interventions, their long-term effects must also be assessed.
Conclusions
After 8 weeks, at a rate of two sessions per week of circuit resistance training with OFE, a better alignment of the thoracic and lumbar spine and pelvic tilt in the standing position was found in middle-aged and older adults. The lumbar curvature in the sitting position was also found to be improved after the training program. These results suggest that programmed training using OFE can be a useful tool for the improvement of the health of older adults, specifically their spine, with only two weekly sessions of circuit resistance training.
The findings of this study highlight the potential for OFE to serve as an accessible and effective tool for improving spinal spine disposition and pelvic tilt among older adults and to reduce age-related spinal misalignments. Communities and policymakers can use these insights to promote health by integrating OFE into public parks and recreational areas, creating safe and well-maintained spaces for older populations to engage in resistance training. Additionally, offering training sessions or reading materials on how to use OFE effectively may address barriers such as a lack of knowledge and ensure proper ergonomic postures.
Data availability
The data presented and/or analysed in this study is available on request from the corresponding authors.
References
Ailon, T., Shaffrey, C. I., Lenke, L. G., Harrop, J. S. & Smith, J. S. Progressive spinal kyphosis in the aging population. Neurosurgery 77, S164–S172 (2015).
Ohyama, S. et al. Sarcopenia is related to spinal sagittal imbalance in patients with spinopelvic mismatch. Eur. Spine J. 28, 1929–1936 (2019).
Urrutia, J. et al. Mid and lower thoracic kyphosis changes during adulthood: The influence of age, sex and thoracic coronal curvature. Arch. Orthop. Trauma Surg. 142, 1731–1737 (2022).
Ostrowska, B., Rożek-Mróz, K. & Giemza, C. Body posture in elderly, physically active males. Aging Male 6, 222–229 (2003).
Grabara, M. Effects of 8-months yoga training on shaping the spine in people over 55. Biomed. Hum. Kinet. 5, 59–64 (2013).
Arshad, R., Pan, F., Reitmaier, S. & Schmidt, H. Effect of age and sex on lumbar lordosis and the range of motion. A systematic review and meta-analysis. J. Biomech. 82, 1–19 (2019).
Kado, D. M., Huang, M., Karlamangla, A. S., Barrett-Connor, E. & Greendale, G. A. Hyperkyphotic posture predicts mortality in older community-dwelling men and women: A prospective study. J. Am. Geriatr. Soc. 52, 1662–1667 (2004).
Kado, D. M., Prenovost, K. & Crandall, C. Narrative review: Hyperkyphosis in older persons. Ann. Intern. Med. 147, 330 (2007).
Pai, A. et al. Estimation and assessment of sagittal spinal curvature and thoracic muscle morphometry in different postures. Proc. Inst. Mech. Eng. H 235, 883–896 (2021).
Wong, A. Y., Karppinen, J. & Samartzis, D. Low back pain in older adults: Risk factors, management options and future directions. Scoliosis Spinal Disord. 12, 14 (2017).
Arja, H., Tiina, K., Ulla Pt, T. & Jari, Y. Trunk muscle strength in flexion, extension, and axial rotation in patients managed with lumbar disc herniation surgery and in healthy control subjects. Spine (Phila Pa 1976) 28, 1068–1073 (2003).
Imagama, S. et al. Influence of spinal sagittal alignment, body balance, muscle strength, and physical ability on falling of middle-aged and elderly males. Eur. Spine J. 22, 1346–1353 (2013).
Kasukawa, Y. et al. Age-related changes in muscle strength and spinal kyphosis angles in an elderly Japanese population. Clin. Interv. Aging 12, 413–420 (2017).
Jenkins, H. J., Downie, A. S., Fernandez, M. & Hancock, M. J. Decreasing thoracic hyperkyphosis—Which treatments are most effective? A systematic literature review and meta-analysis. Musculoskelet. Sci. Pract. 56, 102438 (2021).
Roghani, T. et al. The association between physical function and hyperkyphosis in older females: A systematic review and meta-analysis. J. Geriatr. Phys. Ther. 47, 85–96 (2024).
Ames, C. P. et al. Adult spinal deformity: Epidemiology, health impact, evaluation, and management. Spine Deform 4, 310–322 (2016).
Been, E. & Kalichman, L. Lumbar lordosis. Spine J. 14, 87–97 (2014).
Rissanen, A., Kalimo, H. & Alaranta, H. Effect of intensive training on the isokinetic strength and structure of lumbar muscles in patients with chronic low back pain. Spine (Phila Pa 1976) 20, 333–339 (1995).
Hongo, M., Miyakoshi, N., Shimada, Y. & Sinaki, M. Association of spinal curve deformity and back extensor strength in elderly women with osteoporosis in Japan and the United States. Osteoporos. Int. 23, 1029–1034 (2012).
Mika, A., Unnithan, V. B. & Mika, P. Differences in thoracic kyphosis and in back muscle strength in women with bone loss due to osteoporosis. Spine (Phila Pa 1976) 30, 241–246 (2005).
Liang, C. et al. Spinal sagittal imbalance in patients with lumbar disc herniation: Its spinopelvic characteristics, strength changes of the spinal musculature and natural history after lumbar discectomy. BMC Musculoskelet. Disord. 17, 305 (2016).
Glassman, S. D. et al. Nonsurgical resource utilization in adult spinal deformity. Spine (Phila Pa 1976) 31, 941–947 (2006).
Kernc, D., Strojnik, V. & Vengust, R. Early initiation of a strength training based rehabilitation after lumbar spine fusion improves core muscle strength: A randomized controlled trial. J. Orthop. Surg. Res. 13, 151 (2018).
Ponzano, M., Tibert, N., Bansal, S., Katzman, W. & Giangregorio, L. Exercise for improving age-related hyperkyphosis: a systematic review and meta-analysis with GRADE assessment. Arch. Osteoporos. 16, 140 (2021).
González-Gálvez, N., Gea-García, G. M. & Marcos-Pardo, P. J. Effects of exercise programs on kyphosis and lordosis angle: A systematic review and meta-analysis. PLoS ONE 14, e0216180 (2019).
Watson, S. L. et al. High-intensity exercise did not cause vertebral fractures and improves thoracic kyphosis in postmenopausal women with low to very low bone mass: The LIFTMOR trial. Osteoporos. Int. 30, 957–964 (2019).
Bergström, I., Bergström, K., Kronhed, A.-C.G., Karlsson, S. & Brinck, J. Back extensor training increases muscle strength in postmenopausal women with osteoporosis, kyphosis and vertebral fractures. Adv. Physiother. 13, 110–117 (2011).
Harding, A. T. et al. Exploring thoracic kyphosis and incident fracture from vertebral morphology with high-intensity exercise in middle-aged and older men with osteopenia and osteoporosis: A secondary analysis of the LIFTMOR-M trial. Osteoporos. Int. 32, 451–465 (2021).
Katzman, W. B. et al. Sex differences in response to targeted kyphosis specific exercise and posture training in community-dwelling older adults: A randomized controlled trial. BMC Musculoskelet. Disord. 18, 509 (2017).
Bansal, S., Katzman, W. B. & Giangregorio, L. M. Exercise for improving age-related hyperkyphotic posture: A systematic review. Arch. Phys. Med. Rehabil. 95, 129–140 (2014).
Hojjati, Z. & Sheikhpour, L. Seated exercise therapy improves posture and balance in hyperkyphotic elderly females, a randomized control trail. World Appl. Sci. J. 24, 331–335 (2023).
Chow, H. & Wu, D.-R. Outdoor fitness equipment usage behaviors in natural settings. Int. J. Environ. Res. Public Health 16, 391 (2019).
Chow, H.-W., Mowen, A. & Wu, G. Who is using outdoor fitness equipment and how? The case of Xihu Park. Int. J. Environ. Res. Public Health 14, 448 (2017).
Fernández-Rodríguez, E. F., Merino-Marban, R., Romero-Ramos, O. & López-Fernández, I. A systematic review about the characteristics and patterns of use of outdoor gyms. J. Hum. Sport Exerc. https://doi.org/10.14198/jhse.2020.15.Proc3.21 (2020).
Abelleira-Lamela, T. et al. Sagittal spine disposition and pelvic tilt during outdoor fitness equipment use and their associations with kinanthropometry proportions in middle-aged and older adults. PeerJ 9, e12657 (2021).
Karimizadeh Ardakani, M., Soroush Fard, Z., Amirizadeh, F. & Naderifar, H. Effect of Thoracic Hyper-Kyphosis Posture on Upper Extremity Function of Female Students. J. Rehabil. Sci. Res. 9, (2022).
Abelleira-Lamela, T. et al. Comparative electromyographic analysis in leg press of traditional fitness equipment, traditional outdoor fitness equipment, and a new model of outdoor fitness equipment in trained young men. Appl. Sci. (Switzerland) 14, 7390 (2024).
Hrysomallis, C. & Goodman, C. A review of resistance exercise and posture realignment. J. Strength Condit. Res. 15, 385 (2001).
Marcos-Pardo, P. J., Espeso-García, A., Vaquero-Cristóbal, R., Abelleira-Lamela, T. & González-Gálvez, N. The effect of resistance training with outdoor fitness equipment on the body composition, physical fitness, and physical health of middle-aged and older adults: A randomized controlled trial. Healthcare 12, 726 (2024).
Lorenzetti, S., Dayer, R., Plüss, M. & List, R. Pulling exercises for strength training and rehabilitation: Movements and loading conditions. J. Funct. Morphol. Kinesiol. 2, 33 (2017).
Schubert, C. C., Myers, L. J., Allen, K. & Counsell, S. R. Implementing geriatric resources for assessment and care of elders team care in a veterans affairs medical center: Lessons learned and effects observed. J. Am. Geriatr. Soc. 64, 1503–1509 (2016).
Sung, D.-H., Yoon, S.-D. & Park, G. D. The effect of complex rehabilitation training for 12 weeks on trunk muscle function and spine deformation of patients with SCI. J. Phys. Ther. Sci. 27, 951–954 (2015).
Abelleira-Lamela, T. et al. Electromyographic comparison of traditional fitness machines, outdoor fitness equipment without load selectors, and outdoor fitness equipment with load selectors in a seated chest press exercise in trained young men. Sensors 24, 7740 (2024).
Bhalerao, S. & Kadam, P. Sample size calculation. Int. J. Ayurveda Res. 1, 55 (2010).
Nayasista, A. H. et al. Effect of combined locomotor training and aerobic exercise on increasing handgrip strength in elderly with locomotive syndrome: A randomised controlled trial. Ann. Med. Surg. https://doi.org/10.1016/j.amsu.2022.103800 (2022).
González-Gálvez, N., Marcos-Pardo, P. J., Albaladejo-Saura, M., López-Vivancos, A. & Vaquero-Cristóbal, R. Effects of a Pilates programme in spinal curvatures and hamstring extensibility in adolescents with thoracic hyperkyphosis: A randomised controlled trial. Postgrad. Med. J. 99, 433–441 (2021).
Kemmler, W. et al. High intensity resistance exercise training to improve body composition and strength in older men with osteosarcopenia. Results of the randomized controlled franconian osteopenia and sarcopenia trial (FrOST). Front. Sports Act. Living https://doi.org/10.3389/fspor.2020.00004 (2020).
Esparza-Ros, F., Vaquero-Cristóbal, R. & Marfell-Jones, M. J. International Standards for Anthropometric Assessment -Full Profile- (International Society for Advancement in Kinanthropometry, 2019).
Kellis, E., Adamou, G., Tzilios, G. & Emmanouilidou, M. Reliability of spinal range of motion in healthy boys using a skin-surface device. J. Manipulative Physiol. Ther. 31, 570–576 (2008).
López-Miñarro, P., Muyor, J., Belmonte, F. & Alacid, F. Acute effects of hamstring stretching on sagittal spinal curvatures and pelvic tilt. J. Hum. Kinet. 31, 69–78 (2012).
Muyor, J. M., López-Miñarro, P. A. & Alacid, F. Disposición sagital del raquis lumbar en ciclistas de élite y sedentarios/Sagittal lumbar curvature in elite cyclists and non-athletic subjects. Revista Internacional de Medicina y Ciencias de la Actividad Física y del Deporte 46, (2016).
Marcos-Pardo, P. J. et al. Physical and psychological effects of outdoor fitness equipment training on middle-aged and older adults: Study protocol of a randomised controlled trial. BMJ Open Sport Exerc. Med. 9, e001829 (2023).
Clemons, J. Construct validity of two different methods of scoring and performing push-ups. J. Strength Cond. Res. 33, 2971–2980 (2019).
Vargas-Molina, S. et al. Comparison of blood lactate and perceived exertion responses in two matched time-under-tension protocols. PLoS ONE 15, e0227640 (2020).
Hopkins, W. G., Marshall, S. W., Batterham, A. M. & Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 41, 3–12 (2009).
Jang, H.-J., Hughes, L. C., Oh, D.-W. & Kim, S.-Y. Effects of corrective exercise for thoracic hyperkyphosis on posture, balance, and well-being in older women: A double-blind, group-matched design. J. Geriatr. Phys. Ther. 42, E17–E27 (2019).
Sinaki, M., Brey, R. H., Hughes, C. A., Larson, D. R. & Kaufman, K. R. Balance disorder and increased risk of falls in osteoporosis and kyphosis: Significance of kyphotic posture and muscle strength. Osteoporos. Int. 16, 1004–1010 (2005).
Choi, C. J. et al. Does the kyphotic change decrease the risk of fall?. Clin. Exp. Otorhinolaryngol. 4, 118 (2011).
Pawlowsky, S. B., Hamel, K. A. & Katzman, W. B. Stability of kyphosis, strength, and physical performance gains 1 year after a group exercise program in community-dwelling hyperkyphotic older women. Arch. Phys. Med. Rehabil. 90, 358–361 (2009).
Katzman, W. B., Parimi, N., Gladin, A., Wong, S. & Lane, N. E. Long-term efficacy of treatment effects after a kyphosis exercise and posture training intervention in older community-dwelling adults: A cohort study. J. Geriatr. Phys. Ther. 44, 127–138 (2021).
Matthews, C. E. et al. Amount of time spent in sedentary behaviors in the United States, 2003–2004. Am. J. Epidemiol. 167, 875–881 (2008).
Cho, M. et al. Biomechanical effects of different sitting postures and physiologic movements on the lumbar spine: A finite element study. Bioengineering 10, 1051 (2023).
López-Miñarro, P. A., Muyor, J. M., Alacid, F., Isorna, M. & Vaquero-Cristóbal, R. Sagittal spinal curvatures and pelvic inclination in kayakers. Revista Internacional de Medicina y Ciencias de la Actividad Física y el Deporte 14, (2014).
Dimitrijević, V., Šćepanović, T., Milankov, V., Milankov, M. & Drid, P. Effects of corrective exercises on lumbar lordotic angle correction: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 19, 4906 (2022).
Ghamkhar, L. & Kahlaee, A. H. The effect of trunk muscle fatigue on postural control of upright stance: A systematic review. Gait Posture 72, 167–174 (2019).
Larson, D. J. & Brown, S. H. M. The effects of trunk extensor and abdominal muscle fatigue on postural control and trunk proprioception in young, healthy individuals. Hum. Mov. Sci. 57, 13–20 (2018).
Fitts, R. H. Cellular mechanisms of muscle fatigue. Physiol. Rev. 74, 49–94 (1994).
O’Sullivan, P. B. et al. The effect of different standing and sitting postures on trunk muscle activity in a pain-free population. Spine (Phila Pa 1976) 27, 1238–1244 (2002).
Stevens, V. K. et al. The effect of increasing resistance on trunk muscle activity during extension and flexion exercises on training devices. J. Electromyogr. Kinesiol. 18, 434–445 (2008).
Aramaki, Y., Kakizaki, F., Kawata, S., Omotehara, T. & Itoh, M. Effects of the posterior pelvic tilt sitting posture on thoracic morphology and respiratory function. J. Phys. Ther. Sci. 33, 118–124 (2021).
Frey, M., Poynter, A., Younge, K. & De Carvalho, D. The relationship between lumbopelvic flexibility and sitting posture in adult women. J. Biomech. 84, 204–210 (2019).
Kett, A. R., Sichting, F. & Milani, T. L. The effect of sitting posture and postural activity on low back muscle stiffness. Biomechanics 1, 214–224 (2021).
Szczygieł, E., Zielonka, K., Mętel, S. & Golec, J. Musculo-skeletal and pulmonary effects of sitting position—A systematic review. Ann. Agric. Environ. Med. 24, 8–12 (2017).
Koelé, M. C., Lems, W. F. & Willems, H. C. The clinical relevance of hyperkyphosis: A narrative review. Front. Endocrinol. (Lausanne) https://doi.org/10.3389/fendo.2020.00005 (2020).
Fukuda, A., Tsuhima, E., Wada, K. & Ishibashi, Y. Effects of back extensor strengthening exercises on postural alignment, physical function and performance, self-efficacy, and quality of life in Japanese community-dwelling older adults: A controlled clinical trial. Phys. Ther. Res. 23, 132–142 (2020).
Acknowledgements
The authors would like to thank the “Consejo Superior de Deportes (CSD)”, part of the Spanish Ministry of Culture and Sport, and the “Spanish Ministry of Science, Innovation and Universities” for funding this study.
Funding
This work was supported and funded by the Spanish Ministry of Science, Innovation and Universities (code RTC-2017-6145-1, 2017). T.A-L’s participation in the present research is the result of a 2020–2021 Research Staff Training grant awarded by the UCAM Universidad Católica de Murcia.
Author information
Authors and Affiliations
Contributions
P.J.M-P., R.V-C. and N.G-G. conducted the research design; T.A-L., A.E–G. and N.G-G. conducted the intervention and data collection; P.J.M-P., R.V-C., T.A-L and N.G-G. wrote the main manuscript text; A.E–G. and N.G-G. conducted the statistical analysis; P.J.M.-P. and F.E-R. supervised the above processes and conducted the funding acquisition. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Marcos-Pardo, P.J., Abelleira-Lamela, T., Vaquero-Cristóbal, R. et al. Improving spinal alignment through innovative resistance training with outdoor fitness equipment in middle-aged and older adults: a randomized controlled trial. Sci Rep 15, 14499 (2025). https://doi.org/10.1038/s41598-025-99061-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-99061-1
