
Abstract
To evaluate the accuracy and safety of C1–C2 pedicle screw placement using O-arm navigation, individualized 3D-printed guides, and C-arm fluoroscopy. Clinical data of 47 patients who underwent C1–C2 spinal fixation surgery at our institution between January 2015 and December 2020 were retrospectively analyzed. The cohort included 28 males and 19 females, aged 15–59 years (mean age: 46.23 ± 9.97 years). Patients were categorized into three groups based on the screw placement technique: navigation group (11 cases; O-arm S8 navigation system), guide group (15 cases; individualized 3D-printed guides), and fluoroscopy group (21 cases; C-arm fluoroscopy guided by anatomical landmarks). Outcome measures included surgical time, screw placement time, intraoperative blood loss, single-pass screw placement success rate, screw placement accuracy, and complication rate. Surgical Metrics: The Navigation group demonstrated a mean surgical time of 120.72 ± 11.14 min, screw placement time of 20.00 ± 1.09 min, and blood loss of 225.81 ± 25.58 ml. The Guide group reported significantly shorter surgical time (97.46 ± 9.03 min, P < 0.001), shorter screw placement time (15.80 ± 1.93 min, P < 0.001), and reduced blood loss (162.66 ± 18.52 ml, P < 0.001). The Fluoroscopy group showed longer surgical time (121.04 ± 12.81 min) and higher blood loss (239.04 ± 24.54 ml) compared to the other groups. Screw Placement Success and Accuracy: A total of 188 screws were placed (44 in the Navigation group, 60; guide group, and 84; Fluoroscopy group). The single-pass success rates were 100% (44/44) in the navigation group, 93.3% (56/60) in the guide group, and 80.9% (68/84) in the fluoroscopy group (P = 0.002). Screw placement accuracy was 100% (44/44) in the navigation group, 98.3% (59/60) in the guide group, and 85.7% (72/84) in the fluoroscopy group (P = 0.039). Notably, three screws in the fluoroscopy group breached the vertebral artery foramen; however, no cerebrovascular ischemic events were observed. Complications: Two patients in the fluoroscopy group developed postoperative occipitocervical pain owing to intraoperative irritation of the C2 nerve root. Symptoms resolved after corticosteroid and diuretic therapy. No occipitocervical pain or other complications were reported in the Navigation or Guide group. All the incisions healed without infection or delayed recovery. O-arm S8 navigation system and individualized guide plate assisted atlantoaxial screw placement can achieve high and stable accuracy, which is better than the traditional freehand screw placement technique under fluoroscopy; O-arm navigation technology has an advantage in the one-time success rate of atlantoaxial screw placement, which is higher than that of the guide plate group and the fluoroscopy group; Individualized guide plate combined with lateral fluoroscopy can accurately place atlantoaxial screws, save operation time and reduce bleeding.
Similar content being viewed by others

Introduction
Posterior C1–C2 spinal fixation is an essential method for treating upper cervical spine fractures, C1–C2 joint dislocations, and other related disorders, and is widely utilized in clinical practice1,2,3. However, the C1–C2 region is in close proximity to the vertebral artery and high cervical spinal cord, posing a risk of damaging these structures during screw placement4,5,6. Additionally, due to significant anatomical variability in the C1–C2 region, determining the optimal entry point and screw angle is challenging. Failure in initial screw placement not only increases the difficulty of subsequent screw insertion7,8,9, but also decreases the screw purchase strength, which may adversely affect patient outcomes. Therefore, high precision and high single-pass screw placement success rate are crucial for C1–C2 fixation.
With the development of digital orthopedic technologies, intraoperative 3D navigation systems and individualized 3D-printed guides have emerged as valuable tools to assist in screw placement and provide clinical practitioners with helpful guidance. Numerous studies have reported the clinical applications of 3D navigation technology and individualized 3D-printed guides1,2,3,4,5,6, both of which have demonstrated superior outcomes compared to traditional freehand techniques. However, few studies have directly compared these two technologies in the context of C1–C2 spinal surgery.
To evaluate the clinical value of intraoperative O-arm navigation and individualized 3D-printed guide technologies for C1–C2 screw placement, and to explore their feasibility and accuracy in C1–C2 spinal fixation, this retrospective study analyzes 47 cases of C1–C2 fractures and dislocations treated with posterior cervical spine surgery from January 2015 to December 2020. This study aimed to compare the effectiveness of O-arm navigation, 3D-printed guide technology, and C-arm fluoroscopy-assisted screw placement to provide valuable clinical references for future treatment strategies.
Materials and methods
Inclusion and exclusion criteria
Inclusion criteria:
-
(1)
Age from 15 to 59 patients with reducible C1–C2 dislocations or instability requiring C1–C2 spinal fixation;
-
(2)
No contraindications to surgery, and able to tolerate the procedure;
-
(3)
Willing to participate in the study and provide informed consent.
The exclusion criteria were as follows:
-
(1)
patients with small or malformed pedicles, as seen on imaging, making pedicle screw insertion impossible, and those requiring laminar screw placement;
-
(2)
patients with anatomical variations such as high-riding or aberrant vertebral arteries that interfere with C1–C2 screw placement;
-
(3)
Patients with C1–C2 dislocations that cannot be reduced by traction and require anterior release;
-
(4)
patients with severe comorbidities;
-
(5)
incomplete imaging data or patients lost to follow-up.
General information
In this retrospective study, 52 patients were initially selected, with 5 lost to follow-up. Ultimately, 47 patients who underwent posterior C1–C2 spinal fixation surgery at our hospital from January 2015 to December 2020 were included in this study, all of whom met the aforementioned criteria. The cohort consisted of 28 male and 19 female patients, aged 15–59 years (mean age 46.23 ± 9.97 years). Nineteen patients had developmental deformities with C1–C2 dislocations, 25 had traumatic fractures with dislocations, and 3 had rheumatoid arthritis with C1–C2 dislocation. Clinical symptoms included limited occipitocervical mobility and posterior occipital pain, with 32 patients presenting symptoms or signs of spinal cord involvement. Follow-up duration was average 3–12 months (mean 7.20 ± 4.97 months). The study was approved by the Institutional Ethics Committee (LH-KY-2020-002-118), and informed surgical consent was obtained from all patients.
One-way analysis of variance shows that there was no significant difference in age, gender, BMI index, C1 -C2 pedicle anatomy (height and width) in the three groups. Patients were divided into three groups based on the method of screw insertion; The surgery was performed by the same group of doctors, who freely choose one of the three surgical methods:
-
Navigation group (11 cases, using the O-arm S8 navigation system for screw placement).
-
Guide group (15 patients using individualized 3D-printed guides for screw placement).
-
Fluoroscopy group (21 cases, C-arm fluoroscopy based on anatomical landmarks for screw placement).
-
Further details are provided in Table 1.
Table 1 General information of the three groups of patients.
Equipment and fabrication
Navigation group
An O-arm StealthStation S8 system (Medtronic, USA) was used for navigation. The navigation tools included a navigation probe, navigation retractor, and a 2.25 mm pedicle reamer.
Guide group
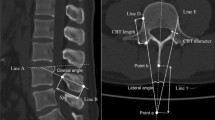
Preoperative CT scans of the C1–C2 region (slice thickness 0.25–0.5 mm) were performed, followed by 3D reconstruction. The scanned images were saved in DICOM format. Using Mimics software, the CT data were converted into a 3D model, and the positions of the screws were then designed (Fig. 1A, B). The C2 screw was placed centrally through the pedicle, while the C1 screw was positioned at the junction of the vertebral artery foramen and inner wall of the spinal canal, directed towards the anterior tubercle of the atlas. The screw diameter was 3.5–4.0 mm. Boolean operations were used to generate the guiding tubes, which were then saved as STL files. The vertebral body model and guiding tubes were then imported into the SolidWorks software, where smoothing treatments were applied. The design of the guiding plate base and arc support structure was finalized and exported as STL files. The arc support was adjusted in Mimics software to ensure stability during surgery while allowing the surgeon to easily manipulate the guide. The guiding tubes were placed at the outermost edge of the guide plate and an arc support was designed to prevent deformation during surgery.

TFabrication of individualized atlantoaxial guide (A, B). Use mimics software to synthesize the CT data into a 3D model, and then design the position of the screw; (C, D). Carry out the corresponding Boolean combination operation in the mimics software, and then carry out the Boolean difference operation, and finally design and form a suitable surgical guide; (E) The completed 3D printed atlantoaxial model and guide plate.
Subsequently, a gripping pillar with a diameter of 6 mm and length of 50 mm was created above the arc, and the corresponding Boolean operations were performed using the Mimics software(20.0 × 64 Materialise, which was runed by IBM computer(T580). Mimics 20.0 by Materialise is a powerful medical image processing software used for 3D reconstruction, analysis, and visualization of medical imaging data from CT and MRI scans. It enables users to extract and segment anatomical structures, create personalized treatment plans, design custom implants, and perform simulations for surgery planning. With tools for 3D printing, finite element analysis, and seamless integration with other Materialise software, Mimics 20.0 is widely used in clinical, research, and medical device design applications. It provides an intuitive interface for efficient and accurate workflows. After Boolean subtraction, the final individualized surgical guide was designed (Fig. 1C, D). The design files were then imported into a 3D printer (Daye 3D Printer S130, China) for dual printing, followed by postprocessing. One guide was printed and used for preoperative simulation on a 1:1 scale C1–C2 model (Fig. 1E). After Successful simulation on a 3D-printed C1-2 model, then the second guide was sterilized and used during the surgery. We recommend using ethylene oxide sterilization or low-temperature plasma sterilization. The specific sterilization parameters are detailed in the discussion.
Fluoroscopy group
Siemens C-arm fluoroscopy system (Siremobil Iso-C3D) was used to facilitate AP/lateral position fluoroscopy in operation.
Surgical methods
Following endotracheal intubation and general anesthesia, cranial traction was applied to maintain cervical alignment. The patient was then positioned prone with the neck flexed by Mayfield head frame. A posterior midline incision was made to expose the posterior arch of the atlas (C1) and lamina and lateral masses of the axis (C2).
Navigation group
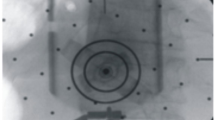
The reference frame was fixed to the spinous process of axis (C2). The O-arm was used to obtain 3D images of the C1–C2 region, which were then transferred to the navigation system. After registering the navigation tools, a navigation probe was placed at the mid-point of the posterior arch of the atlas to verify the accuracy of navigation data. Using real-time 3D images provided by the navigation system, pilot holes were drilled and the pedicle screw pathways were widened in the C2 pedicle and C1 lateral mass (Fig. 2A, B). The screws were threaded and inserted.

Fabrication of nail tracks guided by 3D images (A). Fabrication of the atlas screw track under the guidance of 3D images; (B). Fabrication of Axis’s Screw Road under the Guidance of 3D Image.
Guide group
The soft tissues around the midline of the posterior arch of the atlas and the spinous process of the axis were carefully removed. The C2 guide was placed on the spinous process and lamina of the axis to ensure tight contact and minimize errors. The assistant maintained a constant pressure to stabilize relative position between the pedicle and the guide during the drilling process. A 1.0–1.5 mm Kirschner wire was inserted through the guide at a set angle, advancing approximately 20 mm. The C1 guide was similarly placed on the posterior arch of the atlas, and a 1.0–1.5 mm Kirschner wire was inserted along the guide’s direction to a depth of approximately 20 mm. Kirschner wires of various diameters were used to confirm proper alignment in the pre-planned direction under C-arm fluoroscopy in the lateral view. Once confirmed, the screw pathway was widened to the desired depth, guide was removed, and spherical probe was used to confirm the path. After verifying the accuracy, tapping was performed and the screws were inserted.
Fluoroscopy group
The lateral masses of the axis were further exposed and the upper edge of the C2 pedicle was identified. A hole was drilled 2 mm lateral to the mid-point of the C2 mass. The C2 pedicle’s superior edge was visualized, and the hole was progressively enlarged along the pedicle direction. After every 5 mm of drilling, the hole was checked for bleeding and the walls were probed to confirm completeness. For the atlas, a small curette was used to expose the inferior edge of the posterior arch, approximately 20 mm lateral to the midline, revealing the lateral mass of the atlas. A cotton swab was placed to retract the greater occipital nerve, and a hole was drilled at the center of the lateral mass, directed approximately 5° downward and 10° inward. After every 5 mm of drilling, the walls were probed to ensure the bone integrity. Four Kirschner wires of different diameters were placed to confirm the screw pathway positioning using C-arm fluoroscopy. If the wires were misaligned, the direction was adjusted until the correct positioning was achieved. After satisfactory placement, the holes were tapped and screws were inserted.
Postoperative procedure
After screw insertion was completed in all three groups, internal fixation devices were applied. The surgical area was irrigated, and a burr was used to decorticate the cortical bone of the posterior arch of the atlas and the lamina of the axis. Granular cancellous bone was harvested from the iliac crest and inserted between the atlas and axis. A drain was placed, and the incision was closed in the layers.
Outcome measures
Surgical time
The total surgical time was defined as the time from the start of the skin incision to the completion of suturing.
Screw placement time
Screw placement time was defined as the period from the completion of lamina muscle resection to the insertion of the last screw.
Single-Pass screw placement success rate
Single-pass success was defined as the completion of lamina muscle resection to the insertion of the last screw placement process (including cortical bone perforation, widening of the pedicle screw pathway, and confirmation of the integrity of the screw path with a probe) without the need for adjustments to the hole or screw direction or re-insertion due to screw loosening. If adjustments or re-insertion were required during the process, it was classified as a failure to achieve single-pass screw placement. The single-pass success rate is calculated as follows:
Screw placement accuracy evaluation
Postoperative thin-slice CT scans (slice thickness 0.25–0.5 mm) were performed and reconstructed. The accuracy of screw placement was evaluated using 3D images obtained from postoperative CT scans3. The classification criteria are as follows:
-
Grade 0: All screws are entirely within the pedicle.
-
Grade I: Screw penetration of the pedicle was less than 25% of the screw diameter.
-
Grade II: Screw penetration of the pedicle was between 25% and 50% of the screw diameter.
-
Grade III: Screw penetration of the pedicle exceeding 50% of the screw diameter, with screws entering the vertebral artery foramen or spinal canal.
Statistical analysis
The data were analyzed using SPSS version 19.0. Continuous variables were expressed as mean ± standard deviation (SD). For comparisons between multiple groups, one-way analysis of variance (ANOVA) was used, with the significance level set at P < 0.05. Categorical variables are expressed as frequencies and percentages, and group comparisons were performed using the chi-square test. A two-tailed significance level of α = 0.05 was used for all statistical tests.
Results
Surgical time, screw placement time, blood loss, and Single-Pass screw placement success rate
Surgical time, screw placement time, blood loss, and single-pass screw placement success rates for the navigation, guide, and fluoroscopy groups are shown in Table 2. Statistically significant differences were observed among the three groups in terms of surgical time, screw placement time, blood loss, and single-pass screw placement success rate. The Guide group had a shorter surgical time, shorter screw placement time, and less blood loss than the other two groups. The Navigation group demonstrated a higher single-pass screw placement success rate than the other two groups.
In the Guide group, all four screws that required adjustment were placed in the C1 screw pathway. Of the 16 screws requiring adjustment in the fluoroscopy group, 9 were in the C2 screw pathway and 7 were in the C1 screw pathway.
Screw placement accuracy
In the Navigation group, 44 screws were graded as grade 0 (100% accuracy), with no screws graded as Grade I, II, or III. In the Guide group, 59 screws were graded as grade 0, one screw was graded as Grade I, and no screws were graded as Grade II or III. In the Fluoroscopy group, 72 screws were graded as Grade 0, 6 screws were graded as Grade I, 3 as Grade II, and 3 as Grade III. Screw placement accuracy was 100% in the navigation group, 98.3% in the guide group, and 85.7% in the fluoroscopy group. Statistically significant differences were observed between the groups (P = 0.039), with the fluoroscopy group showing the lowest accuracy. Additionally, in the Fluoroscopy group, 3 screws breached the vertebral artery foramen, but no postoperative cerebrovascular ischemic events were observed. Representative cases are shown in Figs. 3, 4, and 5, respectively.

Patients in the navigation group, male, 15 years old, developmental odontoid nonunion. Atlantoaxial internal fixation under O-arm machine navigation (A, B). Preoperative dynamic X-ray shows atlantoaxial instability; (C) Preoperative sagittal reconstruction CT images showed odontoid nonunion; (D–E) Real-time display of operating tool position in transverse, sagittal, and coronal views; (F, G) Postoperative atlantoaxial frontal and lateral radiographs; (H–K) Postoperative traverse and sagittal CT images showed that the atlantoaxial screw was in good position and did not enter the vertebral foramen and spinal canal.

Patients in the guide group, female, 52 years old, rheumatoid arthritis, atlantoaxial instability. Atlantoaxial internal fixation under the guidance of guide plate (A–C). Preoperative X-rays showing atlantoaxial instability; (D) Preoperative sagittal reconstruction CT images showed atlantoaxial dislocation; (E) Intraoperative picture showing: Guide screw placement using guide plate; (F, G) Postoperative atlantoaxial frontal and lateral radiographs; (H–K). Postoperative traverse and sagittal CT images showed that the atlantoaxial screw was in good position and did not enter the vertebral foramen and spinal canal.

Patients in the fluoroscopy group, female, 57 years old, rheumatoid arthritis, atlantoaxial instability. Atlantoaxial internal fixation with free-hand screw placement under the aid of C-arm fluoroscopy (A–C). Preoperative dynamic X-ray showed atlantoaxial instability; (D) Preoperative MRI showed atlantoaxial dislocation and spinal cord compression; (E) Preoperative sagittal reconstruction CT showed atlantoaxial dislocation; (F) Intraoperative fluoroscopy showed that the positioning needle had been placed in the atlantoaxial nail canal; (I–L). Postoperative anteroposterior and lateral images of atlantoaxial internal fixation; (H–K). The traverse and sagittal CT images showed that the right axial screw entered the foramen of vertebral artery.
Complications
Postoperatively, two patients in the fluoroscopy group developed occipitocervical pain, which was attributed to intraoperative irritation of the C2 nerve root. These symptoms were alleviated by corticosteroid and diuretic treatment. No occipitocervical pain was observed in the Navigation or Guide group. All patients in the three groups showed primary wound healing with no wound infections.
Discussion
Comparison of Single-Pass screw placement success rate and screw placement accuracy
For patients with C1–C2 dislocations, stable C1–C2 fixation is essential for deformity correction and fusion, and the stability of the fixation system relies on the precise placement of screws. Poor screw placement can reduce the strength and corrective ability of the internal fixation system and may lead to various complications such as nerve root injury, spinal cord injury, vascular damage, and fractures10,11,12,13. The traditional method of C1–C2 screw insertion involves C-arm fluoroscopy guidance, relying on anatomical landmarks, clinical experience, and tactile feedback to place the screws. However, C-arm fluoroscopy only assists with the sagittal angle of screw placement, not the angulation of the screw within the pedicle, nor can it assess whether the screw enters the vertebral artery foramen or the spinal canal. Additionally, anatomical variations in the C1–C2 region, changes in patient positioning, and deviation of the entry point can alter the screw trajectory. As a result, using traditional techniques for C1–C2 screw placement carries an inherent risk of error13,14,15,16. If screw position adjustment is required after fluoroscopic imaging, it may decrease the holding strength of the screw, increasing the risk of screw loosening or breakage17,18,19. With the maturation of screw placement techniques and accumulation of clinical experience, C-arm fluoroscopy-assisted freehand placement has yielded acceptable treatment outcomes. However, screw misplacement rates still range from 14 to 23%, with 2.7–3.3% of patients experiencing vertebral artery damage, and some cases even result in death11,20. In the present study, the single-pass success rates for screw placement were 100% in the navigation group, 93.3% in the guide group, and 80.9% in the fluoroscopy group. The Navigation group demonstrated a higher single-pass success rate than the Guide and Fluoroscopy groups. The navigation, guide, and fluoroscopy groups achieved 100%, 98.3%, and 85.7% screw accuracy, respectively. In the Fluoroscopy group, 12 screws breached the cortical bone of the C2 pedicle or the inner cortical bone of the C1 posterior arch, with 3 screws entering the vertebral artery foramen. These results suggest that both O-arm navigation and individualized guides improve screw placement accuracy compared with traditional fluoroscopy, with O-arm navigation offering the highest precision.
Advantages and disadvantages of O-arm navigation and usage precautions
Computer-assisted navigation technology originated in the early 20th century. Early versions of this technology were complicated, time-consuming, and lacked high precision, which limited its clinical application1,10. However, with advancements in computer and imaging technologies, 3D navigation has matured and is increasingly used in the field of spinal surgery16,17. Numerous studies have confirmed that navigation-assisted screw placement can significantly improve the accuracy of pedicle screw insertion1,3,10,16,17. Navigation systems are typically divided into CT-based- and C-arm X-ray-based systems. CT-based navigation systems offer high precision and clear imaging, which is especially beneficial for complex regions like the C1–C2 vertebrae, where X-ray imaging is often difficult. In this study, the O-arm S8 navigation system, which is the latest CT-based intraoperative imaging system, was used for screw placement. This system can provide real-time 3D imaging and guide screw placement with an error margin of less than 2 mm. All screws in the navigation group were successfully placed in a single pass with secure fixation and no loosening postoperatively, demonstrating that O-arm navigation improves the single-pass screw placement success rate and reduces the risk of complications. However, the O-arm navigation system has certain limitations. The reference frame cannot be moved during use; otherwise, erroneous positioning images are produced. In addition, the relative displacement between the C1–C2 vertebrae during positioning can cause image drift. The following precautions and techniques are recommended for optimal use of O-arm navigation. Reference Frame Placement: The reference frame should be placed securely on the spinous process of the axis (C2) to minimize image drift due to relative displacement. Pre-Scan Setup: Before scanning, ensure that the reflective balls on the reference frame and reflective points on the O-arm base are within the range of the infrared camera. Automatic Parameter Settings: The system automatically sets the current to 100 mA, the pulse width to 10ms, and the exposure to 100 kV. After collecting the data, the system reconstructs the 3D images and transfers them to the S8 navigation workstation, which displays the axial, coronal, and sagittal virtual images. Radiation Protection: After data acquisition, wait for at least 10 s before leaving the isolation screen to reduce the X-ray exposure. The navigation system did not emit X-rays during the procedure. Avoid obstruction: During screw placement, avoid obstructing or touching the reference frame to prevent image drift. Accuracy Check: Before and during the screw placement process, the probe was placed at the midpoint of the posterior arch of the atlas to verify the accuracy of the navigation system. Any image drift was corrected immediately. Drilling Technique: When drilling, a burr is used to avoid excessive force that may shift the vertebrae, thereby affecting navigation accuracy. After each 2–4 mm of drilling, stop pushing the vertebra and check the position and direction of the probe. By adhering to these precautions, the accuracy and reliability of O-arm navigation can be maximized, enhancing the overall success of C1–C2 screw placement surgeries.
Advantages and disadvantages of individualized 3D printed guides and usage precautions
In recent years, digital orthopedic technology has rapidly developed, and the use of 3D-printed guides for screw placement has enabled more personalized and precise surgical procedures4,7,12. Preoperative 3D printed models accurately reproduce the anatomy of the C1–C2 region, and individualized 3D printed guides are designed based on pre-established angles and directions. These guides offer optimal entry points and screw trajectories during surgery and are not affected by changes in patient positioning, improve screw placement accuracy, and reduce the risk of spinal cord, nerve, and vascular injury8,18,19. Chen et al.12 applied individualized 3D printed guides to screw placement in 12 C1–C2 specimens, achieving a screw placement accuracy of 97.92%, with only one screw breaching the cortical bone of the pedicle. Overall, the literature suggests that individualized 3D printed guides, compared to freehand placement, reduce surgical time and blood loss compared to freehand placement4,7,8,12,14,15,18,19. In this study, the guide group had less surgical time, screw placement time, and blood loss than both the Fluoroscopy and Navigation groups.
Although the Guide group showed high screw placement accuracy, 3D printed guides could still introduce errors. In our study, the single-pass screw placement success rate in the guide group was 93.3% (56/60), with 4 screws (all C1 screws) requiring adjustment for the head tilt angle. The causes of these errors and methods for their prevention includeC1 Posterior Arch Anatomy: The small, circular shape of the C1 posterior arch and its relatively simple bony structure compared to the axis can cause the guide to not fit precisely during the procedure, leading to errors in the head tilt angle. This could be corrected by adjusting the angle using lateral fluoroscopy. For the axis, the larger spinous process and lamina allow for a better guide fit and reduce the likelihood of head-tilt errors. Micromovements during screw insertion: The C1–C2 vertebrae can experience slight movements under pressure during the drilling process, which may affect the accuracy of screw placement. To mitigate this, the guide should be firmly held in place by the assistant to keep the relative position of the guide and lamina or pedicle and a powered drill should be used during the procedure. Precision of 3D Printed Models and guide fit: If the CT scan slice thickness is set to 1 mm, there may be slight discrepancies between the 3D model and the actual vertebrae. This can lead to small errors in the guide and screw trajectories. To avoid this, CT scan slice thickness should be set between 0.25 mm and 0.5 mm. Preventing Guide Deformation: To prevent deformation of the 3D printed guide during surgery, the guide should be designed with a wide base and bridge structure using rigid materials. Placement of Guide directional sleeve: To reduce the need for extensive dissection of the posterior structures of the C1–C2 vertebrae, the guiding sleeve on the 3D printed guide should be placed at the outermost edge of the guide. Drill Depth Control: To avoid breaching the anterior edge of the vertebral body during screw-path expansion, the reamer should be set to a controlled depth. This depth corresponds to the screw length and length of the guiding sleeve. Guide Sleeve Length and Wall Thickness: The sleeve should have a minimum length of 25 mm and a wall thickness of at least 2 mm to ensure precise guidance and to prevent screw path misalignment. Smooth Internal Surface of Guide Sleeves: The internal diameter of the guide sleeve should be 0.2 mm larger than the drill bit diameter, and it should be smoothed to minimize friction, prevent collisions, and reduce debris generation. Sterilization and Deformation Prevention: To prevent deformation during sterilization, it is recommended to use ethylene oxide sterilization or low-temperature plasma sterilization. Here are the general parameters for ethylene oxide (EO) sterilization: ⑴ Temperature: Typical range: 37–63 °C (100–145 °F) Typical operational temperature: 55–60 °C. ⑵ Humidity: The relative humidity is an important parameter in EO sterilization, typically maintained at 40–80% RH. ⑶EO Concentration: The typical concentration is 450–1200 mg/L; The most effective concentration is usually around 700 mg/L. ⑷Exposure Time: Sterilization cycle duration: 1–6 h, depending on temperature, humidity, and EO concentration. Higher temperature and humidity usually require shorter exposure times. ⑸Vacuum: A vacuum is typically used during the sterilization process to evacuate air and ensure that the EO gas fully penetrates and reaches all areas of the items being sterilized. ⑹Aeration/Exhaust: After sterilization, an aeration phase is required to remove any residual EO gas from the items. This typically lasts 8–12 h to ensure complete removal of EO gas residues.
Low-temperature plasma sterilization typically involves the following parameters: ⑴Temperature: Between 50 °C and 60 °C. ⑵Gas: Primarily hydrogen peroxide (H₂O₂). ⑶Concentration: Usually between 58% and 95%. ⑷Exposure Time: Typically ranging from 45 min to 1 h, depending on the item and equipment. ⑸Pressure: Maintained at or slightly below ambient pressure. ⑹Vacuum: A vacuum pre-treatment is followed by hydrogen peroxide injection and plasma generation.
Individualized 3D printed guides offer high accuracy, ease of use, and low cost for C1–C2 screw placement, but the creation of models and personalized guides requires one to three days, making them unsuitable for emergency surgeries.
Study limitations
Firstly, this study was a retrospective analysis with a relatively small sample size and a short follow-up duration. Future prospective randomized controlled trials with larger sample sizes and multicenter studies are needed to validate O-arm navigation system was used for a relatively short time, and there may be variability in the user experience, which could have impacted the results. Secondly, in this retrospective study, the choice of the surgical method was based on the surgeon’s preference and available resources at the time of the surgery. The decision-making process for the surgical method was influenced by factors such as the surgeon’s familiarity with each technique, the availability of the technology, and the complexity of the patient’s anatomy. Additionally, financial and institutional constraints may have played a role in the choice of technique. However, it is important to note that this is a retrospective analysis, and no formal randomization or predetermined selection criteria were applied to the surgical method. Thirdly, the absence of patients over the age of 59 in a C1–C2 study is valid, especially considering the potential challenges posed by decreased bone mineral density in older patients. The decision to limit the age range in our study was based on our institutional protocol, which prioritizes younger patients in certain types of spinal surgeries due to the nature of the anatomical considerations and surgical risks. This decision was influenced by the desire to maintain homogeneity in the study population. However, we acknowledge that the age limitations of study need further investigation. Fourthly, 32/47 (68%) patients had signs or symptoms of spinal cord involvement. This high rate is reflective of the specific the patients included in the study, many of whom had spinal instability. The incidence of these preoperative neurological symptoms should be considered normal. This high incidence of spinal cord involvement are also related to the number of the cases of the study.
In summary, both the O-arm S8 navigation system and individualized 3D printed guides assist in achieving high and stable screw placement accuracy, superior to traditional freehand C-arm fluoroscopy-guided techniques. O-arm navigation demonstrated an advantage in the single-pass screw placement success rate compared with both the Guide and Fluoroscopy groups. Individualized 3D printed guides, combined with lateral fluoroscopy, provide precise screw placement while saving surgical time and reducing blood loss.
Data availability
The data that support the findings of this study are not openly available due to reasons of sensitivity and are available from the corresponding author upon reasonable request. Data are located in controlled access data storage at Luohe Center Hospital.
References
Jannelli, G. et al. Atlantoaxial posterior screw fixation using intra-operative spinal navigation with three-dimensional isocentric C-arm fluoroscopy. Int. Orthop. 46(2), 321–329 (2022).
Chen, Z. D. et al. C1–C2 pedicle screw fixation for pediatric atlantoaxial dislocation: Initial results and Long-term Follow-up. J. Pediatr. Orthop. 40(2), 65–70 (2020).
Zhao, R. et al. Efficacy comparison of O-arm assisted versus freehand posterior C1–C2 pedicle screw fixation for atlantoaxial fractures. Chin. J. Traumatol. 37(1), 30–36 (2021).
Li, Y. et al. Comparative study of 3D printed navigation template-assisted atlantoaxial pedicle screws versus free-hand screws for type II odontoid fractures. Eur. Spine J. 30(2), 498–506 (2021).
Lee, J. S. et al. Comparative analysis of surgical outcomes of C1-2 fusion spine surgery between intraoperative computed tomography image-based navigation-guided operation and fluoroscopy-guided operation. J. Korean Neurosurg. Soc. 63(2), 237–247 (2020).
Wang, H. et al. Intraoperative real-time three-dimensional navigation-assisted C1–C2 transarticular screw fixation for atlantoaxial instability. Chin. J. Orthop. 39(21), 1311–1319 (2019).
Cheng, J. et al. Accuracy study of individual 3D printed navigation template-assisted C1–C2 screw placement in atlantoaxial fractures. Practical Med. J. 37(18), 2380–2385 (2021).
Minyi, Y. et al. Three-dimensional printed model-assisted screw installation in treating posterior atlantoaxial internal fixation. Sci. Rep. 8(1), 11026 (2018).
Meyer, M. et al. Minimally invasive percutaneous C1–C2 fixation using an intraoperative three-dimensional imaging-based navigation system for management of odontoid fractures. World Neurosurg. 137(5), 266–271 (2020).
Wada, K. et al. Comparison of atlantoaxial fusion with transarticular screws and C1 lateral mass-C2 screws using intraoperative O-arm navigation. World Neurosurg. 141(9), e1005–e1009 (2020).
Yue-Hui, Z. et al. Efficacy and safety of atlantoaxial fluoroscopy-guided pedicle screw fixation in patients younger than 12 years: A radiographic and clinical assessment. Spine 44(20), 1412–1417 (2019).
Pu, X. et al. Clinical application of atlantoaxial pedicle screw placement assisted by a modified 3D-printed navigation template. Clin. (Sao Paulo) 73(7), e259 (2018).
Wu, C. et al. Clinical study of a composite 3D printing navigation template-assisted screw placement in the C2 pedicle or lamina. Chin. J. Spine Spinal Cord 28(11), 982–988 (2018).
Wang, Y. et al. Clinical application of a modified digital navigation template in individual C1–C2 screw placement. Chin. J. Experimental Surg. 37(4), 627–631 (2020).
Ouyang, P. et al. Application of 3D printed navigation templates in atlantoaxial pedicle screw placement. Chin. J. Traumatol. Orthop. 22(10), 862–866 (2020).
Dong, Q. et al. Comparison of accuracy in freehand, 3D printed template-assisted, and navigation-assisted screw placement in scoliosis surgery. Chin. J. Spine Spinal Cord 31(8), 683–692 (2021).
Ling, C. et al. Accuracy study of C-arm combined with CT three-dimensional navigation system for cervical pedicle screw placement. Chin. J. Spine Spinal Cord 32(3), 207–213 (2022).
Tian, Y. et al. A comparative study of C2 pedicle or Pars screw placement with assistance from a 3-dimensional (3D)-printed navigation template versus C-arm based navigation. Med. Sci. Monit. 25(12), 9981–9990 (2019).
Pu, X. et al. Design and application of a novel patient-specific three-dimensional printed drill navigational guiding in atlantoaxial pedicle screw placement. World Neurosurg. 114(6), e1–e10 (2018).
Pham, M. H. et al. Evaluation of C2 pedicle screw placement via the freehand technique by neurosurgical trainees. J. Neurosurg. Spine 29(3), 235–240 (2018).
Acknowledgements
Not applicable.
Funding
The authors were funded by the Medical Science and Technology Research Project of Henan Province. Project Code: LHGJ20201025, and the study was approved by the Institutional Ethics Committee (LH-KY-2020-002-118), and all patients provided informed surgical consent. Yuwei Li conducted this study.
Author information
Authors and Affiliations
Contributions
“Yuwei Li and Zimin Wang wrote the main manuscript text and Xiuzhi Li, Wei Cui, Peng Zhou, and Xiao Wei prepared figures . Li et al. reviewed and selected the final studies for the analysis. Xiuzhi Li, Wei Cui, Peng Zhou, and Xiao Wei advised on study design and data analysis. Yuwei Li drafted the manuscript, which was edited by Haijiao and Zimin Wang. All the authors have read and approved the final manuscript.All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Ethics Review Committee of Luohe Central Hospital reviewed the research project submitted by Dr. Li Yuwei and colleagues and determined that this project met the relevant requirements outlined in the National Guidelines for Biomedical Research Ethics. Upon examination, the committee approved the initiation of relevant scientific research. Project Code: LH-KY-2020-002-118.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, Y., Wang, H., Li, X. et al. Comparison of accuracy in C1–C2 pedicle screw placement: O-arm, 3D guides, and C-arm fluoroscopy. Sci Rep 15, 15731 (2025). https://doi.org/10.1038/s41598-025-99884-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-99884-y
