
Abstract
The biological underpinnings of post-stroke cognitive function are largely unknown, and protein investigations can point towards important pathways for further study. We profiled plasma levels of 91 neurology-related proteins (Olink Neurology panel) and serum Neurofilament light chain (NfL) levels in 205 cases in the Sahlgrenska Academy Study on Ischemic Stroke. Blood was sampled in the acute and convalescent (3 months post-stroke) phase. Cognitive outcome was evaluated by the Barrow Neurological Institute Screen for Higher Cerebral Functions 7 years post-stroke. In linear regression models, 6 and 5 proteins in the acute and convalescent phase, respectively, were univariably associated with cognitive outcome at False Discovery Rate (FDR) < 0.05, and 9 and 8 at p < 0.05 after adjustment for age, sex, education and sampling day (model 1) and/or additional adjustment for stroke severity (model 2). Of these, 15 proteins contributed with information in multi-protein models on at least one time-point. These included brain-expressed proteoglycans (NCAN, BCAN, GPC5, SPOCK1); contactin-5 (CNTN5); metabolic enzymes (HAGH, NMNAT1); cluster of differentiation (CD)-proteins (SIGLEC1, CLEC10A, CD200R1); GDNF family receptor alpha-1 (GFR-alpha-1); brorin (VWC2); beta-nerve growth factor (beta-NGF); myostatin (GDF-8); and NfL. We identified novel candidate protein biomarkers of post-stroke cognitive outcome that likely reflect different biological processes, warranting further exploration.
Similar content being viewed by others


Introduction
The incidence of ischemic stroke before 70 years of age is increasing1. Globally, about 60% of the people who are currently living with the consequences of ischemic stroke are under the age of 70 years2, and they face the risk of living with these consequences for many years. Despite that a large proportion of patients in this age group has mild stroke as defined by the degree of neurological impairment, results from recent studies highlight that unfavorable outcomes are common. These include cognitive impairment3,4 as well as fatigue, depressive symptoms5,6 and a relatively high risk of recurrent vascular events7,8,9,10. We and others have shown that reduced cognitive function in ischemic stroke survivors negatively affects the ability to return to work, social participation, and quality of life11,12. In line with this, and as recognized in recent works, there is an unmet need of increased understanding of the biological processes influencing post-stroke cognitive outcomes13,14. Indeed, post-stroke cognitive outcome can be conceptualized as a summation of direct stroke-related effects, such as infarct size and localization, but also pre-stroke cognitive reserve, concomitant microvascular and neurodegenerative pathologies, such as cerebral small vessel disease and (early) Alzheimer’s disease, with the molecular interplay poorly understood13,14,15. Identification of protein biomarkers associated with post-stroke cognitive function has the potential to indicate candidate pathophysiological processes, inform further mechanistic investigations, and ultimately contribute to the identification of novel therapeutic targets. Blood-based biomarkers also have the potential to guide interventions for persons with increased risk for cognitive decline after stroke.
Recently, our group reported multiple novel candidate plasma protein biomarkers of neurological outcome after ischemic stroke by measuring 91 proteins involved in neurobiological processes (Olink Neurology Panel)16. The same assay has been used by others to identify novel plasma protein biomarkers of Alzheimer’s disease (AD)17,18,19 and cognitive function in population-based cohorts20, but to the best of our knowledge not in stroke cohorts. Given that post-stroke cognition is likely influenced by both stroke-specific and general neurodegenerative processes13,14, blood-based biomarkers of cognitive function are not necessarily completely overlapping between post-stroke and population-based cohorts. We thus sought to profile these proteins for association with cognitive outcome in a relatively young ischemic stroke cohort with long-term follow-up. Our primary aim was to identify plasma protein biomarkers of long-term cognitive outcomes in the early phase after ischemic stroke, that in turn can point towards biological processes in merit of further investigation.
Methods
Study population and baseline characteristics
This study sample comprises of 205 cases from a sub-study within the longitudinal observational cohort study Sahlgrenska Academy Study on Ischemic Stroke (SAHLSIS) with available blood samples from all sampling points during follow-up, i.e. from the acute phase, and follow-up visits at 3 months and 7 years, and data from cognitive testing at long-term follow-up. The design of SAHLSIS and the present sub-study has been described in detail elsewhere16. In short, cases with first-ever or recurrent acute ischemic stroke at age 18–69 years were included consecutively at the stroke unit at the Sahlgrenska University Hospital, Gothenburg in 1998 to 2003. Acute ischemic stroke was defined as an episode of focal brain dysfunction with acute onset, lasting > 24 h, and of presumed vascular cause with no signs of hemorrhage or another cause on neuroimaging. All patients included in this study underwent imaging of the brain (computed tomography and/or magnetic resonance) as part of the clinical routine investigation. Participants underwent additional work-up according to national guidelines and were excluded if further evaluation showed another etiology than stroke. Complete information on vascular risk factors was registered at the 3-month follow-up by examinations and a structured questionnaire. Definitions were as follows, hypertension: pharmacological treatment for hypertension and/or systolic blood pressure ≥ 160 mmHg, and/or diastolic blood pressure ≥ 90 mmHg; diabetes mellitus: dietary or pharmacological treatment and/or fasting plasma glucose ≥ 7.0 mmol/L; hyperlipidemia: pharmacological treatment, total fasting serum cholesterol > 5.0 mmol/L, and/or LDL > 3.0 mmol/L; smoking: current smoking as opposed to never or former (cessation at least one year from inclusion). Information on attained education was obtained from questionnaires and grouped into categories: (1) elementary school or less (completed or non-completed elementary school), (2) upper secondary school or vocational school, and (3) university. Acute stroke severity was defined as the worst score by the Scandinavian Stroke Scale (SSS) within the first 7 days after stroke onset and converted to the internationally more commonly used NIH Stroke Scale (NIHSS) scores using an algorithm21 to facilitate comparisons with other studies. Of note, during the inclusion period of this study, acute revascularization therapy was not yet part of the routine clinical practice.
Cognitive outcome 7 years post-stroke
All surviving study participants in the SAHLSIS sub-study described above were invited to follow-up visits approximately 7 years after the index stroke (median 7.5 years, IQR − 5.9 to + 5.6 weeks), i.e. these visits took place from 2006 to 2011. The participation rate was 82%, and reasons for drop-out have been described in detail elsewhere22. Cognitive testing was performed by the Barrow Neurological Institute Screen (BNIS) for Higher Cerebral Functions, a comprehensive and reliable screening instrument for cognitive dysfunction23 with high sensitivity22,24 and good validity24 in stroke patients. All study participants were tested by the same research nurse (Ingrid Eriksson), who was trained in administering the BNIS and continually supervised by two neuropsychologists (HS and Caisa Hofgren). The BNIS total score (maximum 50) reflects the overall cognitive function and consists of a pre-screen (level of consciousness 3 points, basic language 3 points, and level of cooperation 3 points) to evaluate whether the participant is capable to take part in further testing, and 7 ensuing subscales: speech and language functions (15 points), orientation (3 points), attention/concentration (3 points), visuospatial function and visual problem solving (8 points), memory (7 points), affect (4 points), and awareness (1 point). The BNIS is intended as a screening test to identify persons with possible cognitive dysfunction that might benefit from further neuropsychological evaluation, and inherently a higher sensitivity than specificity is thus preferred. However, there is yet no established optimal cut-off value for indicating possible cognitive dysfunction by the BNIS and different cut-offs have been suggested23. An early suggestion was < 47 points for persons ≤ 55 years and < 43 points for persons > 55 years of age25. The cut-off level for persons ≤ 55 years of age was supported in a later validation study of the BNIS based on conventional neuropsychological tests in a cohort of stroke cases with good functional outcome, but for cases > 55 years of age the optimal cut-off level was < 41 points (sensitivity 92% and specificity 85%)24. For descriptive purposes in the present study, the cut-off values for possible cognitive dysfunction that we used thus were < 47 points for cases ≤ 55 years and < 41 points for cases > 55 years.
Other assessments at the 7-year follow-up visit
Presence of vascular risk factors was reassessed by questionnaires. Recurrent strokes and neurological comorbidities with plausible influence on protein measurements or outcome were identified through questionnaires and national registers, and diagnoses were verified by review of medical records as described26.
Blood sampling
Venous blood samples were drawn during the acute (median 4 days after index stroke, interquartile range (IQR) 3–6 days) and convalescent (3 months; median 98 days, IQR 93–109 days) phases. Additional blood samples were drawn at the 7-year visit. On all occasions, blood was collected between 8.30 and 10.30 a.m. after an overnight fast. Blood was drawn in tubes containing 10% by volume ethylenediaminetetraacetic acid (EDTA). Plasma was isolated within 2 h by centrifugation at 2000×g at 4 °C for 20 min, aliquoted, and stored at − 80 °C pending analysis.
Measurement of proteins levels
Plasma levels of 91 neurology-related proteins were measured using the highly sensitive and specific Proximity Extension Assay (PEA)27 using the Neurology panel (Olink Proteomics, Uppsala, Sweden). In brief, analyses were performed according to the manufacturer’s protocol by a board-certified laboratory technician at Olink, blinded to the clinical information. The 3 samples from each case were placed on the same plate, to limit the impact of inter-run variability. Samples not passing quality control (n = 5) were excluded from further analysis. Plasma protein levels were measured as Normalized Protein eXpression (NPX) values, which is a relative quantification given on a log2 scale. For individual protein read-outs below the limit of detection (n = 19 in total), levels were set to the lowest limit of detection (see Table S1 for details). Mean intra- and inter-run coefficients of variation was 6.5% and 11.5%, respectively, as detailed16. All investigated proteins, including their full protein name, Uniprot ID and encoding gene, are listed in Table S1. Of note the version of the Olink Neurology panel used here did not contain the neuroaxonal damage marker Neurofilament light chain (NfL). However, we have previously measured serum NfL concentrations using a Single Molecule Array (SiMoA) assay in the SAHLSIS, and reported these results in relation to functional and neurological outcomes26. Thus, we included these NfL data in the present study to be able to compare the results for the other proteins with NfL.
Statistical analyses
Bivariate correlations were assessed by Spearman’s rank correlation. Proteins were clustered hierarchically based on degree of covariation according to Euclidean distance. The total BNIS score was treated as a continuous variable and linear regression was used to investigate associations between individual protein levels and BNIS scores. Scatter plots of all assessed proteins by BNIS scores were manually viewed, and 3 deemed outliers were removed from the linear regression analyses (beta-NGF: 1 study participant, all sampling points; CLM-6; 1 study participant, all sampling points; GZMA: 1 study participant, acute phase levels). For plasma proteins measured by the Olink PEA the NPX value is given on a log2 scale, and thus the yielded β-value corresponds to the predicted change in BNIS score per each doubling of the protein level. Previously measured serum NfL levels (pg/mL) were therefore log2 transformed to harmonize these β-values with the Olink data.
Pre-specified adjustments were made for the potential confounding factors age at inclusion, sex, educational level, and day of blood draw (model 1), and additionally also for acute stroke severity (model 2). Our primary aim was to identify candidate acute and 3-month markers of long-term cognitive outcome independent of these clinical variables, but we also performed univariable and cross-sectional analyses of protein levels and cognitive outcome at the 7-year follow-up for comparisons.
Study participants with missing information were as follows: education n = 4; hyperlipidemia at baseline: n = 4; information on vascular risk factors at the 7-year follow-up: n = 2; time until blood draw: n = 3 (acute phase), n = 1 (3 months); missing Olink protein measurements due to samples not passing quality control: n = 2 (acute phase), n = 2 (3 months), n = 1 (7 years); missing serum NfL levels: n = 45 (acute phase), n = 5 (3 months), n = 3 (7 years). Participants with missing information were only excluded in statistical analyses including this (these) specific variable(s). From 1998 to 2000, serum was not collected in the acute phase, explaining the majority (n = 44) of the missing NfL measurements at this time-point.
Least absolute shrinkage and selection operator (LASSO) regression was used to identify proteins at each sampling point, that contributed to the prediction of cognitive outcome above the clinical variables age, sex, education, sampling day (multiprotein model 1) and stroke severity (multiprotein model 2). Repeated cross-validation (fivefold, repeated 20 times) and a grid search approach with a fixed alpha of 1 (R package glmnet) were used to identify the optimal lambda value for each model. For acute phase protein levels, two sets of LASSO regression procedures were made: one including acute NfL levels (n = 45 participants with missing information thus excluded) and one without this variable. As acute NfL levels were not among selected proteins in the first set, we proceeded with the second set only.
Linear regression analyses for selected proteins were rerun in a sensitivity analysis excluding participants with a recurrent stroke between inclusion and the 7-year follow-up and/or a neurological comorbidity (n = 29).
For the individual protein analyses, the Benjamini and Hochberg method was used to control the false discovery rate (FDR) of multiple testing28. Associations with FDR < 0.05 were considered statistically significant, and associations with FDR ≥ 0.05 but a two-tailed p < 0.05 were considered suggestive. However, it is of note that adjustment for multiple comparisons by number of investigated proteins (n = 92) is arbitrary as many of the investigated proteins were highly correlated (Tables S2–S4), thus not equating to 92 independent comparisons. In the remaining analyses, a two-tailed p < 0.05 was considered statistically significant.
Statistical analyses were performed in R version 4.4.1 or IBM SPSS Statistics version 29.
Results
Of the 209 participants with measured plasma protein levels, 205 completed the 7-year BNIS test and were thus included in the present study. Reasons for not completing the BNIS were aphasia (n = 2) and poor vision (n = 2). For the included study participants, clinical characteristics at baseline with correlations to the total BNIS scores at the 7-year follow-up are given in Table 1. Most participants experienced a mild stroke, and none received acute recanalization therapy (intravenous thrombolysis or thrombectomy). Total BNIS scores were nearly normally distributed (median 41, IQR 37–44) and 121 participants (59%) had a score indicative of possible cognitive dysfunction. Age and educational level were moderately correlated to 7-year BNIS scores (r = − 0.36, p < 1 × 10−6 and r = 0.36, p < 1 × 10−6, respectively), whereas hypertension, diabetes mellitus, and stroke severity (NIHSS) were weakly so (|r| < 0.3, Table 1).
Associations between acute-phase protein levels and 7-year cognitive outcome
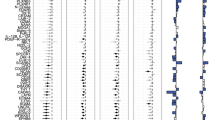
Results from the linear regression analyses for associations between individual protein levels measured in the acute phase and 7-year cognitive testing results are shown in Fig. 1 and detailed in Table S5. In the univariable analyses acute phase levels of 6 proteins were significantly associated with 7-year BNIS scores (FDR < 0.05, Fig. 1A). Of these, BCAN, NCAN and SIGLEC1 were also suggestively associated (p < 0.05) after adjustment for age, sex, educational level, and day of blood draw (model 1), with NCAN and SIGLEC1 remaining so after additional adjustment for acute stroke severity (model 2). Acute phase levels of 6 further proteins were suggestively associated with BNIS scores in model 1 and/or model 2 (p < 0.05, Fig. 1A), but none with FDR < 0.05.

Associations between individual protein levels in the acute phase of ischemic stroke and 7-year cognitive outcome, together with correlations for 17 selected proteins. (A) Associations between protein levels in the acute stroke phase and cognitive outcome 7 years after index stroke for proteins associated at p < 0.05 in any analysis of individual protein levels. Associations are visualized in forest plots with β values and 95% confidence intervals derived from univariable linear regression, and multivariable linear regression models adjusted for age, sex, education and blood sampling day (model 1). Associations in model 2 are additionally adjusted for acute stroke severity (NIH stroke scale [NIHSS]). Associations with p < 0.05 are shown in black, and for proteins marked in bold text font, univariable associations were associated at false discovery rate (FDR) < 0.05. The β-value corresponds to the predicted change in the Barrow Neurological Institute Screen (BNIS) for Higher Cerebral Functions total score per each doubling of protein level and a positive β-value to higher protein levels being associated with a more favorable cognitive outcome. (B) Hierarchical protein clusters in the acute stroke phase for proteins associated with cognitive outcome at p < 0.05 in any analysis of individual protein levels. The full hierarchical cluster tree based on degree of covariation according to Euclidean distance is displayed and a selected number of clusters are visually highlighted by bold squares in the heat map. Information on the association between protein levels and cognitive outcome at 7 years according to the BNIS total score are given in the first rows, with adjustments as in Panel A. Proteins selected by LASSO regression to contribute with information in multiprotein models of 7-year cognitive outcome are marked in bold. In following rows, bivariate Spearman’s rank correlation coefficients (r) between protein levels and clinical variables are displayed, where correlations with p < 0.05 are marked in colour. Positive correlations (r > 0) between protein levels, increasing acute stroke severity (NIHSS), and age are marked red, and inverse correlations (r < 0) are marked blue. For sex, a positive correlation (r > 0, red boxes) corresponds to higher protein levels in males than females, and for remaining clinical variables a positive correlation corresponds to higher protein levels in participants with that factor prevalent.
Among the 17 acute-phase proteins associated with cognitive outcome at p < 0.05 in any of the regression analyses, there were 6 main protein clusters. Higher protein levels were associated with lower cognitive performance in 4 clusters, and with better cognitive performance in 2 clusters (Fig. 1B).
We next applied LASSO regression to identify the proteins contributing with information in acute phase multiprotein models of cognitive outcome. Starting with all 92 proteins, 9 proteins across the 6 main clusters were selected (Table 2). In the first model that included information on age, sex, education, and sampling day (multiprotein model 1), 8 proteins were selected, and in the second model that also included stroke severity (NIHSS), 7 proteins were selected.
Associations between convalescent phase protein levels and 7-year cognitive outcome
At the 3-month follow-up, individual levels of 22 proteins were associated with 7-year cognitive outcome at p < 0.05 in either univariable or multivariable analyses, of which 5 proteins were significant at FDR < 0.05 in the univariable analyses (Fig. 2A and Table S5). These 22 proteins clustered into 5 main groups (Fig. 2B), where only the cluster of BCAN, NCAN and CD200R1 contained proteins for which higher 3-month levels were associated with better cognitive performance; for the remaining clusters inverse associations were observed. Ten proteins (including BCAN, NCAN, beta-NGF, SIGLEC1 and VWC2) were common to both the acute and convalescent stroke phase, but there were also differing examples. For instance, and in contrast to acute phase levels, 3-month levels of SPOCK1 and GDF-8 were not associated to cognitive outcome (p > 0.42 for both, Table S5). Also, levels of NfL, HAGH, and NMNAT1 were associated when measured at 3 months, but not in the acute stroke phase (p > 0.13 for all, acute phase levels, Table S5). Further, 3-month levels of NfL were only associated to 7-year BNIS scores before adjustment for acute stroke severity (i.e. univariably and in model 1, Fig. 2A, and Table S5).

Associations between individual protein levels in the convalescent stroke phase and 7-year cognitive outcome, together with correlations for 22 selected proteins. Associations between protein levels at the 3-month follow-up and cognitive outcome 7 years after index stroke, and hierarchical clusters for proteins associated with cognitive outcome at p < 0.05 in any analysis of individual protein levels. Panels (A,B) as in Fig. 1.
Three-month levels of 11 proteins were selected using LASSO regression to contribute with information in multi-protein models of cognitive outcome and these included both common and differential proteins compared to the acute phase sampling (Table 2).
Cross-sectional associations between protein levels and cognitive function 7 years post-stroke
For comparison, we also investigated cross-sectional associations between protein levels and cognitive testing scores at the 7-year follow-up (Fig. 3A and Table S5). There were fewer clusters of proteins associated to concomitant BNIS scores (Fig. 3B, and Table S5), and only 5 proteins contributed with information in multiprotein models (Table 2). Of these, all but ADAM22 and CDH3 had been associated to cognitive outcome also when measured at an earlier sampling point.

Cross-sectional associations between individual protein levels and cognitive outcome at the 7-year follow-up, together with correlations for 22 selected proteins. Cross-sectional associations between protein levels and cognitive outcome at follow-up 7 years after index stroke, and hierarchical clusters for proteins associated with cognitive testing scores at p < 0.05 in any analysis of individual protein levels. Panels (A,B) as in Fig. 1, except linear regressions models were not adjusted for sampling day.
Sensitivity analyses
For proteins associated to 7-year BNIS scores at p < 0.1 in the adjusted analyses of individual protein levels (model 1–2), linear regression analyses were rerun in a sensitivity analysis excluding cases with recurrent stroke and/or a neurological comorbidity before the 7-year follow-up (n = 29), with results essentially unchanged (Table S6).
Discussion
This exploratory study of 92 neurology-related proteins is the broadest investigation of putative blood protein biomarkers for long-term post-stroke cognitive outcome to our knowledge. We identified novel candidate biomarkers that followed different trajectories after the acute stroke phase, clustered into separate groups, and contributed with information in multi-protein models of 7-year cognitive outcome. We interpret these results as a reflection in blood of different biological processes involved in post-stroke cognition.
Of the candidate protein biomarkers reported in this study, NfL has been previously investigated in blood for association to post-stroke cognitive outcomes. Our present finding that higher 3-month NfL concentrations are associated with lower cognitive function in young and middle-aged ischemic stroke survivors with mild stroke is in line with the reported associations to post-stroke cognitive decline and dementia risk in stroke cohorts of older age29,30. NfL concentrations have also been associated with stroke severity26, infarct size31, cerebral small vessel disease burden29,32, and post-stroke functional outcome26,31,33, factors in turn known to influence and/or correlate with post-stroke cognitive function. For many of the other markers we report here, previous investigations suggest a role in biological processes of importance for cognitive function, e.g. in population-based cohorts20,34,35, in relation to vascular dementia36, AD17,18,19,37,38, and cerebral white matter hyperintensities39, as well in experimental work40,41. These candidate markers include BCAN and NCAN that are emerging biomarkers of cognitive and neuroimaging phenotypes17,20,35,42, and GFR-alpha 1 that has been associated with incident dementia43.
Our investigation complements previous studies with information on the profiled proteins in relation to cognition specifically in the post-stroke setting. It is conceivable that cognitive function post-stroke is influenced by both infarct-related and general neurodegenerative processes, and it follows that individual biomarkers may reflect both or either of these processes. Possibly reflecting an infarct-related process, we note that some proteins (e.g. NfL, BCAN, CLEC10A, CNTN5, GDF-8, GPC5, HAGH, and SPOCK1) were associated to cognitive outcome when measured in the acute or convalescent stroke phase, but not in the adjusted cross-sectional analyses at the 7-year follow-up in our study. Further investigations are of course needed to confirm if this represents true stroke-specific trajectories, but we have previously reported differences in protein levels by time after stroke in the same study cohort16,26. For the neuroaxonal injury-biomarker NfL, the observed association to cognitive outcome is likely explained by reflection of stroke severity, of which subacute NfL levels are especially informative26,31,33. In line with this, the association between 3-month NfL levels and cognitive outcome was not retained after adjustment for acute stroke severity in the present study. In contrast, levels of all remaining examples above except CNTN5, contributed in multi-protein models also including acute stroke severity, suggesting that there is a time-window early post-stroke where plasma levels of some proteins reflect biological processes that influence long-term cognitive outcome independent of stroke severity. Validation in additional stroke cohorts is needed to confirm these findings.
Our goal was to identify candidate protein biomarkers in the early post-stroke phase of long-term cognitive outcome, that in turn can point towards biological processes in merit of further investigation. In our data, we observed the highest number of clusters among associated proteins in the acute and convalescent stroke phase, and it follows that a higher number of proteins contributed with information in multi-protein models at these sampling points compared to the cross-sectional 7-year analyses. This likely means that a larger number of biological processes influencing cognitive outcome was reflected early after stroke by profiling of the proteins investigated in this study. Further, it was possible to discern different protein types and functions among the candidate acute and 3-month markers (Fig. 4). For instance, BCAN and NCAN are brain-specific extracellular matrix chondroitin sulfate proteoglycans, whereas GDF-8 (myostatin) and NfL both clustered singly among candidates. Metabolic enzymes NMNAT1 and HAGH (also known as glyoxalase II) clustered together, both involved in cellular processes of importance in neurodegenerative diseases and ageing, including oxidative stress protection44,45. NMNAT1 is protective after experimental ischemic stroke46,47,48 and increased plasma levels of HAGH has been reported in pre-symptomatic AD18. SIGLEC1 and CLEC10A are both immune cell-specific membrane proteins differentially expressed in microglia during AD49, and differential expression of SIGLEC1 in blood leukocytes is associated with progression of cerebral white matter hyperintensities39. VWC2, a bone morphogenetic protein (BMP)-antagonist predominantly expressed in the brain (GTEx) clustered together with the neurotrophic factor receptor GFR-alpha-1, and both have previous support as potential novel cognition biomarkers17,19,20,43. VWC2 and GFR-alpha-1 clustered together with additional proteins including the endothelial BMP-receptor SKR3 (i.e. ACVRL1 or ALK1) which plays a central role in vasculogenesis50, and both GFR-alpha 1 and SKR3 have been suggested as a possible mediators between poor cardiovascular health and incident dementia43. Taken together, proteins with currently annotated metabolic, neuroprotective, neurotrophic, immunologic, and angiogenic functions are among the identified novel candidates, pointing to a role of such pathways in post-stroke cognitive function.

Candidate acute and/or 3-month markers of long-term cognitive outcome. Protein types and selected gene ontology (GO) biological processes for the proteins associated at p < 0.05 in the adjusted analyses of individual proteins levels (model 1 and/or 2) or contributing with information in multiprotein models of long-term cognitive outcome, in the acute or convalescent stroke phase. BMP-antagonist bone morphogenetic protein-antagonist, CD-proteins cluster of differentiation proteins.
Strengths of this study include the inclusion of consecutive and clinically well-characterized study participants followed long term. We used a validated, sensitive cognitive screening instrument spanning across different cognitive domains23, and analyzed protein level associations to the entire cognitive testing scale score. Repeated blood samplings were standardized, and levels of a large number of proteins were analyzed simultaneously by a multiplex method with high specificity27, with undertaken measures to limit the impact of run-to-run variability as detailed16. We have also previously provided in-depth information on protein levels trajectories after stroke, differences between stroke cases and controls, and associations to stroke severity and neurological outcome for the proteins included in the present study16,26, enabling comparisons.
There are also important study limitations to consider, including previously discussed16 impact on generalizability to cases with more severe strokes and older age, and circulating levels not necessarily reflecting protein levels in the cerebrospinal fluid (CSF) or brain. Indeed, correlations between plasma and CSF levels have been reported to vary among the proteins investigated17. Also, this study is exploratory, and the results need replication. However, we know of no similar cohort for validation at this time, and a majority of the reported proteins have previous support as candidate cognition biomarkers as detailed above. Moreover, cognitive function was only evaluated at the long-term follow-up, and we did not have information on cognitive ability pre-stroke or cognitive testing scores in age and sex-matched controls, precluding discernment of direct stroke-caused impairments and early versus late post-stroke changes in cognitive ability. Still, a majority of the relatively young study participants investigated here was in full-time employment at the time of index stroke, indicating a normal cognitive functioning at baseline, and efforts to provide in-depth data on trajectories of both biomarkers and cognitive outcome after stroke are underway by both us and others13,51,52. Also, levels of NfL and the other 91 investigated proteins were measured using two different methods (i.e. NfL with the quantitative SiMoA technology and the other proteins with the Olink Proximity Extension Assay) and in serum and plasma, respectively, why effect sizes between NfL and the other protein levels cannot be directly compared. Further, the inclusion period of the study was relatively long, and plasma samples were stored several years at − 80 °C prior to analysis. However, we visually inspected scatter plots of acute plasma proteins levels (the samples stored the longest) by sampling date and found no instances of lower protein levels in participants sampled early during the study period, i.e. we found no signs of plasma protein degradation by storage time. Finally, to investigate possible associations to infarct volume and cerebral small vessel disease, an interesting future perspective is to complement our results with neuroimaging data, and to investigate possible differences between ischemic stroke etiological subtypes that the present study is underpowered to uncover.
Here, we conducted an exploratory study of 92 neurology-related circulating proteins and identified candidate novel blood biomarkers that likely reflect different biological processes of importance for long-term cognitive function after stroke. Validation in independent stroke cohorts and additional mechanistic investigations are warranted.
Data availability
Summary statistics are provided as Supplemental material. Anonymized data will be shared upon reasonable request from a qualified academic investigator to the corresponding author as long as data transfer agrees with EU legislation on the general data protection regulation (GDPR) and with decisions by the Ethical Review Board of Sweden and the University of Gothenburg, the latter which should be regulated in a data transfer agreement.
References
Global, regional, and national burden of stroke and its risk factors, 1990–2021: A systematic analysis for the global burden of disease study 2021. Lancet Neurol. 23, 973–1003. https://doi.org/10.1016/s1474-4422(24)00369-7 (2024).
Feigin, V. L. et al. World Stroke Organization: Global Stroke Fact Sheet 2025. Int. J. Stroke 20, 132–144. https://doi.org/10.1177/17474930241308142 (2025).
Planton, M. et al. Neuropsychological outcome after a first symptomatic ischaemic stroke with ‘good recovery’. Eur. J. Neurol. 19, 212–219. https://doi.org/10.1111/j.1468-1331.2011.03450.x (2012).
Schaapsmeerders, P. et al. Long-term cognitive impairment after first-ever ischemic stroke in young adults. Stroke 44, 1621–1628. https://doi.org/10.1161/strokeaha.111.000792 (2013).
Pedersen, A. et al. Fatigue 7 years post-stroke: Predictors and correlated features. Acta Neurol. Scand. 146, 295–303. https://doi.org/10.1111/ane.13665 (2022).
Amaricai, E. & Poenaru, D. V. The post-stroke depression and its impact on functioning in young and adult stroke patients of a rehabilitation unit. J. Ment. Health. 25, 137–141. https://doi.org/10.3109/09638237.2015.1022251 (2016).
Rutten-Jacobs, L. C. et al. Long-term risk of recurrent vascular events after young stroke: The FUTURE study. Ann. Neurol. 74, 592–601. https://doi.org/10.1002/ana.23953 (2013).
Redfors, P. et al. Stroke subtype predicts outcome in young and middle-aged stroke sufferers. Acta Neurol. Scand. https://doi.org/10.1111/j.1600-0404.2012.01653.x (2012).
Leys, D. Long-term follow-up after minor ischaemic strokes or transient ischaemic attacks: Not as good as previously thought. Eur. J. Neurol. 30, 2591–2592. https://doi.org/10.1111/ene.15906 (2023).
Broman, J. et al. Long-term risk of recurrent vascular events and mortality in young stroke patients: Insights from a multicenter study. Eur. J. Neurol. 30, 2675–2683. https://doi.org/10.1111/ene.15850 (2023).
Samuelsson, H. et al. Cognitive function is an important determinant of employment amongst young ischaemic stroke survivors with good physical recovery. Eur. J. Neurol. 28, 3692–3701. https://doi.org/10.1111/ene.15014 (2021).
Mole, J. A. & Demeyere, N. The relationship between early post-stroke cognition and longer term activities and participation: A systematic review. Neuropsychol. Rehabil. 30, 346–370. https://doi.org/10.1080/09602011.2018.1464934 (2020).
Rost, N. S. et al. Cognitive impairment and dementia after stroke: Design and rationale for the DISCOVERY study. Stroke 52, e499–e516. https://doi.org/10.1161/strokeaha.120.031611 (2021).
O’Sullivan, M. J., Li, X., Galligan, D. & Pendlebury, S. T. Cognitive recovery after stroke: Memory. Stroke 54, 44–54. https://doi.org/10.1161/strokeaha.122.041497 (2023).
Cramer, S. C., Richards, L. G., Bernhardt, J. & Duncan, P. Cognitive deficits after stroke. Stroke 54, 5–9. https://doi.org/10.1161/strokeaha.122.041775 (2023).
Lagging, C. et al. Investigation of 91 proteins implicated in Neurobiological processes identifies multiple candidate plasma biomarkers of stroke outcome. Sci. Rep. 12, 20080. https://doi.org/10.1038/s41598-022-23288-5 (2022).
Whelan, C. D. et al. Multiplex proteomics identifies novel CSF and plasma biomarkers of early Alzheimer’s disease. Acta Neuropathol. Commun. 7, 169. https://doi.org/10.1186/s40478-019-0795-2 (2019).
Ahmad, S. et al. CDH6 and HAGH protein levels in plasma associate with Alzheimer’s disease in APOE Ε4 carriers. Sci. Rep. 10, 8233. https://doi.org/10.1038/s41598-020-65038-5 (2020).
Jiang, Y. et al. Large-scale plasma proteomic profiling identifies a high-performance biomarker panel for Alzheimer’s disease screening and staging. Alzheimers Dement. 18, 88–102. https://doi.org/10.1002/alz.12369 (2022).
Harris, S. E. et al. Neurology-related protein biomarkers are associated with cognitive ability and brain volume in older age. Nat. Commun. 11, 800. https://doi.org/10.1038/s41467-019-14161-7 (2020).
Gray, L. J., Ali, M., Lyden, P. D. & Bath, P. M. Interconversion of the National Institutes of Health Stroke Scale and Scandinavian Stroke Scale in Acute Stroke. J. Stroke Cerebrovasc. Dis. 18, 466–468. https://doi.org/10.1016/j.jstrokecerebrovasdis.2009.02.003 (2009).
Redfors, P. et al. The Barrow neurological Institute screen for higher cerebral functions in cognitive screening after stroke. J. Stroke Cerebrovasc. Dis. 23, 349–355. https://doi.org/10.1016/j.jstrokecerebrovasdis.2013.04.026 (2014).
Prigatano, G. P., Rosenstein, L. D. & Denney, D. A. Screening for more than level of cognitive functioning: The BNI screen for higher cerebral functions. Brain Inj. 36, 479–487. https://doi.org/10.1080/02699052.2022.2051208 (2022).
Boosman, H., Visser-Meily, J. M., Post, M. W., Duits, A. & van Heugten, C. M. Validity of the Barrow Neurological Institute (BNI) screen for higher cerebral functions in stroke patients with good functional outcome. Clin. Neuropsychol. 27, 667–680. https://doi.org/10.1080/13854046.2013.777787 (2013).
Prigatano, G. P., Amin, K. & Rosenstein, L. D. Administration and scoring manual for the BNI screen for higher cerebral functions. Barrow Neurol. Inst. (1995).
Pedersen, A. et al. Circulating neurofilament light in ischemic stroke: Temporal profile and outcome prediction. J. Neurol. 266, 2796–2806. https://doi.org/10.1007/s00415-019-09477-9 (2019).
Assarsson, E. et al. Homogenous 96-plex PEA immunoassay exhibiting high sensitivity, specificity, and excellent scalability. PLoS One. 9, e95192. https://doi.org/10.1371/journal.pone.0095192 (2014).
Benjamini, Y. & Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B (Methodol). 57, 289–300 (1995).
Egle, M. et al. Neurofilament light chain predicts future dementia risk in cerebral small vessel disease. J. Neurol. Neurosurg. Psychiatry. 92, 582–589. https://doi.org/10.1136/jnnp-2020-325681 (2021).
Wang, J. H. et al. Circulating neurofilament light predicts cognitive decline in patients with post-stroke subjective cognitive impairment. Front. Aging Neurosci. 13, 665981. https://doi.org/10.3389/fnagi.2021.665981 (2021).
Tiedt, S. et al. Serum neurofilament light: A biomarker of neuroaxonal injury after ischemic stroke. Neurology 91, e1338–e1347. https://doi.org/10.1212/wnl.0000000000006282 (2018).
Gattringer, T. et al. Serum neurofilament light is sensitive to active cerebral small vessel disease. Neurology 89, 2108–2114. https://doi.org/10.1212/wnl.0000000000004645 (2017).
Pujol-Calderón, F. et al. Neurofilament changes in serum and cerebrospinal fluid after acute ischemic stroke. Neurosci. Lett. 698, 58–63. https://doi.org/10.1016/j.neulet.2018.12.042 (2019).
Newman, A. B. et al. Evaluation of associations of growth differentiation factor-11, growth differentiation factor-8 and their binding proteins follistatin and follistatin-like protein-3 with dementia and cognition. J. Gerontol. Biol. Sci. Med. Sci. https://doi.org/10.1093/gerona/glad019 (2023).
Tin, A. et al. Identification of circulating proteins associated with general cognitive function among middle-aged and older adults. Commun. Biol. 6, 1117. https://doi.org/10.1038/s42003-023-05454-1 (2023).
Minta, K. et al. Brevican and neurocan peptides as potential cerebrospinal fluid biomarkers for differentiation between vascular dementia and Alzheimer’s disease. J. Alzheimers Dis. 79, 729–741. https://doi.org/10.3233/jad-201039 (2021).
Dauar, M. T. et al. Characterization of the contactin 5 protein and its risk-associated polymorphic variant throughout the Alzheimer’s disease spectrum. Alzheimers Dement. 19, 2816–2830. https://doi.org/10.1002/alz.12868 (2023).
Oveisgharan, S. et al. Proteins linking APOE Ɛ4 with Alzheimer’s disease. Alzheimers Dement. 20, 4499–4511. https://doi.org/10.1002/alz.13867 (2024).
Jickling, G. C. et al. Progression of cerebral white matter hyperintensities is related to leucocyte gene expression. Brain 145, 3179–3186. https://doi.org/10.1093/brain/awac107 (2022).
Cao, J. Y. et al. Expression of nerve growth factor carried by pseudotyped lentivirus improves neuron survival and cognitive functional recovery of post-ischemia in rats. CNS Neurosci. Ther. 24, 508–518. https://doi.org/10.1111/cns.12818 (2018).
Végh, M. J. et al. Reducing hippocampal extracellular matrix reverses early memory deficits in a mouse model of Alzheimer’s disease. Acta Neuropathol. Commun. 2, 76. https://doi.org/10.1186/s40478-014-0076-z (2014).
Walker, R. M. et al. The circulating proteome and brain health: Mendelian randomisation and cross-sectional analyses. Transl. Psychiatry. 14, 204. https://doi.org/10.1038/s41398-024-02915-x (2024).
Beydoun, M. A. et al. Plasma proteomic biomarkers and the association between poor cardiovascular health and incident dementia: The UK Biobank study. Brain Behav. Immun. 119, 995–1007. https://doi.org/10.1016/j.bbi.2024.05.005 (2024).
Lautrup, S., Sinclair, D. A., Mattson, M. P. & Fang, E. F. NAD(+) in brain aging and neurodegenerative disorders. Cell. Metab. 30, 630–655. https://doi.org/10.1016/j.cmet.2019.09.001 (2019).
de Bari, L. et al. Interplay among oxidative stress, Methylglyoxal pathway and S-glutathionylation. Antioxidants (Basel). 10. https://doi.org/10.3390/antiox10010019 (2020).
Zhang, Y. et al. Nicotinamide mononucleotide adenylyltransferase 1 regulates cerebral ischemia-induced blood-brain barrier disruption through NAD(+)/SIRT1 signaling pathway. Mol. Neurobiol. 59, 4879–4891. https://doi.org/10.1007/s12035-022-02903-6 (2022).
Liang, J., Wang, P., Wei, J., Bao, C. & Han, D. Nicotinamide mononucleotide adenylyltransferase 1 protects neural cells against ischemic injury in primary cultured neuronal cells and mouse brain with ischemic stroke through AMP-activated protein kinase activation. Neurochem. Res. 40, 1102–1110. https://doi.org/10.1007/s11064-015-1569-2 (2015).
Wang, P. et al. Neuroprotection by nicotinamide mononucleotide adenylyltransferase 1 with involvement of autophagy in an aged rat model of transient cerebral ischemia and reperfusion. Brain Res. 1723, 146391. https://doi.org/10.1016/j.brainres.2019.146391 (2019).
Kim, D. W. et al. Amyloid-beta and Tau pathologies act synergistically to induce novel disease stage-specific microglia subtypes. Mol. Neurodegener. 17, 83. https://doi.org/10.1186/s13024-022-00589-x (2022).
Roman, B. L. & Hinck, A. P. ALK1 signaling in development and disease: New paradigms. Cell. Mol. Life Sci. 74, 4539–4560. https://doi.org/10.1007/s00018-017-2636-4 (2017).
Brännmark, C. et al. Rationale and protocol for a longitudinal observational cohort study of trajectories of recovery and biomarkers poststroke. BMJ Open. 13, e072493. https://doi.org/10.1136/bmjopen-2023-072493 (2023).
Quinn, T. J. et al. Research protocol—Assessing Post-Stroke Psychology Longitudinal Evaluation (APPLE) study: A prospective cohort study in stroke. Cereb. Circ. Cogn. Behav. 3, 100042. https://doi.org/10.1016/j.cccb.2022.100042 (2022).
Acknowledgements
We wish to thank the study participants and their next of kin, without whom this work would not have been possible. We are also grateful to the research nurses and physicians in our group for their excellent work with the follow-up visits.
Funding
Open access funding provided by University of Gothenburg.
The Swedish Heart and Lung Foundation (20220184); the Swedish Research Council (2021-01114); the Swedish state under the agreement between the Swedish government and the county councils, the ALF agreement (ALFGBG-965328); the Swedish Stroke Association; the King Gustaf V: s and Queen Victoria’s Foundation; the Agneta Prytz-Folke’s and Gösta Folke’s Foundation; Göteborg Foundation for Neurological Research; and the John and Brit Wennerström’s Foundation for Neurological Research.
Author information
Authors and Affiliations
Contributions
CJ, AP, TS and CL conceived and designed the study. CJ and KJ designed and led data acquisition on stroke outcomes, and AP contributed to data acquisition on clinical characteristics of study participants. CJ and TS were responsible protein measurements. SF wrote the R-script for the LASSO regression analyses, and CL performed the analyses. Remaining statistical analyses were performed by CL and supervised by MP. All authors contributed to the interpretation of results. The first draft of the manuscript was written by CL and all authors reviewed subsequent versions for intellectual content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
KJ received consulting fees from Janssen; the other authors declare no competing interests.
Ethical approval
Written informed consent or consultant consent from next-of-kin were obtained for all participants prior to enrollment. This study was approved by the Regional Ethics Review Board in Gothenburg, Sweden (registration numbers: 469-99, T553-03, 413-04, T665-07) and performed in accordance with the 1964 Helsinki Declaration.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lagging, C., Pedersen, A., Petzold, M. et al. Profiling 92 circulating neurobiological proteins identifies novel candidate biomarkers of long-term cognitive outcome after ischemic stroke. Sci Rep 15, 15328 (2025). https://doi.org/10.1038/s41598-025-99735-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-99735-w
